

Interstitial Lung Disease Is Associated with Sleep Disorders in Rheumatoid Arthritis Patients

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. General Characteristics of the Study Population
2.2. Characteristic of Sleep, Psychological Factors, and Quality of Life
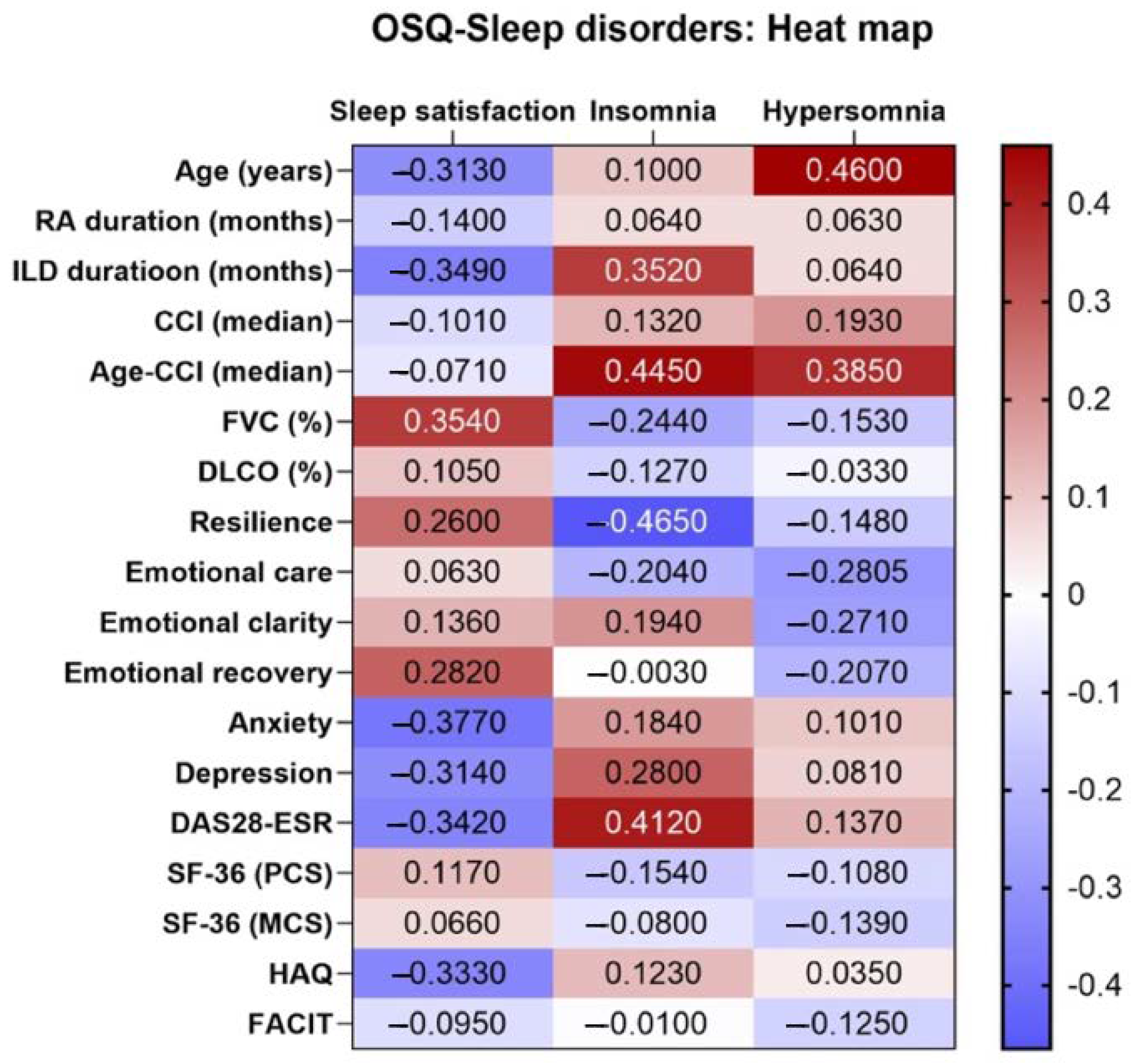
2.3. Correlations between Sleep and Clinical and Psychological Characteristics in Cases and Controls
2.4. Multivariate Analysis
3. Discussion
4. Materials and Methods
4.1. Design and Data Source
4.1.1. Cases
4.1.2. Controls
4.2. Study Protocol
4.3. Outcome Measures and Definitions
4.3.1. Variables: Sleep, Psychosocial Factors, and Physical Functioning
4.3.2. Variables Associated with Interstitial Lung Disease
4.3.3. Other Variables
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Silva-Fernández, L.; Macía-Villa, C.; Seoane-Mato, D.; Cortés-Verdú, R.; Romero-Pérez, A.; Quevedo-Vila, V.; Fábregas-Canales, D.; Antón-Pagés, F.; Añez, G.; Brandy, A.; et al. The prevalence of rheumatoid arthritis in Spain. Sci. Rep. 2020, 10, 21551. [Google Scholar] [CrossRef] [PubMed]
- Mena-Vázquez, N.; Ruiz-Limón, P.; Moreno-Indias, I.; Manrique-Arija, S.; Tinahones, F.J.; Fernández-Nebro, A. Expansion of Rare and Harmful Lineages is Associated with Established Rheumatoid Arthritis. J. Clin. Med. 2020, 9 Pt 1, 1044. [Google Scholar] [CrossRef] [PubMed]
- Gabbay, E.; Tarala, R.; Will, R.; Carroll, G.; Adler, B.; Cameron, D.; Lake, F.R. Interstitial lung disease in recent onset rheumatoid arthritis. Am. J. Respir. Crit. Care Med. 1997, 156 Pt 1, 528–535. [Google Scholar] [CrossRef]
- Rodríguez Portal, J.A.; Brito García, N.; Díaz Del Campo Fontecha, P.; Valenzuela, C.; Ortiz, A.M.; Nieto, M.A.; Mena-Vázquez, N.; Cano-Jiménez, E.; Castellví, I.; Aburto, M.; et al. SER-SEPAR recommendations for the management of rheumatoid arthritis-related interstitial lung disease. Part 1: Epidemiology, risk factors and prognosis. Reumatol. Clin. 2022, 18, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Mena-Vázquez, N.; Rojas-Gimenez, M.; Romero-Barco, C.M.; Gandía-Martínez, M.; Perez-Gómez, N.; Godoy-Navarrete, F.J.; Manrique-Arija, S.; Garcia-Studer, A.; Calvo-Gutiérrez, J.; Varela, C.F.; et al. Analysis of comorbidity in rheumatoid arthritis-associated interstitial lung disease: A nested case-cohort study. Biomed. Pharmacother. 2023, 157, 114049. [Google Scholar] [CrossRef]
- Purabdollah, M.; Lakdizaji, S.; Rahmani, A.; Hajalilu, M.; Ansarin, K. Relationship between Sleep Disorders, Pain and Quality of Life in Patients with Rheumatoid Arthritis. J. Caring Sci. 2015, 4, 233–241. [Google Scholar] [CrossRef]
