
Three-Dimensional Printing and Digital Flow in Human Medicine: A Review and State-of-the-Art
 ,
,
Abstract
:1. Introduction
2. Search Strategy
3. A Brief History of 3D Technology
4. Three-Dimensional Technology for Multi-Professional Collaboration and Patient Quality of Life
5. Digital Flow in 3D Printing
- Three-dimensional image acquisition;
- Three-dimensional Modeling;
- Three-dimensional printing.
5.1. Image Acquisition
5.2. Three-Dimensional Modeling
5.3. Three-Dimensional Printing
6. Experiences with the Use of 3D Technology in Medicine
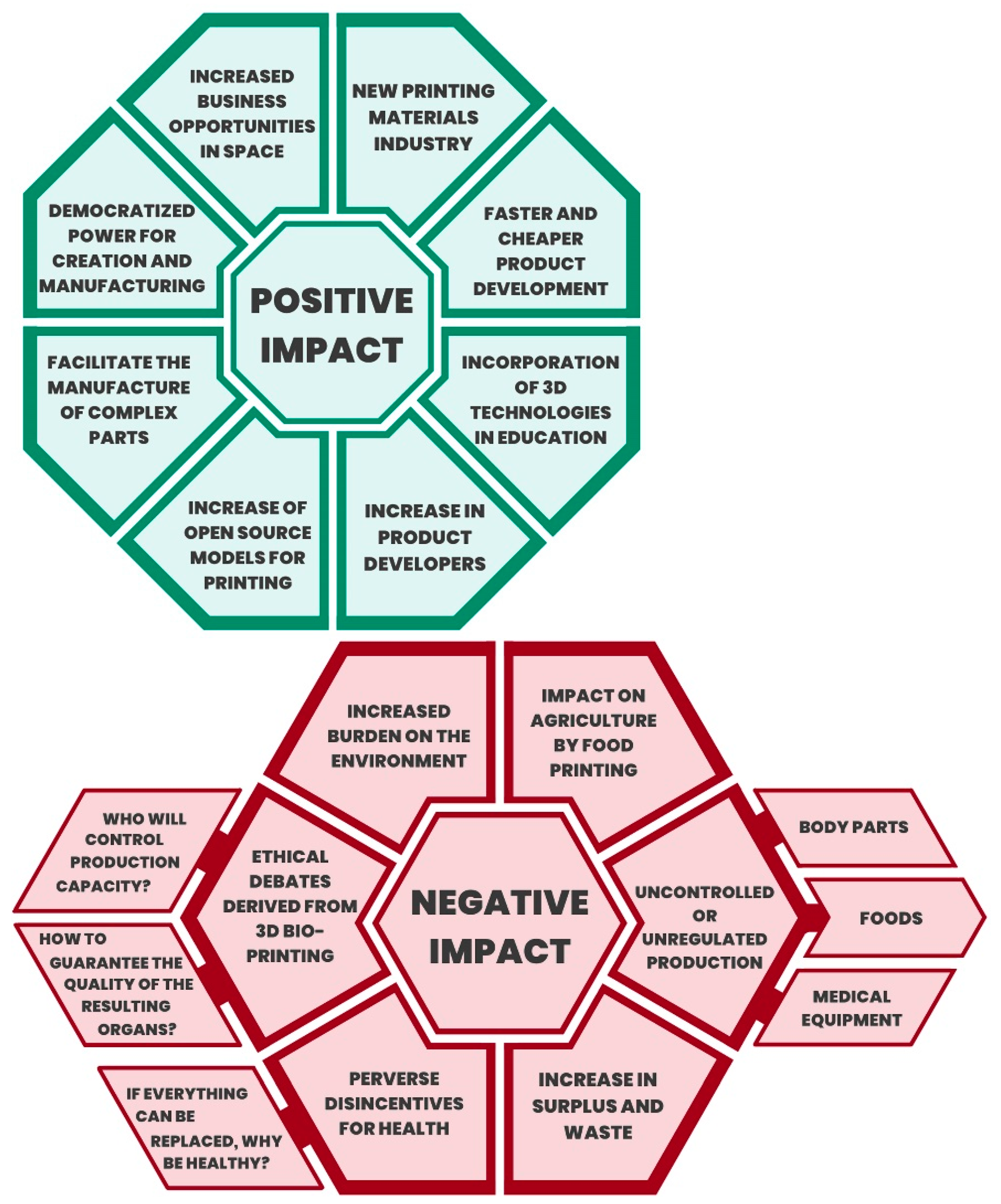
7. Three-Dimensional Technology and Digital Transformation and the Impact on Medicine and Public Health
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Schwab, K. La Cuarta Revolución Industrial; DEBATE: Madrid, Spain, 2016. [Google Scholar]
- Presidencia de consejo de Ministros. Decreto Legislativo N° 1412 Normativa sobre Transformación Digital, Normatividad del Centro Nacional de Seguridad Digital; PCM: Lima, Peru, 2018. Available online: https://www.gob.pe/institucion/pcm/normas-legales/289706-1412 (accessed on 28 November 2022).
