
Comparison of Models for 3D Printing of Solitary Fibrous Tumor Obtained Using Open-Source Segmentation Software

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient
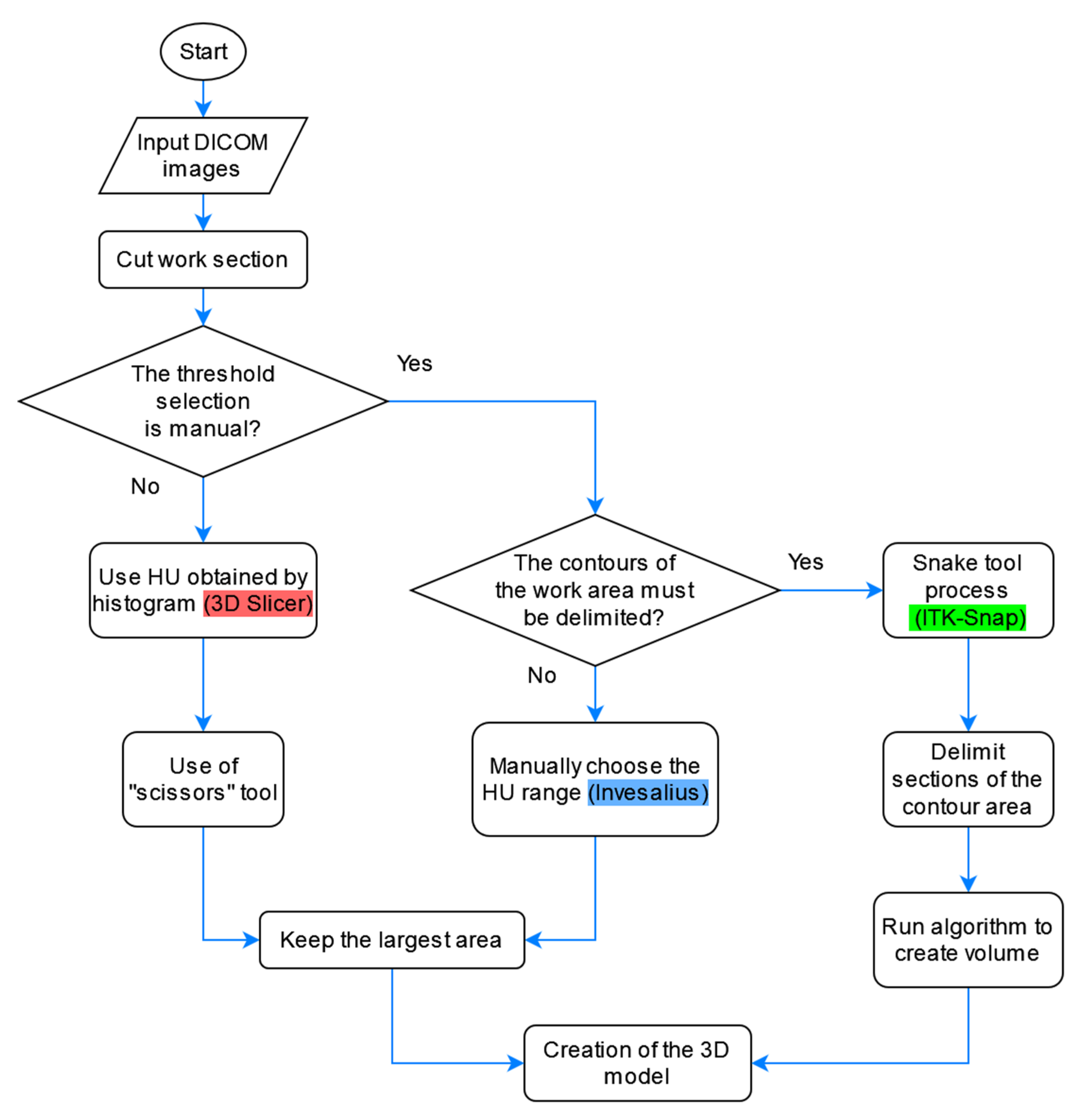
2.2. Software Selection
2.3. Segmentation Process of the Healthy Part of the Lung
2.3.1. 3D Slicer
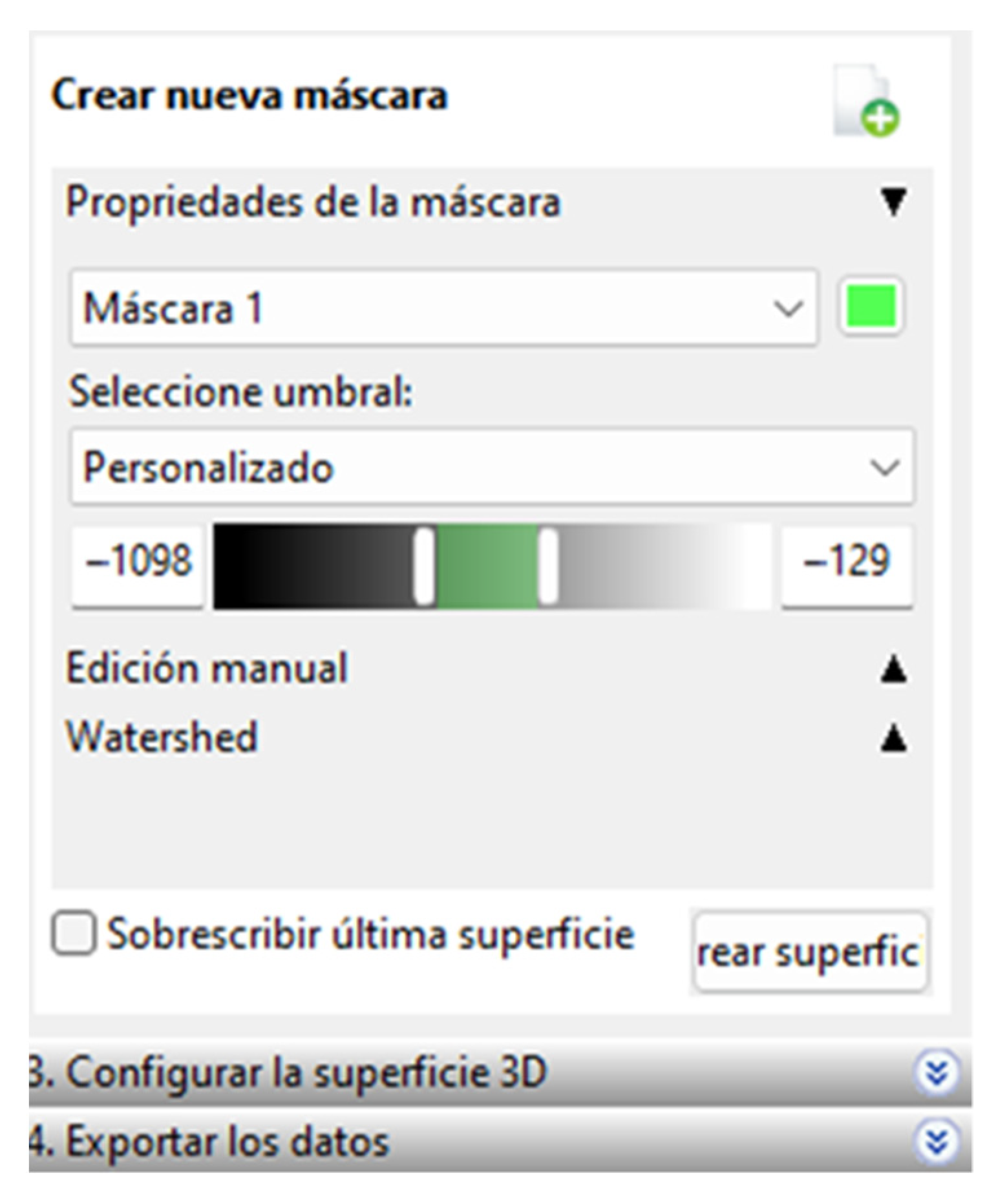
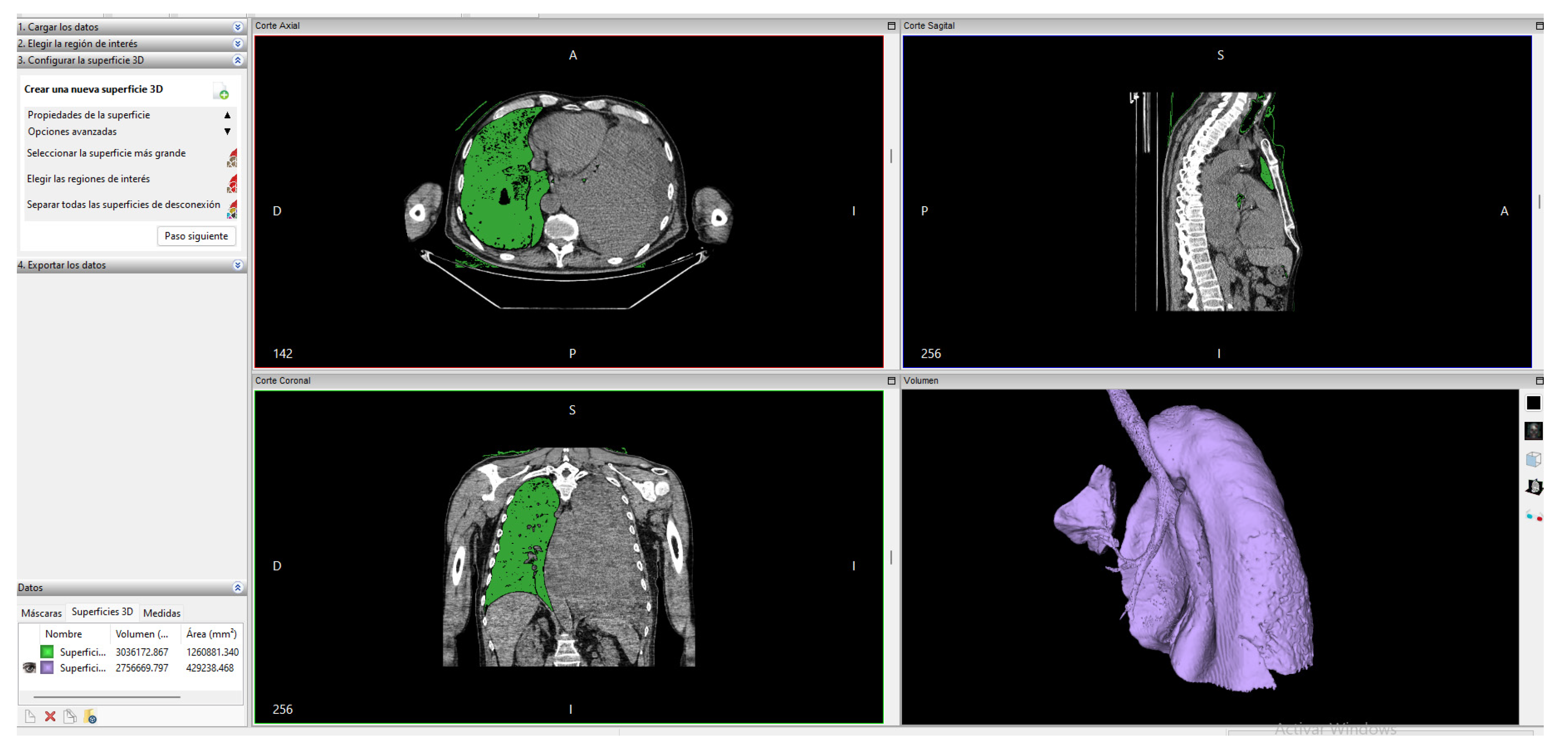
2.3.2. Invesalius
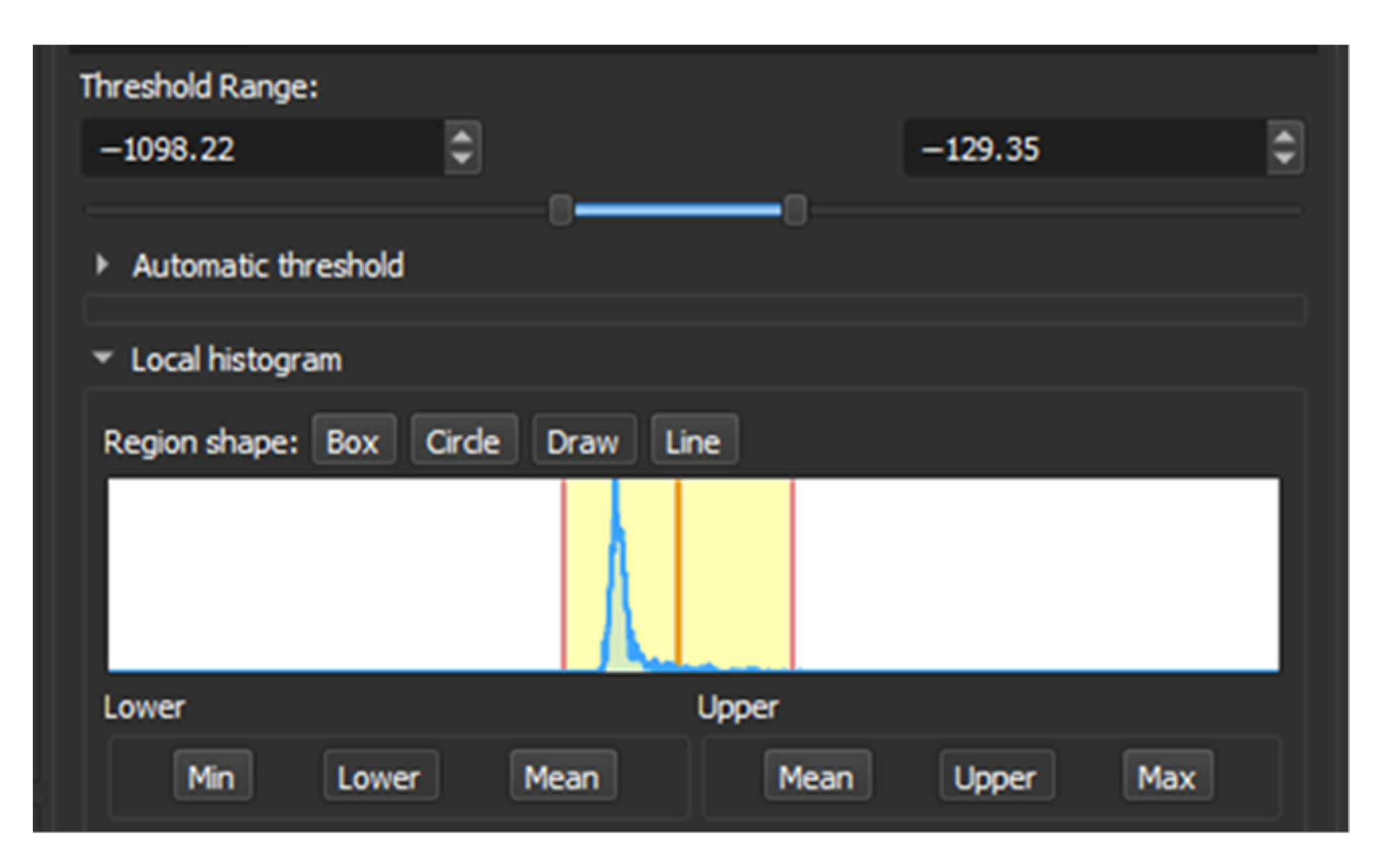
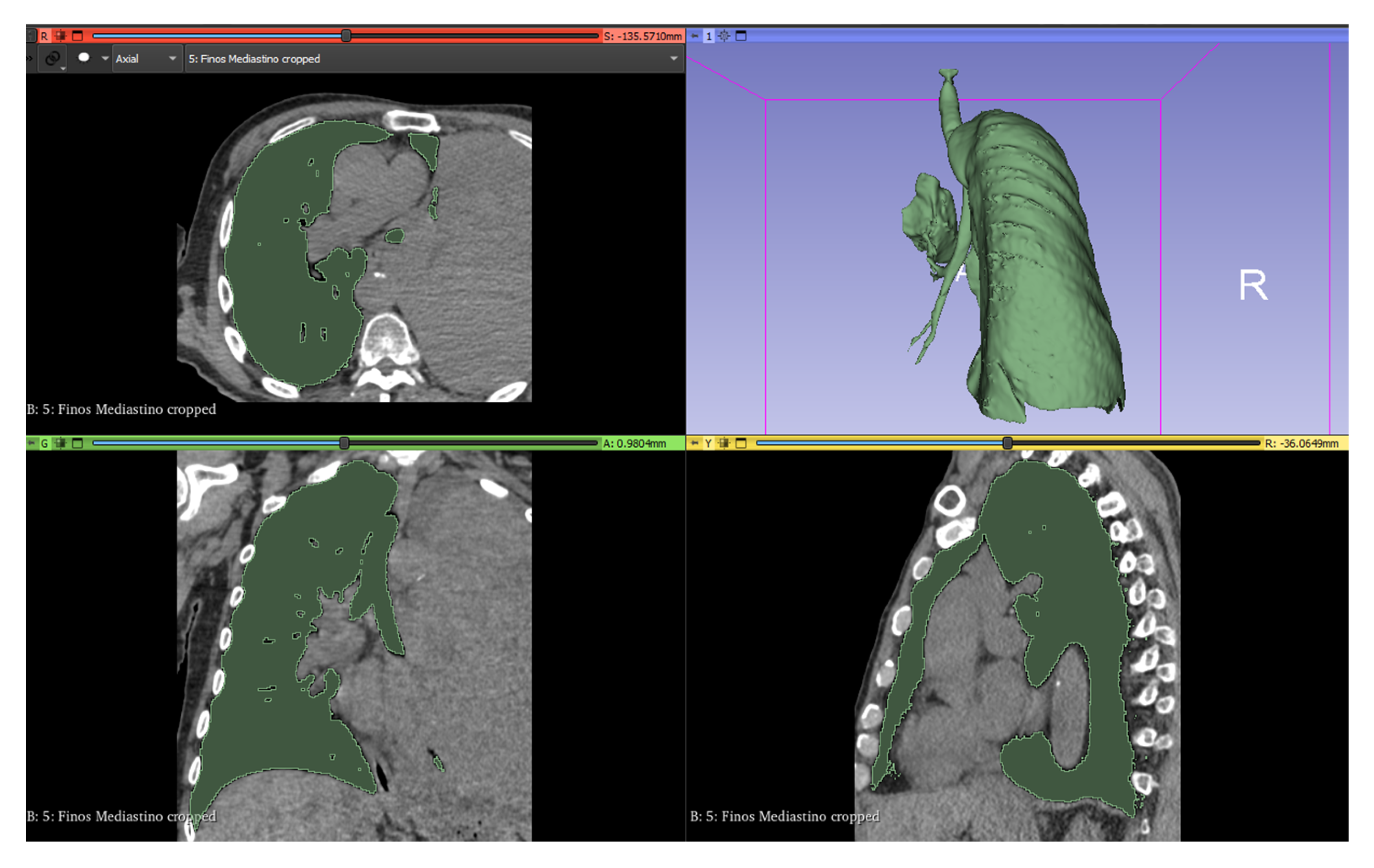
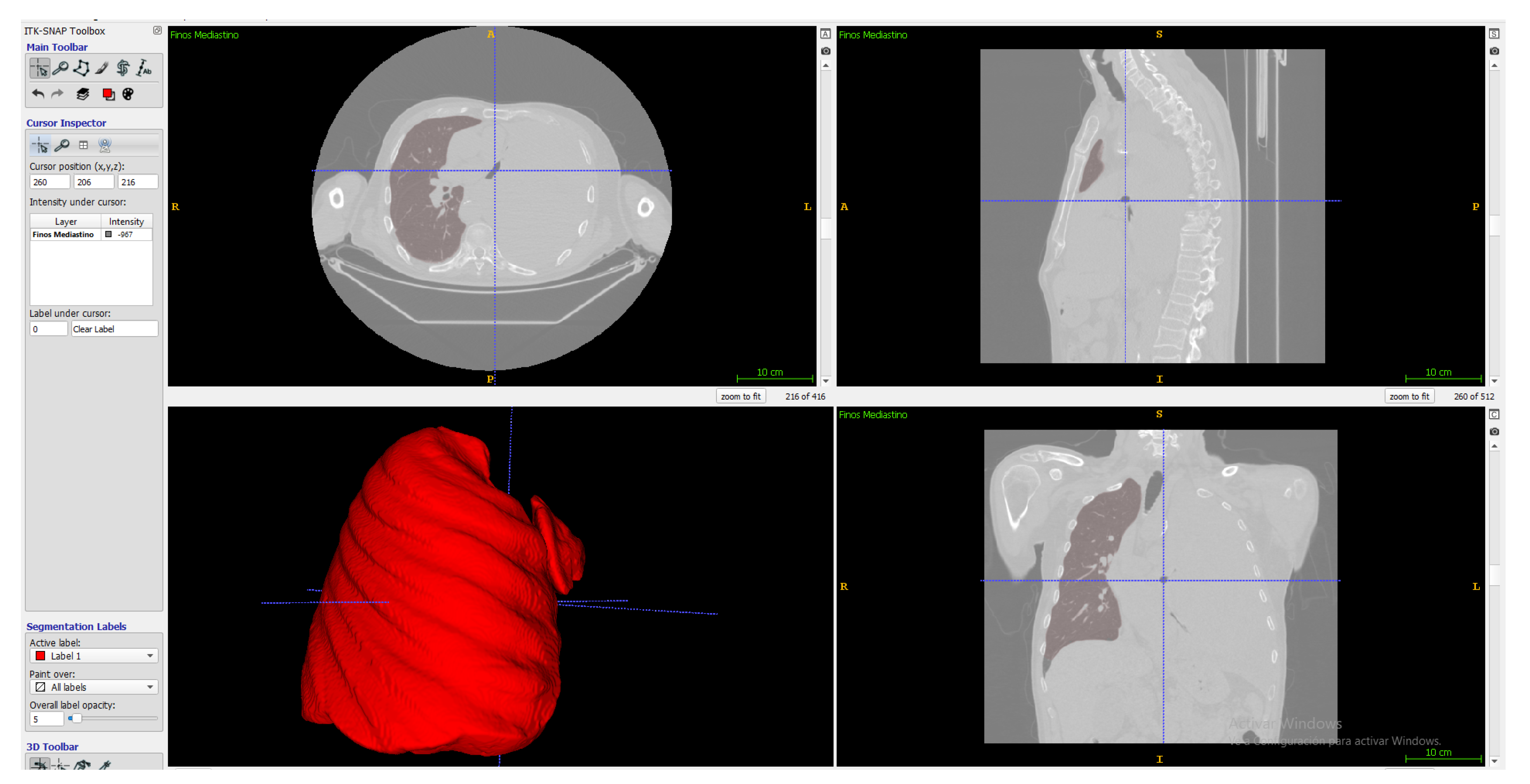
2.3.3. ITK-Snap
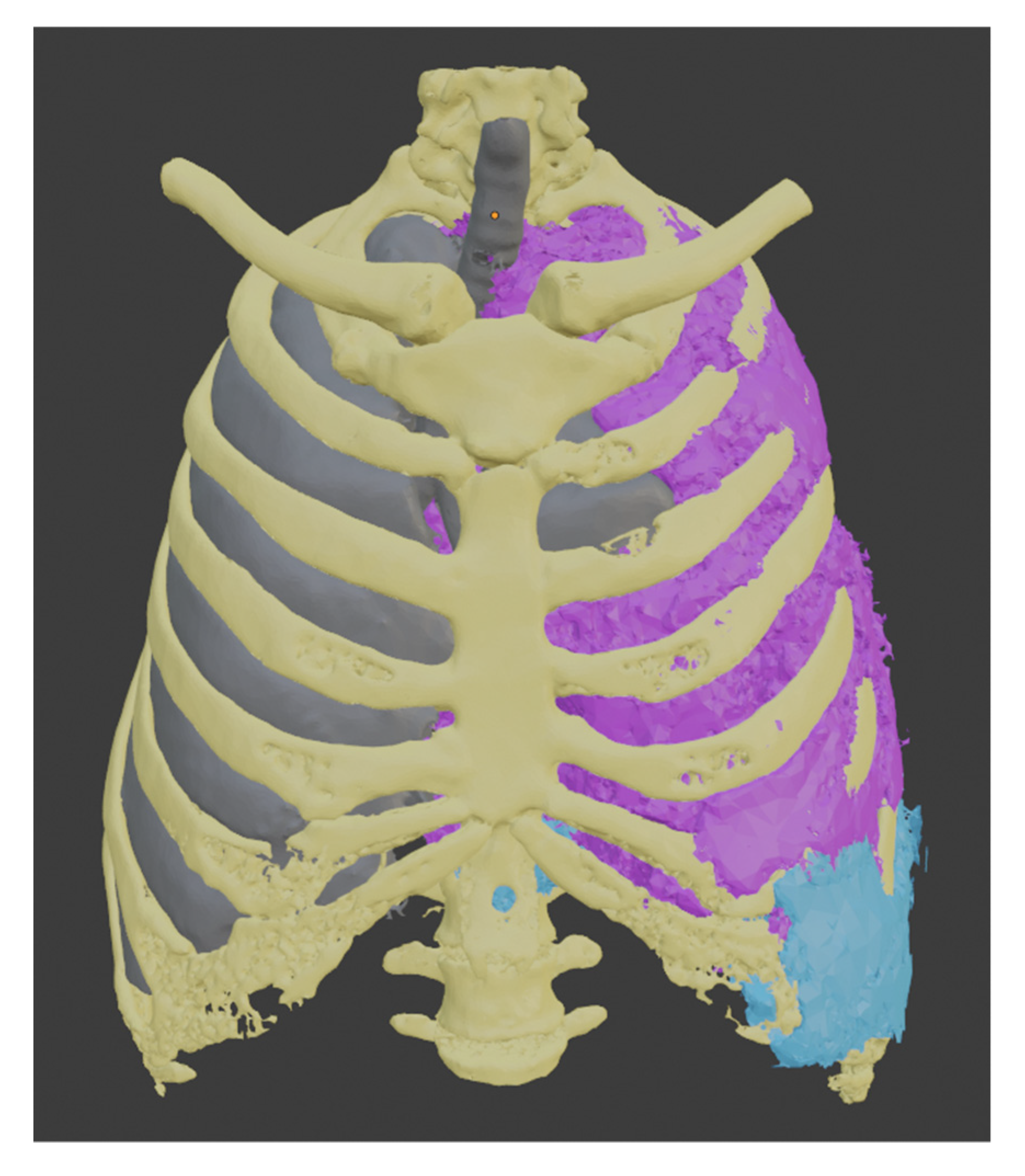
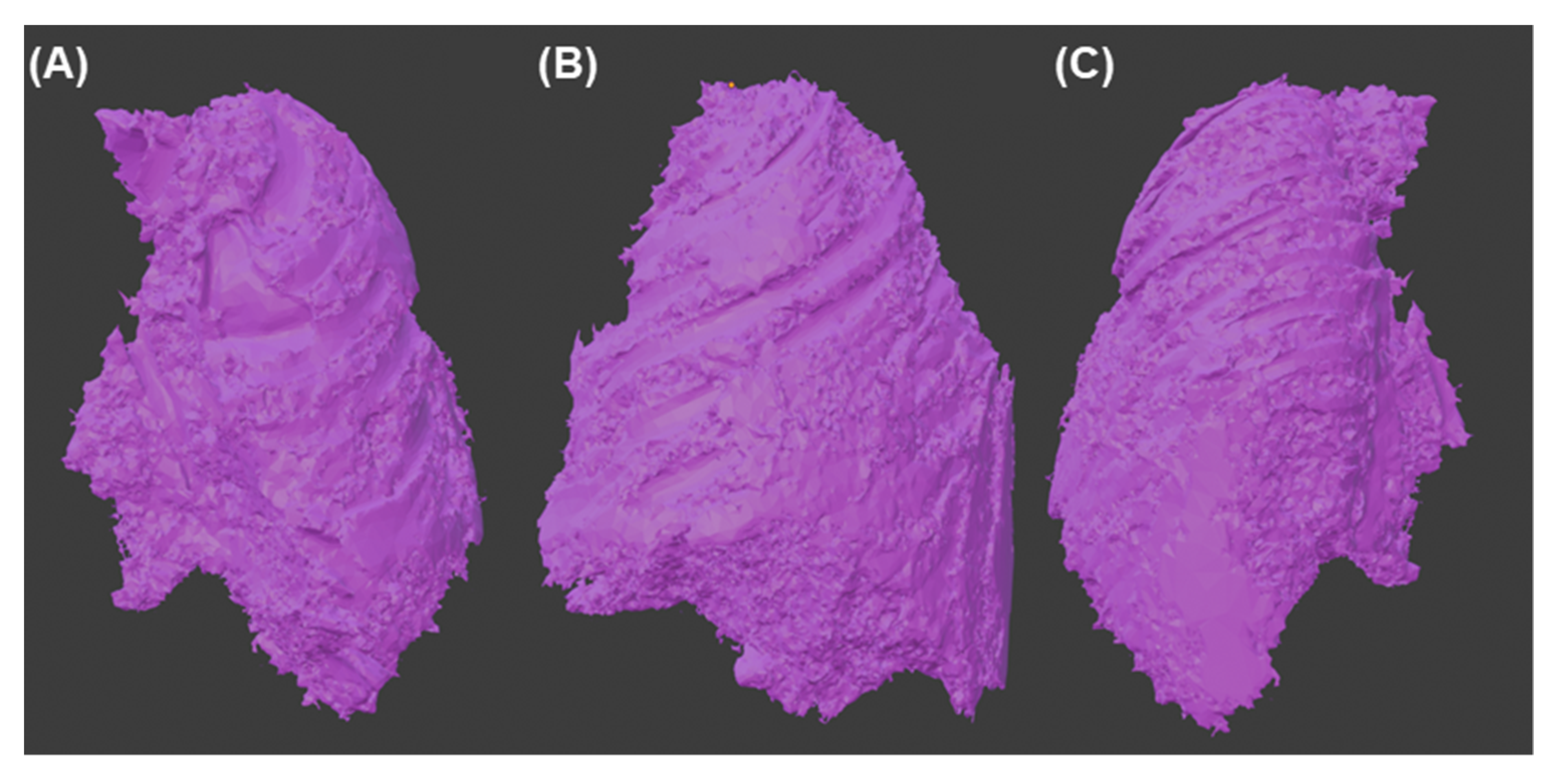
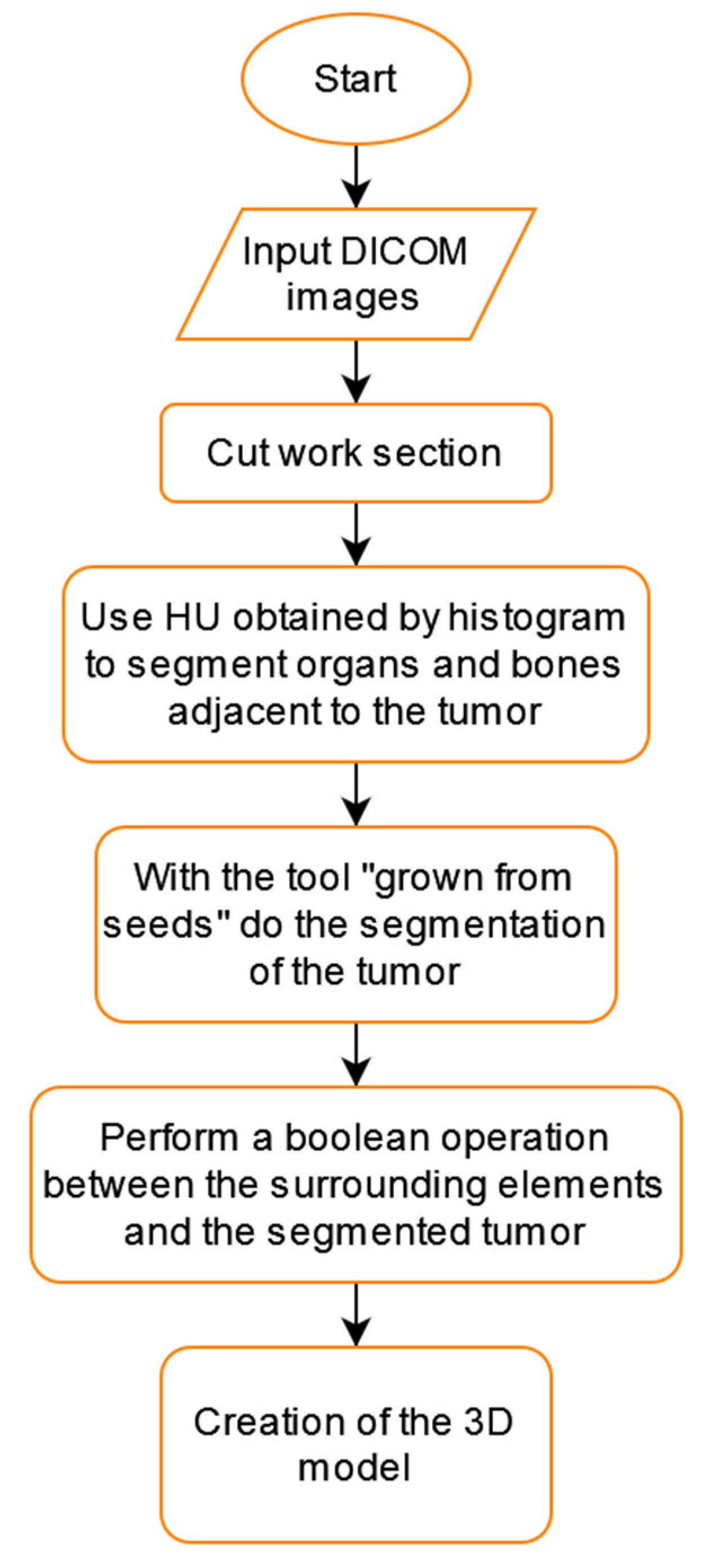
2.4. Tumor Segmentation Process
3. Results
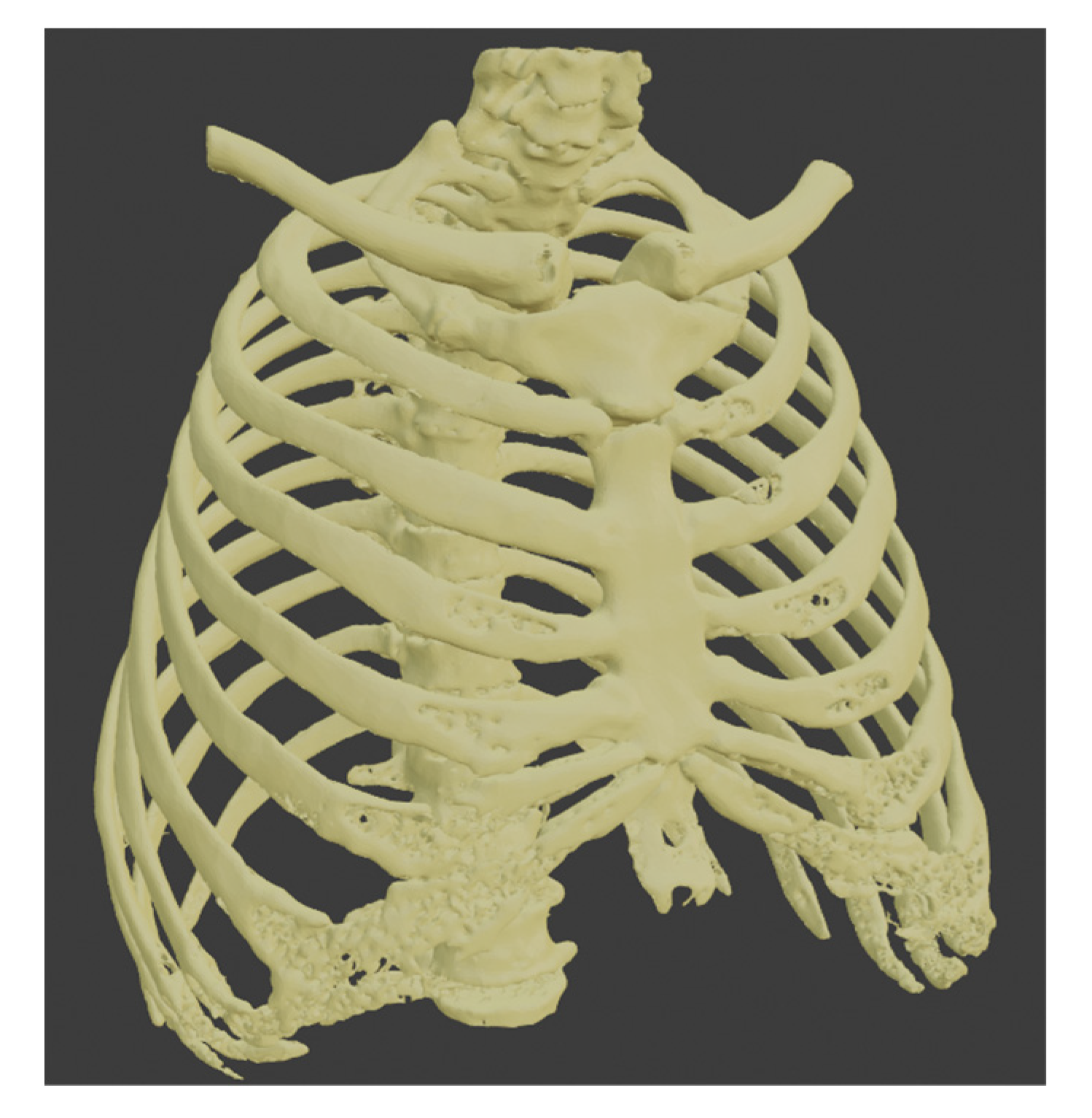
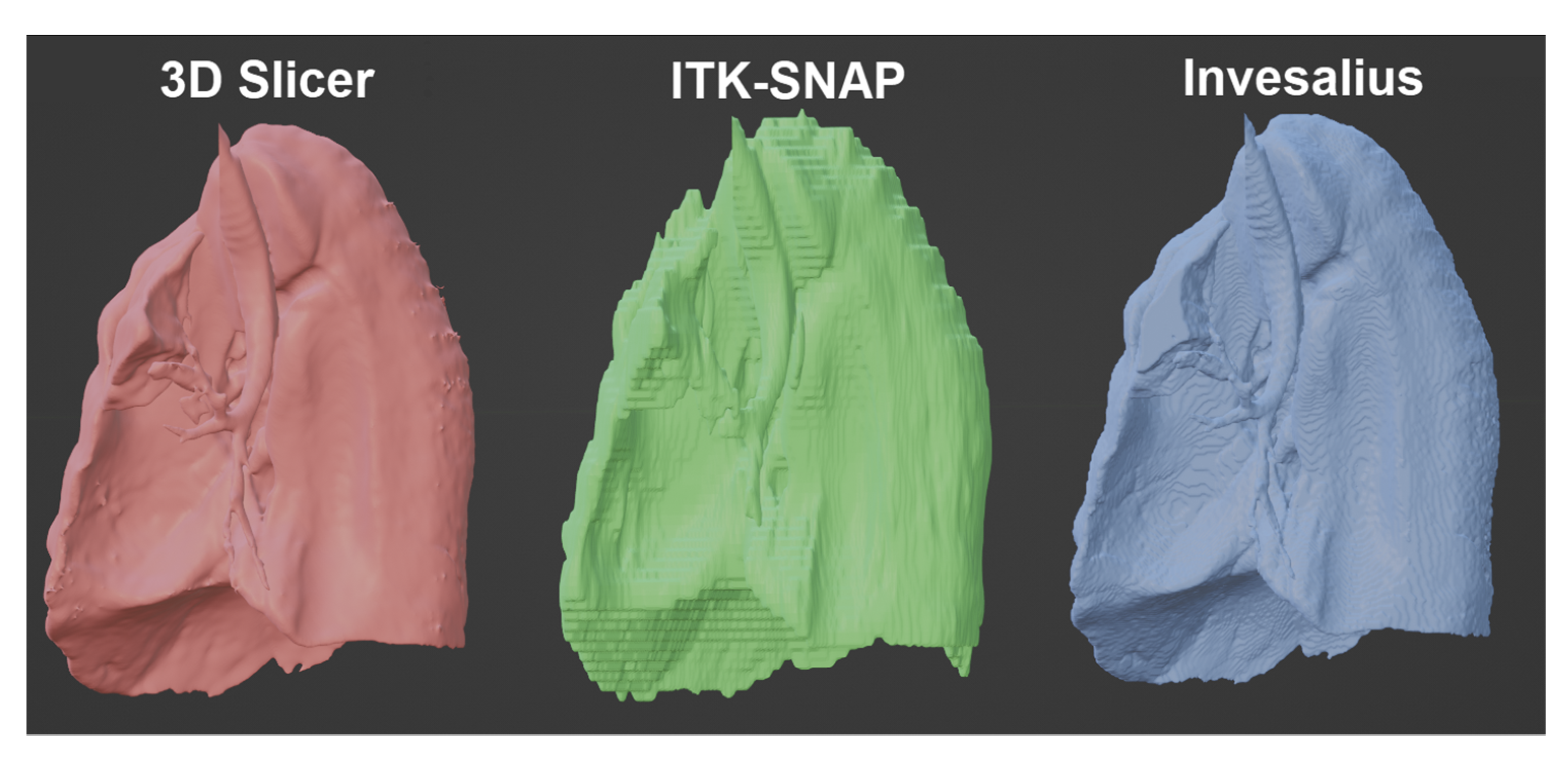
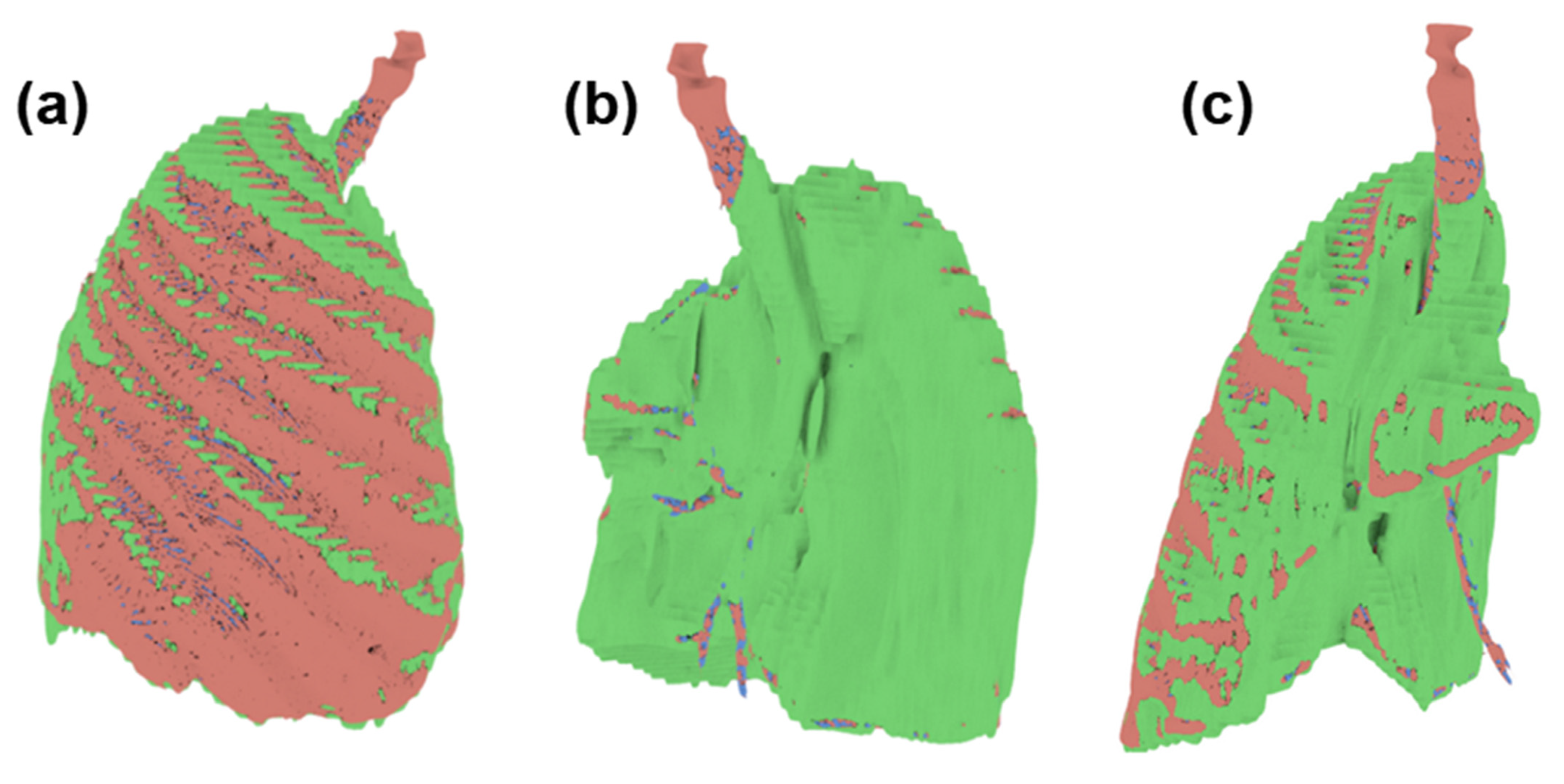
Comparison of the Models Obtained from the Healthy Part of the Lung
