
COVID-19 Acute Respiratory Distress Syndrome: Treatment with Helmet CPAP in Respiratory Intermediate Care Unit by Pulmonologists in the Three Italian Pandemic Waves
 , and
, and
Abstract
:Highlights
- Good clinical outcomes with H-CPAP in RICU, especially in mild and moderate CARDS.
- Significant improvement of prognosis in the three different waves: patients’ diseases were found to be progressively slightly less severe. (No patient had yet received at least one dose of vaccination against COVID-19.)
- H-CPAP success strongly correlates with worst PaO2/FiO2 ratio and D-dimer level at admission.
- Relevance of proper management during hospitalization by pulmonologists in RICU.
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Clinical Procedures and Monitoring
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographic, Clinical and Outcomes Assessments across the Three Waves
3.2. Complications
3.3. Predictors of the H-CPAP Success and Survival/Death Outcomes
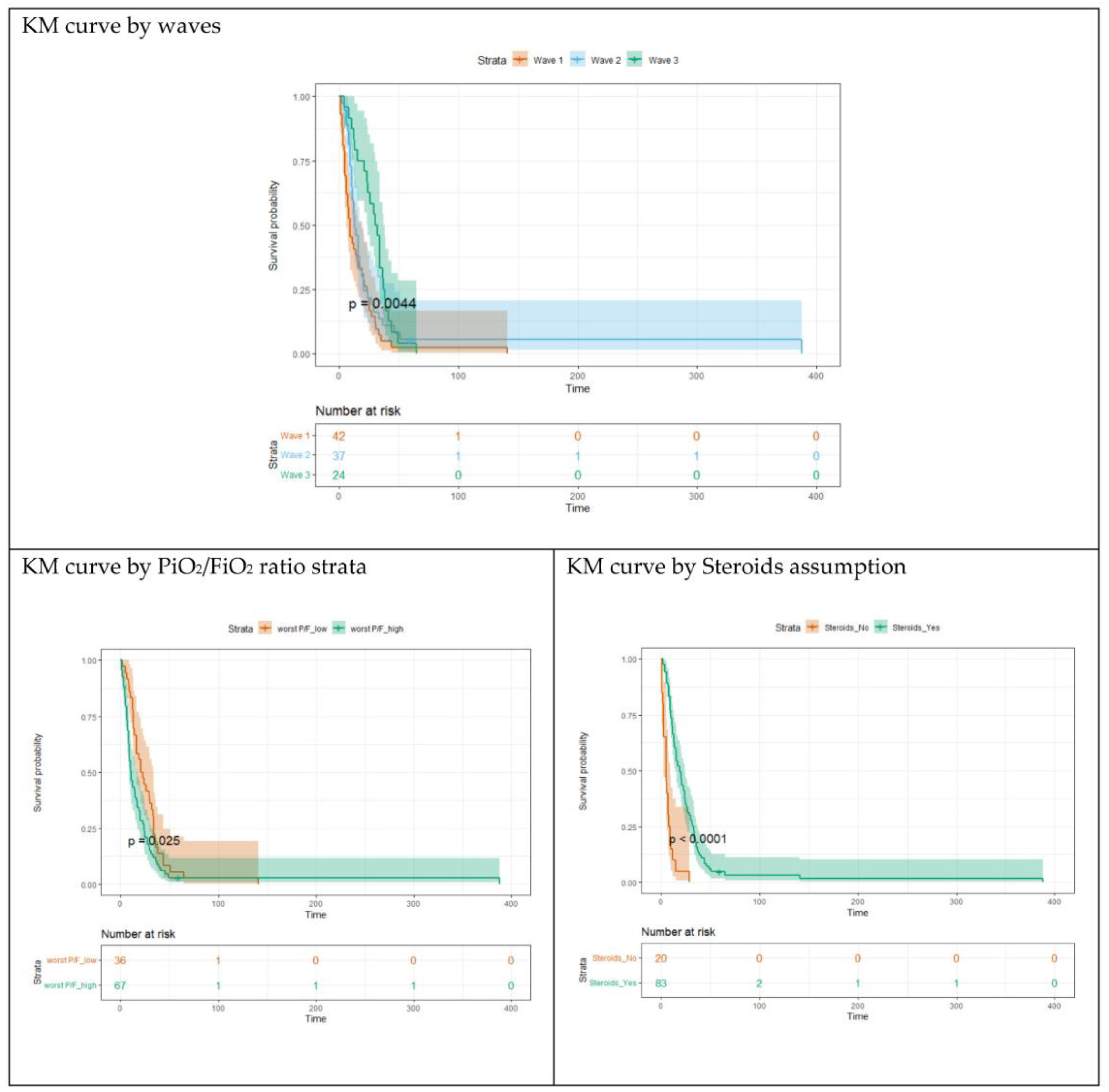
3.4. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ren, L.-L.; Wang, Y.-M.; Wu, Z.-Q.; Xiang, Z.-C.; Guo, L.; Xu, T.; Jiang, Y.-Z.; Xiong, Y.; Li, Y.-J.; Li, X.-W.; et al. Identification of a novel coronavirus causing severe pneumonia in human: A descriptive study. Chin. Med. J. 2020, 133, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 NovelCoronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality Among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Grassi, A.; Foti, G.; Laffey, J.G.; Bellani, G. Noninvasive mechanical ventilation in early acute respiratory distress syndrome. Pol. Arch. Intern. Med. 2017, 127, 614–620. [Google Scholar] [CrossRef]
- Demoule, A.; Hill, N.; Navalesi, P. Can we prevent intubation in patients with ARDS? Intensive Care Med. 2016, 42, 768–771. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef]
