
Involvement of Local Authorities in the Protection of Residents’ Health in the Light of the Smart City Concept on the Example of Polish Cities

Abstract
:1. Introduction
- assess the involvement of Polish city authorities in protecting the health of their residents, and thus estimate their predisposition to be smart according to the sustainable SC concept (the level of readiness to meet the key needs of residents);
- identify the relationship between the size of the city and its commitment to identifying the health needs of its residents and the extent of actual healthcare efforts;
- formulate recommendations for improving health promotion activities in Polish cities.
2. Literature Overview
2.1. The Role of City Government in Smart City Development
- strategic goal: the city has a strategy that includes investment in Smart City solutions;
- data: the city collects data and information on the operation of the city and the needs of its residents, which it then processes and makes available, guaranteeing transparent and universal access to information for all stakeholders;
- technology: the city implements and uses modern technology to provide residents with the highest possible level of public services;
- governance and service delivery models: the city is adapting traditional organizational delivery models to take advantage of data and digital opportunities and investing in systemic partnership models focused on shared outcomes;
- stakeholder engagement: the city is systematically improving the uptake of digital services and taking steps to prevent digital exclusion.
2.2. Healthcare Issues in Smart City Literature
3. Materials and Methods
3.1. Research Intentions and Methods
- few studies on healthcare in cities aspiring to be smart and operating in developing economies;
- the need to supplement analyses in the social-management aspects of smart cities;
- conceptual and, less often, practical dimension of research on the real activities of Smart City authorities on the process of improving the quality of life of residents;
- lack of implementation;
- low implementation rate;
- average implementation rate;
- high implementation rate;
- very high implementation rate.
- Assessment of the city government’s involvement in activities in each area, taking into account statistical measures of central tendency (arithmetic mean; dominant; and median) and measures of variation (standard deviation; coefficient of variation). Central tendency measures were used to indicate the average and most frequent levels of involvement of city authorities in protecting the health of residents. The measures of variation were used to reflect the differences between the studied cities.
- (a)
- arithmetic mean:where:
- —the variable value;
- N—the number of variables;
- (b)
- dominant:where:
- —the lower bound of the class in which the dominant is found;
- —the size of the dominant interval;
- the size of the interval preceding the dominant interval;
- —the size of the interval following the interval of the dominant;
- —the dominant interval;
- (c)
- median:when N is odd:when N is even:where:
- —the variable value;
- N—the number of variables;
- (d)
- standard deviation:where:
- —the variable value;
- N—the number of variables;
- (e)
- coefficient of variation:where:
- —arithmetic mean;
- s—standard deviation.
- Identification of the relationship between monitoring the identified health needs of residents and the size of the city and the real actions of local governments to protect residents using Spearman’s rank correlation coefficient. It identifies the strength and direction of correlations between variables. The assumed significance level is p < 0.01. This coefficient takes values from −1 to 1. The higher its absolute value, the stronger the relationship between the variables. The coefficient was used to verify whether the size of the city and the monitoring of the health needs of residents are related to the level of involvement of the city authorities in healthcare activities.
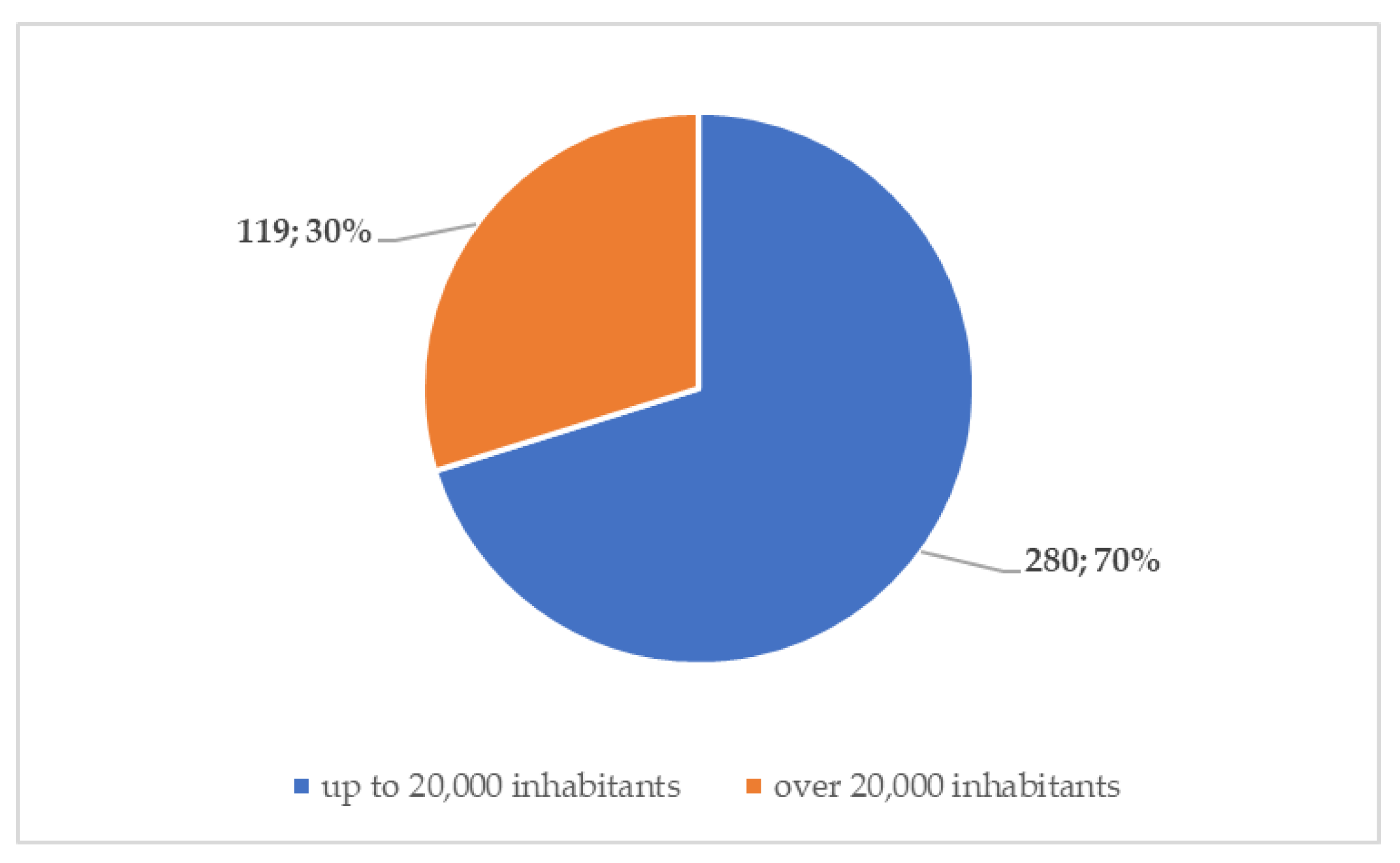
3.2. Research Sample Characteristics
4. Results
4.1. Assessment of the City Government’s Commitment to Specific Areas of Healthcare
4.2. Interdependence Analysis: Health Needs Monitoring—Healthcare Activities and City Size—Healthcare Activities
- between health needs monitoring and individual healthcare activities to answer the question: Whether and to what extent does monitoring the health needs of residents affect the subsequent involvement of the surveyed cities in real healthcare activities?
- between the size of cities, expressed in terms of population, and individual health measures, to obtain an answer to the question: Does the size of a city determine the scale of the city’s involvement in health-promoting activities for its residents?