- -
- Intersect Face: 6272
- -
- Zero Faces: 21,941
- -
- Thin Faces: 2157
- -
- Sharp Edge: 3576
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.S.; Antonescu, C.R.; Hajdu, C.; Ferrone, C.R.; Hussain, M.; Lewis, J.J.; Brennan, M.F.; Coit, D.G. Clinicopathologic correlates of solitary fibrous tumors. Cancer 2002, 94, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Han, G.; Zhang, Z.; Shen, X.; Wang, K.; Zhao, Y.; He, J.; Gao, Y.; Shan, X.; Xin, G.; Li, C.; et al. Doege-Potter syndrome: A review of the literature including a new case report. Medicine 2017, 96, e7417. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Hinostroza, M.; Moya-Salazar, J.; Dávila, J.; Absencio, A.Y.; Contreras-Pulache, H. Doege-Potter syndrome due to endothoracic solitary hypoglycemic fibrous tumor. Clin. Case Rep. 2022, 10, e05611. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, T.; Ozcan, G.; Siddique, A.S.; Araneta, R.N., III; Slater, D.E.; Khan, A. Doege-Potter Syndrome with a Benign Solitary Fibrous Tumor: A Case Report and Literature Review. Case Rep. Oncol. 2021, 14, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-C.; Huang, H.-Y. Solitary fibrous tumor: An evolving and unifying entity with unsettled issues. Histol. Histopathol. 2019, 34, 313–334. [Google Scholar] [CrossRef] [PubMed]
- Badawy, M.; Nada, A.; Crim, J.; Kabeel, K.; Layfield, L.; Shaaban, A.; Elsayes, K.M.; Gaballah, A.H. Solitary fibrous tumors: Clinical and imaging features from head to toe. Eur. J. Radiol. 2022, 146, 110053. [Google Scholar] [CrossRef] [PubMed]
- Honnorat, J.; Antoine, J.-C. Paraneoplastic neurological syndromes. Orphanet J. Rare Dis. 2007, 2, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preim, B.; Botha, C. Chapter 