- Brambilla, A.M.; Aliberti, S.; Prina, E.; Nicoli, F.; Del Forno, M.; Nava, S.; Ferrari, G.; Corradi, F.; Pelosi, P.; Bignamini, A.; et al. Helmet CPAP vs. oxygen therapy in severe hypoxemic respiratory failure due to pneumonia. Intensiv. Care Med. 2014, 40, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Cosentini, R.; Brambilla, A.M.; Aliberti, S.; Bignamini, A.; Nava, S.; Maffei, A.; Martinotti, R.; Tarsia, P.; Monzani, V.; Pelosi, P. Faculty Opinions recommendation of Helmet continuous positive airway pressure vs oxygen therapy to improve oxygenation in community-acquired pneumonia: A randomized, controlled trial. Chest 2010, 138, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Brochard, L.; Marini, J.J.; Slutsky, A.S.; Mancebo, J.; Ranieri, V.M.; Thompson, B.T.; Papazian, L.; Schultz, M.J.; Amato, M.; et al. Respiratory support in patients with acute respiratory distress syndrome: An expert opinion. Crit. Care 2017, 21, 240. [Google Scholar] [CrossRef] [PubMed]
- Sakuraya, M.; Okano, H.; Masuyama, T.; Kimata, S.; Hokari, S. Efficacy of non-invasive and invasive respiratory management strategies in adult patients with acute hypoxaemic respiratory failure: A systematic review and network meta-analysis. Crit. Care 2021, 25, 414. [Google Scholar] [CrossRef]
- Ferreyro, B.L.; Angriman, F.; Munshi, L.; Del Sorbo, L.; Ferguson, N.D.; Rochwerg, B.; Ryu, M.J.; Saskin, R.; Wunsch, H.; da Costa, B.R.; et al. Association of Noninvasive Oxygenation Strategies with All-Cause Mortality in Adults with Acute Hypoxemic Respiratory Failure: A Systematic Review and Me-ta-analysis. JAMA 2020, 324, 57–67. [Google Scholar] [CrossRef]
- Patel, B.K.; Wolfe, K.S.; Pohlman, A.S.; Hall, J.B.; Kress, J.P. Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients with Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2016, 315, 2435–2441. [Google Scholar] [CrossRef]
- Ferioli, M.; Cisternino, C.; Leo, V.; Pisani, L.; Palange, P.; Nava, S. Protecting healthcare workers from SARS-CoV-2 infection: Practical indications. Eur. Respir. Rev. 2020, 29, 200068. [Google Scholar] [CrossRef]
- Ferrer, M.; Esquinas, A.; Leon, M.; Gonzalez, G.; Alarcon, A.; Torres, A. Noninvasive ventilation in severe hypoxemic respiratory failure: A randomized clinical trial. Am. J. Respir. Crit. Care Med. 2003, 168, 1438–1444. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S; Springer: Berlin, Germany, 2002. [Google Scholar] [CrossRef]