- running information and education activities for residents oriented towards health promotion, prevention, and creation of conditions conducive to health, which is based on indirect contact, e.g., using mass media;
- running information and education activities for residents focusing on health promotion, prevention, and creation of conditions conducive to health, which is based on direct contact, e.g., thematic meetings with experts;
- organizing and carrying out immunizations for residents;
- organizing hygienic and medical care for children and teenage students.
- establishing new green zones in the city, such as squares and parks;
- running information and education activities for residents oriented towards health promotion, prevention, and creation of conditions conducive to health, which are based on indirect contact, e.g., using mass media;
- running information and education activities for residents focusing on health promotion, prevention, and creation of conditions conducive to health, which are based on direct contact, e.g., thematic meetings with experts.
5. Discussion
- before developing a municipal health action strategy—they should identify and then monitor the health needs of the community, which would increase the efficiency and effectiveness of public action;
- healthcare activities should be holistic and sequential, because only then can they be effective and improve the quality of urban life, and therefore should include not only sports and recreation and investment in medical infrastructure, but also health education, prevention, and environmental and climate protection;
- activities in the area of population health education should be strengthened and developed, as they can reduce morbidity and thus reduce budget expenditures on medical care; they are also an effective support for preventive healthcare;
- environmental and climate protection activities also need to be improved, both on the part of the city authorities and the residents themselves; an important role in this process is played by the formation of environmental awareness and desired behavior.
6. Conclusions
- the activities of the surveyed cities focus on the sphere of recreation and sports, which contributes to both health and resident satisfaction, but may involve a focus on image effects and ignoring other areas related to healthcare;
- health education and environmental and climate protection are the areas in which the surveyed cities are least involved, posing a serious threat to the continuity and holistic nature of efforts to maintain and improve community health;
- the surveyed cities are strongly differentiated in terms of investment in medical infrastructure (a high engagement rating dominates with a relatively low arithmetic mean);
- actions for specific areas of healthcare are more strongly determined by the fact of monitoring health needs than by the size of the city, this is especially true for health education and environmental and climate protection.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Falco, S.; Angelidou, M.; Addie, J.-P.D. From the “Smart City” to the “smart metropolis”? Building resilience in the urban periphery. Eur. Urban Reg. Stud. 2019, 26, 205–223. [Google Scholar] [CrossRef] [Green Version]
- Qayyum, S.; Ullah, F.; Al-Turjman, F.; Mojtahedi, M. Managing smart cities through six sigma DMADICV method: A reviewbased conceptual framework. Sustain. Cities Soc. 2021, 72, 103022. [Google Scholar] [CrossRef]
- Bina, O.; Inch, A.; Pereira, L. Beyond techno-utopia and its discontents: On the role of utopianism and speculative fiction in shaping alternatives to the Smart City imaginary. Futures 2020, 115, 102475. [Google Scholar] [CrossRef]
- Datta, A. A 100 smart cities, a 100 utopias. Dialogues Hum. Geogr. 2015, 5, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Grossi, G.; Pianezzi, D. Smart cities: Utopia or neoliberal ideology? Cities 2017, 69, 79–85. [Google Scholar] [CrossRef]
- Valdez, A.-M.; Cook, M.; Potter, S. Roadmaps to utopia: Tales of the Smart City. Urban Stud. 2018, 55, 3385–3403. [Google Scholar] [CrossRef]
- Anthopoulos, L. Smart utopia VS smart reality: Learning by experience from 10 Smart City cases. Cities 2017, 63, 128–148. [Google Scholar] [CrossRef]
- Engelbert, J.; van Zoonen, L.; Hirzalla, F. Excluding citizens from the European Smart City: The discourse practices of pursuing and granting smartness. Technol. Forecast. Soc. Chang. 2019, 142, 347–353. [Google Scholar] [CrossRef]
- Shelton, T.; Lodato, T. Actually existing smart citizens. City 2019, 23, 35–52. [Google Scholar] [CrossRef]
- Arnkil, R.; Järvensivu, A.; Koski, P.; Piirainen, T. Exploring Quadruple Helix Outlining User Oriented Innovation Models. Työraportteja. 85/2010. Working Papers. Available online: https://trepo.tuni.fi/handle/10024/65758 (accessed on 10 January 2023).
