The Role and Efficacy of Vitamin C in Sepsis: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:Highlights
- Sepsis is a significant global healthcare burden and the leading cause of in-patient mortality.
- Our analysis showed that vitamin C adjunct therapy was linked to a significant decrease in mortality, duration of vasopressor used, and SOFA scores in septic patients.
- There is a further need for a large, randomized control trial to define a clearer role of vitamin C in the care of septic patients.
Abstract
1. Introduction
Clinical Rationale for the Study
2. Materials and Methods
2.1. Eligibility Criteria
- were RCTs with supraphysiologic doses of vitamin C as an intervention in septic patients with the standard of care as the control arm.
- had patients aged > 18 years.
- were available in the English language regardless of date or status of publications.
2.2. Information Sources
2.3. Trial Selection and Evaluation
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
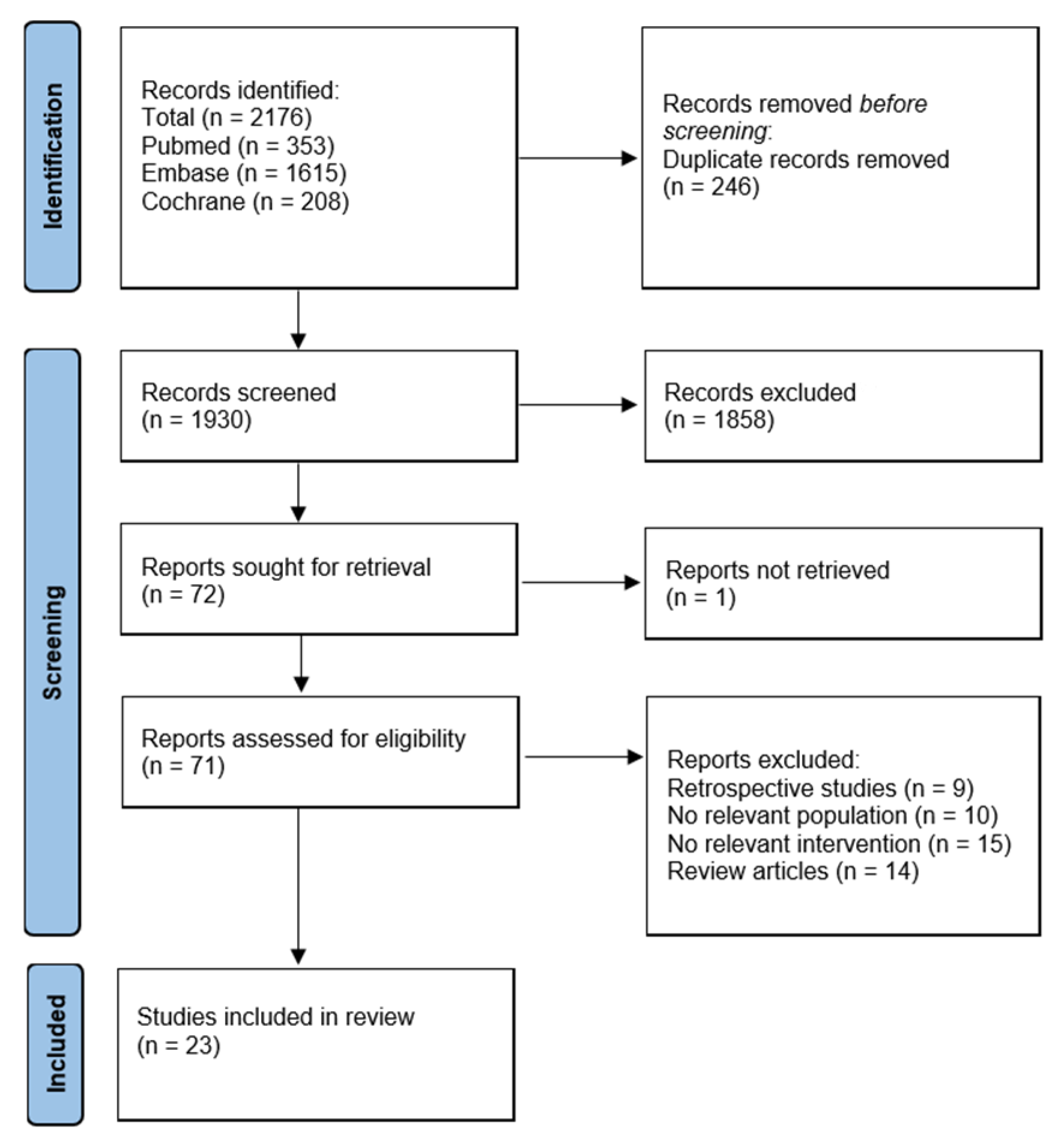
3.1. Literature Search
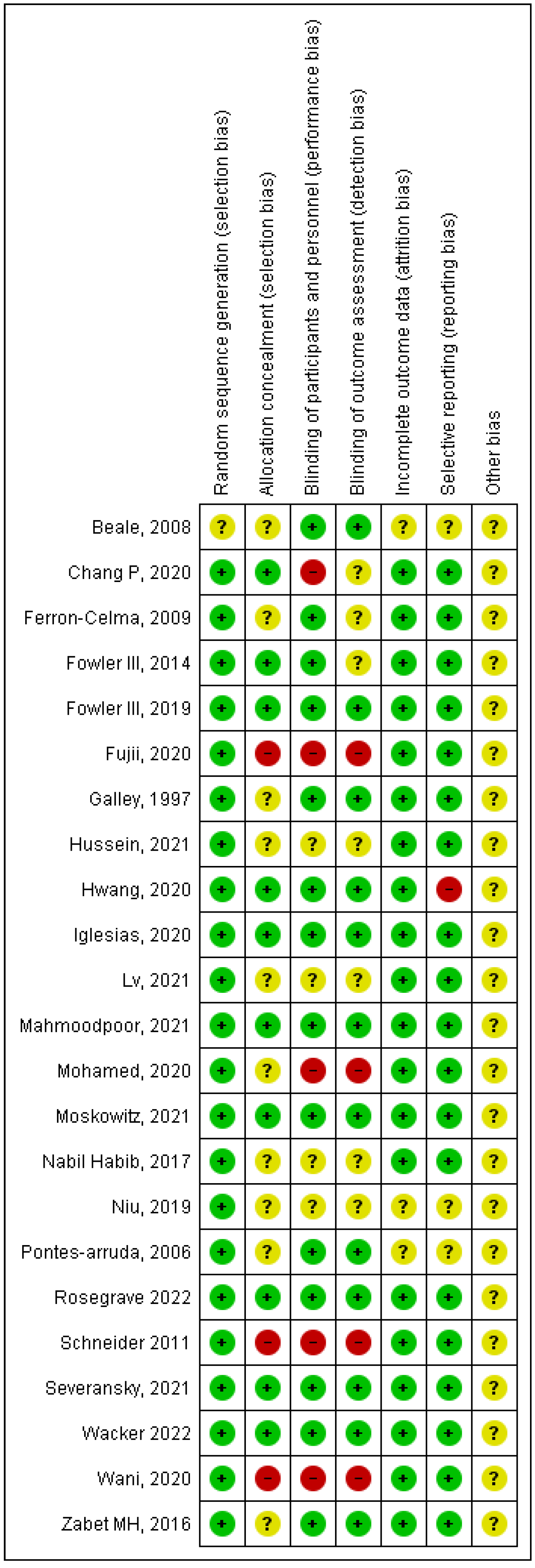
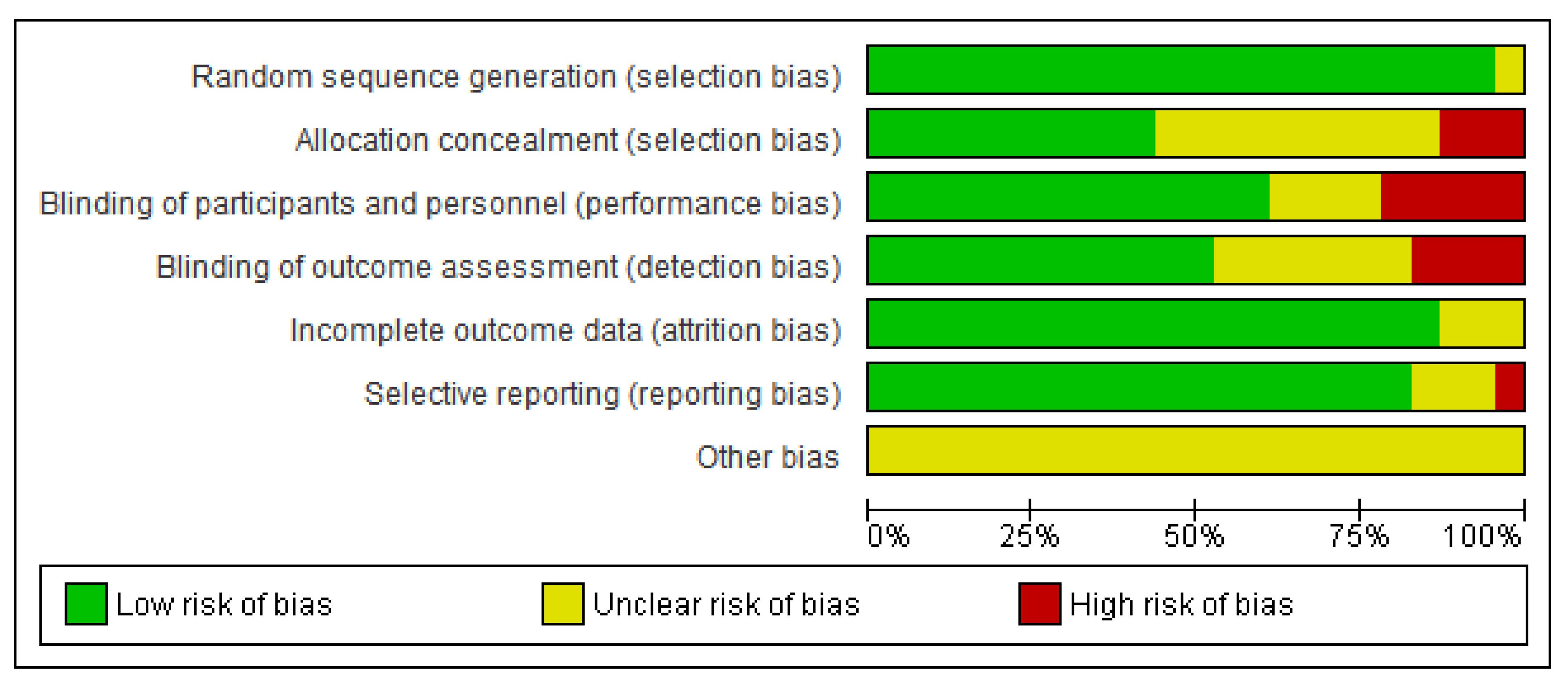
3.2. Risk of Bias
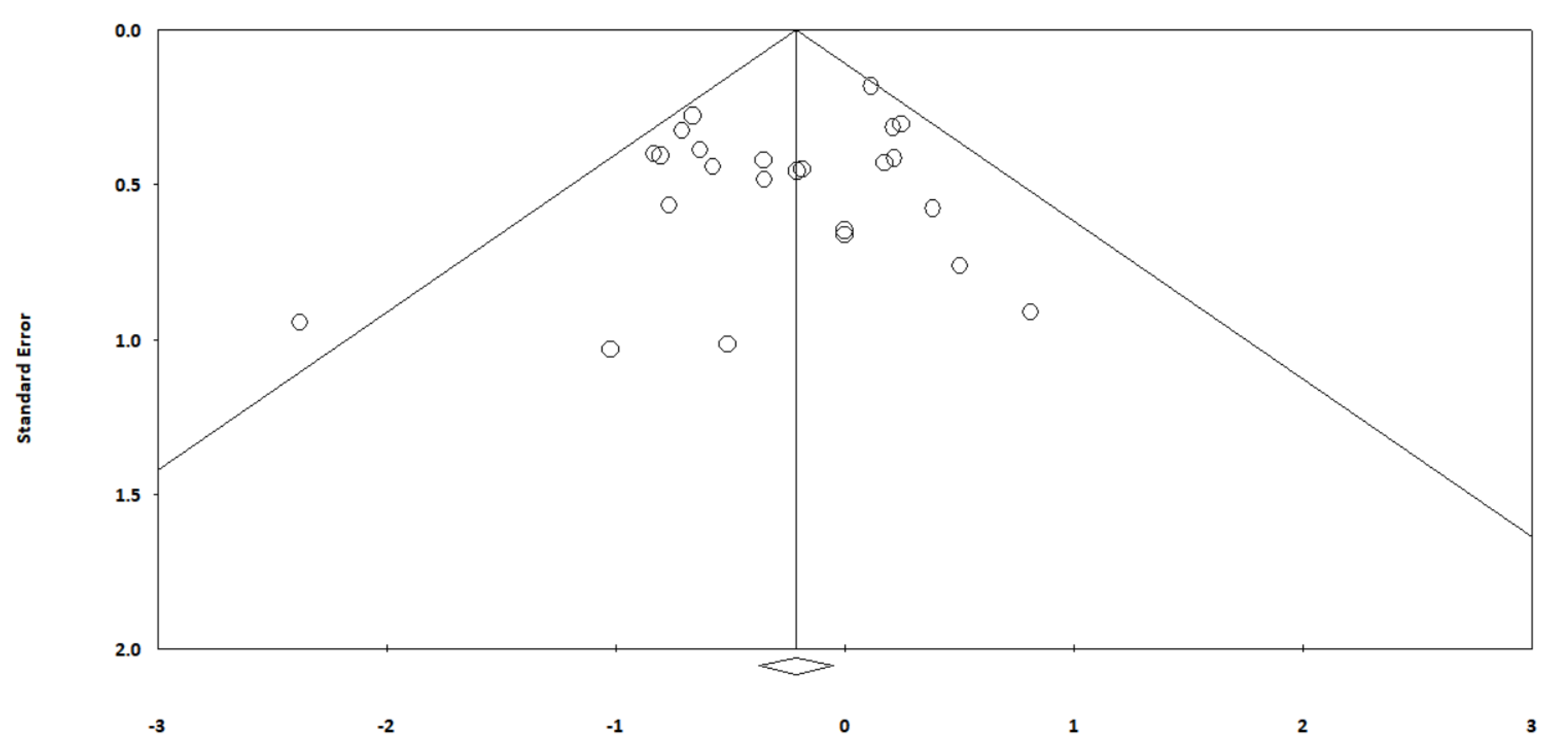
3.3. Publication Bias
3.4. Results of Quantitative Analysis
3.4.1. Mortality
Overall
Intravenous Dosing
Enteral Dosing
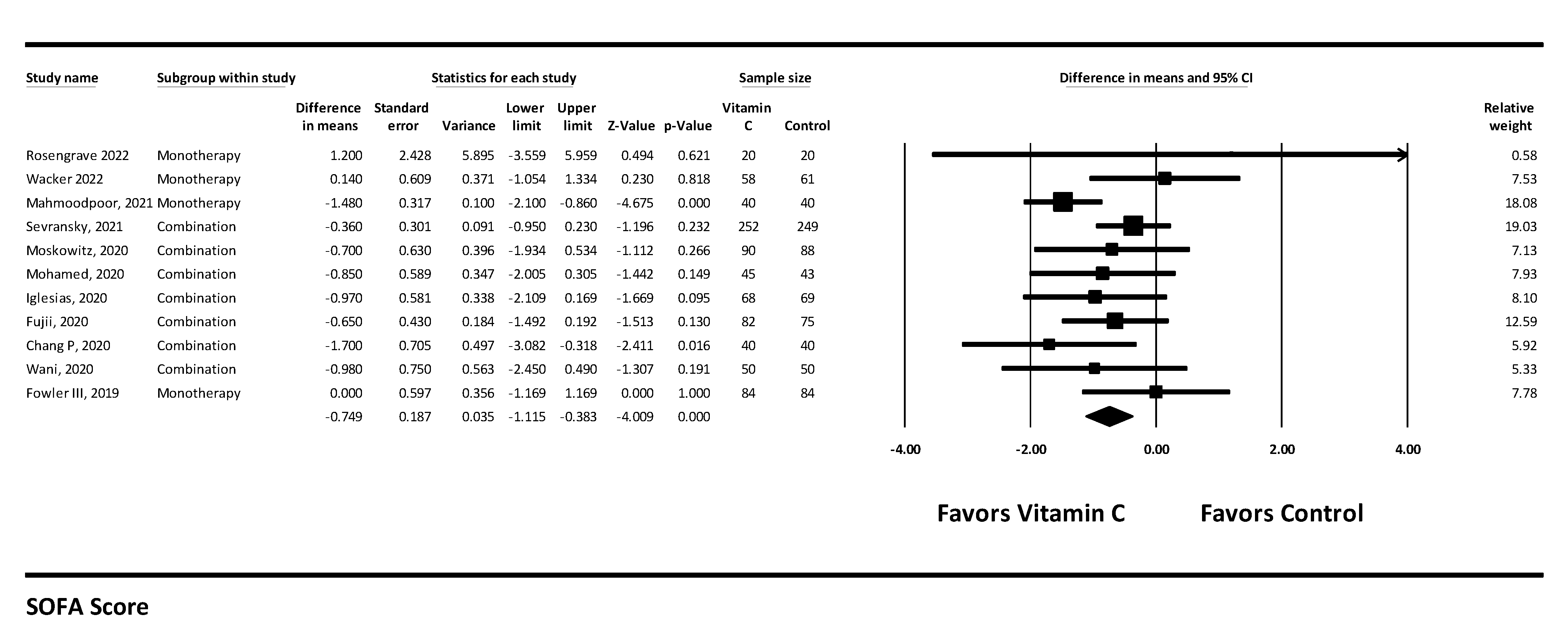
3.4.2. SOFA Score
3.4.3. Hospital Length of Stay
3.4.4. ICU Length of Stay
3.4.5. Duration of Vasopressors Use
3.5. Subgroup Analysis
3.5.1. Monotherapy
3.5.2. Combination Therapy
3.6. Sensitivity Analysis
3.7. Summary of Results
4. Discussion
Clinical Implications and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Tracey, K.J.; Fong, Y.; Hesse, D.G.; Manogue, K.R.; Lee, A.T.; Kuo, G.C.; Lowry, S.F.; Cerami, A. Anti-cachectin/TNF monoclonal antibodies prevent septic shock during lethal bacteraemia. Nature 1987, 330, 662–664. [Google Scholar] [CrossRef] [PubMed]
- Ulloa, L.; Tracey, K.J. The “cytokine profile”: A code for sepsis. Trends Mol. Med. 2005, 11, 56–63. [Google Scholar] [CrossRef]
- Adhikari, N.K.; Fowler, R.A.; Bhagwanjee, S.; Rubenfeld, G.D. Critical care and the global burden of critical illness in adults. Lancet 2010, 376, 1339–1346. [Google Scholar] [CrossRef]
- Luhr, R.; Cao, Y.; Söderquist, B.; Cajander, S. Trends in sepsis mortality over time in randomised sepsis trials: A systematic literature review and meta-analysis of mortality in the control arm, 2002–2016. Crit. Care 2019, 23, 241. [Google Scholar] [CrossRef] [Green Version]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Liu, C.; Li, J. Comparison of Vitamin C and its derivative antioxidant activity: Evaluated by using density functional theory. ACS Omega 2020, 5, 25467–25475. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Luo, D.; Wan, X.; Liu, Y.; Liu, J.; Bian, Z.; Tong, T. Detecting the skewness of data from the sample size and the five-number summary. arXiv 2020, arXiv:2010.05749. [Google Scholar]
- Rosengrave, P.; Spencer, E.; Williman, J.; Mehrtens, J.; Morgan, S.; Doyle, T.; Van Der Heyden, K.; Morris, A.; Shaw, G.; Carr, A.C. Intravenous vitamin C administration to patients with septic shock: A pilot randomised controlled trial. Crit. Care 2022, 26, 26. [Google Scholar] [CrossRef] [PubMed]
- Wacker, D.A.; Burton, S.L.; Berger, J.P.; Hegg, A.J.; Heisdorffer, J.; Wang, Q.; Medcraft, E.J.; Reilkoff, R.A. Evaluating Vitamin C in Septic Shock: A Randomized Controlled Trial of Vitamin C Monotherapy. Crit. Care Med. 2021, 50, e458–e467. [Google Scholar] [CrossRef] [PubMed]
- Lv, S.J.; Zhang, G.H.; Xia, J.M.; Yu, H.; Zhao, F. Early use of high-dose vitamin C is beneficial in treatment of sepsis. Ir. J. Med. Sci. 2021, 190, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodpoor, A.; Shadvar, K.; Sanaie, S.; Hadipoor, M.R.; Pourmoghaddam, M.A.; Saghaleini, S.H. Effect of Vitamin C on mortality of critically ill patients with severe pneumonia in intensive care unit: A preliminary study. BMC Infect. Dis. 2021, 21, 616. [Google Scholar] [CrossRef] [PubMed]
