
Suspected Hematuria: Adverse Effects of Rivaroxaban in Older Adult Treated for Atrial Fibrillation
 , and
, and
Abstract
:1. Introduction
- Performing a comprehensive medication review of prescribed drugs, nonprescription drugs (over-the-counter, OTC medication), dietary products, and medical devices for each indication;
- Selecting, initiating, modifying, or administering medication therapy;
- Providing verbal education and training designed to enhance patient understanding of the type and purpose of the prescribed drugs, OTC medication, dietary products, and medical devices, as well as education about the recommended dosage regimen, the time of administration, and, if so applicable, specific requirements (for example, taking medication at a specific time, taking medication with a meal or after fasting, the appropriate application of inhalation dosage forms, etc.), and other important recommendations;
- Providing information, support services, and resources designed to enhance patient adherence, such as education about the risks of irregular medication intake or the self-initiated discontinuation of therapy, as well as the monitoring of problems and/or difficulties related to therapy application;
- Monitoring and evaluating the safety of applied therapy, such as identifying, resolving, and preventing medication-related problems, including adverse drug events by controlling the risk of a cumulative effect caused by certain drugs and evaluating the significant contraindications, possible drug–drug, drug–food, or drug–disease/condition interactions, and/or adverse effects;
- Monitoring and evaluating patients’ response to therapy and effectiveness of the applied therapy, namely the control of the desired therapeutic outcomes;
- Documenting the pharmaceutical care provided for the patient and the pharmaceutical intervention that was undertaken, as well as communication with other healthcare providers.
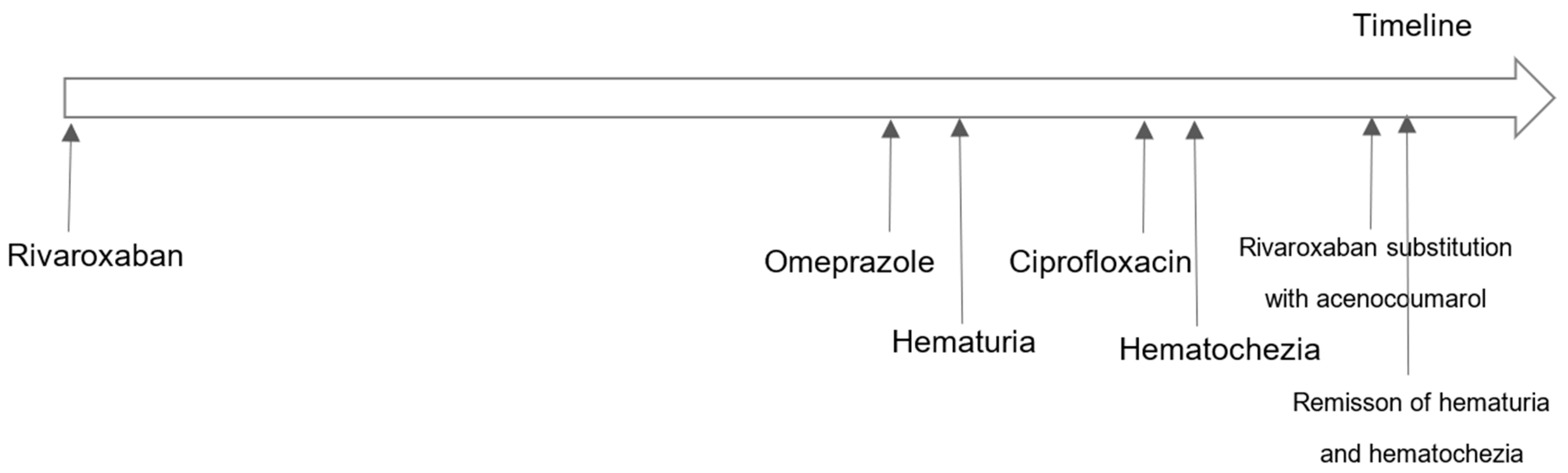
2. Detailed Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). WHO Launches Global Effort to Halve Medication-Related Errors in 5 Years. Available online: https://www.who.int/news/item/29-03-2017-who-launches-global-effort-to-halve-medication-related-errors-in-5-years (accessed on 12 December 2023).