- Klasnic, J. Specific barriers for quadruple helix innovation model development—Case of Croatia. In Proceedings of the ENTRENOVA Conference, Rovinj, Croatia, 8–9 September 2016; IRENET: Zagreb, Croatia, 2016; pp. 399–407. [Google Scholar]
- de Waal, M.; Dignum, M. The citizen in the Smart City. How the Smart City could transform citizenship. Inf. Technol. 2017, 59, 263–273. [Google Scholar] [CrossRef]
- March, H.; Ribera-Fumaz, R. Smart contradictions: The politics of making Barcelona a Self-sufficient city. Eur. Urban Reg. Stud. 2016, 23, 816–830. [Google Scholar] [CrossRef] [Green Version]
- Capdevila, I.; Zarlenga, M. Smart City or smart citizens? The Barcelona Case. J. Strategy Manag. 2015, 8, 266–282. [Google Scholar] [CrossRef]
- Carayannis, E.G.; Campbell, D.F.J. Triple Helix, Quadruple Helix and Quintuple Helix and how do knowledge, innovation, and environment relate to each other? Int. J. Soc. Ecol. Sustain. Dev. 2010, 1, 41–69. [Google Scholar] [CrossRef]
- Cardullo, P.; Kitchin, R. Smart urbanism and smart citizenship: The neoliberal logic of ‘citizen-focused’ smart cities in Europe. Environ. Plan. C Politics Space 2019, 37, 813–830. [Google Scholar] [CrossRef] [Green Version]
- Giffinger, R. Smart cities ranking: An effective instrument for the positioning of the cities? ACE Archit. City Environ. 2010, 4, 7–26. [Google Scholar] [CrossRef] [Green Version]
- Samarakkody, A.; Amaratunga, D.; Haigh, R. Characterising Smartness to Make Smart Cities Resilient. Sustainability 2022, 14, 12716. [Google Scholar] [CrossRef]
- Shen, L.; Huang, Z.; Wong, S.W.; Liao, S.; Lou, Y. A holistic evaluation of Smart City performance in the context of China. J. Clean. Prod. 2018, 200, 667–679. [Google Scholar] [CrossRef]
- Cohen, B. The 3 Generations of Smart Cities. 2015. Available online: https://www.fastcompany.com/3047795/the-3-generations-of-smart-cities (accessed on 9 October 2022).
- Korenik, A. Rozwój Zrównoważony na Przykładzie Miast Inteligentnych. 2019. Available online: https://www.researchgate.net/publication/337608287_Rozwoj_zrownowazony_na_przykladzie_miast_inteligentnych_smart_cities?channel=doi&linkId=5de03c3c299bf10bc32ec9dd (accessed on 10 January 2023).