- Presidencia del Consejo de Ministros. Laboratorio de Gobierno y Transformación Digital. Plataforma Digital única del Estado Peruano; PCM: Lima, Peru, 2019. Available online: https://www.gob.pe/8256 (accessed on 28 November 2022).
- Diario El Peruano. Decreto de Urgencia que crea el Sistema Nacional de Transformación Digital—Decreto de Urgencia—n° 006-2020—Poder Ejecutivo—Decretos de Urgencia [Internet]; El Peruano. 2020. Available online: https://busquedas.elperuano.pe/normaslegales/decreto-de-urgencia-que-crea-el-sistema-nacional-de-transfor-decreto-de-urgencia-n-006-2020-1844001-1/ (accessed on 28 November 2022).
- Voelcker, H.B.; Requicha, A.A.G. Geometric Modeling of Mechanical Parts and Processes. Computer 1977, 10, 48–57. [Google Scholar] [CrossRef]
- Kietzmann, J.; Pitt, L.; Berthon, P. Disruptions, decisions, and destinations: Enter the age of 3-D printing and additive manufacturing. Bus. Horiz. 2015, 58, 209–215. [Google Scholar] [CrossRef]
- George, M.; Aroom, K.R.; Hawes, H.G.; Gill, B.S.; Love, J. 3D Printed Surgical Instruments: The Design and Fabrication Process. World J. Surg. 2017, 41, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-H.; Chang, K.-H. Chapter 5—Rapid Prototyping; University of Salford: Amsterdam, The Netherlands, 2013. [Google Scholar] [CrossRef]
- Jasveer, S.; Jianbin, X. Comparison of Different Types of 3D Printing Technologies. Int. J. Sci. Res. Publ. 2018, 8, 1–9. [Google Scholar] [CrossRef]
- Peng, Q.; Tang, Z.; Liu, O.; Peng, Z. Rapid prototyping-assisted maxillofacial reconstruction. Ann. Med. 2015, 47, 186–208. [Google Scholar] [CrossRef]
- Trenfield, S.J.; Awad, A.; Madla, C.M.; Hatton, G.B.; Firth, J.; Goyanes, A.; Gaisford, S.; Basit, A.W. Shaping the future: Recent advances of 3D printing in drug delivery and healthcare. Expert Opin. Drug Deliv. 2019, 16, 1081–1094. [Google Scholar] [CrossRef]
- Espera, A.H.; Dizon, J.R.C.; Chen, Q.; Advincula, R.C. 3D-printing and advanced manufacturing for electronics. Prog. Addit. Manuf. 2019, 4, 245–267. [Google Scholar] [CrossRef]
- Verhoeven, T.J.; Coppen, C.; Barkhuysen, R.; Bronkhorst, E.M.; Merkx, M.A.W.; Bergé, S.J.; Maal, T. Three dimensional evaluation of facial asymmetry after mandibular reconstruction: Validation of a new method using stereophotogrammetry. Int. J. Oral Maxillofac. Surg. 2013, 42, 19–25. [Google Scholar] [CrossRef]
- Salazar-Gamarra, R.; Seelaus, R.; Da Silva, J.V.L.; Da Silva, A.M.; Dib, L.L. Monoscopic photogrammetry to obtain 3D models by a mobile device: A method for making facial prostheses. J. Otolaryngol. Head Neck Surg. 2016, 45, 33. [Google Scholar] [CrossRef]
- Lauren, M.; McIntyre, F. 4D clinical imaging for dynamic CAD. Int. J. Dent. 2013, 2013, 690265. [Google Scholar] [CrossRef]
- Bader, C.; Kolb, D.; Weaver, J.C.; Sharma, S.; Hosny, A.; Costa, J.; Oxman, N. Making data matter: Voxel printing for the digital fabrication of data across scales and domains. Sci. Adv. 2018, 4, eaas8652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed Eng Online 2016, 15, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, S.N.; El-Sheikha, J.; Lowe, D. The development of a Patients Concerns Inventory (PCI) to help reveal patients concerns in the head and neck clinic. Oral Oncol. 2009, 45, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Gamarra, R.; Moraes, C.A.D.C.; Seelaus, R.M.; Silva JVLDa Dib, L.L.; Ulloa, J.J. Introdução à metodologia “Mais Identidade”: Próteses faciais 3D com a utilização de tecnologias acessíveis para pacientes sobreviventes de câncer no rosto. Comun. Cient Técn Odontol. 2019, 2, 251–272. [Google Scholar] [CrossRef]