- Katz, P.; Pedro, S.; Michaud, K. Sleep Disorders Among Individuals With Rheumatoid Arthritis. Arthritis Care Res. 2022, 75, 1250–1260. [Google Scholar] [CrossRef]
- Brionez, T.F.; Assassi, S.; Reveille, J.D.; Learch, T.J.; Diekman, L.; Ward, M.M.; Davis, J.C.J.; Weisman, M.H.; Nicassio, P. Psychological correlates of self-reported functional limitation in patients with ankylosing spondylitis. Arthritis Res. Ther. 2009, 11, R182. [Google Scholar] [CrossRef]
- Hörnberg, K.; Pomeroy, J.; Sandberg, C.; Ångström, L.; Södergren, A.; Sundström, B. Isotemporal Substitution of Time Between Sleep and Physical Activity: Associations With Cardiovascular Risk Factors in Early Rheumatoid Arthritis. ACR Open Rheumatol. 2021, 3, 138–146. [Google Scholar] [CrossRef]
- Spira, A.P.; Stone, K.L.; Redline, S.; Ensrud, K.E.; Ancoli-Israel, S.; Cauley, J.A.; Yaffe, K. Actigraphic Sleep Duration and Fragmentation in Older Women: Associations With Performance Across Cognitive Domains. Sleep 2017, 40, zsx073. [Google Scholar] [CrossRef]
- Irwin, M.R.; Opp, M.R. Sleep Health: Reciprocal Regulation of Sleep and Innate Immunity. Neuropsychopharmacology 2017, 42, 129–155. [Google Scholar] [CrossRef] [PubMed]
- Deniz, O.; Cavusoglu, C.; Satis, H.; Salman, R.B.; Varan, O.; Atas, N.; Coteli, S.; Dogrul, R.T.; Babaoglu, H.; Oncul, A.; et al. Sleep quality and its associations with disease activity and quality of life in older patients with rheumatoid arthritis. Eur. Geriatr. Med. 2023, 14, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.-G.; Teoh, A.; Roberts, M.; Wheatley, J. The prevalence of poor sleep quality and its associated factors in patients with interstitial lung disease: A cross-sectional analysis. ERJ Open Res. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Dockray, S.; Wardle, J. Positive affect and psychobiological processes relevant to health. J. Personal. 2009, 77, 1747–1776. [Google Scholar] [CrossRef]
- Liu, L.; Xu, X.; Xu, N.; Wang, L. Disease activity, resilience and health-related quality of life in Chinese patients with rheumatoid arthritis: A multi-center, cross-sectional study. Health Qual. Life Outcomes 2017, 15, 149. [Google Scholar] [CrossRef] [PubMed]
- Cano-García, L.; Mena-Vázquez, N.; Manrique-Arija, S.; Redondo-Rodriguez, R.; Romero-Barco, C.M.; Fernández-Nebro, A. Ability to Participate in Social Activities of Rheumatoid Arthritis Patients Compared with Other Rheumatic Diseases: A Cross-Sectional Observational Study. Diagnostics 2021, 11, 2258. [Google Scholar] [CrossRef]
- Cano-García, L.; Mena-Vázquez, N.; Manrique Arija, S.; Hernández-Sánchez, M.D.; Segura-Ruiz, R.; Domínguez-Quesada, C.; Fernández-Nebro, A. Psychological factors associated with sleep disorders in patients with axial spondyloarthritis or psoriatic arthritis: A multicenter cross-sectional observational study. J. Clin. Nurs. 2021, 30, 266–275. [Google Scholar] [CrossRef]