- Lai, C.S.; Jia, Y.; Dong, Z.; Wang, D.; Tao, Y.; Lai, Q.H.; Wong, R.T.K.; Zobaa, A.F.; Wu, R.; Lai, L.L. A Review of Technical Standards for Smart Cities. Clean Technol. 2020, 2, 19. [Google Scholar] [CrossRef]
- Shayan, S.; Kim, K.P. Understanding correlations between social risks and sociodemographic factors in smart city development. Sustain. Cities Soc. 2022, 89, 104320. [Google Scholar] [CrossRef]
- Alizadeh, H.; Sharifi, S. Societal smart city: Definition and principles for post-pandemic urban policy and practice. Cities 2023, 134, 104207. [Google Scholar] [CrossRef]
- Wang, M.; Zhou, T. Does smart city implementation improve the subjective quality of life? Evidence from China. Technol. Soc. 2023, 72, 102161. [Google Scholar] [CrossRef]
- Ahmad, A.; Ahmad, T.; Ahmad, M.; Kumar, C.; Alenezi, F.; Nour, M. A complex network-based approach for security and governance in the smart green city. Expert Syst. Appl. 2023, 214, 119094. [Google Scholar] [CrossRef]
- Deng, G.; Fei, S. Exploring the factors influencing online civic engagement in a smart city: The mediating roles of ICT self-efficacy and commitment to community. Comput. Hum. Behav. 2023, 143, 107682. [Google Scholar] [CrossRef]
- Sheikh, H.; Mitchell, P.; Foth, M. More-than-human smart urban governance: A research agenda. Digit. Geogr. Soc. 2023, 4, 100045. [Google Scholar] [CrossRef]
- Kaginalkar, A.; Kumar, S.; Gargava, P.; Niyogi, D. Stakeholder analysis for designing an urban air quality data governance ecosystem in smart cities. Urban Clim. 2023, 48, 101403. [Google Scholar] [CrossRef]
- Elbaz, K.; Hoteit, I.; Shaban, W.M.; Shen, S.-L. Spatiotemporal air quality forecasting and health risk assessment over smart city of NEOM. Chemosphere 2023, 313, 137636. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-W. Can smart cities bring happiness to promote sustainable development? Contexts and clues of subjective well-being and urban livability. Dev. Built Environ. 2023, 13, 100108. [Google Scholar] [CrossRef]
- Rodrigues, M.; Franco, M.; Oliveira, C.; Pinto Borges, A.; Silva, R.J. How have smartness cities responded to the pandemic? An empirical study. Cities 2023, 135, 104241. [Google Scholar] [CrossRef]
- Caragliu, A.; Del Bo, C.; Nijkamp, P. Smart Cities in Europe. J. Urban Technol. 2011, 18, 15–38. [Google Scholar] [CrossRef]
- Dameri, R.P. Searching for Smart City definition: A comprehensive proposal. Int. J. Comput. Technol. 2013, 11, 75–128. [Google Scholar] [CrossRef]
- Komninos, N. The Age of Intelligent Cities: Smart Environments and Innovation-for All Strategies; Routledge: London, UK, 2014. [Google Scholar]
- Vujković, P.; Ravšelj, D.; Umek, L.; Aristovnik, A. Bibliometric Analysis of Smart Public Governance Research: Smart City and Smart Government in Comparative Perspective. Soc. Sci. 2022, 11, 293. [Google Scholar] [CrossRef]
- Albino, V.; Berardi, U.; Dangelico, R.M. Smart Cities: Definitions, Dimensions, Performance, and Initiatives. J. Urban Technol. 2015, 22, 54–73. [Google Scholar] [CrossRef]
- Lim, S.B.; Yigitcanlar, T. Participatory Governance of Smart Cities: Insights from e-Participation of Putrajaya and Petaling Jaya, Malaysia. Smart Cities 2022, 5, 5. [Google Scholar] [CrossRef]
- Willis, K.S.; Nold, C. SmartAirQ: A Big Data Governance Framework for Urban Air Quality Management in Smart Cities. Front. Environ. Sci. 2022, 10, 785129. [Google Scholar]
- He, W.; Li, W.; Deng, P. Legal Governance in the Smart Cities of China: Functions, Problems, and Solutions. Sustainability 2022, 14, 9738. [Google Scholar] [CrossRef]
- Nina, X.; Hao, Z.; Huije, L.; Rongxial, Y.; Jia, W.; Zhongke, F. Performance Analysis of Smart City Governance: Dynamic Impact of Beijing 12345 Hotline on Urban Public Problems. Sustainability 2022, 14, 9986. [Google Scholar]
- Bokhari, S.A.A.; Myeong, S. Artificial Intelligence-Based Technological-Oriented Knowledge Management, Innovation, and E-Service Delivery in Smart Cities: Moderating Role of E-Governance. Appl. Sci. 2022, 12, 8732. [Google Scholar] [CrossRef]
- Carrato-Gómez, A.; Roig-Segovia, E. From the sustainable city to the hub city: Obsolescence and renewal of urban indicators. Ciudad Y Territ. Estud. Territ. 2022, 54, 563–578. [Google Scholar] [CrossRef]
- Faraji, S.J.; Jafari Nozar, M.; Arash, M. The analysis of smart governance scenarios of the urban culture in multicultural cities based on two concepts of “cultural intelligence” and “smart governance”. GeoJournal 2021, 86, 357–377. [Google Scholar] [CrossRef]
- Vitálišová, K.; Sýkorová, K.; Koróny, S.; Rojíková, D. Benefits and Obstacles of Smart Governance in Cities. In Science and Technologies for Smart Cities; SmartCity 360 2021; Lecture Notes of the Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering, LNICST, 442 LNICST; Springer: Cham, Switzerland, 2022; pp. 366–380. [Google Scholar]