4-Image Analysis for Medical Visualization. In Visual Computing for Medicine, 2nd ed.; Preim, B., Botha, C., Eds.; Morgan Kaufmann: Boston, MA, USA, 2014; pp. 111–175. ISBN 978-0-12-415873-3. [Google Scholar]
- Kim, J.J.; Nam, H.; Kaipatur, N.R.; Major, P.W.; Flores-Mir, C.; Lagravere, M.O.; Romanyk, D.L. Reliability and accuracy of segmentation of mandibular condyles from different three-dimensional imaging modalities: A systematic review. Dentomaxillofac. Radiol. 2020, 49, 20190150. [Google Scholar] [CrossRef] [PubMed]
- Matsiushevich, K.; Belvedere, C.; Leardini, A.; Durante, S. Quantitative comparison of freeware software for bone mesh from DICOM files. J. Biomech. 2019, 84, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Fyllingen, E.H.; Stensjøen, A.L.; Berntsen, E.M.; Solheim, O.; Reinertsen, I. Glioblastoma Segmentation: Comparison of Three Different Software Packages. PLoS ONE 2016, 11, e0164891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlíková, P.; Sochorová, L.; Snížková, O.; Malý, V.; Staněk, I. Solitary fibrous tumor of the pleura as a rare cause of severe hypoglycemia: Doege-Potter syndrome. Rozhl. V Chir. Mesic. Ceskoslovenske Chir. Spol. 2020, 99, 95–98. [Google Scholar] [CrossRef]
- Flores Cruz, G.; Aguila Gómez, M.V.; Lazo Vargas, A.; Alarcón Delgado, M.M.; Luna Catari, M.K.; Marconi Poma, E.R. Síndrome de Doege-Potter, Tumor Fibroso Solitario Endotorácico Hipoglicemiante, ¿Cuando y Cómo lo Diagnóstico? y ¿Cual es mi Conducta Final?: Presentación de un Caso y Revisión de la Literatura. Rev. Médica Paz 2019, 25, 48–57. [Google Scholar]
- Estradioto, L.; de Araujo, R.B.; Neto, N.B.; de Araújo, V.B.; Coelho, M.d.S.; da Silva, L.L.G. Doege-Potter syndrome: A rare presentation of a solitary fibrous tumor of the pleura. Braz. J. Oncol. 2021, 17, 1–4. [Google Scholar] [CrossRef]