- Kim, K.W.; Kang, S.-H.; Yoon, I.-Y.; Lee, S.D.; Ju, G.; Han, J.W.; Kim, T.H.; Lee, C.S.; Kim, T. Prevalence and clinical characteristics of insomnia and its subtypes in the Korean elderly. Arch. Gerontol. Geriatr. 2017, 68, 68–75. [Google Scholar] [CrossRef]
- Ford, E.S.; Cunningham, T.J.; Giles, W.H.; Croft, J.B. Trends in insomnia and excessive daytime sleepiness among U.S. adults from 2002 to 2012. Sleep Med. 2015, 16, 372–378. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hays, R.D.; Martin, S.A.; Sesti, A.M.; Spritzer, K.L. Psychometric properties of the Medical Outcomes Study Sleep measure. Sleep Med. 2005, 6, 41–44. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; de la Coba, P.; Duschek, S.; Reyes Del Paso, G.A. Reliability, Factor Structure and Predictive Validity of the Widespread Pain Index and Symptom Severity Scales of the 2010 American College of Rheumatology Criteria of Fibromyalgia. J. Clin. Med. 2020, 9, 2460. [Google Scholar] [CrossRef] [PubMed]
- Paz García-Portilla, M.; Sáiz, P.A.; Díaz-Mesa, E.M.; Fonseca, E.; Arrojo, M.; Sierra, P.; Sarramea, F.; Sánchez, E.; Goikole, J.M.; Balanzá, V.; et al. Psychometric performance of the Oviedo Sleep Questionnaire in patients with severe mental disorder. Rev. Psiquiatr. Salud Ment. 2009, 2, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Valiensi, S.M.; Belardo, M.A.; Pilnik, S.; Izbizky, G.; Starvaggi, A.P.; Castelo Branco, C. Sleep quality and related factors in postmenopausal women. Maturitas 2019, 123, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Myall, K.J.; West, A.; Kent, B.D. Sleep and interstitial lung disease. Curr. Opin. Pulm. Med. 2019, 25, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Mavroudi, M.; Papakosta, D.; Kontakiotis, T.; Domvri, K.; Kalamaras, G.; Zarogoulidou, V.; Zarogoulidis, P.; Latka, P.; Huang, H.; Hohenforst-Schmidt, W.; et al. Sleep disorders and health-related quality of life in patients with interstitial lung disease. Sleep Breath. 2018, 22, 393–400. [Google Scholar] [CrossRef]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Wang, M.; Campomayor, C.O.; Collado-Hidalgo, A.; Cole, S. Sleep deprivation and activation of morning levels of cellular and genomic markers of inflammation. Arch. Intern. Med. 2006, 166, 1756–1762. [Google Scholar] [CrossRef]