- Ambwani, S.; Misra, A.K.; Kumar, R. Medication Errors: Is it the Hidden Part of the Submerged Iceberg in Our Health-care System? Int. J. Appl. Basic Med. Res. 2019, 9, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.J.; Pontefract, S.K. Adverse drug reactions. Clin. Med. 2016, 16, 481–485. [Google Scholar] [CrossRef]
- Hohl, C.M.; Small, S.S.; Peddie, D.; Badke, K.; Bailey, C.; Balka, E. Why Clinicians Don’t Report Adverse Drug Events: Qualitative Study. JMIR Public Health Surveill. 2018, 4, e21. [Google Scholar] [CrossRef]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef]
- Nickel, C.H.; Ruedinger, J.M.; Messmer, A.S.; Maile, S.; Peng, A.; Bodmer, M.; Kressig, R.W.; Kraehenbuehl, S.; Bingisser, R. Drug-related emergency department visits by elderly patients presenting with non-specific complaints. Scand. J. Trauma. Resusc. Emerg. Med. 2013, 21, 15. [Google Scholar] [CrossRef]
- Al-Taie, A. Implications of Health Care Providers by Physicians’ and Pharmacists’ Attitudes and Perceptive Barriers towards Interprofessional Collaborative Practices. Braz. J. Pharm. Sci. 2022, 58, e20983. [Google Scholar] [CrossRef]
- American Pharmacist Association (APA). ASHP Statement on the Role of Pharmacists in Primary Care. Available online: https://www.ashp.org/-/media/assets/policy-guidelines/docs/statements/pharmacists-role-primary-care.pdf (accessed on 12 December 2023).
- Folic, M.M.; Jankovic, S.M. Factors affecting outcome in hospitalized patients treated according to recommendations from clinical pharmacologists. Int. J. Clin. Pharmacol. Ther. 2023, 61, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Fernández, E.V.; Warriner, C.L.; David, T.; Gordon, E.; Twigg, G.; Carroll, N.V. Potential cost savings by prevention of adverse drug events with a novel medication review program. J. Am. Pharm. Assoc. 2020, 60, 462–469.e4. [Google Scholar] [CrossRef]
- Pharmaceutical Chamber of Serbia (PCS). Guideline of Good Apothecary Practice, 2021 [Farmaceutska Komora Srbije. Vodič Dobre Apotekarske Prakse]. Available online: https://api.pks.rs/storage/assets/%D0%92%D0%9E%D0%94%D0%98%D0%A7%20%D0%B4%D0%BE%D0%B1%D1%80%D0%B5%20%D0%B0%D0%BF%D0%BE%D1%82%D0%B5%D0%BA%D0%B0%D1%80%D1%81%D0%BA%D0%B5%20%D0%BF%D1%80%D0%B0%D0%BA%D1%81%D0%B5.pdf (accessed on 12 December 2023).
- Bluml, B.M. Definition of medication therapy management: Development of professionwide consensus. J. Am. Pharm Assoc. 2005, 45, 566–572. [Google Scholar] [CrossRef]
- American Pharmacists Association. (n.d.). Medication Therapy Management (MTM). APhA Foundation. Available online: https://www.aphafoundation.org/medication-therapy-management (accessed on 12 December 2023).
- Groninger, H.; Phillips, J.M. Gross Hematuria: Assessment and Management at the End of Life. J. Hosp. Palliat. Nurs. 2012, 14, 184–188. [Google Scholar] [CrossRef]
- British Heart Foundation. Anticoagulant Medicines. Available online: https://www.bhf.org.uk/-/media/files/information-and-support/publications/medical-information-sheets/anticoagulant-medicines-is08.pdf?rev=da1668faf40f41c8807671d8be26668e&hash=047EEB7219024D87CF679B67FFB9156E (accessed on 30 January 2024).