- Salazar-Gamarra, R.; Oliveira, J.A.P.; Dib, L.L. A estética em reabilitação bucomaxilofacial. Rev. APCD Estética 2019, 5, 20–27. [Google Scholar]
- Denise, H.C.; Ting, S.; Lin, C.Y.; Lin, C.L.K.; Lin, Y.L.C. Relationships of exercise timing with sleep, fatigue and rest—Activity rhythms of lung cancer patients in Taiwan: An exploratory study. Cancer Care 2020, 29, e13233. [Google Scholar] [CrossRef]
- Bibb, R.; Eggbeer, D.; Paterson, A. Medical Modelling: The Application of Advanced Design and Rapid Prototyping Techniques in Medicine; Woodhead Pub.: New York, NY, USA, 2020. [Google Scholar]
- Jakus, A.E. An Introduction to 3D Printing—Past, Present, and Future Promise. In 3D Printing in Orthopaedic Surgery; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1–15. [Google Scholar] [CrossRef]
- Lobat, T. Applications of Biomedical Engineering in Dentistry; Springer Nature: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Tincopa, J.P.; Salazar-Gamarra, R.; Lopez-Hinostroza, M.; Moya-Salazar, B.; Contreras-Pulache, H.; Moya-Salazar, J. Comparison of Models for 3D Printing of Solitary Fibrous Tumor Obtained Using Open-Source Segmentation Software. Appl. Syst. Innov. 2022, 5, 116. [Google Scholar] [CrossRef]
- Driscoll, R.M. Clinical Applications of Digital Dental Technology; Wiley Library: Hoboken, NJ, USA, 2015. [Google Scholar] [CrossRef]
- Tamimi, F.; Hirayama, H. Digital Restorative Dentistry a Guide to Materials, Equipment and Clinical Procedures; Springer Nature: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Mishra, S. Application of 3D printing in medicine. Indian Heart J. 2016, 68, 108–109. [Google Scholar] [CrossRef] [Green Version]
- Lane, J.; Mait, J.; Unnanuntana, A.; Hirsch, B.; Shaffer, A.; Shonuga, O. Materials in Fracture Fixation. Compr. Biomater. 2011, 6, 219–235. [Google Scholar] [CrossRef]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef]
- Karageorgiou, V.; Kaplan, D. Porosity of 3D biomaterial scaffolds and osteogenesis. Biomaterials 2005, 26, 5474–5491. [Google Scholar] [CrossRef] [PubMed]
- Sidambe, A. Biocompatibility of Advanced Manufactured Titanium Implants—A Review. Materials 2014, 7, 8168–8188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khorsandi, D.; Fahimipour, A.; Abasian, P.; Saber, S.S.; Seyedi, M.; Ghanavati, S.; Ahmad, A.; De Stephanis, A.A.; Taghavinezhaddilami, F.; Leonova, A.; et al. 3D and 4D printing in dentistry and maxillofacial surgery: Printing techniques, materials, and applications. Acta Biomater. 2021, 122, 26–49. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Gamarra, R.; Cárdenas-Bocanegra, A.; Masch, U.; Da Costa Moraes, C.A.; Seelaus, R.; Lopes Da Silva, J.V.; Lauria Dib, L. Color translation from monoscopic photogrammetry +ID Methodology into a Polyjet final 3D printed facial prosthesis. F1000Research 2022, 11, 582. [Google Scholar] [CrossRef]
- Malateaux, G.; Salazar-Gamarra, R.; de Souza Silva, J.; Gallego Arias Pecorari, V.; Suffredini, I.B.; Dib, L.L. Ultraviolet C as a method of disinfecting medical silicone used in facial prostheses: An in vitro study. J. Prosthet. Dent. 2021, 126, 452.e1–452.e6. [Google Scholar] [CrossRef]
- Sun, L.; Hua, G.; Cheng, T.C.E.; Wang, Y. How to price 3D-printed products? Pricing strategy for 3D printing platforms. Int. J. Prod. Econ. 2020, 226, 107600. [Google Scholar] [CrossRef]
- Arbabian, M.E.; Wagner, M.R. The Impact of 3D Printing on Manufacturer-Retailer Supply Chains. Eur. J. Oper. Res. 2020, 285, 538–552. [Google Scholar] [CrossRef]