- Stone, K.L.; Blackwell, T.L.; Ancoli-Israel, S.; Barrett-Connor, E.; Bauer, D.C.; Cauley, J.A.; Ensrud, K.E.; Hoffman, A.R.; Mehra, R.; Stefanick, M.L.; et al. Sleep Disordered Breathing and Risk of Stroke in Older Community-Dwelling Men. Sleep 2016, 39, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Gulia, K.K.; Kumar, V.M. Sleep disorders in the elderly: A growing challenge. Psychogeriatrics 2018, 18, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Moraes, W.; Piovezan, R.; Poyares, D.; Bittencourt, L.R.; Santos-Silva, R.; Tufik, S. Effects of aging on sleep structure throughout adulthood: A population-based study. Sleep Med. 2014, 15, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Redline, S.; Kirchner, H.L.; Quan, S.F.; Gottlieb, D.J.; Kapur, V.; Newman, A. The effects of age, sex, ethnicity, and sleep-disordered breathing on sleep architecture. Arch. Intern. Med. 2004, 164, 406–418. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, R.M.; van Munster, B.C.; van Kempen, M.F.; de Rooij, S.E.J.A. Physiological melatonin levels in healthy older people: A systematic review. J. Psychosom. Res. 2016, 86, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.M.; Williams, W.P., 3rd; Kriegsfeld, L.J. Aging in the circadian system: Considerations for health, disease prevention and longevity. Exp. Gerontol. 2009, 44, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Mattis, J.; Sehgal, A. Circadian Rhythms, Sleep, and Disorders of Aging. Trends Endocrinol. Metab. 2016, 27, 192–203. [Google Scholar] [CrossRef]
- Cohen, Z.L.; Eigenberger, P.M.; Sharkey, K.M.; Conroy, M.L.; Wilkins, K.M. Insomnia and Other Sleep Disorders in Older Adults. Psychiatr. Clin. N. Am. 2022, 45, 717–734. [Google Scholar] [CrossRef]
- Stainer, A.; Tonutti, A.; De Santis, M.; Amati, F.; Ceribelli, A.; Bongiovanni, G.; Torrisi, C.; Iacopino, A.; Mangiameli, G.; Aliberti, S.; et al. Unmet needs and perspectives in rheumatoid arthritis-associated interstitial lung disease: A critical review. Front. Med. 2023, 10, 1129939. [Google Scholar] [CrossRef]
- Song, J.W.; Lee, H.-K.; Lee, C.K.; Chae, E.J.; Jang, S.J.; Colby, T.V.; Kim, D.S. Clinical course and outcome of rheumatoid arthritis-related usual interstitial pneumonia. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 2013, 30, 103–112. [Google Scholar]
- Palagini, L.; Moretto, U.; Novi, M.; Masci, I.; Caruso, D.; Drake, C.L.; Riemann, D. Lack of Resilience Is Related to Stress-Related Sleep Reactivity, Hyperarousal, and Emotion Dysregulation in Insomnia Disorder. J. Clin. Sleep Med. 2018, 14, 759–766. [Google Scholar] [CrossRef]
- Baglioni, C.; Spiegelhalder, K.; Lombardo, C.; Riemann, D. Sleep and emotions: A focus on insomnia. Sleep Med. Rev. 2010, 14, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Implementation of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). Epidemiol. Bull. 1997, 18, 1–4.