- Syed, A.A.; Knowlson, S.; Sculthorpe, R.; Farthing, D.; DeWilde, C.; Farthing, C.A.; Larus, T.L.; Martin, E.; Brophy, D.F.; Gupta, S.; et al. Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. J. Transl. Med. 2014, 12, 32. [Google Scholar]
- Truwit, J.D.; Hite, R.D.; Morris, P.E.; DeWilde, C.; Priday, A.; Fisher, B.; Thacker, L.R.; Natarajan, R.; Brophy, D.F.; Sculthorpe, R.; et al. Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients with Sepsis and Severe Acute Respiratory Failure: The CITRIS-ALI Randomized Clinical Trial. JAMA 2019, 322, 1261–1270. [Google Scholar]
- Zabet, M.H.; Mohammadi, M.; Ramezani, M.; Khalili, H. Effect of high-dose Ascorbic acid on vasopressor’s requirement in septic shock. J. Res. Pharm. Pract. 2016, 5, 94–100. [Google Scholar] [PubMed]
- Nabil Habib, T.; Ahmed, I. Early adjuvant intravenous vitamin C treatment in septic shock may resolve the vasopressor dependence. Int. J. Microbiol. Adv. Immunol. 2017, 5, 77–81. [Google Scholar]
- Ferrón-Celma, I.; Mansilla, A.; Hassan, L.; Garcia-Navarro, A.; Comino, A.M.; Bueno, P.; Ferrón, J.A. Effect of vitamin C administration on neutrophil apoptosis in septic patients after abdominal surgery. J. Surg. Res. 2009, 153, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Galley, H.F.; Howdle, P.D.; Walker, B.E.; Webster, N.R. The effects of intravenous antioxidants in patients with septic shock. Free Radic. Biol. Med. 1997, 23, 768–774. [Google Scholar] [CrossRef]
- Hussein, A.A.; Sabry, N.A.; Abdalla, M.S.; Farid, S.F. A prospective, randomised clinical study comparing triple therapy regimen to hydrocortisone monotherapy in reducing mortality in septic shock patients. Int. J. Clin. Pract. 2021, 75, e14376. [Google Scholar] [CrossRef]
- Wani, S.J.; Mufti, S.A.; Jan, R.A.; Shah, S.U.; Qadri, S.M.; Khan, U.H.; Bagdadi, F.; Mehfooz, N.; Koul, P.A. Combination of vitamin C, thiamine and hydrocortisone added to standard treatment in the management of sepsis: Results from an open label randomised controlled clinical trial and a review of the literature. Infect. Dis. 2020, 52, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Sevransky, J.E.; Rothman, R.E.; Hager, D.N.; Bernard, G.R.; Brown, S.M.; Buchman, T.G.; Busse, L.W.; Coopersmith, C.M.; DeWilde, C.; Ely, E.W.; et al. Effect of Vitamin C, Thiamine, and Hydrocortisone on Ventilator- and Vasopressor-Free Days in Patients with Sepsis: The VICTAS Randomized Clinical Trial. JAMA 2021, 325, 742–750. [Google Scholar] [CrossRef]
- Moskowitz, A.; Huang, D.T.; Hou, P.C.; Gong, J.; Doshi, P.B.; Grossestreuer, A.V.; Andersen, L.W.; Ngo, L.; Sherwin, R.L.; Berg, K.M.; et al. Effect of Ascorbic Acid, Corticosteroids, and Thiamine on Organ Injury in Septic Shock: The ACTS Randomized Clinical Trial. JAMA 2020, 324, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Mohamed, Z.U.; Prasannan, P.; Moni, M.; Edathadathil, F.; Prasanna, P.; Menon, A.; Nair, S.; Greeshma, C.; Sathyapalan, D.T.; et al. Vitamin C Therapy for Routine Care in Septic Shock (ViCTOR) Trial: Effect of Intravenous Vitamin C, Thiamine, and Hydrocortisone Administration on Inpatient Mortality among Patients with Septic Shock. Indian J. Crit. Care Med. 2020, 24, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, J.; Vassallo, A.V.; Patel, V.V.; Sullivan, J.B.; Cavanaugh, J.; Elbaga, Y. Outcomes of Metabolic Resuscitation Using Ascorbic Acid, Thiamine, and Glucocorticoids in the Early Treatment of Sepsis: The ORANGES Trial. Chest 2020, 158, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.Y.; Ryoo, S.M.; Park, J.E.; Jo, Y.H.; Jang, D.H.; Suh, G.J.; Kim, T.; Kim, Y.J.; Kim, S.; Cho, H.; et al. Combination therapy of vitamin C and thiamine for septic shock: A multi-centre, double-blinded randomized, controlled study. Intensive Care Med. 2020, 46, 2015–2025. [Google