- Srinivas, N.R. Cranberry juice ingestion and clinical drug-drug interaction potentials; review of case studies and perspectives. J. Pharm. Pharm. Sci. 2013, 16, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Mueck, W.; Stampfuss, J.; Kubitza, D.; Becka, M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin. Pharmacokinet. 2014, 53, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef]
- Camm, A.J.; Pinto, F.J.; Hankey, G.J.; Andreotti, F.; Hobbs, F.D.; Writing Committee of the Action for Stroke Prevention Alliance. Non-vitamin K antagonist oral anticoagulants and atrial fibrillation guidelines in practice: Barriers to and strategies for optimal implementation. Europace 2015, 17, 1007–1017. [Google Scholar] [CrossRef]
- Meschia, J.F.; Bushnell, C.; Boden-Albala, B.; Braun, L.T.; Bravata, D.M.; Chaturvedi, S.; Creager, M.A.; Eckel, R.H.; Elkind, M.S.; Fornage, M.; et al. Guidelines for the primary prevention of stroke: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 3754–3832. [Google Scholar] [CrossRef] [PubMed]
- Henke, P.K.; Kahn, S.R.; Pannucci, C.J.; Secemksy, E.A.; Evans, N.S.; Khorana, A.A.; Creager, M.A.; Pradhan, A.D.; American Heart Association Advocacy Coordinating Committee. Call to Action to Prevent Venous Thromboembolism in Hospitalized Patients: A Policy Statement From the American Heart Association. Circulation 2020, 141, e914–e931, Erratum in Circulation 2020, 141, e932; Erratum in Circulation 2021, 143, e249. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef]
- Liu, Z.; Song, D.; Wang, L.; Wang, C.; Zhou, J.; Sun, J.; Guo, L. Rivaroxaban vs. warfarin for the treatment and prevention of venous thromboembolism: A meta-analysis. Front. Surg. 2023, 10, 1086871. [Google Scholar] [CrossRef]
- Kampouraki, E.; Abohelaika, S.; Avery, P.; Biss, T.; Murphy, P.; Wynne, H.; Kamali, F. Elderly people are inherently sensitive to the pharmacological activity of rivaroxaban: Implications for DOAC prescribing. J. Thromb. Thrombolysis 2021, 52, 170–178. [Google Scholar] [CrossRef]
- Kubitza, D.; Becka, M.; Zuehlsdorf, M.; Mueck, W. Body weight has limited influence on the safety, tolerability, pharmacokinetics, or pharmacodynamics of rivaroxaban (BAY 59-7939) in healthy subjects. J. Clin. Pharmacol. 2007, 47, 218–226, Erratum in J. Clin. Pharmacol. 2008, 48, 1366–1367. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration (FDA). Approved Drug Products: Irbesartan Oral Tablets. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/020757s059s067lbl.pdf (accessed on 12 December 2023).
- Andersson, T.; Miners, J.O.; Veronese, M.E.; Birkett, D.J. Identification of human liver cytochrome P450 isoforms mediating secondary omeprazole metabolism. Br. J. Clin. Pharmacol. 1994, 37, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Gibson, C.M.; Cheng, S.; Ollier, C.; Nicolas, O.; Bergougnan, L.; Perrin, L.; LaCreta, F.P.; Hurbin, F.; Dubar, M. Differential effects of omeprazole and pantoprazole on the pharmacodynamics and pharmacokinetics of clopidogrel in healthy subjects: Randomized, placebo-controlled, crossover comparison studies. Clin. Pharmacol. Ther. 2011, 89, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Soons, P.A.; van den Berg, G.; Danhof, M.; van Brummelen, P.; Jansen, J.B.; Lamers, C.B.; Breimer, D.D. Influence of single- and multiple-dose omeprazole treatment on nifedipine pharmacokinetics and effects in healthy subjects. Eur. J. Clin. Pharmacol. 1992, 42, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Q.; Andersson, T.B.; Ahlström, M.; Weidolf, L. Comparison of inhibitory effects of the proton pump-inhibiting drugs omeprazole, esomeprazole, lansoprazole, pantoprazole, and rabeprazole on human cytochrome P450 activities. Drug Metab. Dispos. 2004, 32, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Zvyaga, T.; Chang, S.Y.; Chen, C.; Yang, Z.; Vuppugalla, R.; Hurley, J.; Thorndike, D.; Wagner, A.; Chimalakonda, A.; Rodrigues, A.D. Evaluation of six proton pump inhibitors as inhibitors of various human cytochromes P450: Focus on cytochrome P450 2C19. Drug Metab. Dispos. 2012, 40, 1698–1711. [Google Scholar] [CrossRef] [PubMed]