- Vilca-Pareja, V.; Luque Ruiz de Somocurcio, A.; Delgado-Morales, R.; Medina Zeballos, L. Emotional Intelligence, Resilience, and Self-Esteem as Predictors of Satisfaction with Life in University Students. Int. J. Environ. Res. Public Health 2022, 19, 16548. [Google Scholar] [CrossRef] [PubMed]
- Arrayás-Grajera, M.J.; Tornero-Quiñones, I.; Gavilán-Carrera, B.; Luque-Reca, O.; Peñacoba-Puente, C.; Sierra-Robles, Á.; Carbonell-Baeza, A.; Estévez-López, F. Fibromyalgia: Evidence for Deficits in Positive Psychology Resources. A Case-Control Study from the Al-Ándalus Project. Int. J. Environ. Res. Public Health 2021, 18, 12021. [Google Scholar] [CrossRef]
- Fernandez-Berrocal, P.; Extremera, N.; Ramos, N. Validity and reliability of the Spanish modified version of the Trait Meta-Mood Scale. Psychol. Rep. 2004, 94 Pt 1, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Covic, T.; Cumming, S.R.; Pallant, J.F.; Manolios, N.; Emery, P.; Conaghan, P.G.; Tennant, A. Depression and anxiety in patients with rheumatoid arthritis: Prevalence rates based on a comparison of the Depression, Anxiety and Stress Scale (DASS) and the hospital, Anxiety and Depression Scale (HADS). BMC Psychiatry 2012, 12, 6. [Google Scholar] [CrossRef]
- Covic, T.; Pallant, J.F.; Tennant, A.; Cox, S.; Emery, P.; Conaghan, P.G. Variability in depression prevalence in early rheumatoid arthritis: A comparison of the CES-D and HAD-D Scales. BMC Musculoskelet. Disord. 2009, 10, 18. [Google Scholar] [CrossRef]
- Matcham, F.; Rayner, L.; Steer, S.; Hotopf, M. The prevalence of depression in rheumatoid arthritis: A systematic review and meta-analysis. Rheumatology 2013, 52, 2136–2148. [Google Scholar] [CrossRef]
- Esteve-Vives, J.; Batlle-Gualda, E.; Reig, A. Spanish version of the Health Assessment Questionnaire: Reliability, validity and transcultural equivalency. Grupo para la Adaptación del HAQ a la Población Española. J. Rheumatol. 1993, 20, 2116–2122. [Google Scholar]
- Kozłowska, K.A.; Formanowicz, D.; Bączyk, G. The Link between the Demographic and Clinical Factors and Fatigue Symptoms among Rheumatoid Arthritis Patients. Int. J. Environ. Res. Public Health 2022, 19, 14681. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E.J.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Narváez, J.; Díaz Del Campo Fontecha, P.; Brito García, N.; Bonilla, G.; Aburto, M.; Castellví, I.; Cano-Jiménez, E.; Mena-Vázquez, N.; Nieto, M.A.; Ortiz, A.M.; et al. SER-SEPAR recommendations for the management of rheumatoid arthritis-related interstitial lung disease. Part 2: Treatment. Reumatol. Clin. 2022, 18, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Gil-Bona, J.; Sabaté, A.; Miguelena Bovadilla, J.M.; Adroer, R.; Koo, M.; Jaurrieta, E. Charlson index and the surgical risk scale in the analysis of surgical mortality. Cir. Esp. 2010, 88, 174–179. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]