- Meng, W.; Zhu, H.-H.; Li, H.; Wang, G.; Wei, D.; Feng, X. Solitary fibrous tumors of the pleura with Doege-Potter syndrome: A case report and three-decade review of the literature. BMC Res. Notes 2014, 7, 515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes de Oliveira Santos, B.; Silva da Costa, M.D.; Centeno, R.S.; Cavalheiro, S.; Antônio de Paiva Neto, M.; Lawton, M.T.; Chaddad-Neto, F. Clinical Application of an Open-Source 3D Volume Rendering Software to Neurosurgical Approaches. World Neurosurg. 2018, 110, e864–e872. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.; Wang, J.; Yao, J.; Hang, F.; Lei, X.; Cao, Y. Three-dimensional image reconstruction with free open-source OsiriX software in video-assisted thoracoscopic lobectomy and segmentectomy. Int. J. Surg. Lond. Engl. 2017, 39, 16–22. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 3D Slicer | ITK-Snap | Invesalius | |
|---|---|---|---|
| Volume (mm3) | 3,113,176.6472 | 3,340,029.03 | 3,021,873.5068 |
| Volume (cm3) | 3113.17 | 3340.02 | 3021.87 |
| Triangles | 810,194 | 244,149 | 472,749 |
| Faces | 809,595 | 244,149 | 471,671 |
| Edges | 1,214,692 | 366,334 | 708,046 |
| Vertices | 405,851 | 122,189 | 235,907 |
| Size (Mb) | 39.9 | 41.7 | 23.2 |
| Non-Manifold edge | 0 | 0 | 3 |
| Bad contig edges | 0 | 0 | 4 |
| Intersect face | 2992 | 0 | 0 |
| Zero faces | 7443 | 0 | 4 |
| Zero edges | 10 | 0 | 0 |
| Thin faces | 4523 | 11 | 35 |
| Sharp edge | 757 | 11 | 29 |
| Time-consuming | 3 min 40 s | 3 min 5 s | 5 min 32 s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tincopa, J.P.; Salazar-Gamarra, R.; Lopez-Hinostroza, M.; Moya-Salazar, B.; Contreras-Pulache, H.; Moya-Salazar, J. Comparison of Models for 3D Printing of Solitary Fibrous Tumor Obtained Using Open-Source Segmentation Software. Appl. Syst. Innov. 2022, 5, 116. https://doi.org/10.3390/asi5060116
Tincopa JP, Salazar-Gamarra R, Lopez-Hinostroza M, Moya-Salazar B, Contreras-Pulache H, Moya-Salazar J. Comparison of Models for 3D Printing of Solitary Fibrous Tumor Obtained Using Open-Source Segmentation Software. Applied System Innovation. 2022; 5(6):116. https://doi.org/10.3390/asi5060116
Chicago/Turabian StyleTincopa, Jean Pierre, Rodrigo Salazar-Gamarra, Madaleine Lopez-Hinostroza, Belén Moya-Salazar, Hans Contreras-Pulache, and Jeel Moya-Salazar. 2022. "Comparison of Models for 3D Printing of Solitary Fibrous Tumor Obtained Using Open-Source Segmentation Software" Applied System Innovation 5, no. 6: 116. https://doi.org/10.3390/asi5060116