
Evaluation of Ocular Biometric Parameters Following Cataract Surgery

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olson, R.J.; Braga-Mele, R.; Chen, S.H.; Miller, K.M.; Pineda, R., 2nd; Tweeten, J.P.; Musch, D.C. Cataract in the Adult Eye Preferred Practice Pattern®. Ophthalmology 2017, 124, 1–119. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J.S. Cataracts. Lancet 2017, 390, 600–612. [Google Scholar] [CrossRef]
- Resnikoff, S.; Pascolini, D.; Etya’ale, D.; Kocur, I.; Pararajasegaram, R.; Pokharel, G.P.; Mariotti, S.P. Global data on visual impairment in the year 2002. Bull. World Health Organ. 2004, 82, 844–851. [Google Scholar]
- Patoni Popescu, I.S.; Mușat, O.; Stanca, S.; Coman Cernat, C.C.; Patoni, C.; Negru, S.; Teodoru, A.; Feier, H.; Danielescu, C. Vital dyes in macular hole surgery. Exp. Ther. Med. 2021, 21, 527. [Google Scholar] [CrossRef] [PubMed]
- Stanca, H.T.; Tăbăcaru, B.; Baltă, F.; Mălăescu, M.; Stanca, S.; Munteanu, M.; Dărăbuș, D.; Roșca, C.; Teodoru, A.C. Cumulative visual impact of two coagulability disorders: A case report. Exp. Ther. Med. 2020, 20, 218. [Google Scholar] [CrossRef] [PubMed]
- Teodoru, A.C.; Cerghedean-Florea, M.E. Management of Black Cataract; European Society of Cataract and Refractive Surgery: Vilamoura, Portugal, 2022. [Google Scholar]
- Cerghedean-Florea, M.E.; Teodoru, A.C. Surgical Approach in Phacomorphic Glaucoma; European Society of Cataract and Refractive Surgery: Vilamoura, Portugal, 2022. [Google Scholar]
- Cerghedean-Florea, M.E. Cataract Management in the Patient with Iridocyclitis; Romanian Society of Cataract and Refractive Surgery Congress: Sinaia, Romania, 2021. [Google Scholar]
- Moshetova, L.K.; Nesterov, A.P.; Ugorov, E.A. Clinical Ophthalmology Guidelines; GEOTAR-Media Publishing: Moscow, Russia, 2008; pp. 72–83. [Google Scholar]
- Das, B.N.; Thompson, J.R.; Patel, R.; Rosenthal, A.R. The prevalence of eye disease in Leicester: A comparison of adults of Asian and European descent. J. R. Soc. Med. 1994, 87, 219–222. [Google Scholar] [PubMed]