- The Recovery Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Confalonieri, M.; Urbino, R.; Potena, A.; Piattella, M.; Parigi, P.; Puccio, G.; Della Porta, R.; Giorgio, C.; Blasi, F.; Umberger, R.; et al. Hydrocortisone infusion for severe communi-ty-acquired pneumonia: A preliminary randomized study. Am. J. Respir. Crit. Care Med. 2005, 171, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Santus, P.; Radovanovic, D.; Saderi, L.; Marino, P.; Cogliati, C.; De Filippis, G.; Rizzi, M.; Franceschi, E.; Pini, S.; Giuliani, F.; et al. Severity of respiratory failure at admission and in-hospital mortality in patients with COVID-19: A prospective observational multicentre study. BMJ Open 2020, 10, e043651. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Cao, J.; Wang, Q.; Shi, Q.; Liu, K.; Luo, Z.; Chen, X.; Chen, S.; Yu, K.; Huang, Z.; et al. D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: A case control study. J. Intensiv. Care 2020, 8, 49. [Google Scholar] [CrossRef]
- Gattinoni, L.; Coppola, S.; Cressoni, M.; Busana, M.; Rossi, S.; Chiumello, D. COVID-19 Does Not Lead to a “Typical” Acute Res-piratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 201, 1299–1300. [Google Scholar] [CrossRef] [PubMed]
- Dhont, S.; Derom, E.; Van Braeckel, E.; Depuydt, P.; Lambrecht, B.N. The pathophysiology of “happy” hypoxemia in COVID. Respir. Res. 2020, 21, 198. [Google Scholar] [CrossRef]
- Han, R.; Huang, L.; Jiang, H.; Dong, J.; Peng, H.; Zhang, D. Early Clinical and CT Manifestations of Coronavirus Disease 2019 (COVID-19) Pneumonia. Am. J. Roentgenol. 2020, 215, 338–343. [Google Scholar] [CrossRef]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensive Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef]
- Chiumello, D.; Esquinas, A.M.; Moerer, O.; Terzi, N. A systematic technical review of the systems for the continuous positive airway pressure. Minerva Anestesiol. 2012, 78, 1385–1393. [Google Scholar]
- Fazzini, B.; Page, A.; Pearse, R.; Puthucheary, Z. Prone positioning for non-intubated spontaneously breathing patients with acute hypoxaemic respiratory failure: A systematic review and meta-analysis. Br. J. Anaesth. 2021, 128, 352–362. [Google Scholar] [CrossRef]