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.Q.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. Part B Eng. 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Emile, S.H.; Wexner, S.D. Systematic review of the applications of three-dimensional printing in colorectal surgery. Color. Dis. 2019, 21, 261–269. [Google Scholar] [CrossRef]
- Perica, E.R.; Sun, Z. A Systematic Review of Three-Dimensional Printing in Liver Disease. J. Digit. Imaging 2018, 31, 692–701. [Google Scholar] [CrossRef]
- Francoisse, C.A.; Sescleifer, A.M.; King, W.T.; Lin, A.Y. Three-dimensional printing in medicine: A systematic review of pediatric applications. Pediatr. Res. 2020, 89, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Prince, J.D. 3D Printing: An Industrial Revolution. J. Electron. Resour. Med. Libr. 2014, 11, 39–45. [Google Scholar] [CrossRef]
- Hong, C.J.; Giannopoulos, A.A.; Hong, B.Y.; Witterick, I.J.; Irish, J.C.; Lee, J.; Vescan, A.; Mitsouras, D.; Dang, W.; Campisi, P.; et al. Clinical applications of three-dimensional printing in otolaryngology–head and neck surgery: A systematic review. Laryngoscope 2019, 129, 2045–2052. [Google Scholar] [CrossRef] [PubMed]
- Randazzo, M.; Pisapia, J.; Singh, N.; Thawani, J. 3D printing in neurosurgery: A systematic review. Surg. Neurol. Int. 2016, 7, S801–S809. [Google Scholar] [CrossRef] [Green Version]
- Lau, I.; Sun, Z. Three-dimensional printing in congenital heart disease: A systematic review. J. Med. Radiat. Sci. 2018, 65, 226–236. [Google Scholar] [CrossRef]
- Sun, Z.; Lee, S.Y. A systematic review of 3-D printing in cardiovascular and cerebrovascular diseases. Anatol. J. Cardiol. 2017, 17, 423–435. [Google Scholar] [CrossRef]
- Langridge, B.; Cantab, B.A.; Momin, S.; Coumbe, B.; Hons, B.A.; Woin, E.; Griffin, M.; Butler, P. Systematic Review of the Use of 3-Dimensional Printing in Surgical Teaching and Assessment 2017. J. Surg. Educ. 2018, 75, 209–221. [Google Scholar] [CrossRef]
- Sun, Z.; Liu, D. A systematic review of clinical value of three-dimensional printing in renal disease. Quant. Imaging Med. Surg. 2018, 8, 311–325. [Google Scholar] [CrossRef] [Green Version]
- Chao, I.; Young, J.; Chuen, J.; Weinberg, L.; Rachbuch, C. The application of three-dimensional printing technology in anaesthesia: A systematic review 2017. Anaesthesia 2017, 72, 641–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tino, R.; Yeo, A.; Leary, M.; Brandt, M.; Kron, T. A systematic review on 3D-Printed imaging and dosimetry phantoms in radiation therapy. Technol. Cancer Res. Treat. 2019, 18, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Rooney, M.K.; Rosenberg, D.M.; Braunstein, S.; Cunha, A.; Damato, A.L.; Ehler, E.; Pawlicki, T.; Robar, J.; Tatebe, K.; Golden, D.W. Three-dimensional printing in radiation oncology: A systematic review of the literature. J. Appl. Clin. Med. Phys. 2020, 21, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Crafts, T.D.; Ellsperman, S.E.; Wannemuehler, T.J.; Bellicchi, T.D.; Shipchandler, T.Z.; Mantravadi, A.V. Three-Dimensional Printing and Its Applications in Otorhinolaryngology–Head and Neck Surgery. Otolaryngol. Head Neck Surg. 2017, 156, 999–1010. [Google Scholar] [CrossRef] [Green Version]
- Bertana, V.; Catania, F.; Cocuzza, M.; Ferrero, S.; Scaltrito, L.; Pirri, C.F. Medical and biomedical applications of 3D and 4D printed polymer nanocomposites. In 3D and 4D Printing of Polymer Nanocomposite Materials; Elsevier: Amsterdam, The Netherlands, 2020; pp. 325–366. [Google Scholar] [CrossRef]
- Ministerio de Salud. Resolución Directoral 000117-2022-DG-INSNSB del 08 de Junio de 2022. Por lo cual se Aprueba la “Guía de Procedimiento: Impresión de Modelos Anatómicos en 3D”; MINSA: Lima, Peru, 2022.