- Teodoru, A.C. Complicațiile Facoemulsificării; Carol Davila Publishing: Bucharest, Romania, 2012; ISBN 978-973-708-644-0. [Google Scholar]
- Nema, H.V.; Nema, N. Textbook of Ophthalmology, 6th ed.; Jaypee Brothers Medical Publishers: New Delhi, India, 2008; ISBN 10-9350255073. [Google Scholar]
- Lam, D.; Rao, S.K.; Ratra, V.; Liu, Y.; Mitchell, P.; King, J.; Tassignon, M.J.; Jonas, J.; Pang, C.P.; Chang, D.F. Cataract. Nat. Rev. Dis. Primers 2015, 1, 15014. [Google Scholar] [CrossRef]
- Van den Bruel, A.; Gailly, J.; Devriese, S.; Welton, N.J.; Shortt, A.J.; Vrijens, F. The protective effect of ophthalmic viscoelastic devices on endothelial cell loss during cataract surgery: A meta-analysis using mixed treatment comparisons. Br. J. Ophthalmol. 2011, 95, 5–10. [Google Scholar] [CrossRef]
- Kessel, L.; Andresen, J.; Tendal, B.; Erngaard, D.; Flesner, P.; Hjortdal, J. Toric Intraocular Lenses in the Correction of Astigmatism during Cataract Surgery: A Systematic Review and Meta-analysis. Ophthalmology 2016, 123, 275–286. [Google Scholar] [CrossRef] [Green Version]
- Lam, D.K.; Chow, V.W.; Ye, C.; Ng, P.K.; Wang, Z.; Jhanji, V. Comparative evaluation of aspheric toric intraocular lens implantation and limbal relaxing incisions in eyes with cataracts and ≤3 dioptres of astigmatism. Br. J. Ophthalmol. 2016, 100, 258–262. [Google Scholar] [CrossRef]
- Hoffer, K.J.; Shammas, H.J.; Savini, G.; Huang, J. Multicenter study of optical low-coherence interferometry and partial-coherence interferometry optical biometers with patients from the United States and China. J. Cataract. Refract. Surg. 2016, 42, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Fukumitsu, H.; Camps, V.J.; Piñero, D.P. Intrasession Repeatability of Biometric Measurements Obtained with a Low-Coherence Interferometry System in Pseudophakic Eyes. Curr. Eye Res. 2020, 45, 221–226. [Google Scholar] [CrossRef]