Scholar] [CrossRef]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of Vitamin C, Hydrocortisone, and Thiamine vs Hydrocortisone Alone on Time Alive and Free of Vasopressor Support Among Patients with Septic Shock: The VITAMINS Randomized Clinical Trial. JAMA 2020, 323, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.; Liao, Y.; Guan, J.; Guo, Y.; Zhao, M.; Hu, J.; Zhou, J.; Wang, H.; Cen, Z.; Tang, Y.; et al. Combined Treatment with Hydrocortisone, Vitamin C, and Thiamine for Sepsis and Septic Shock: A Randomized Controlled Trial. Chest 2020, 158, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.J.; Qin, B.Y.; Yang, K.L.; Fan, Q.B.; Liu, W.Q.; Wang, C.Z. Effect of early exogenous vitamin C supplementation on prognosis of sepsis patients. China J. Mod. Med. 2019, 29, 65–69. [Google Scholar]
- Beale, R.J.; Sherry, T.; Lei, K.; Campbell-Stephen, L.; McCook, J.; Smith, J.; Venetz, W.; Alteheld, B.; Stehle, P.; Schneider, H. Early enteral supplementation with key pharmaconutrients improves Sequential Organ Failure Assessment score in critically ill patients with sepsis: Outcome of a randomized, controlled, double-blind trial. Crit. Care Med. 2008, 36, 131–144. [Google Scholar] [CrossRef]
- Pontes-Arruda, A.; Aragão, A.M.; Albuquerque, J.D. Effects of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in mechanically ventilated patients with severe sepsis and septic shock. Crit. Care Med. 2006, 34, 2325–2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, A.; Markowski, A.; Momma, M.; Seipt, C.; Luettig, B.; Hadem, J.; Wilhelmi, M.; Manns, M.P.; Wedemeyer, J. Tolerability and efficacy of a low-volume enteral supplement containing key nutrients in the critically ill. Clin. Nutr. 2011, 30, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B. Free radicals and antioxidants: Updating a personal view. Nutr. Rev. 2012, 70, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Michels, A.J.; Hagen, T.M.; Frei, B. Human genetic variation influences vitamin C homeostasis by altering vitamin C transport and antioxidant enzyme function. Annu. Rev. Nutr. 2013, 33, 45–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marik, P.E. Vitamin C for the treatment of sepsis: The scientific rationale. Pharmacol. Ther. 2018, 189, 63–70. [Google Scholar] [CrossRef]
- Cárcamo, J.M.; Pedraza, A.; Bórquez-Ojeda, O.; Golde, D.W. Vitamin C suppresses TNF alpha-induced NF kappa B activation by inhibiting I kappa B alpha phosphorylation. Biochemistry 2002, 41, 12995–13002. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Yang, H.; Czura, C.J.; Sama, A.E.; Tracey, K.J. HMGB1 as a late mediator of lethal systemic inflammation. Am. J. Respir. Crit. Care Med. 2001, 164, 1768–1773. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, B.M.; Fisher, B.J.; Kraskauskas, D.; Farkas, D.; Brophy, D.F.; Fowler, A.A.; Natarajan, R. Vitamin C: A novel regulator of neutrophil extracellular trap formation. Nutrients 2013, 5, 3131–3151. [Google Scholar] [CrossRef] [Green Version]
- Hemilä, H. Vitamin C and Infections. Nutrients 2017, 9, 339. [Google Scholar] [CrossRef] [Green Version]
- Molina, N.; Morandi, A.C.; Bolin, A.P.; Otton, R. Comparative effect of fucoxanthin and vitamin C on oxidative and functional parameters of human lymphocytes. Int. Immunopharmacol. 2014, 22, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Luo, G.; Yuan, J.; Wang, Y.; Yang, X.; Wang, X.; Li, G.; Liu, Z.; Zhong, N. Vitamin C mitigates oxidative stress and tumor necrosis factor-alpha in severe community-acquired pneumonia and LPS-induced macrophages. Mediat. Inflamm. 2014, 2014, 426740. [Google Scholar] [CrossRef] [Green Version]
- Dahl, H.; Degré, M. The effect of ascorbic acid on production of human interferon and the antiviral activity in vitro. Acta. Pathol. Microbiol. Scand. B 1976, 84b, 280–284. [Google Scholar] [CrossRef]