{kind=link}
| Variable | RA-ILD N = 35 | RA without ILD N = 35 | p-Value |
|---|---|---|---|
| Clinical characteristics | |||
| Age, years, mean (SD) | 69.7 (9.3) | 66.6 (7.0) | 0.130 |
| Age >60 years, n (%) | 27 (77.1) | 29 (82.9) | 0.550 |
| Male sex; n (%) | 20 (57.1) | 20 (57.1) | 1.000 |
| Duration of RA, months, median (IQR) | 149.8 (93.3–245.5) | 133.7 (67.8–204.2) | 0.384 |
| Duration of ILD, months, mean (SD) | 66.1 (47.2) | - | - |
| RF+ (>10), n (%) | 33 (94.3) | 31 (88.6) | 0.393 |
| High RF (>60), n (%) | 24 (68.6) | 17 (48.6) | 0.089 |
| ACPA+ (>20), n (%) | 32 (91.4) | 31 (88.6) | 0.690 |
| Radiographic erosions, n (%) | 21 (60.0) | 19 (55.6) | 0.705 |
| Comorbid conditions | |||
| Smoking history | 0.760 | ||
| Nonsmokers, n (%) | 17 (48.6) | 18 (51.4) | |
| Ex-smokers, n (%) | 10 (28.6) | 8 (22.9) | |
| Active smokers, n (%) | 8 (22.9) | 9 (25.7) | |
| Dyslipidemia, n (%) | 13 (37.1) | 12 (53.3) | 0.873 |
| Sleep apnea, n (%) | 4 (11.4) | 3 (8.6) | 0.690 |
| Arterial hypertension, n (%) | 19 (54.3) | 13 (37.1) | 0.150 |
| Obesity (BMI > 30), n (%) | 6 (17.1) | 6 (17.1) | 1.000 |
| Diabetes mellitus, n (%) | 7 (20.0) | 6 (17.1) | 0.759 |
| CCI, median (IQR) | 2.0 (1.0–3.0) | 1.0 (1.0–2.0) | 0.099 |
| Age-CCI, median (IQR) | 4.0 (3.0–5.0) | 3.0 (3.0–5.0) | 0.042 |
| Treatment | |||
| csDMARDs, n (%) | 28 (80.0) | 33 (94.3) | 0.074 |
| Methotrexate, n (%) | 19 (54.3) | 27 (77.1) | 0.040 |
| Leflunomide, n (%) | 3 (8.6) | 6 (17.1) | 0.284 |
| Sulfasalazine, n (%) | 2 (5.7) | 2 (5.7) | 1.000 |
| Hydroxychloroquine, n (%) | 6 (17.1) | 0 (0.0) | 0.010 |
| Mycophenolate, n (%) | 4 (11.4) | 0 (0.0) | 0.032 |
| bDMARDs, n (%) | 22 (62.9) | 18 (51.4) | 0.334 |
| Anti-TNF, n (%) | 4 (11.4) | 11 (31.4) | 0.041 |
| Tocilizumab, n (%) | 3 (8.6) | 2 (5.7) | 0.643 |
| Abatacept, n (%) | 13 (37.1) | 3 (8.6) | 0.004 |
| Rituximab, n (%) | 2 (5.7) | 0 (0.0) | 0.151 |
| JAK inhibitors, n (%) | 0 (0.0) | 2 (5.7) | 0.151 |
| Glucocorticoids, n (%) | 22 (62.9) | 6 (17.1) | 0.001 |
| Pulmonary function tests | |||
| FVC < 80%, n (%) | 28 (80.0) | 5 (14.3) | <0.001 |
| FVC predicted (%), mean (SD) | 63.0 (17.1) | 83.4 (4.4) | <0.001 |
| FEV1 < 80%, n (%) | 23 (67.6) | 5 (14.3) | 0.001 |
| FEV1 predicted (%), mean (SD) | 68.7 (15.9) | 84.0 (11.5) | <0.001 |
| DLCO <80%, n (%) | 29 (85.3) | 3 (8.6) | <0.001 |
| DLCO-SB predicted (%), mean (SD) | 61.0 (15.2) | 85.9 (7.9) | <0.001 |
| HRCT pattern | |||
| UIP, n (%) | 29 (82.9) | 0 (0.0) | <0.001 |
| NSIP, n (%) | 6 (17.1) | 0 (0.0) | <0.001 |
| Variable | RA-ILD N = 35 | RA without ILD N = 35 | p-Value |
|---|---|---|---|
| Sleep quality (OSQ) | |||
| Subjective satisfaction with sleep, mean (SD) | 3.5 (0.9) | 4.0 (0.8) | 0.033 |
| Severity of insomnia, mean (SD) | 17.9 (7.8) | 11.7 (4.8) | 0.001 |
| Insomnia ICD-10, n (%) | 15 (42.9) | 7 (20.0) | 0.039 |
| Hypersomnia, mean (SD) | 5.8 (2.3) | 4.4 (1.4) | 0.005 |