- Mandal, P.; Berrow, E.J.; Naroo, S.A.; Wolffsohn, J.S.; Uthoff, D.; Holland, D.; Shah, S. Validity and repeatability of the Aladdin ocular biometer. Br. J. Ophthalmol. 2014, 98, 256–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Savini, G.; Wu, F.; Yu, X.; Yang, J.; Yu, A.; Yu, Y.; Wang, Q. Repeatability and reproducibility of ocular biometry using a new noncontact optical low-coherence interferometer. J. Cataract. Refract. Surg. 2015, 41, 2233–2241. [Google Scholar] [CrossRef]
- Sabatino, F.; Findl, O.; Maurino, V. Comparative analysis of optical biometers. J. Cataract. Refract. Surg. 2016, 42, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Ning, X.; Yang, Y.; Yan, H.; Zhang, J. Anterior chamber depth—A predictor of refractive outcomes after age-related cataract surgery. BMC Ophthalmol. 2019, 19, 134. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, P.C.; Hütz, W.W. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J. Cataract. Refract. Surg. 2010, 36, 1479–1485. [Google Scholar] [CrossRef]
- López, C.G.; López, V.G.; Juan, V.; Martin, R. Change in Axial Length Pre and Post Cataract Surgery Measured with IOL Master. J. Clin. Exp. Ophthalmol. 2016, 7, 544. [Google Scholar] [CrossRef] [Green Version]
- Kaup, S.; Shivalli, S.; Ks, D.; Arunachalam, C.; Varghese, R.C. Central corneal thickness changes in bevel-up versus bevel-down phacoemulsification cataract surgery: Study protocol for a randomised, triple-blind, parallel group trial. BMJ Open 2016, 6, e012024. [Google Scholar] [CrossRef] [Green Version]
- Sugar, A.; Sadri, E.; Dawson, D.G.; Musch, D.C. Refractive stabilization after temporal phacoemulsification with foldable acrylic intraocular lens implantation. J. Cataract. Refract. Surg. 2001, 27, 1741–1745. [Google Scholar] [CrossRef]