- Hajduk, S. Modele Smart City a zarządzanie przestrzenne miast. Pol. J. Econ. 2020, 302, 123–139. [Google Scholar]
- Founoun, A.; Hayar, A.; Essefar, K.; Haqiq, A. Agile Governance Supported by the Frugal Smart City. Lect. Notes Netw. Syst. 2022, 334, 95–105. [Google Scholar]
- Laurini, R. A primer of knowledge management for Smart City governance. Land Use Policy 2021, 111, 104832. [Google Scholar] [CrossRef]
- Maurya, K.K.; Biswas, A. Performance assessment of governance in Indian Smart City development. Smart Sustain. Built Environ. 2021, 10, 653–680. [Google Scholar] [CrossRef]
- Fonseca, D.; Sanchez-Sepulveda, M.; Necchi, S.; Peña, E. Towards Smart City governance. Case study: Improving the interpretation of quantitative traffic measurement data through citizen participation. Sensors 2021, 21, 5321. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y. Toward sustainable governance: Strategic analysis of the Smart City Seoul portal in Korea. Sustainability 2021, 13, 5886. [Google Scholar] [CrossRef]
- Saadah, M. Artificial Intelligence for Smart Governance; towards Jambi Smart City. IOP Conf. Ser. Earth Environ. Sci. 2021, 717, 012030. [Google Scholar] [CrossRef]
- Wolniak, R.; Jonek-Kowalska, I. The Creative Services Sector in Polish Cities. J. Open Innov. Technol. Mark. Complex. 2022, 8, 17. [Google Scholar] [CrossRef]
- Jonek-Kowalska, I.; Wolniak, R. Sharing Economies’ Initiatives in Municipal Authorities’ Perspective: Research Evidence from Poland in the Context of Smart Cities’ Development. Sustainability 2022, 14, 2064. [Google Scholar] [CrossRef]
- Dohn, K.; Kramarz, M.; Przybylska, E. Interaction with City Logistics Stakeholders as a Factor of the Development of Polish Cities on the Way to Becoming Smart Cities. Energies 2022, 15, 4103. [Google Scholar] [CrossRef]
- Tantau, A.; Şanta, A.-M.I. New Energy Policy Directions in the European Union Developing the Concept of Smart Cities. Smart Cities 2021, 4, 15. [Google Scholar] [CrossRef]
- Naterer, A.; Žižek, A.; Lavrič, M. The quality of integrated urban strategies in light of the Europe 2020 strategy: The case of Slovenia. Cities 2018, 72, 369–378. [Google Scholar] [CrossRef]
- Jonek-Kowalska, I. Health Care in Cities Perceived as Smart in the Context of Population Aging—A Record from Poland. Smart Cities 2022, 5, 65. [Google Scholar] [CrossRef]
- Jonek-Kowalska, I. Municipal Waste Management in Polish Cities—Is It Really Smart? Smart Cities 2022, 5, 83. [Google Scholar] [CrossRef]
- Baltac, V. Smart Cities—A View of Societal Aspects. Smart Cities 2019, 2, 33. [Google Scholar] [CrossRef] [Green Version]
- Klimovský, D.; Pinterič, U.; Šaparnienė, D. Human Limitations to Introduction of Smart Cities: Comparative Analysis from Two CEE Cities. Transylv. Rev. Adm. Sci. 2016, 80–96. Available online: https://rtsa.ro/tras/index.php/tras/article/view/473 (accessed on 10 January 2023).
- Cepeliauskaite, G.; Keppner, B.; Simkute, Z.; Stasiskiene, Z.; Leuser, L.; Kalnina, I.; Kotovica, N.; Andiņš, J.; Muiste, M. Smart-Mobility Services for Climate Mitigation in Urban Areas: Case Studies of Baltic Countries and Germany. Sustainability 2021, 13, 4127. [Google Scholar] [CrossRef]
- Kopacova, H. Reflexion of citizens’ needs in city strategies: The case study of selected cities of Visegrad group countries. Cities 2019, 84, 159–171. [Google Scholar] [CrossRef]
- Kronenberg, J.; Haase, A.; Łszkiewicz, E.; Antal, A.; Baravikova, A.; Biernacka, M.; Dushkova, D.; Filčak, R.; Haase, D.; Ignatieva, M.; et al. Environmental justice in the context of urban green space availability, accessibility, and attractiveness in postsocialist cities. Cities 2020, 106, 102862. [Google Scholar] [CrossRef]
- Carminati, M.; Sinha, G.R.; Mohdiwale, S.; Ullo, S.L. Miniaturized Pervasive Sensors for Indoor Health Monitoring in Smart Cities. Smart Cities 2021, 4, 8. [Google Scholar] [CrossRef]
- Allam, Z.; Jones, D.S. On the Coronavirus (COVID-19) Outbreak and the Smart City Network: Universal Data Sharing Standards Coupled with Artificial Intelligence (AI) to Benefit Urban Health Monitoring and Management. Healthcare 2020, 8, 46. [Google Scholar] [CrossRef] [Green Version]
- Rathi, V.K.; Rajput, N.K.; Mishra, S.; Grover, B.A.; Tiwari, P.; Jaiswal, A.K.; Hossain, M.S. An edge AI-enabled IoT healthcare monitoring system for smart cities. Comput. Electr. Eng. 2021, 96, 107524. [Google Scholar] [CrossRef]
- Ghazal, T.M.; Hasan, M.K.; Alshurideh, M.T.; Alzoubi, H.M.; Ahmad, M.; Akbar, S.S.; Al Kurdi, B.; Akour, I.A. IoT for Smart Cities: Machine Learning Approaches in Smart Healthcare—A Review. Future Internet 2021, 13, 218. [Google Scholar] [CrossRef]