- Longhini, F.; Bruni, A.; Garofalo, E.; Navalesi, P.; Grasselli, G.; Cosentini, R.; Foti, G.; Mattei, A.; Ippolito, M.; Accurso, G.; et al. Helmet continuous positive airway pressure and prone positioning: A proposal for an early management of COVID-19 patients. Pulmonology 2020, 26, 186–191. [Google Scholar] [CrossRef]
- Radovanovic, D.; Rizzi, M.; Pini, S.; Saad, M.; Chiumello, D.A.; Santus, P. Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal. J. Clin. Med. 2020, 9, 1191. [Google Scholar] [CrossRef] [PubMed]
- Ing, R.J.; Bills, C.; Merritt, G.; Ragusa, R.; Bremner, R.M.; Bellia, F. Role of Helmet-Delivered Noninvasive Pressure Support Ventilation in COVID-19 Patients. J. Cardiothorac. Vasc. Anesthesia 2020, 34, 2575–2579. [Google Scholar] [CrossRef]
- Piluso, M.; Scarpazza, P.; Oggionni, E.; Celeste, A.; Bencini, S.; Bernareggi, M.; Bonacina, C.; Cattaneo, R.; Melacini, C.; Raschi, S.; et al. Helmet Continuous Positive Airway Pressure in COVID-19 Related Acute Respiratory Distress Syndrome in Respiratory Intermediate Care Unit. Austin J. Infect. Dis. 2021, 8, 1061. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Hentschker, C.; Westhoff, M.; Weber-Carstens, S.; Janssens, U.; Kluge, S.; Pfeifer, M.; Spies, C.; Welte, T.; Rossaint, R.; et al. Observational study of changes in utilization and outcomes in mechanical ventilation in COVID-19. PLoS ONE 2022, 17, e0262315. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Tobin, M.J. Basing Respiratory Management of COVID-19 on Physiological Principles. Am. J. Respir. Crit. Care Med. 2020, 201, 1319–1320. [Google Scholar] [CrossRef]
- Matthay, M.A.; Arabi, Y.; Arroliga, A.C.; Bernard, G.; Bersten, A.D.; Brochard, L.J.; Calfee, C.S.; Combes, A.; Daniel, B.M.; Ferguson, N.D.; et al. A New Global Definition of Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2023; ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Wave1 Mean [Median] (SD) N = 150 | Wave2 Mean [Median] (SD) N = 180 | Wave3 Mean [Median] (SD) N = 185 | Tot | p-Value | Post Hoc |