- Olsen, T. Calculation of intraocular lens power: A review. Acta Ophthalmol. Scand. 2007, 85, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Uçakhan, O.O.; Ozkan, M.; Kanpolat, A. Anterior chamber parameters measured by the Pentacam CES after uneventful phacoemulsification in normotensive eyes. Acta Ophthalmol. 2009, 87, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Prinz, A.; Neumayer, T.; Buehl, W.; Kiss, B.; Sacu, S.; Drexler, W.; Findl, O. Influence of severity of nuclear cataract on optical biometry. J. Cataract. Refract. Surg. 2006, 32, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- Rajan, M.S.; Keilhorn, I.; Bell, J.A. Partial coherence laser interferometry vs conventional ultrasound biometry in intraocular lens power calculations. Eye 2002, 16, 552–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drexler, W.; Findl, O.; Menapace, R.; Rainer, G.; Vass, C.; Hitzenberger, C.K.; Fercher, A.F. Partial coherence interferometry: A novel approach to biometry in cataract surgery. Am. J. Ophthalmol. 1998, 126, 524–534. [Google Scholar] [CrossRef]
- Chylack, L.T., Jr.; Wolfe, J.K.; Singer, D.M.; Leske, M.C.; Bullimore, M.A.; Bailey, I.L.; Friend, J.; McCarthy, D.; Wu, S.Y. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch. Ophthalmol. 1993, 111, 831–836. [Google Scholar] [CrossRef]
- Pereira, F.A.; Cronemberger, S. Ultrasound biomicroscopic study of anterior segment changes after phacoemulsification and foldable intraocular lens implantation. Ophthalmology 2003, 110, 1799–1806. [Google Scholar] [CrossRef]
- Hoffer, K.J. Axial dimension of the human cataractous lens. Arch. Ophthalmol. 1993, 111, 914–918. [Google Scholar] [CrossRef]
- Caglar, C.; Batur, M.; Eser, E.; Demir, H.; Yaşar, T. The Stabilization Time of Ocular Measurements after Cataract Surgery. Semin. Ophthalmol. 2017, 32, 412–417. [Google Scholar] [CrossRef]
- Singh, R.; Vasavada, A.R.; Janaswamy, G. Phacoemulsification of brunescent and black cataracts. J. Cataract. Refract. Surg. 2001, 27, 1762–1769. [Google Scholar] [CrossRef]
- Behndig, A.; Lundberg, B. Transient corneal edema after phacoemulsification: Comparison of 3 viscoelastic regimens. J. Cataract. Refract. Surg. 2002, 28, 1551–1556. [Google Scholar] [CrossRef]