| Hypersomnia ICD-10 | 2 (5.7) | 1 (2.9) | 0.555 |
| Positive psychological factors | |||
| Resilience, mean (SD) | 97.1 (30.6) | 111.7 (22.8) | 0.027 |
| Emotional intelligence (TMMS-24) | |||
| Emotional attention, mean (SD) | 22.1 (6.8) | 23.8 (5.6) | 0.248 |
| Low, n (%) | 13 (37.1) | 9 (25.7) | 0.584 |
| Adequate, n (%) | 21 (60.0) | 25 (71.4) | 0.584 |
| High, n (%) | 1 (2.9) | 1 (2.9) | 0.584 |
| Emotional clarity, mean (SD) | 22.1 (7.5) | 24.6 (4.6) | 0.089 |
| Low, n (%) | 16 (45.7) | 6 (17.1) | 0.023 |
| Adequate, n (%) | 17 (48.6) | 28 (80.0) | 0.023 |
| High, n (%) | 2 (5.7) | 1 (2.9) | 0.023 |
| Emotional recovery, mean (SD) | 20.2 (8.3) | 25.3 (6.4) | 0.006 |
| Low, n (%) | 17 (48.6) | 3 (8.6) | 0.002 |
| Adequate, n (%) | 16 (45.7) | 28 (80.0) | 0.002 |
| High, n (%) | 2 (5.7) | 4 (11.4) | 0.002 |
| Mood disorders (HADS scale) | |||
| Anxiety, mean (SD) | 7.0 (4.0–9.0) | 3.0 (0.0–5.0) | 0.006 |
| Anxiety ≥11, n (%) | 8 (22.9) | 3 (8.6) | 0.101 |
| Depression, median (IQR) | 6.5 (3.0–9.5) | 3.0 (2.0–6.0) | 0.008 |
| Depression ≥11, n (%) | 10 (28.6) | 5 (14.3) | 0.145 |
| Inflammatory activity | |||
| DAS28-ESR, mean (SD) | 3.2 (1.1) | 2.8 (1.0) | 0.028 |
| Remission-low activity, n (%) | 66 (60.0) | 68 (66.7) | 0.315 |
| Moderate-high activity, n (%) | 44 (40.0) | 34 (33.3) | 0.315 |
| VAS pain, median (IQR) | 4.0 (3.0–6.0) | 4.0 (2.0–5.0) | 0.283 |
| VAS general patient, median (IQR) | 5.0 (3.0–6.0) | 3.0 (1.0–4.0) | 0.046 |
| Physical function | |||
| HAQ, median (IQR) | 1.2 (0.6) | 0.7 (0.6) | 0.003 |
| Fatigue | |||
| FACIT, median (IQR) | 21.6 (7.1) | 20.4 (6.6) | 0.461 |
| Quality of life | |||
| SF-36 PCS, mean (SD) | 30.4 (9.8) | 35.7 (10.9) | 0.032 |
| SF-36 MCS, median (IQR) | 37.6 (11.7) | 44.2 (12.8) | 0.038 |
| Predictor | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| B | 95% CI | B | 95% CI | p-Value | |
| Sleep satisfaction * | |||||
| Female sex | 0.308 | −0.134, 0.751 | |||
| Age > 60 years | −0.771 | −1.310, −0.231 | −0.730 | −1.223, −0.237 | 0.004 |
| ILD | −0.486 | −0.914, −0.058 | −0.408 | −0.814, −0.020 | 0.048 |
| Age-CCI | −0.162 | −0.288, −0.035 | |||
| DAS28-ESR | −0.326 | −0.544, −0.109 | −0.242 | −0.434, −0.030 | 0.026 |
| Resilience | 0.007 | −0.001, 0.015 | |||
| ER | 0.034 | 0.007, 0.062 | |||
| Depression | −0.077 | −0.127, −0.027 | |||
| Severity of insomnia ** | |||||
| Female sex | 0.392 | −3.101, 3.884 | |||
| Age > 60 years | −0.099 | −4.544, 4.347 | |||
| ILD | 6.257 | 3.148, 9.366 | 3.995 | 1.125, 6.865 | 0.007 |
| Age-CCI | 1.240 | 0.291, 2.430 | |||
| DAS28-ESR | 2.494 | 0.797, 4.192 | |||
| Resilience | −0.130 | −0.184, −0.076 | −0.109 | −0.160, −0.058 | <0.001 |
| ER | −0.138 | −0.357, 0.081 | |||
| Depression | 0.721 | 0.343, 1.099 | |||
| Hypersomnia *** | |||||
| Female sex | 0.417 | −0.584, 1.417 | |||
| Age > 60 years | 1.320 | 0.332, 2.308 | |||
| ILD | 1.400 | 0.465, 2.335 | 0.995 | 0.045, 1.945 | 0.040 |