|---|---|---|---|---|---|---|
| Socio-demographic features | ||||||
| Age | 61.9 [63.3] (10.8) | 63.5 [65] (10.9) | 62.2 [64] (11.2) | 515 | 0.316 | |
| Sex | ||||||
| Females | N = 27; 24.3% | N = 38; 34.2% | N = 46; 41.4% | 111 | 0.310 | |
| Males | N = 123; 30.4% | N = 142; 35.1% | N = 139; 34.7% | 404 | ||
| Body Mass Index (BMI) | 29.4 [29.4] (4.7) | 30.2 [29] (6.6) | 29.7 [29] (4.7) | 361 | 0.847 | |
| Smoke | ||||||
| No | N = 104; 39.2% | N = 69; 26% | N = 92; 34.7% | 265 | <0.001 | 1 vs. 2,3 |
| Yes | N = 1; 4.2% | N = 8; 33.5% | N = 15; 62.5% | 24 | ||
| Ex-smokers | N = 45; 26% | N= 65; 37.6% | N = 63; 36.4% | 173 | ||
| Comorbidity and prognostic score | ||||||
| Hypertension | ||||||
| No | N = 78; 32.9% | N = 74; 31.2% | N = 85; 35.9% | 237 | 0.142 | |
| Yes | N = 72; 25.9% | N = 106; 38.1% | N = 100; 36% | 278 | ||
| Ischemic cardiac disease | ||||||
| No | N = 132; 29.7% | N = 150; 33.8% | N = 163; 36.5% | 445 | 0.349 | |
| Yes | N = 15; 25% | N = 26; 43.3% | N = 19; 31.7% | 60 | ||
| Cardiovascular disease | ||||||
| No | N = 129; 30.3% | N = 144; 33.8% | N = 153; 35.9% | 426 | 0.357 | |
| Yes | N = 21; 23.6% | N = 36; 40.4% | N = 32; 36% | 89 | ||
| Hypercholesterolemia | ||||||
| No | N = 122; 28.3% | N = 152; 35.3% | N = 157; 36.4% | 431 | 0.646 | |
| Yes | N = 28; 33.3% | N = 28; 33.3% | N = 28; 33.3% | 84 | ||
| Diabetes | ||||||
| No | N = 139; 32.7% | N = 136; 32% | N = 150; 35.3% | 425 | <0.001 | 1 vs. 2,3 |
| Yes | N = 11; 12.2% | N = 44; 48.9% | N = 35; 38.9% | 90 | ||
| Neoplasia | ||||||
| No | N = 144; 31% | N = 149; 32.1% | N = 171; 36.9% | 464 | <0.001 | 2 vs. 1,3 |
| Yes | N = 6; 11.8% | N = 31; 60.8% | N = 14; 27.5% | 51 | ||
| Chronic obstructive pulmonary disease (COPD)/asthma | ||||||
| No | N = 136; 29.4% | N = 158; 34.2% | N = 168; 36.4% | 462 | 0.571 | |
| Yes | N = 14; 26.4% | N = 22; 41.5% | N = 17; 32.1% | 53 | ||
| Chronic renal failure | ||||||
| No | N = 149; 30.5% | N = 164; 33.6% | N = 175; 35.9% | 488 | 0.004 | 1 vs. 2,3 |
| Yes | N = 1; 3.7% | N = 16; 59.3% | N = 10; 37% | 27 | ||