- Hwang, H.B.; Lyu, B.; Yim, H.B.; Lee, N.Y. Endothelial Cell Loss after Phacoemulsification according to Different Anterior Chamber Depths. J. Ophthalmol. 2015, 2015, 210716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galgauskas, S.; Juodkaite, G.; Tutkuvienė, J. Age-related changes in central corneal thickness in normal eyes among the adult Lithuanian population. Clin. Interv. Aging 2014, 9, 1145–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, L.; Zhao, F.; Ke, X.; Zhao, J.; Shi, M. Correlation Between Degree of Lens Opacity and the Phacoemulsification Energy Parameters Using Different Imaging Methods in Age-Related Cataract. Transl. Vis. Sci. Technol. 2022, 11, 24. [Google Scholar] [CrossRef]
- Liovic Milec, M.; Sekelj, S.; Konjevic-Pernar, S. Postoperative Corneal Edema after Phacoemulsification. SEEMEDJ 2022, 6, 113–120. [Google Scholar] [CrossRef]
- Alpins, N.A. A new method of analyzing vectors for changes in astigmatism. J. Cataract. Refract. Surg. 1993, 19, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Duke-Elder, S.; Stewart, S.; Abrams, D. System of Ophthalmology: Ophthalmic Optics and Refraction, 1st ed.; Mosby Publishing: St Louis, MO, USA, 1970; Volume 5, ISBN 100853137587. [Google Scholar]
- Klijn, S.; van der Sommen, C.M.; Sicam, V.A.; Reus, N.J. Value of posterior keratometry in the assessment of surgically induced astigmatic change in cataract surgery. Acta Ophthalmol. 2016, 94, 494–498. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Wang, X.; Zhang, H.; Pang, Y.; Wei, R.H. Clinical evaluation of surgery-induced astigmatism in cataract surgery using 2.2 mm or 1.8 mm clear corneal micro-incisions. Int. J. Ophthalmol. 2017, 10, 68–71. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Groups | Males | Females |
|---|---|---|
| Average | 69.71 ± 8.35 | 73.44 ± 6.20 |
| 50–59 years | 4 | |
| 60–69 years | 13 | 16 |
| 70–79 years | 11 | 29 |
| 80–90 years | 3 | 7 |