| Age-CCI | 0.329 | 0.043, 0.615 | |||
| DAS28-ESR | 0.139 | −0.379, 0.656 | |||
| Resilience | −0.020 | −0.037, −0.003 | |||
| ER | −0.100 | −0.159, −0.042 | −0.080 | −0.141, −0.029 | 0.011 |
| Depression | 0.103 | −0.014, 0.220 | |||
| Predictor | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| B | 95% CI | B | 95% CI | p-Value | |
| Sleep satisfaction * | |||||
| Female sex | 0.150 | −0.496, 0.796 | |||
| Age > 60 years | −0.792 | −1.503, −0.081 | −0.817 | −1.458, −0.177 | 0.014 |
| Age-CCI | −0.054 | −0.228, 0.120 | |||
| FVC | 0.019 | 0.001, 0.037 | |||
| UIP pattern | −1.292 | −0.240, −2.343 | −1.419 | −2.344, −0.493 | 0.004 |
| DAS28-ESR | −0.334 | −0.659, −0.009 | −0.324 | −0.601, −0.046 | 0.024 |
| Resilience | 0.008 | −0.002, 0.018 | |||
| Depression | −0.057 | −0.133, 0.020 | |||
| Severity of insomnia ** | |||||
| Female sex | −1.583 | −7.065, 3.898 | |||
| Age > 60 years | 0.449 | −6.043, 6.491 | |||
| Age-CCI | 1.869 | 0.536, 3.202 | 1.584 | 0.499, 2.669 | 0.006 |
| FVC | −0.113 | −0.272, 0.046 | |||
| UIP pattern | 3.979 | −5.659, 10.618 | |||
| DAS28-ESR | 3.423 | 0.743, 6.103 | 2.436 | 1.321–5.194 | 0.041 |
| Resilience | −0.118 | −0.197, −0.038 | −0.114 | −0.179, −0.048 | 0.001 |
| Depression | 0.608 | −0.029, 1.244 | |||
| Hypersomnia *** | |||||
| Female sex | 0.650 | −0.988, 2.288 | |||
| Age > 60 years | 2.013 | 0.281, 3.745 | 2.208 | 0.423–3.994 | 0.017 |
| Age-CCI | 0.452 | 0.035, 0.869 | |||
| FVC | 0.007 | −0.042, 0.057 | |||
| UIP pattern | 2.000 | −0.837, 4.837 | |||
| DAS28-ESR | −0.342 | −1.216, 0.533 | |||
| Resilience | −0.004 | −0.031, 0.023 | |||
| Depression | −0.038 | −0.234, 0.169 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mena-Vázquez, N.; Redondo-Rodriguez, R.; Cabezudo-García, P.; Garcia-Studer, A.; Ortiz-Márquez, F.; Borregón-Garrido, P.; Martín-Valverde, M.; Ureña-Garnica, I.; Manrique-Arija, S.; Cano-García, L.; et al. Interstitial Lung Disease Is Associated with Sleep Disorders in Rheumatoid Arthritis Patients. Clocks & Sleep 2023, 5, 755-769. https://doi.org/10.3390/clockssleep5040049
Mena-Vázquez N, Redondo-Rodriguez R, Cabezudo-García P, Garcia-Studer A, Ortiz-Márquez F, Borregón-Garrido P, Martín-Valverde M, Ureña-Garnica I, Manrique-Arija S, Cano-García L, et al. Interstitial Lung Disease Is Associated with Sleep Disorders in Rheumatoid Arthritis Patients. Clocks & Sleep. 2023; 5(4):755-769. https://doi.org/10.3390/clockssleep5040049
Chicago/Turabian StyleMena-Vázquez, Natalia, Rocío Redondo-Rodriguez, Pablo Cabezudo-García, Aimara Garcia-Studer, Fernando Ortiz-Márquez, Paula Borregón-Garrido, Manuel Martín-Valverde, Inmaculada Ureña-Garnica, Sara Manrique-Arija, Laura Cano-García, and et al. 2023. "Interstitial Lung Disease Is Associated with Sleep Disorders in Rheumatoid Arthritis Patients" Clocks & Sleep 5, no. 4: 755-769. https://doi.org/10.3390/clockssleep5040049