- Pramanik, M.I.; Lau, R.; Demirkan, H.; Azad, A.K. Smart health: Big data enabled health paradigm within smart cities. Expert Syst. Appl. 2017, 87, 370–383. [Google Scholar] [CrossRef]
- Poongodi, M.; Sharma, A.; Hamdi, M.; Maode, M.; Chilamkurti, N. Smart healthcare in smart cities: Wireless patient monitoring system using IoT. J. Supercomput. 2021, 77, 12230–12255. [Google Scholar] [CrossRef]
- Sanghavi, J. Review of Smart Healthcare Systems and Applications for Smart Cities. In ICCCE 2019; Kumar, A., Mozar, S., Eds.; Lecture Notes in Electrical Engineering; Springer: Singapore, 2019; Volume 570. [Google Scholar] [CrossRef]
- Hossain, M.S.; Muhammad, G.; Alamri, A. Smart healthcare monitoring: A voice pathology detection paradigm for smart cities. Multimed. Syst. 2019, 25, 565–575. [Google Scholar] [CrossRef]
- Ali, Z.; Muhammad, G.; Alhamid, M.F. An Automatic Health Monitoring System for Patients Suffering From Voice Complications in Smart Cities. IEEE Access 2017, 5, 3900–3908. [Google Scholar] [CrossRef]
- Tseng, K.C.; Hsu, C.L.; Chuang, Y.H. Designing an Intelligent Health Monitoring System and Exploring User Acceptance for the Elderly. J. Med. Syst. 2013, 37, 9967. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Rho, M.J. Perception of Influencing Factors on Acceptance of Mobile Health Monitoring Service: A Comparison between Users and Non-users. Healthc. Inform. Res. 2013, 19, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Haluza, D.; Jungwirth, D. ICT and the future of healthcare: Aspects of pervasive health monitoring. Inform. Health Soc. Care 2018, 43, 1–11. [Google Scholar] [CrossRef]
- Ashton, J. The Healthy Cities Project: A Challenge for Health Education. Health Educ. Q. 1991, 18, 39–48. [Google Scholar] [CrossRef]
- Goldstein, G. Healthy Cities: Overview of a WHO International Program. In Healthy Cities. Research and Practice; Davies, J.K., Ed.; Michael Kelly Routledge: London, UK, 2013. [Google Scholar] [CrossRef]
- Flynn, B.C.; Ray, D.W.; Rider, M.S. Empowering Communities: Action Research through Healthy Cities. Health Educ. Q. 1994, 21, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Kegler, M.C.; Twiss, J.M.; Look, V. Assessing Community Change at Multiple Levels: The Genesis of an Evaluation Framework for the California Healthy Cities Project. Health Educ. Behav. 2000, 27, 760–779. [Google Scholar] [CrossRef] [PubMed]
- Adams, L. Healthy cities, healthy participation. Health Educ. J. 1989, 48, 179–182. [Google Scholar] [CrossRef]
- Rocha, N.P.; Dias, A.; Santinha, G.; Rodrigues, M.; Queirós, A.; Rodrigues, C. Smart Cities and Public Health: A Systematic Review. Procedia Comput. Sci. 2019, 164, 516–523. [Google Scholar] [CrossRef]
- Trencher, G.; Karvonen, A. Stretching ‘smart’: Advancing health and well-being through the Smart City agenda. Local Environ. 2017, 24, 610–627. [Google Scholar] [CrossRef]
- Casino, F.; Patsakis, C.; Batista, E.; Borràs, E.; Martínez-Balleste, A. Healthy routes in the Smart City: A context-aware mobile recommender. IEEE Softw. 2017, 34, 42–47. [Google Scholar] [CrossRef]
- Yu, L.; Tao, S.; Gao, W.; Zhang, G.; Lin, K. Intelligent Farm Relaxation for Smart City based on Internet of Things: Management System and Service Model. Local Environ. 2016, 24, 610–627. [Google Scholar] [CrossRef]
- Hussain, S.A.; Ramaiah, C.S.; Prasad, M.N.G.; Hussain, S.M. Milk products monitoring system with arm processor for early detection of microbial activity. In Proceedings of the 2016 3rd MEC International Conference on Big Data and Smart City (ICBDSC), Muscat, Oman, 15–16 March 2016. [Google Scholar]
- Hamadeh, S. Roadmap for Future Food Systems and Smart Cities: Making the Ecosystem Contentious and Policies. In Sustainable Energy-Water-Environment Nexus in Deserts; Heggy, E., Bermudez, V., Vermeersch, M., Eds.; Advances in Science, Technology & Innovation; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Scherer, C.; Holm, P. FoodSmart City Dublin: A Framework for Sustainable Seafood. Food Ethics 2020, 5, 7. [Google Scholar] [CrossRef]
- Wang, Z. Research on Smart City Environment Design and Planning Based on Internet of Things. J. Sens. 2022, 2022, 2348573. [Google Scholar] [CrossRef]
- Oueida, S.; Aloqaily, M.; Ionescu, S. A smart healthcare reward model for resource allocation in Smart City. Multimed. Tools Appl. 2019, 78, 24573–24594. [Google Scholar] [CrossRef]
- Chauhan, A.; Jakhar, S.K.; Chauhan, C. The interplay of circular economy with industry 4.0 enabled Smart City drivers of healthcare waste disposal. J. Clean. Prod. 2021, 279, 123854. [Google Scholar] [CrossRef]
- Xue, K.; Yu, K.; Zhang, H.; Liang, X. Research on health promotion strategies of public recreation space in the coastal area of Qingdao City Center, China. Sustain. Energy Technol. Assess. 2022, 52, 102144. [Google Scholar] [CrossRef]