- Shirasaka, Y.; Sager, J.E.; Lutz, J.D.; Davis, C.; Isoherranen, N. Inhibition of CYP2C19 and CYP3A4 by omeprazole metabolites and their contribution to drug-drug interactions. Drug Metab. Dispos. 2013, 41, 1414–1424. [Google Scholar] [CrossRef]
- Pereira, F.; von Gunten, A.; Rosselet Amoussou, J.; De Giorgi Salamun, I.; Martins, M.M.; Verloo, H. Polypharmacy Among Home-Dwelling Older Adults: The Urgent Need for an Evidence-Based Medication Management Model. Patient Prefer. Adherence 2019, 13, 2137–2143. [Google Scholar] [CrossRef]
- Maher, R.L.; Hanlon, J.; Hajjar, E.R. Clinical consequences of polypharmacy in elderly. Expert. Opin. Drug Saf. 2014, 13, 57–65. [Google Scholar] [CrossRef]
- Foerster, K.I.; Hermann, S.; Mikus, G.; Haefeli, W.E. Drug-Drug Interactions with Direct Oral Anticoagulants. Clin. Pharmacokinet. 2020, 59, 967–980, Erratum in: Clin. Pharmacokinet. 2020, 59, 1647. [Google Scholar] [CrossRef] [PubMed]
- Burgos-Gonzalez, A.; Huerta, C.; Peñalver, M.J.; Sordo, L.; Pulido, J.; Soriano, L.C. Effect of tramadol and DOACs with special attention to dabigatran on concomitant use, on the risk of mayor bleeding using BIFAP database in Spain. Pharmacoepidemiol. Drug Saf. 2023, 32, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Byrd, D.C.; Gaskins, S.E.; Parrish, A.M.; Freeman, L.B. Warfarin and ciprofloxacin interaction: Case report and controversy. J. Am. Board. Fam. Pract. 1999, 12, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Bianco, T.M.; Bussey, H.I.; Farnett, L.E.; Linn, W.D.; Roush, M.K.; Wong, Y.W. Potential warfarin-ciprofloxacin interaction in patients receiving long-term anticoagulation. Pharmacotherapy 1992, 12, 435–439. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Question | Yes | No | Do Not Know | Score |
|---|---|---|---|---|
| 1. Are there previous conclusive reports on this reaction? | +1 | 0 | 0 | 0 |
| 2. Did the adverse event appear after the suspected drug was administered? | +2 | −1 | 0 | +2 |
| 3. Did the adverse event improve when the drug was discontinued or a specific antagonist was administered? | +1 | 0 | 0 | +1 |
| 4. Did the adverse event reappear when the drug was readministered? | +2 | −1 | 0 | 0 |
| 5. Are there alternative causes that could on their own have caused the reaction? | −1 | +2 | 0 | +2 |
| 6. Did the reaction reappear when a placebo was given? | −1 | +1 | 0 | 0 |
| 7. Was the drug detected in blood or other fluids in concentrations known to be toxic? | +1 | 0 | 0 | 0 |
| 8. Was the reaction more severe when the dose was increased or less severe when the dose was decreased? | +1 | 0 | 0 | 0 |
| 9. Did the patient have a similar reaction to the same or similar drugs in any previous exposure? | +1 | 0 | 0 | 0 |
| 10. Was the adverse event confirmed by any objective evidence? | +1 | 0 | 0 | 0 |
| Total Score 5 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rapaić, A.; Milošević, E.; Todorović, N.; Janjić, N.; Lalić-Popović, M.; Milošević, N. Suspected Hematuria: Adverse Effects of Rivaroxaban in Older Adult Treated for Atrial Fibrillation. Reports 2024, 7, 11. https://doi.org/10.3390/reports7010011
Rapaić A, Milošević E, Todorović N, Janjić N, Lalić-Popović M, Milošević N. Suspected Hematuria: Adverse Effects of Rivaroxaban in Older Adult Treated for Atrial Fibrillation. Reports. 2024; 7(1):11. https://doi.org/10.3390/reports7010011
Chicago/Turabian StyleRapaić, Aleksandra, Ekaterina Milošević, Nemanja Todorović, Nataša Janjić, Mladena Lalić-Popović, and Nataša Milošević. 2024. "Suspected Hematuria: Adverse Effects of Rivaroxaban in Older Adult Treated for Atrial Fibrillation" Reports 7, no. 1: 11. https://doi.org/10.3390/reports7010011