- Ma, S.Q.; Zhang, Y.P.; Wang, M.; Liang, Y.H.; Ren, L.; Ren, L.Q. Recent progress in 4D printing of stimuli-responsive polymeric materials. Sci. China Technol. Sci. 2019, 63, 532–544. [Google Scholar] [CrossRef]
- Menegaz, A.M.; de Ávila Quevedo, L.; Muniz, L.C.; Finlayson, T.L.; Ayala, G.X.; Cascaes, A.M. Changes in young children’s oral health-related behaviours and caregiver knowledge: A cluster randomized controlled trial in Brazil. Community Dent. Oral Epidemiol. 2020, 48, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Marques, I.C.P.; Ferreira, J.J.M. Digital transformation in the area of health: Systematic review of 45 years of evolution. Health Technol. 2020, 10, 575–586. [Google Scholar] [CrossRef]
- Delloite, T.D.C. Digital transformation Shaping the future of European healthcare. Digit Transform 2020, 3, 1–61. [Google Scholar]
- Mesko, B. Digital Health Technologies and Well-Being in the Future. IT Prof. 2020, 22, 20–23. [Google Scholar] [CrossRef]
- Moya-Salazar, J.; Gomez-Saenz, L.; Cañari, B.; Contreras-Pulache, H. Scientific research and innovation response to COVID-19 in Peru. F1000research 2021, 10, 399. [Google Scholar] [CrossRef]
- Arroyo, J. Salud: La Reforma Silenciosa; Universidad Peruana Cayetano Heredia: Lima, Peru, 2015. [Google Scholar] [CrossRef]
- Salmi, M.; Akmal, J.S.; Pei, E.; Wolff, J.; Jaribion, A.; Khajavi, S.H. 3D printing in COVID-19: Productivity estimation of the most promising open source solutions in emergency situations. Appl. Sci. 2020, 10, 4004. [Google Scholar] [CrossRef]
- Pedraja, J.; Maestre, J.M.; Rabanal, J.M.; Morales, C.; Aparicio, J.; del Moral, I. Role of 3D printing for the protection of surgical and critical care professionals in the COVID-19 pandemic. Rev. Esp. Anestesiol. Reanim. 2020, 67, 417–424. [Google Scholar] [CrossRef]
- Tarfaoui, M.; Nachtane, M.; Goda, I.; Qureshi, Y.; Benyahia, H. 3D printing to support the shortage in personal protective equipment caused by COVID-19 pandemic. Materials 2020, 13, 3339. [Google Scholar] [CrossRef] [PubMed]
- Tino, R.; Moore, R.; Antoline, S.; Ravi, P.; Wake, N.; Ionita, C.N.; Morris, J.M.; Decker, S.J.; Sheikh, A.; Rybicki, F.J.; et al. COVID-19 and the role of 3D printing in medicine. 3D Print Med. 2020, 6, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, J.; Goldstein, T.; Trahan, S.; Neuwirth, A.; Tatoris, K.; Decker, S. A 3D-printed nasopharyngeal swab for COVID-19 diagnostic testing. 3D Print Med. 2020, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Gino, B.; Wang, Z.; D’Entremont, P.; Renouf, T.S.; Dubrowski, A. Automated Inflating Resuscitator (AIR): Design and Development of a 3D-Printed Ventilator Prototype and Corresponding Simulation Scenario Based on the Management of a Critical COVID-19 Patient. Cureus 2020, 12, e9134. [Google Scholar] [CrossRef] [PubMed]
- Skrzypczak, N.G.; Tanikella, N.G.; Pearce, J.M. Open source high-temperature RepRap for 3-D printing heat-sterilizable PPE and other applications. HardwareX 2020, 8, e00130. [Google Scholar] [CrossRef]


{kind=link}
| Classification and Applications of 3D Printing | |||
|---|---|---|---|
| BIOMODEL PRINTING | Printing of an anatomical model whose added value is in visualizing and interacting with an anatomical fragment. No connotation of surgical planning; they are intended to be a materialized reproduction of the anatomy. Among its advantages is to improve the dimension of understanding the anatomy. It is widely used in multiple specialties that carry surgical connotations for diagnostic and planning purposes, as well as creating a value of confidence in the patient’s environment. | ||