- Karpińska, T.; Kawecki, Z.; Kandefer-Szerszeń, M. The influence of ultraviolet irradiation, L-ascorbic acid and calcium chloride on the induction of interferon in human embryo fibroblasts. Arch. Immunol. Ther. Exp. 1982, 30, 33–37. [Google Scholar]
- Siegel, B.V. Enhancement of interferon production by poly(rI)-poly(rC) in mouse cell cultures by ascorbic acid. Nature 1975, 254, 531–532. [Google Scholar] [CrossRef] [PubMed]
- Scholz, S.S.; Borgstedt, R.; Ebeling, N.; Menzel, L.C.; Jansen, G.; Rehberg, S. Mortality in septic patients treated with vitamin C: A systematic meta-analysis. Crit. Care 2021, 25, 17. [Google Scholar] [CrossRef] [PubMed]
- Sato, R.; Hasegawa, D.; Prasitlumkum, N.; Ueoka, M.; Nishida, K.; Takahashi, K.; Nasu, M.; Dugar, S. Effect of IV High-Dose Vitamin C on Mortality in Patients with Sepsis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Care Med. 2021, 49, 2121–2130. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.J.; Ortiz-Reyes, A.; Dhaliwal, R.; Clarke, J.; Hill, A.; Stoppe, C.; Lee, Z.Y.; Heyland, D.K. IV Vitamin C in Critically Ill Patients: A Systematic Review and Meta-Analysis. Crit. Care Med. 2022, 50, e304–e312. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Yang, C.; Yu, X. Effect of vitamin C on prognosis of critically ill patients: A Meta-analysis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2019, 31, 942–948. [Google Scholar] [PubMed]
- Ao, G.; Li, J.; Yuan, Y.; Wang, Y.; Nasr, B.; Bao, M.; Gao, M.; Qi, X. Intravenous vitamin C use and risk of severity and mortality in COVID-19: A systematic review and meta-analysis. Nutr. Clin. Pract. 2022, 37, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Keya, T.A.; Leela, A.; Fernandez, K.; Habib, N.; Rashid, M. Effect of Vitamin C Supplements on Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Curr. Rev. Clin. Exp. Pharmacol. 2022, 17, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Salanti, G.; Belletti, A.; Bellomo, R.; Carr, A.; Furukawa, T.A.; Luethi, N.; Luo, Y.; Putzu, A.; Sartini, C.; et al. Effect of adjunctive vitamin C, glucocorticoids, and vitamin B1 on longer-term mortality in adults with sepsis or septic shock: A systematic review and a component network meta-analysis. Intensive Care Med. 2022, 48, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Assouline, B.; Faivre, A.; Verissimo, T.; Sangla, F.; Berchtold, L.; Giraud, R.; Bendjelid, K.; Sgardello, S.; Elia, N.; Pugin, J.; et al. Thiamine, Ascorbic Acid, and Hydrocortisone as a Metabolic Resuscitation Cocktail in Sepsis: A Meta-Analysis of Randomized Controlled Trials With Trial Sequential Analysis. Crit. Care Med. 2021, 49, 2112–2120. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Hu, C.; Huang, W.; Xu, Q.; Hu, B.; Li, J. Effect of Combined Hydrocortisone, Ascorbic Acid and Thiamine for Patients with Sepsis and Septic Shock: A Systematic Review and Meta-Analysis. Shock 2021, 56, 880–889. [Google Scholar] [CrossRef]
- Fong, K.M.; Au, S.Y.; Ng, G.W.Y. Steroid, ascorbic acid, and thiamine in adults with sepsis and septic shock: A systematic review and component network meta-analysis. Sci. Rep. 2021, 11, 15777. [Google Scholar] [CrossRef] [PubMed]
- Ge, Z.; Huang, J.; Liu, Y.; Xiang, J.; Gao, Y.; Walline, J.H.; Lu, X.; Yu, S.; Zhao, L.; Li, Y. Thiamine combined with vitamin C in sepsis or septic shock: A systematic review and meta-analysis. Eur. J. Emerg. Med. 2021, 28, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Zeng, J.; Li, D.-H.; Yang, G.-Y.; Wang, K.; Deng, H.-F.; Jiang, H. Efficacy of intravenous vitamin C intervention for septic patients: A systematic review and meta-analysis based on randomized controlled trials. Am. J. Emerg. Med. 2021, 50, 242–250. [Google Scholar] [CrossRef]
- Wei, X.-B.; Wang, Z.-H.; Liao, X.-L.; Guo, W.-X.; Wen, J.-Y.; Qin, T.-H.; Wang, S.-H. Efficacy of vitamin C in patients with sepsis: An updated meta-analysis. Eur. J. Pharmacol. 2020, 868, 172889. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.U.; Hwang, J.Q.; Gardner, T.H.; Repas, K.; Delee, R.; Yu, S.; Smith, B.; Banks, P.A.; Conwell, D.L. Lactated Ringer’s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin. Gastroenterol. Hepatol. 2011, 9, 710–717.e1. [Google Scholar] [CrossRef]