- Ramaiah, M.; Avtar, R. Urban Green Spaces and Their Need in Cities of Rapidly Urbanizing India: A Review. Urban Sci. 2019, 3, 94. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Zhang, Y.; Qian, P. The Effect of Innovation-Driven Strategy on Green Economic Development in China—An Empirical Study of Smart Cities. Int. J. Environ. Res. Public Health 2019, 16, 1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almalki, F.A.; Alsamhi, S.H.; Sahal, R.; Hasan, J.; Hawbani, A.; Rajput, S.; Saif, A.; Morgan, J.; Breslin, J. Green IoT for Eco-Friendly and Sustainable Smart Cities: Future Directions and Opportunities. Mob. Netw. Appl. 2021. [Google Scholar] [CrossRef]
- Sharma, P.K.; Kumar, N.; Park, J.H. Blockchain Technology Toward Green IoT: Opportunities and Challenges. IEEE Netw. 2020, 34, 263–269. [Google Scholar] [CrossRef]
- Varjovi, A.E.; Babaie, S. Green Internet of Things (GIoT): Vision, applications and research challenges. Sustain. Comput. Inform. Syst. 2020, 28, 100448. [Google Scholar] [CrossRef]
- Sarkar, S.; Debnath, A. Green IoT: Design Goals, Challenges and Energy Solutions. In Proceedings of the 2021 6th International Conference on Communication and Electronics Systems (ICCES), Coimbatre, India, 8–10 July 2021; pp. 637–642. [Google Scholar] [CrossRef]
- Maalsen, S. ‘We’re the cheap smart home’: The actually existing smart home as rented and shared. Soc. Cult. Geogr. 2022, 1–20. [Google Scholar] [CrossRef]
- Maalsen, S.; Wolifson, P.; Dowling, R. Gender in the Australian innovation ecosystem: Planning smart cities for men, Gender. Place Cult. 2023, 30, 299–320. [Google Scholar] [CrossRef]
- Rakhimova, N.; McAslan, D.; Pijawka, D. Measuring child-friendly cities: Developing and piloting an indicator assessment tool for sustainable neighborhood planning. J. Urban. Int. Res. Placemak. Urban Sustain. 2022, 1–27. [Google Scholar] [CrossRef]
- Tironi, M.; Valderrama, M. Worth-making in a datafied world: Urban cycling, smart urbanism, and technologies of justification in Santiago de Chile. Inf. Soc. 2022, 38, 100–116. [Google Scholar] [CrossRef]
- Quitzow, L. Smart grids, smart households, smart neighborhoods—Contested narratives of prosumage and decentralization in Berlin’s urban Energiewende, Innovation. Eur. J. Soc. Sci. Res. 2022, 36, 107–122. [Google Scholar] [CrossRef]
- Chatterjee, I. Marx’s “Species Being” as an Ontological Revolution Against the “Green City/Global City” Agenda: Two Possible Moments of Reclaiming “Species Life”. Capital. Nat. Social. 2023. [Google Scholar] [CrossRef]
- Antenucci, I.; Tomasello, F. Three shades of ‘urban-digital citizenship’: Borders, speculation, and logistics in Cape Town. Citizsh. Stud. 2022. [Google Scholar] [CrossRef]
- Jirón, P.; Imilan, W.; Osterling, E. Evangelists of the urban future. A decolonial critique of the smart city narrative in Santiago de Chile. City 2022, 26, 664–683. [Google Scholar] [CrossRef]
- Rosol, M.; Blue, G. From the smart city to urban justice in a digital age. City 2022, 26, 684–705. [Google Scholar] [CrossRef]
- Zhou, Y.; Xiao, F.; Deng, W. Is smart city a slogan? Evidence from China. Asian Geogr. 2022. [Google Scholar] [CrossRef]


{kind=link}
| Research Area | Survey Questions |
|---|---|
| Please Rate the Extent to Which the Activities Listed below Have Been Implemented by the City Government over the Past 5 Years. | |
| (1) monitoring the health needs of residents | 1. monitor the identified health needs of the population |
| (2) health education | 2. run information and education activities for residents targeting health promotion, prevention and creation of conditions conducive to health, based on direct contact, e.g., thematic meetings with experts; 3. run information and education activities for residents targeting health promotion, prevention and creation of conditions conducive to health, based on indirect contact, e.g., using mass media; 4. organize thematic sports events for residents to promote a healthy lifestyle, e.g., a run, a match |
| (3) healthcare infrastructure | 5. with the city’s funds, implement investments in the infrastructure of medical entities, e.g., purchase of new equipment, renovation of the building |
| (4) preventive healthcare | 6. organize prevention programs for city residents, e.g., on addictions and mental problems 7. organize hygienic and medical care for children and teenage students 8. organize and carry out immunizations for residents |
| (5) environment and recreation | 9. establish new green zones in the city, such as squares and parks 10. reduce air pollution 11. create an outdoor gym in the city 12. build publicly accessible sports facilities in the city, e.g., soccer fields |
| Research Area | Survey Questions | |||||
|---|---|---|---|---|---|---|