| Apache II score | 10.6 [10] (3.6) | 10.3 [11] (5.0) | 9.7 [10] (4.3) | 513 | 0.110 | |
| Variables | Wave1 Mean [Median] (SD) N = 150 | Wave2 Mean [Median] (SD) N = 180 | Wave3 Mean [Median] (SD) N = 185 | Tot | p-Value | Post Hoc |
|---|---|---|---|---|---|---|
| Pharmacological treatment during hospitalization | ||||||
| Antivirals | ||||||
| No | N = 46; 11.3% | N = 176; 43.3% | N = 184; 45.3% | 406 | <0.001 | 1 vs. 2,3 |
| Yes | N = 104; 95.4% | N = 4; 3.7% | N = 1; 0.9% | 109 | ||
| Remdesivir | ||||||
| No | N = 146; 29% | N = 177; 35.1% | N = 181; 35.9% | 504 | 0.822 | |
| Yes | N = 4; 36.4% | N = 3; 27.3% | N = 4; 36.4% | 11 | ||
| Azithromycin | ||||||
| No | N = 113; 43.6% | N = 70; 27.0% | N = 76; 29.3% | 259 | <0.001 | 1 vs. 2,3 |
| Yes | N = 37; 14.5% | N = 110; 43% | N = 109; 42.6% | 256 | ||
| Tocilizumab | ||||||
| No | N = 139; 27.6% | N= 180; 35.7% | N = 185; 36.7% | 504 | <0.001 | 1 vs. 2,3 |
| Yes | N = 11; 100% | N = 0; 0% | N = 0; 0% | 11 | ||
| Plaquenil | ||||||
| No | N = 5; 1.4% | N= 180; 48.6% | N = 185; 50% | 370 | <0.001 | 1 vs. 2,3 |
| Yes | N = 145; 100% | N = 0; 0% | N = 0; 0% | 145 | ||
| Steroids | ||||||
| No | N = 32; 86.5% | N = 4; 10.8% | N = 1; 2.7% | 37 | <0.001 | 1 vs. 2,3 |
| Yes | N = 118; 24.7% | N = 176; 36.8% | N = 184; 38.5% | 478 | ||
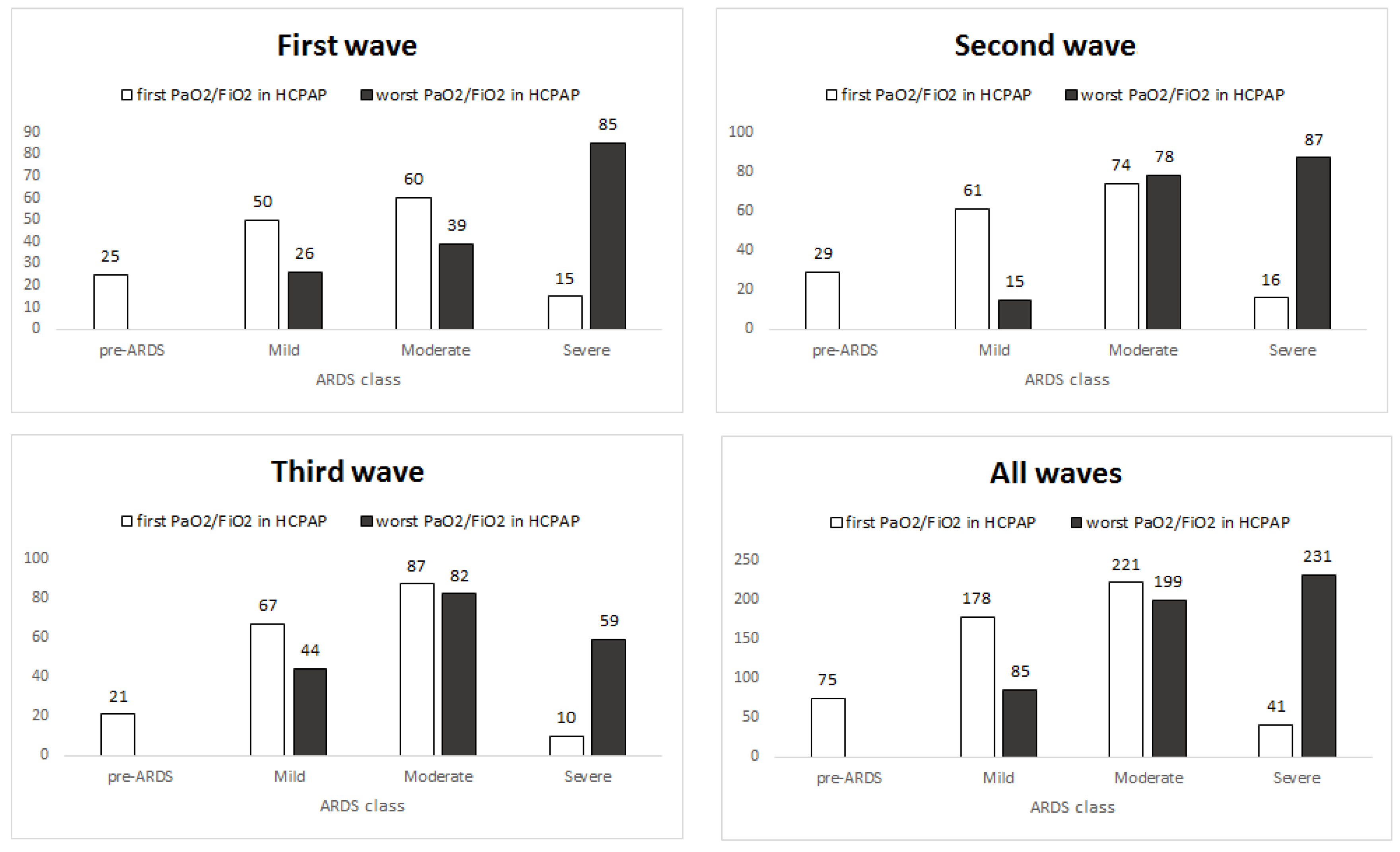
| COVID-19 Acute Respiratory Distress Syndrome (CARDS) classes at admission and Intensive Care Unit (ICU) transfer | ||||||
| CARDS classes (admission) | ||||||
| Pre-CARDS | N = 25; 33.3% | N = 29; 38.7% | N = 21; 28% | 75 | 0.486 | |
| Mild | N = 50; 28.1% | N = 61; 34.3% | N = 67; 37.6% | 178 | ||
| Moderate | N = 60; 27.1% | N = 74; 33.5% | N= 87; 39.4% | 221 | ||
| Severe | N = 15; 36.6% | N = 16; 39% | N = 10; 24.4% | 41 | ||
| Intensive Care Unit | ||||||
| No | N = 118; 28.6% | N = 143; 34.7% | N = 151; 36.7% | 412 | 0.777 | |
| Yes | N = 32; 31.1% | N = 37; 35.9% | N = 34; 33% | 103 | ||
| Blood tests | ||||||
| D-dimer test (admission) (ng/mL) | 3629.8 [630] (9423) | 586.6 [296] (1521) | 443.2 [288] (919) | 502 | <0.001 | 1 vs. 2,3 |
| D-dimer test (worst) (ng/mL) | 6939.2 [2067] (12382) | 3571.9 [1049] (9468) | 2447 [719] (5054) | 503 | <0.001 | 1 vs. 2,3 |