- Hopkinson, D.A. High-Dose Intravenous Vitamin C as an Adjunctive Treatment for Sepsis in Rwanda. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04088591?type=Intr&cond=vitamin+c&draw=3&rank=40 (accessed on 1 January 2022).
- Kotanidou, A.; Vitamin, C. Hydrocortisone and Thiamine for Septic Shock (CORVICTES). University of Athens. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03592693?type=Intr&cond=vitamin+c&draw=3&rank=41 (accessed on 1 January 2022).
- Liu, Z. Clinical Efficacy of Megadose Vitamin C in Sepsis (CEMVIS). Zhujiang Hospital. Available online: https://www.clinicaltrials.gov/ct2/show/NCT05194189?rslt=Without&type=Intr&cond=vitamin+c&draw=2&rank=16 (accessed on 1 January 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Name | No. of Patients | Type of Therapy | Inclusion Criteria | Exclusion Criteria | Primary Outcome | Secondary Outcome |
|---|---|---|---|---|---|---|
| Rosengrave, 2022 [12] | 40 | Monotherapy | Receiving intravenous antimicrobial therapy specifically for infection, receiving ≥ 5 μg/min noradrenaline or adrenaline, SOFA score ≥ 2 | Age < 18 years, consent could not be obtained, patient not expected to survive 24 h, known G6PD deficiency, known or suspected, pregnancy or breastfeeding. | Vasopressor requirement | Vasopressor dose delivered, SOFA scores, oxygenation parameters, and length of ICU and hospital stay, and ICU and hospital mortality |
| Wacker, 2022 [13] | 124 | Monotherapy | Adult patients within 24 h of onset of septic shock | Inability to obtain written consent and initiate study drug within 24 h of eligibility, known history of nephrolithiasis, and shock occurring immediately following cardiac arrest. | 28-day mortality | ICU mortality, time to lactate clearance, need for renal replacement therapy (RRT), changes in severity-of-disease index scores, and duration of ICU and hospital stay |
| Lv, 2021 [14] | 117 | Monotherapy | Admitted to the ICU, age 18–75 years, meet criteria of sepsis, no vitamin C treatment before admission | Terminal-stage patients, pregnant or lactating females, long-term use of hormones or immunosuppressive agents, active malignancy, mental disorders, autoimmune diseases | 28-day mortality | Changes in the SOFA scores in the first 72 h after ICU admission, application time of vasoactive drugs, duration of time in ICU, procalcitonin clearance |
| Mahmoodpoor, Jun 2021 [15] | 80 | Monotherapy | Patients with severe pneumonia | Age 18–80 years, renal insufficiency, history of vitamin C usage during past 48 h., pregnancy or breastfeeding, life expectancy of fewer than 24 h, G6PD deficiency, DKA, nephrolithiasis | Days on mechanical ventilation, vasopressor use and dose, 28-day mortality | CRP, procalcitonin, ICU length of stay (LOS) |
| Fowler III, 2014 phase I [16] | 24 | Monotherapy | Presence of a SIRS, suspected or proven infection, presence of sepsis-induced organ dysfunction | Terminal Cancer or Expected Survival < 24 h | Ascorbic acid safety and tolerability | Days on vasopressor, ventilator-free days, ICU length of stay, 28-day mortality |
| Fowler III, 2019 [17] | 167 | Monotherapy | Should meet 2 of 4 SIRS criteria with the following: Mechanically ventilation, PaO2:FiO2 < 300 mm Hg, bilateral opacities by chest radiography within 1 week of known clinical insult, new or worsening respiratory symptoms without evidence of left atrial hypertension, suspected or proven infection | Age < 18 years, non-English speaking, >48 h had elapsed since they met ARDS criteria, pregnant or breastfeeding, not expected to survive 24 h, receiving home oxygen greater than 2 L/min: history of interstitial lung disease, DAH, DKA, nephrolithiasis | Change in SOFA score from baseline to 96 h, change in plasma biomarkers of inflammation (CRP) and vascular injury (thrombomodulin levels) | All-cause 28-day mortality, ventilator-free days, ICU-free days, hospital-free days, SOFA score, vasopressor use, GCS, creatinine level |