| Please Rate the Extent to Which the Activities Listed below Have Been Implemented by the City Government over the Past 5 Years. | Average | Dominant | Median | Stan. Deviation | Variation Coefficient | |
| (1) monitoring the health needs of residents | 1. monitor the identified health needs of the population | 3.24 | 4.00 | 3.00 | 1.05 | 32.28% |
| (2) health education | 2. run information and education activities for residents targeting health promotion, prevention and creation of conditions conducive to health, based on direct contact, e.g., thematic meetings with experts; | 3.83 | 4.00 | 4.00 | 1.05 | 27.27% |
| 3. run information and education activities for residents targeting health promotion, prevention and creation of conditions conducive to health, based on indirect contact, e.g., using mass media; | 3.73 | 4.00 | 4.00 | 1.02 | 27.02% | |
| 4. organize thematic sports events for residents to promote a healthy lifestyle, e.g., a run, a match | 4.14 | 5.00 | 4.00 | 1.04 | 25.14% | |
| (3) healthcare infrastructure | 5. with the city’s funds, implement investments in the infrastructure of medical entities, e.g., purchase of new equipment, renovation of the building | 3.62 | 5.00 | 4.00 | 1.28 | 35.32% |
| (4) preventive healthcare | 6. organize prevention programs for city residents, e.g., on addictions and mental problems | 4.22 | 5.00 | 4.00 | 0.91 | 21.56% |
| 7. organize hygienic and medical care for children and teenage students | 3.98 | 4.00 | 4.00 | 0.94 | 23.71% | |
| 8. organize and carry out immunizations for residents | 4.04 | 5.00 | 5.00 | 1.02 | 24.22% | |
| (5) environment and recreation | 9. establish new green zones in the city, such as squares and parks | 4.02 | 4.00 | 4.00 | 1.04 | 25.85% |
| 10. reduce air pollution | 3.91 | 4.00 | 4.00 | 0.93% | 23.66% | |
| 11. create an outdoor gym in the city | 4.45 | 5.00 | 5.00 | 0.84 | 18.84% | |
| 12. build publicly accessible sports facilities in the city, e.g., soccer fields | 4.23 | 5.00 | 5.00 | 1.02 | 24.22% |
| Research Area | Survey Questions | Interdependencies Surveyed | |
|---|---|---|---|
| Please Rate the Extent to Which the Activities Listed below Have Been Implemented by the City Government over the Past 5 Years. | (1) Monitoring of Health Needs—Healthcare Activities | (2) Size of the City—Healthcare Activities | |
| (1) monitoring the health needs of residents | 1. monitor the identified health needs of the population | 1.0000 * | 0.0761 |
| (2) health education | 2. run information and education activities for residents targeting health promotion, prevention and creation of conditions conducive to health, based on direct contact, e.g., thematic meetings with experts; | 0.3960 * | 0.1846 * |
| 3. run information and education activities for residents targeting health promotion, prevention and creation of conditions conducive to health, based on indirect contact, e.g., using mass media; | 0.4181 * | 0.2379 * | |
| 4. organize thematic sports events for residents to promote a healthy lifestyle, e.g., a run, a match | 0.3225 * | 0.2225 * | |
| (3) healthcare infrastructure | 5. with the city’s funds, implement investments in the infrastructure of medical entities, e.g., purchase of new equipment, renovation of the building | 0.3147 * | 0.1865 * |
| (4) preventive healthcare | 6. organize prevention programs for city residents, e.g., on addictions and mental problems | 0.3108 * | 0.1166 |
| 7. organize hygienic and medical care for children and teenage students | 0.3531 * | 0.1786 * | |
| 8. organize and carry out immunizations for residents | 0.4001 * | 0.1452 * | |
| (5) environment and recreation | 9. establish new green zones in the city, such as squares and parks | 0.2658 * | 0.3225 * |
| 10. reduce air pollution | 0.3006 * | 0.1706 * | |
| 11. create an outdoor gym in the city | 0.2056 * | 0.2182 * | |
| 12. build publicly accessible sports facilities in the city, e.g., soccer fields | 0.2599 * | 0.1545 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wielicka-Gańczarczyk, K.; Jonek-Kowalska, I. Involvement of Local Authorities in the Protection of Residents’ Health in the Light of the Smart City Concept on the Example of Polish Cities. Smart Cities 2023, 6, 744-763. https://doi.org/10.3390/smartcities6020036
Wielicka-Gańczarczyk K, Jonek-Kowalska I. Involvement of Local Authorities in the Protection of Residents’ Health in the Light of the Smart City Concept on the Example of Polish Cities. Smart Cities. 2023; 6(2):744-763. https://doi.org/10.3390/smartcities6020036
Chicago/Turabian StyleWielicka-Gańczarczyk, Karolina, and Izabela Jonek-Kowalska. 2023. "Involvement of Local Authorities in the Protection of Residents’ Health in the Light of the Smart City Concept on the Example of Polish Cities" Smart Cities 6, no. 2: 744-763. https://doi.org/10.3390/smartcities6020036