| Ferritin (admission) (ng/mL) | 1993.3 [1283] (1943) | 1894.4 [1027] (2542) | 3551.1 [1712] (4384) | 186 | 0.183 | |
| Ferritin (worst)(ng/mL) | 2750.4 [1631] (3115) | 2368.9 [1274] (2864) | 2008.9 [1540] (1498 | 205 | 0.290 | |
| Interleukin-6 (admission) (pg/mL) | 64.8 [32] (83.4) | 60.8 [33] (78.0) | 58.8 [34] (73.4) | 377 | 0.925 | |
| Interleukin-6 (worst)(pg/mL) | 338.2 [89] (950.5) | 171.8 [103.5] (235.7) | 113.1 [65.5] (164.5) | 398 | 0.029 | 2 vs. 3 |
| Variables | Wave1 Mean [Median] (SD) N = 150 | Wave2 Mean [Median] (SD) N = 180 | Wave3 Mean [Median] (SD) N = 185 | Tot | p-Value | Post Hoc |
|---|---|---|---|---|---|---|
| Helmet Continuous Positive Air Pressure (H-CPAP) treatments | ||||||
| Positive End Expiratory Pressure (PEEP) | 12.8 [12] (2.0) | 9.7 [9] (7.0) | 8.1 [8] (1.2) | 512 | <0.001 | 1 vs. 2 vs. 3 |
| FiO2 | 81.3 [80] (12.4) | 70.2 [70] (11.6) | 71.8 [70] (9.4) | 514 | <0.001 | 1 vs. 2,3 |
| PaO2/FiO2 (in oxygen) | 132.3 [115.5] (64.4) | 159.6 [137] (53.8) | 147.5 [130] (64.0) | 514 | 0.001 | 1 vs. 2,3 |
| First PaO2/FiO2 (in H-CPAP) | 217.8 [203.5] (105.8) | 212.1 [199.5] (91.8) | 202.8 [195] (77.4) | 515 | 0.747 | |
| Worst PaO2/FiO2 (in H-CPAP) | 100.5 [80] (56.5) | 116.7 [100.5] (53.8) | 147.0 [135] (64.5) | 477 | <0.001 | 1 vs. 2 vs. 3 |
| PaO2/FiO2 post-pronation (in H-CPAP) | 242.4 [227.5] (119.6) | 273.3 [227.5] (108.6) | 249.7 [240] (97.1) | 396 | 0.051 | |
| Proned | ||||||
| No | N = 54; 50.9% | N = 24; 22.6% | N = 28; 26.4% | 106 | <0.001 | 1 vs. 2,3 |
| Yes | N = 96; 23.5% | N = 156; 38.1% | N= 157; 38.4% | 409 | ||
| Do Not Intubate (DNI) | 0.002 | 3 vs. 1,2 | ||||
| No | N = 128; 27.2% | N = 164; 34.9% | N = 178; 37.9% | 470 | ||
| Yes | N = 22; 48.9% | N = 16; 35.6% | N = 7; 15.6% | 45 | ||
| Outcomes | ||||||
| Death | ||||||
| No | N = 108; 26.2% | N = 143; 34.7% | N = 161; 39.1% | 412 | 0.003 | 1 vs. 3 |
| Yes | N = 42; 40.8% | N = 37; 35.9% | N = 24; 23.3% | 103 | ||
| H-CPAP success | ||||||
| No | N = 57; 36.8% | N = 55; 35.5% | N = 43; 27.7% | 155 | 0.014 | 1 vs. 3 |
| Yes | N = 93; 25.8% | N = 125; 34.7% | N = 142; 39.4% | 360 | ||