| Zabet MH, 2016 [18] | 28 | Monotherapy | Patients with septic shock as per Surviving Sepsis Campaign and with the following criteria: Presence of SIRS with suspected or proven infection and presence of sepsis-induced organ dysfunction | Concomitant use of other antioxidants, corticosteroids administration, contraindication for high-dose ascorbic acid including bilateral ureteric obstruction, chronic hemodialysis, iron overload, oxalate stone formers, hemochromatosis, and glucose-6-phosphate dehydrogenase (G6PD) deficiency | Vasopressor dose and duration | Duration of Intensive Care Unit (ICU) stay and 28-day mortality |
| Nabil Habib, 2017 [19] | 100 | Monotherapy | Admitted with the diagnosis of Septic shock | Pregnant and lactating females, history of oxalate nephrolithiasis, G6PD deficiency, PNH, hereditary hemochromatosis, shock not due to sepsis, or patients with mixed type of shock | Need for organ supportive measures and Length of ICU stay | In-ICU mortality |
| Ferron-Celma, 2009 [20] | 20 | Monotherapy | Age > 18, meets sepsis criteria, undergoing abdominal surgery, POSSUM score > 30% | Age < 18 years old, unable to obtain consent | Neutrophil apoptosis via Fas receptor expression and caspase-3, poly (ADP-ribose) polymerase (PARP), and Bcl-2 levels in neutrophils | Mortality |
| Galley, 1997 [21] | 30 | Combination therapy | Meet septic shock criteria, receiving vasoconstrictor therapy (epinephrine, norepinephrine, dopamine) | Age < 21 years old, unable to obtain consent | Total lipid peroxidase, malondialdehyde, Arginine: Citrulline, total Nitrite, reactive redox iron, total antioxidant capacity | Mortality |
| Hussein, 2021 [22] | 94 | Combination therapy | With septic shock on ICU admission or development during ICU stay | Pregnancy and lactation, contraindication to any of the components of the triple therapy regimen, G6PD deficiency, receiving another type of steroid during their stay, immunosuppressive medications, cancer patients, DNR/DNI patients | 28-day in-hospital mortality and ICU mortality | Shock time and duration on pressors |
| Wani, 2020 [23] | 100 | Combination therapy | Admitted with a diagnosis of sepsis and septic shock with a serum lactate level of >2 mmol/L | Age < 18 years, Pregnancy | In-hospital mortality | 30-day mortality, hospital LOS, duration of vasopressor therapy, lactate clearance, change in serum lactate, and the SOFA score over the first 4 days |
| Sevransky, 2021 [24] | 501 | Combination therapy | Suspected or confirmed infection, ICU admission, acute respiratory and/or cardiovascular organ dysfunction attributed to sepsis and requiring vasopressor (regardless of agent or dose) | Age < 18 years old, cardiovascular or respiratory organ failure requiring treatment, life expectancy < 30 days, DNR/DNI and current hospitalization > 30 days at the time of randomization, allergies to intervention, primary hyperoxaluria, oxalate nephropathy, G6PD deficiency, pregnancy, or known active breastfeeding, incarceration | Number of ventilator and vasopressor-free days in the first 30 days following the day of randomization | 30-day mortality |
| Moskowitz, 2020 [25] | 205 | Combination therapy | Age > 18 years, with suspected or confirmed infection and were receiving a vasopressor because of sepsis | Allergic to study drug components had a clinical indication for any of the study drugs, symptomatic kidney stones within the last year, G6PD deficiency, hemochromatosis, ESRD, or RRT, not expected to survive 24 h | Change in the (SOFA) score between enrollment and 72 h | Renal failure and 30-day mortality |