| PROSTHESIS PRINTING | Intermediate prototypes | These materialize the desired shape, finally transforming into another biomaterial yet to be made available to be printed directly. An example of this application is buccomaxillofacial rehabilitation for missing parts of the face, worked on by a specialist dental surgeon. | |
| Direct prosthesis | Internal | They aimed at printing biomaterials that can substitute another autologous substance to be implanted. Their regulation is as tightly restricted as pharmacology since they interact with the physiological environment. The most commonly used materials are Titanium, PEEK, and PMMA. Depending on each country, these materials require demonstration and approval by governmental agencies, such as FDA, ANVISA, DIGEMID, or others. An example of these prostheses is Neurosurgical Prostheses, worked by the transdisciplinary team of neurosurgery. | |
| External | They aimed at coupling bioinert materials on the surface of the body. Commonly used materials are PET, PLA, ABS, and Resins with biocompatibility certificates. An example of these prostheses is those of the extremities. They are worked by the transdisciplinary team composed of orthopedic physicians, engineers specialized in biomedical equipment, and other related technicians. | ||
| SURGICAL GUIDES | Non-strict | They are surgical guides that only serve as an intraoperative reference but do not have a strip or hole where a cutting or drilling instrument can strictly perform active action on the patient. An example of this would be that a jaw is printed with the shape of the cut that is needed and that has the necessary measurements, but there is no guarantee that these measurements can be transported to the act of cutting. | |
| Strict | Non-functional | They have strips and holes that can be placed on the corresponding anatomy and effectively fixed, guaranteeing cuts and perforations as virtually planned. The contact between the active part of the cutting or drilling instrument has to be metal to metal to ensure tightness. | |
| Functional | When strict surgical guides are used, at the same time, a functional surgical–prosthetic result is planned. For example, airway or antagonist teeth ensure masticatory, swallowing, speech, and other stomatognathic functions in head and neck reconstructions. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salazar-Gamarra, R.; Contreras-Pulache, H.; Cruz-Gonzales, G.; Binasco, S.; Cruz-Gonzales, W.; Moya-Salazar, J. Three-Dimensional Printing and Digital Flow in Human Medicine: A Review and State-of-the-Art. Appl. Syst. Innov. 2022, 5, 126. https://doi.org/10.3390/asi5060126
Salazar-Gamarra R, Contreras-Pulache H, Cruz-Gonzales G, Binasco S, Cruz-Gonzales W, Moya-Salazar J. Three-Dimensional Printing and Digital Flow in Human Medicine: A Review and State-of-the-Art. Applied System Innovation. 2022; 5(6):126. https://doi.org/10.3390/asi5060126
Chicago/Turabian StyleSalazar-Gamarra, Rodrigo, Hans Contreras-Pulache, Gloria Cruz-Gonzales, Salvatore Binasco, William Cruz-Gonzales, and Jeel Moya-Salazar. 2022. "Three-Dimensional Printing and Digital Flow in Human Medicine: A Review and State-of-the-Art" Applied System Innovation 5, no. 6: 126. https://doi.org/10.3390/asi5060126