| Outcome (Dependent) Variable | Independent Variables | Coeff (b) | exp(b) = Odds Ratio (OR) # | Lower Lim OR 95% CI | Upper Lim OR 95% CI | p-Value | Nagelkerke R2 |
|---|---|---|---|---|---|---|---|
| H-CPAP success (yes vs. no) | Worst PaO2/FiO2 (in H-CPAP) | 0.037 | 1.038 | 1.028 | 1.048 | <0.001 | 0.54 |
| FiO2 in H-CPAP | −0.057 | 0.944 | 0.915 | 0.974 | <0.001 | ||
| Steroids (yes vs. no) | 2.63 | 13.915 | 2.611 | 74.207 | 0.001 | ||
| D-dimer at admission (×1000) | −0.1 | 0.905 | 0.980 | 1 | 0.031 | ||
| average PEEP | −0.13 | 0.878 | −0.260 | −0.001 | 0.048 | ||
| Death (yes vs. no) | Worst PaO2/FiO2 (in H-CPAP) | −0.038 | 0.963 | 0.951 | 0.974 | <0.001 | 0.41 |
| Steroids (yes vs. no) | −1.45 | 0.233 | 0.075 | 0.730 | 0.012 | ||
| Lactate dehydrogenase (LDH) at admission | 0.001 | 1.001 | 0.999 | 1.003 | 0.088 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piluso, M.; Ferrari, C.; Pagani, S.; Usai, P.; Raschi, S.; Parachini, L.; Oggionni, E.; Melacini, C.; D’Arcangelo, F.; Cattaneo, R.; et al. COVID-19 Acute Respiratory Distress Syndrome: Treatment with Helmet CPAP in Respiratory Intermediate Care Unit by Pulmonologists in the Three Italian Pandemic Waves. Adv. Respir. Med. 2023, 91, 383-396. https://doi.org/10.3390/arm91050030
Piluso M, Ferrari C, Pagani S, Usai P, Raschi S, Parachini L, Oggionni E, Melacini C, D’Arcangelo F, Cattaneo R, et al. COVID-19 Acute Respiratory Distress Syndrome: Treatment with Helmet CPAP in Respiratory Intermediate Care Unit by Pulmonologists in the Three Italian Pandemic Waves. Advances in Respiratory Medicine. 2023; 91(5):383-396. https://doi.org/10.3390/arm91050030
Chicago/Turabian StylePiluso, Martina, Clarissa Ferrari, Silvia Pagani, Pierfranco Usai, Stefania Raschi, Luca Parachini, Elisa Oggionni, Chiara Melacini, Francesca D’Arcangelo, Roberta Cattaneo, and et al. 2023. "COVID-19 Acute Respiratory Distress Syndrome: Treatment with Helmet CPAP in Respiratory Intermediate Care Unit by Pulmonologists in the Three Italian Pandemic Waves" Advances in Respiratory Medicine 91, no. 5: 383-396. https://doi.org/10.3390/arm91050030