| Mohamed, 2020 [26] | 88 | Combination therapy | Adult non-pregnant patients with septic shock with initiation inotropic/presser support within 6 h of presentation | Patients with burns, limitations of care due to terminal illness, acute liver failure, pregnancy | Mortality during the inpatient stay | Time to shock reversal, change in SOFA score over 72 h, need for mechanical ventilation, incidence of new-onset AKI and ICU/hospital LOS. |
| Iglesias, 2020 [27] | 137 | Combination therapy | Adults > 18 years of age with a primary diagnosis of sepsis or septic shock or diagnosis of sepsis or septic shock within 12 h of admission to the ICU | Age < 18, pregnancy, DNR/DNI, terminal end-stage disease, required immediate surgery, HIV positive with a CD4 < 50 mm2, G6PD deficiency, transferred from another hospital | Resolution of shock and change in SOFA score. | 28-day mortality, ICU mortality, hospital mortality, procalcitonin clearance, hospital LOS, ICU LOS, ventilator-free days. |
| Hwang, 2020 [28] | 111 | Combination therapy | Adult patients (19–89 years old) presented and were diagnosed with septic shock. | Transferred from another hospital with vasopressor administration or mechanical ventilator support, limitations to treatment due to terminal disease or DNR/DNI, receiving vitamin C or thiamine before enrolment, cardiac arrest before enrolment, renal or ureteral stones | The change in SOFA score between the time of admission and 72 h after admission | Shock reversal and 28-day mortality |
| Fujii, 2020 [29] | 216 | Combination therapy | Diagnosed with septic shock within a maximum of 24 h before enrollment, vasopressor dependent for at least 2 h at the time of enrollment | Age < 18 years, DNR/DNI, imminent death, diagnosis of septic shock longer than 24 h ago, known or suspected disease with a strong indication or contraindication for any of the study drugs, another indication for hydrocortisone use other than septic shock. | Time alive and free of vasopressors at day 7 after randomization | 28-day, 90-day, ICU, and hospital mortality, 28-day cumulative vasopressor free days, 28-day cumulative mechanical ventilation-free days, 28-day renal replacement therapy–free days, change in SOFA score at day 72 h, 28-day ICU-free days and hospital LOS |
| Chang P, 2020 [30] | 80 | Combination therapy | Meeting the diagnostic criteria for sepsis, >18 years of age and procalcitonin > 2 ng/mL when entering the ICU | Pregnancy, terminal disease or DNR/DNI orders, major bleeding, cardiogenic shock, paraquat poisoning, persistent nonremovable infection sources. | 28-day all-cause mortality | Organ protection, procalcitonin reduction, adverse events related to therapy |
| Niu, 2019 [31] | 234 | Monotherapy | Age 18–75, meet diagnostic criteria for sepsis, no vitamin C used earlier in the hospitalization | Terminal-stage patients, pregnant or lactating females, long-term use of hormones or immunosuppressive agents, active malignancy, mental disorders | 28 Day mortality | 72 h change in SOFA, duration of vasopressors, elimination of Calcitonin, ICU length of stay |
| Beale, 2008 [32] | 55 | Enteral pharma-co-nutrition supplement (Intestamin) | Age > 18 years old, meeting SIRS criteria and at least one organ dysfunction occurring within 24 h. of ICU admission, APACHE II score >10, expected LOS in the ICU > 3 days, and indication for enteral nutrition for > 5 days | Cardiogenic shock or severe congestive heart failure NYHA class IV), severe, Pre-existing, parenchymal liver disease with clinically significant portal hypertension (Childs C), COPD, chronic renal failure requiring dialysis, pregnancy, AIDS, Immunosuppression, active cancer treatment | SOFA score | Mortality, length of stay and organ dysfunction |