| Total | 31 (37.3%) | 52 (62.7%) |
| Ocular Biometric and Keratometric Parameters | Preoperative Values Mean ± SD (min; max) | Postoperative Values Mean ± SD (min; max) | p Value |
|---|---|---|---|
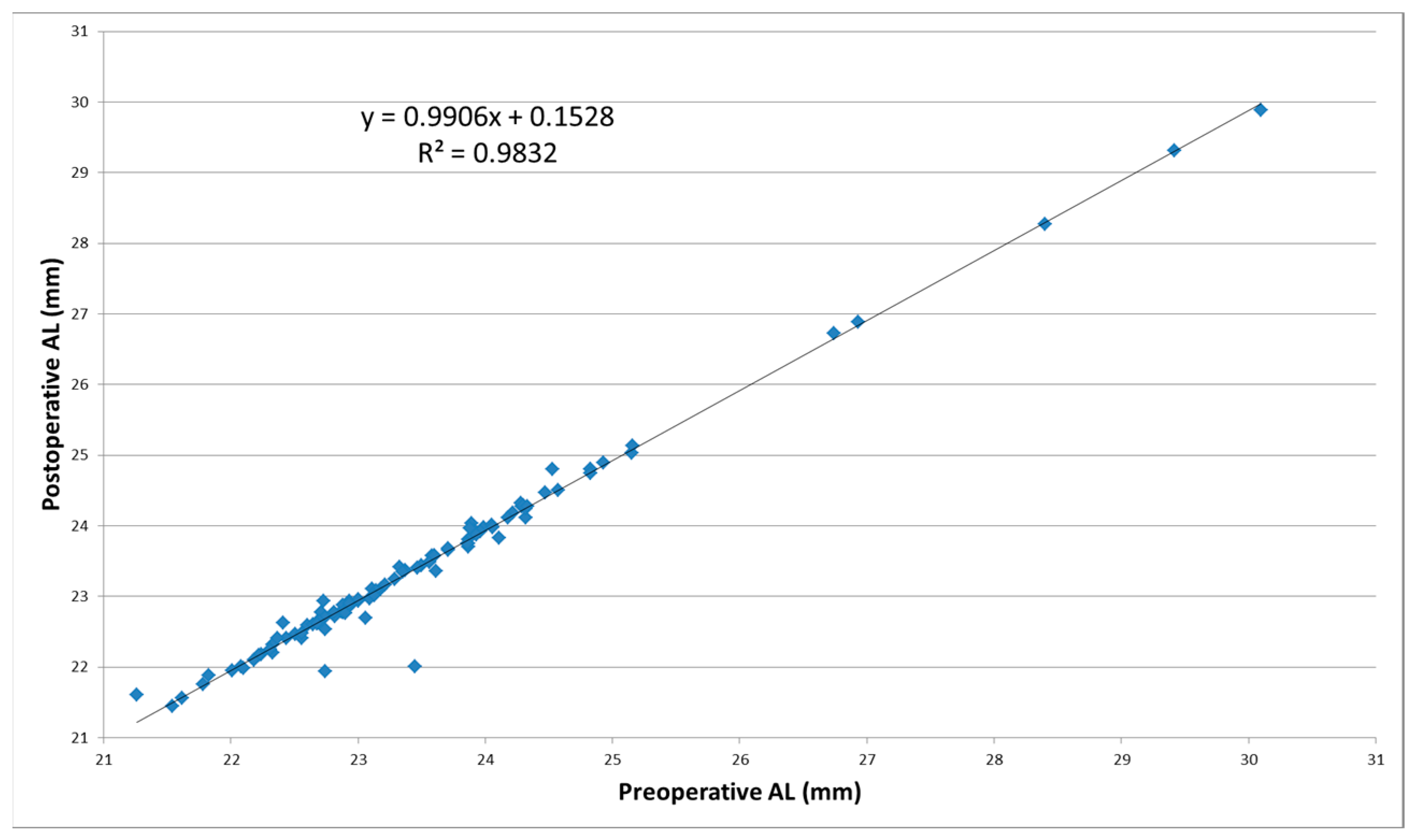
| Axial length (mm) | 23.53 ± 1.41 (21.26; 30.10) | 23.46 ± 1.40 (21.45; 29.89) | <0.001 |
| Anterior chamber depth (mm) | 3.23 ± 0.51 (2.19; 5.10) | 4.34 ± 0.51 (2.49; 5.18) | <0.001 |
| Lens thickness (mm) | 4.48 ± 0.35 (3.71; 5.22) | 0.79 ± 0.12 (0.56; 1.00) | <0.001 |
| Corneal central thickness (µm) | 546.49 ± 35.24 (486; 634) | 558.84 ± 38.23 (491; 654) | <0.01 |
| Degree of anterior corneal astigmatism (CYL) | −0.707 ± 0.612 (−3.650; 0.970) | −0.796 ± 0.559 (−3.550; 0.000) | 0.0296 |
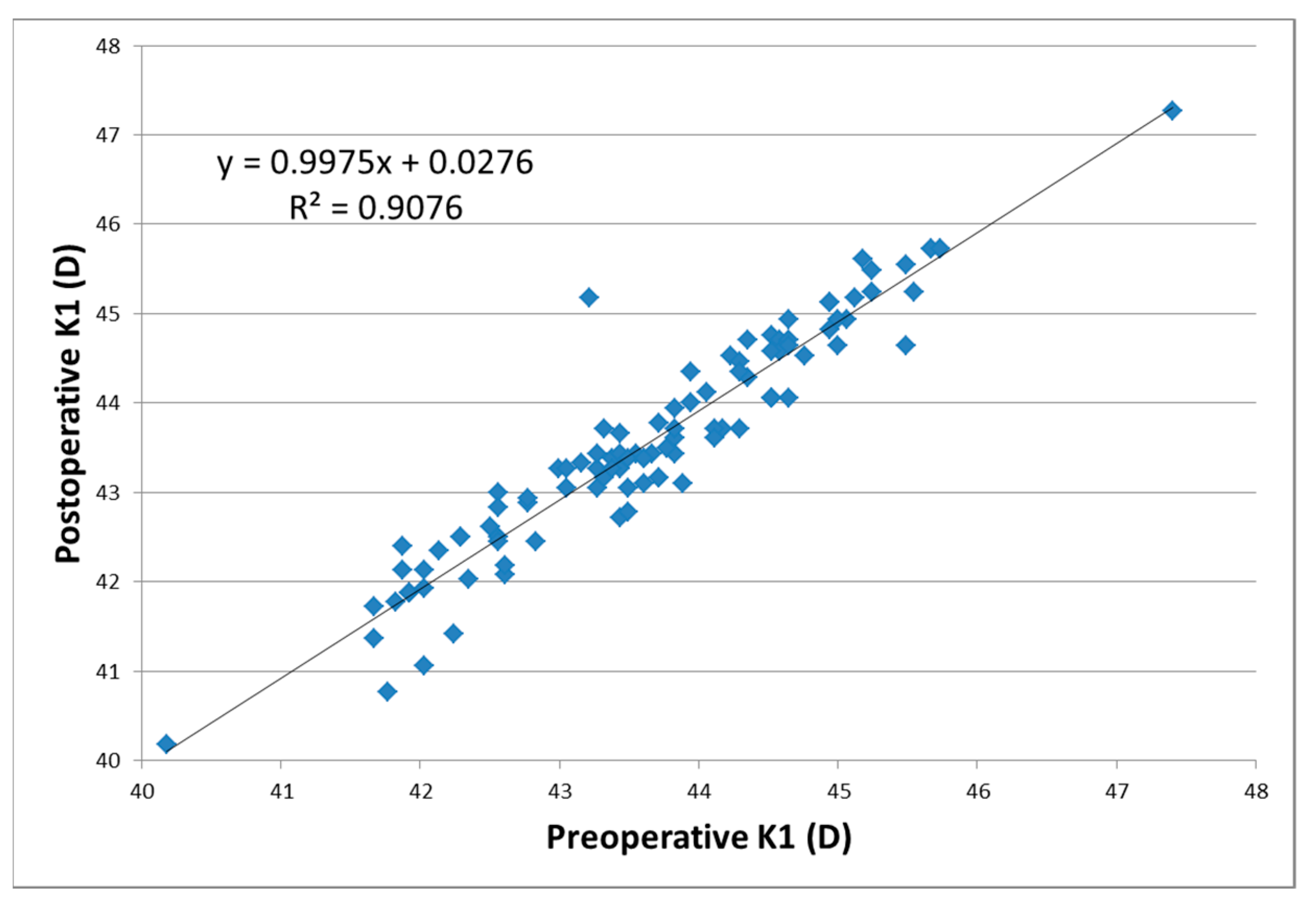
| The flattest point/meridian K1 (D) | 43.67 ± 1.21 (40.18; 47.40) | 43.59 ± 1.26 (40.18; 47.27) | 0.0152 |
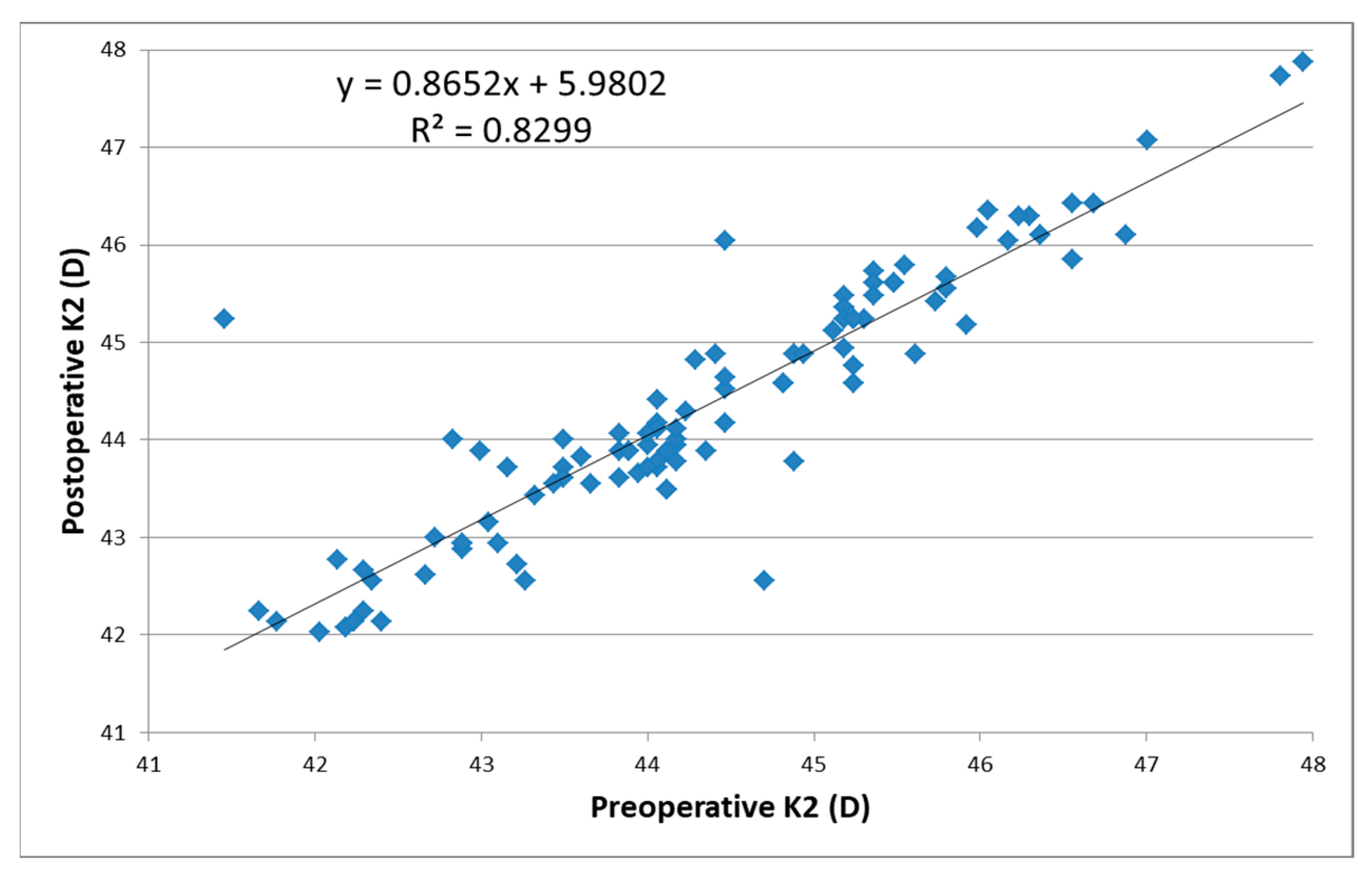
| The steepest/meridian point K2 (D) | 44.37 ± 1.39 (41.46; 47.94) | 44.37 ± 1.32 (42.03; 47.87) | 0.4854 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teodoru, C.A.; Cerghedean-Florea, M.-E.; Tănăsescu, C.; Dura, H.; Fleacă, R.; Munteanu, M.; Stanca, H.; Popescu, F.G.; Roman, M.D.; Nicula, G.Z.; et al. Evaluation of Ocular Biometric Parameters Following Cataract Surgery. Reports 2023, 6, 3. https://doi.org/10.3390/reports6010003
Teodoru CA, Cerghedean-Florea M-E, Tănăsescu C, Dura H, Fleacă R, Munteanu M, Stanca H, Popescu FG, Roman MD, Nicula GZ, et al. Evaluation of Ocular Biometric Parameters Following Cataract Surgery. Reports. 2023; 6(1):3. https://doi.org/10.3390/reports6010003
Chicago/Turabian StyleTeodoru, Cosmin Adrian, Maria-Emilia Cerghedean-Florea, Ciprian Tănăsescu, Horațiu Dura, Radu Fleacă, Mihnea Munteanu, Horia Stanca, Florina Georgeta Popescu, Mihai Dan Roman, Gheorghe Zsolt Nicula, and et al. 2023. "Evaluation of Ocular Biometric Parameters Following Cataract Surgery" Reports 6, no. 1: 3. https://doi.org/10.3390/reports6010003