| Pontes-aruda, 2006 [33] | 103 | Continuously tube-fed with a diet enriched with Eicosapentaenoic acid, Gamma Linolenate, and antioxidants | Age > 18 years old with clinical diagnosis of severe sepsis or septic shock, requiring mechanical ventilation and enteral access. | Age < 18 years, significant limitation of survival prognosis and/or incurable disease, chronic renal insufficiency, acute pancreatitis without established origin, head trauma with a GCS score < 5, recent stroke or subarachnoid hemorrhage, immunologic suppression, no indication for enteral nutrition or imminence of receiving parenteral nutrition, receiving partial parenteral nutrition, presence of uncontrolled diarrhea, recent GIB, planned to wean from mechanical ventilation | 28-day mortality | Changes in oxygenation status, time receiving mechanical ventilation, period in the intensive care setting, and development of new organ dysfunctions. |
| Schneider 2011 [34] | 58 | Enteral supplement Intestamin | Age 18–75 years, sepsis, or SIRS (APACHEscore 10–30), absence of severe gastrointestinal tract or metabolic diseases, enteral feeding within 48 h of admission with obtained written consent. | Expected patient survival less than 6 days, pregnancy or lactation, hemodynamically unstable, severe liver disease with cytolysis, gastrointestinal surgery in the last 4 weeks, severe enteritis/colitis, short intestine syndrome, GIB requiring intervention, and inability to enterally feed | ICU LOS | Hospital LOS, mortality, ventilator requirement and vasopressor requirement. |
| Outcomes | Relative Risk (95% CI) | Risk Difference (95% CI) | No. of Studies (Total Patients) | Certainty (GRADE) | |
|---|---|---|---|---|---|
| Risk with Control | Risk Difference with Vitamin C | ||||
| Overall Mortality | OR = 0.778 (0.635 to 0.954) | 32 deaths per 100 | 6 less deaths per 100 (1 fewer to 10 fewer) | 23 (2705) | Low a |
| Mortality with IV Vitamin C regimens | OR = 0.780 (628 to 0.968) | 37 deaths per 100 | 6 less deaths per 100 (1 fewer to 10 fewer) | 20 (2489) | Low b |
| Mortality with Enteral Vitamin C regimens | OR = 0.782 (0.367 to 1.665) | 37 deaths per 100 | 5 less deaths per 100 (21 fewer to 10 more) | 3 (216) | Very Low c |
| Mortality with Vitamin C Monotherapy | OR = 0.515 (0.390 to 0.680) | 42 deaths per 100 | 15 fewer deaths per 100 (21 fewer to 9 fewer) | 10 (941) | Moderate d |
| Mortality with Combination regimens containing Vitamin C | OR = 1.023 (0.836 to 1.251) | 34 deaths per 100 | No significant difference (4 fewer to 5 more) | 13 (1764) | Low e |
| Outcomes | Number of Studies | Sample Size | Absolute Effect Size (95% CI) | Certainty (GRADE) | |
|---|---|---|---|---|---|
| Control | Vitamin C | ||||
| SOFA Score | 11 | 819 | 829 | 0.75 lower (−1.12 lower to −0.38 lower) | Low a |
| Duration of vasopressor use | 9 | 449 | 449 | 1.03 fewer days (1.62 fewer to 0.45 fewer) | Very Low b |
| Duration of vasopressor use | 9 | 449 | 449 | 1.03 fewer days (1.62 fewer to 0.45 fewer) | Very Low b |
| ICU length of stay | 12 | 333 | 333 | 0.81 fewer days (1.64 fewer to 0.02 more) | Very Low c |
| Hospital length of stay | 6 | 239 | 239 | 1.32 more days (1.07 fewer to 3.71 more) | Very Low d |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhammad, M.; Jahangir, A.; Kassem, A.; Sattar, S.B.A.; Jahangir, A.; Sahra, S.; Niazi, M.R.K.; Mustafa, A.; Zia, Z.; Siddiqui, F.S.; et al. The Role and Efficacy of Vitamin C in Sepsis: A Systematic Review and Meta-Analysis. Adv. Respir. Med. 2022, 90, 281-299. https://doi.org/10.3390/arm90040038
Muhammad M, Jahangir A, Kassem A, Sattar SBA, Jahangir A, Sahra S, Niazi MRK, Mustafa A, Zia Z, Siddiqui FS, et al. The Role and Efficacy of Vitamin C in Sepsis: A Systematic Review and Meta-Analysis. Advances in Respiratory Medicine. 2022; 90(4):281-299. https://doi.org/10.3390/arm90040038
Chicago/Turabian StyleMuhammad, Marwah, Ahmad Jahangir, Ali Kassem, Saud Bin Abdul Sattar, Abdullah Jahangir, Syeda Sahra, Muhammad Rafay Khan Niazi, Ahmad Mustafa, Zeeshan Zia, Fasih Sami Siddiqui, and et al. 2022. "The Role and Efficacy of Vitamin C in Sepsis: A Systematic Review and Meta-Analysis" Advances in Respiratory Medicine 90, no. 4: 281-299. https://doi.org/10.3390/arm90040038