Outcome and Post-Surgical Lung Biopsy Change in Management of ARDS: A Proportional Prevalence Meta-Analysis

 , ,
, ,
Abstract
:Highlights
- Lung biopsy in ARDS patients lead to a change in management in 3/4 patients.
- Despite changes in management and pathology-directed treatment, there was significant mortality in ARDS patients who had lung biopsy.
- High rates of complications from lung biopsy were observed in ARDS patients who had lung biopsy.
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Outcomes
2.4. Statistical Analysis
3. Results
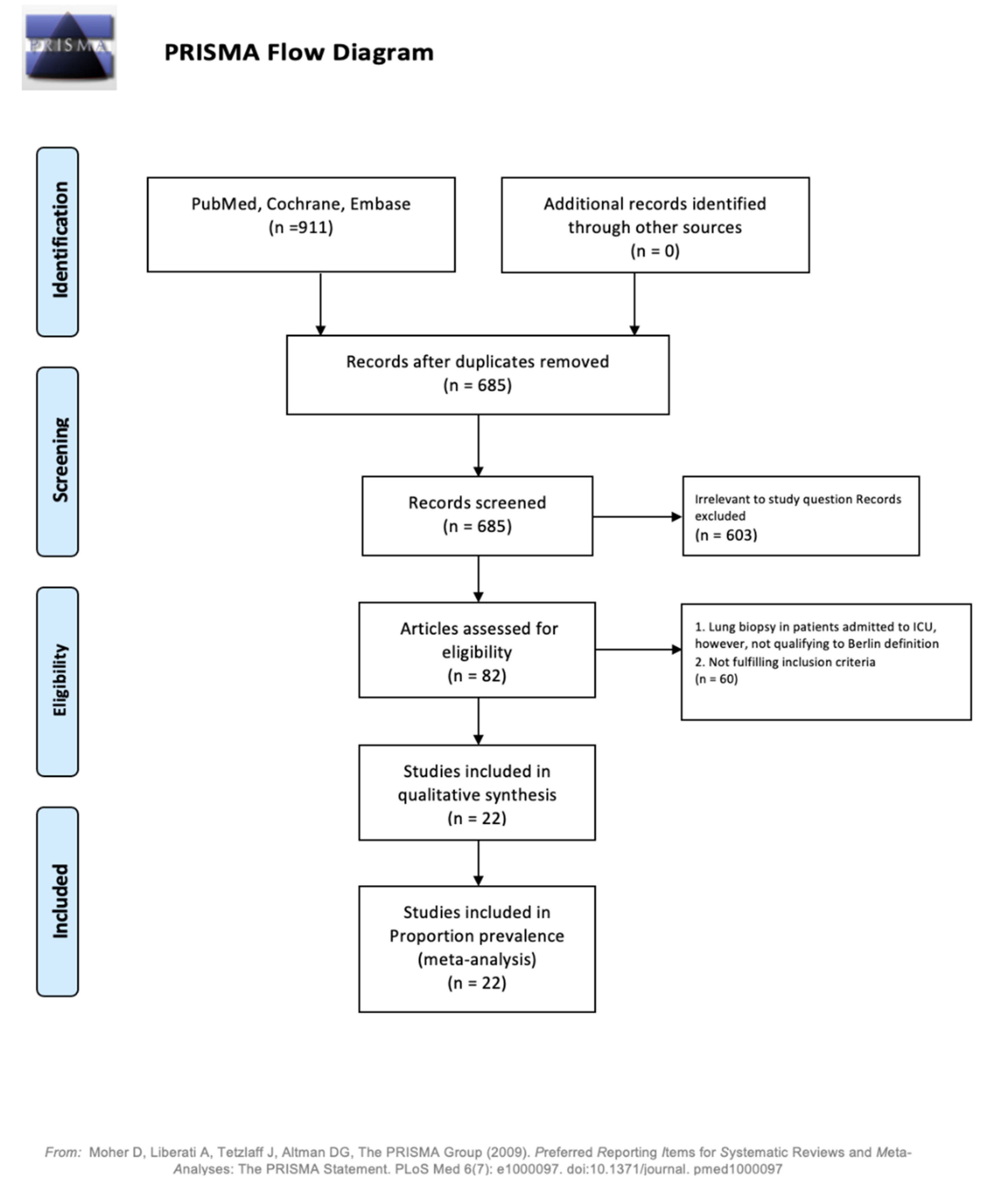
3.1. Search Results and Study Characteristics
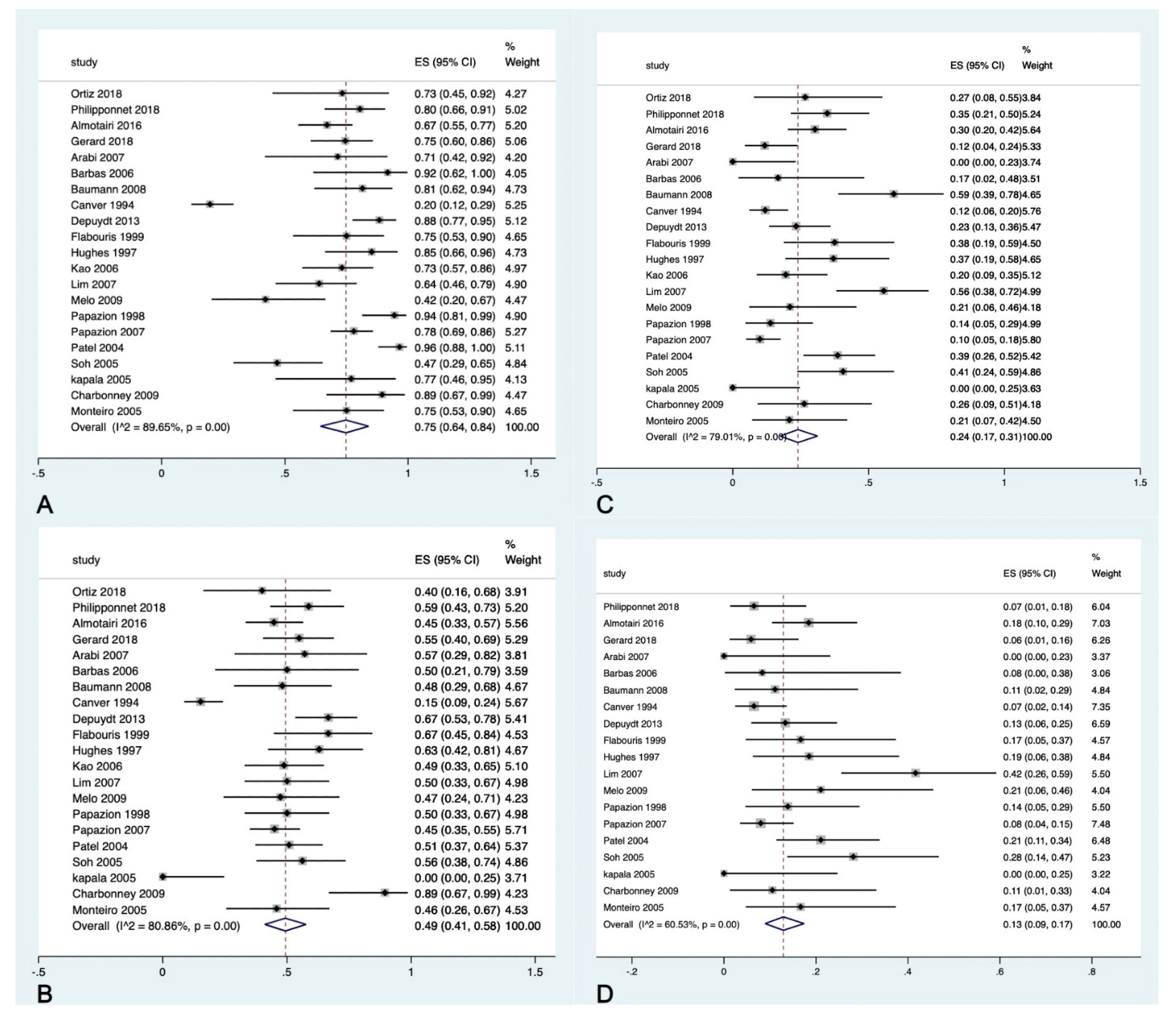
3.2. Primary Outcomes
3.3. Secondary Outcomes
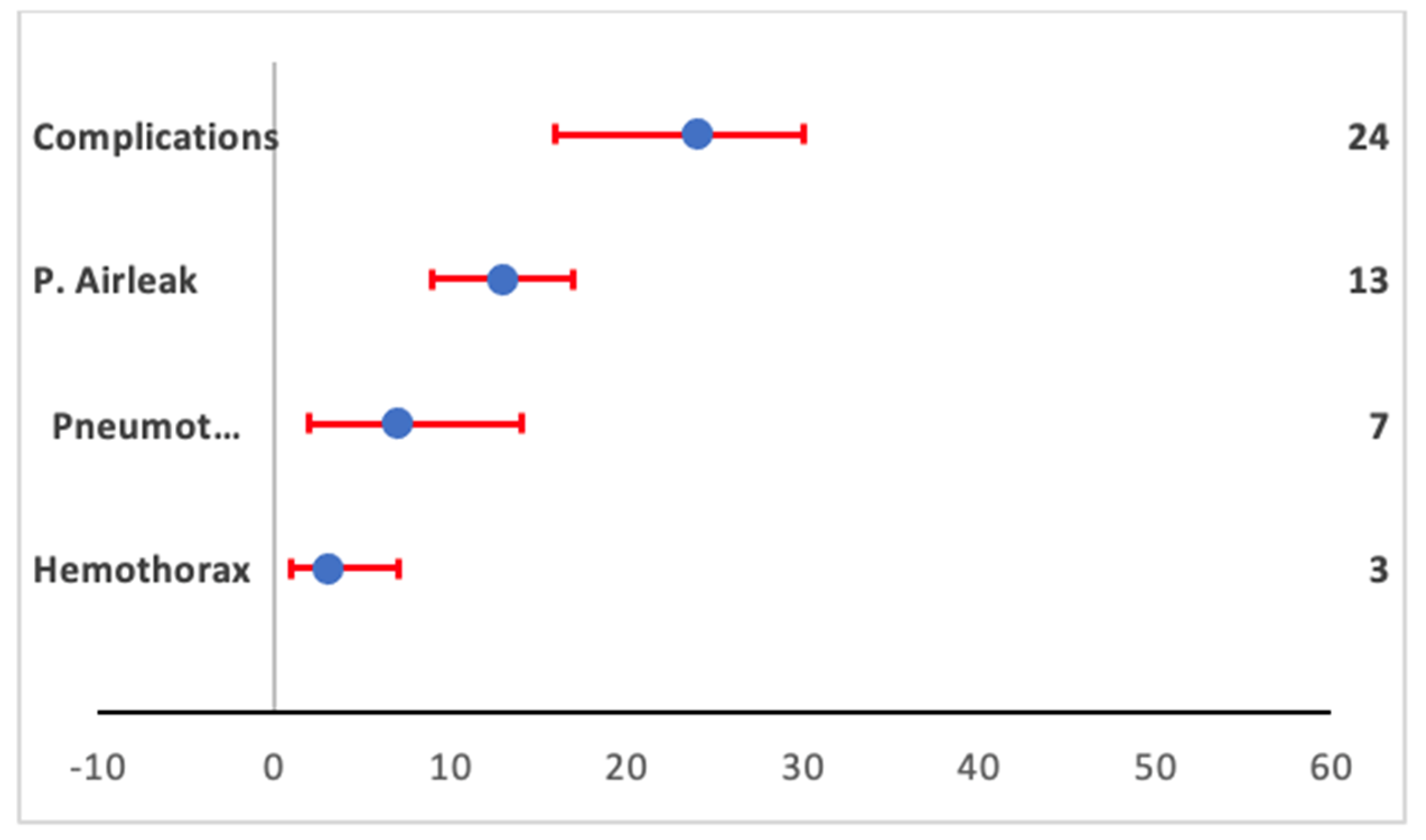
3.3.1. Complications
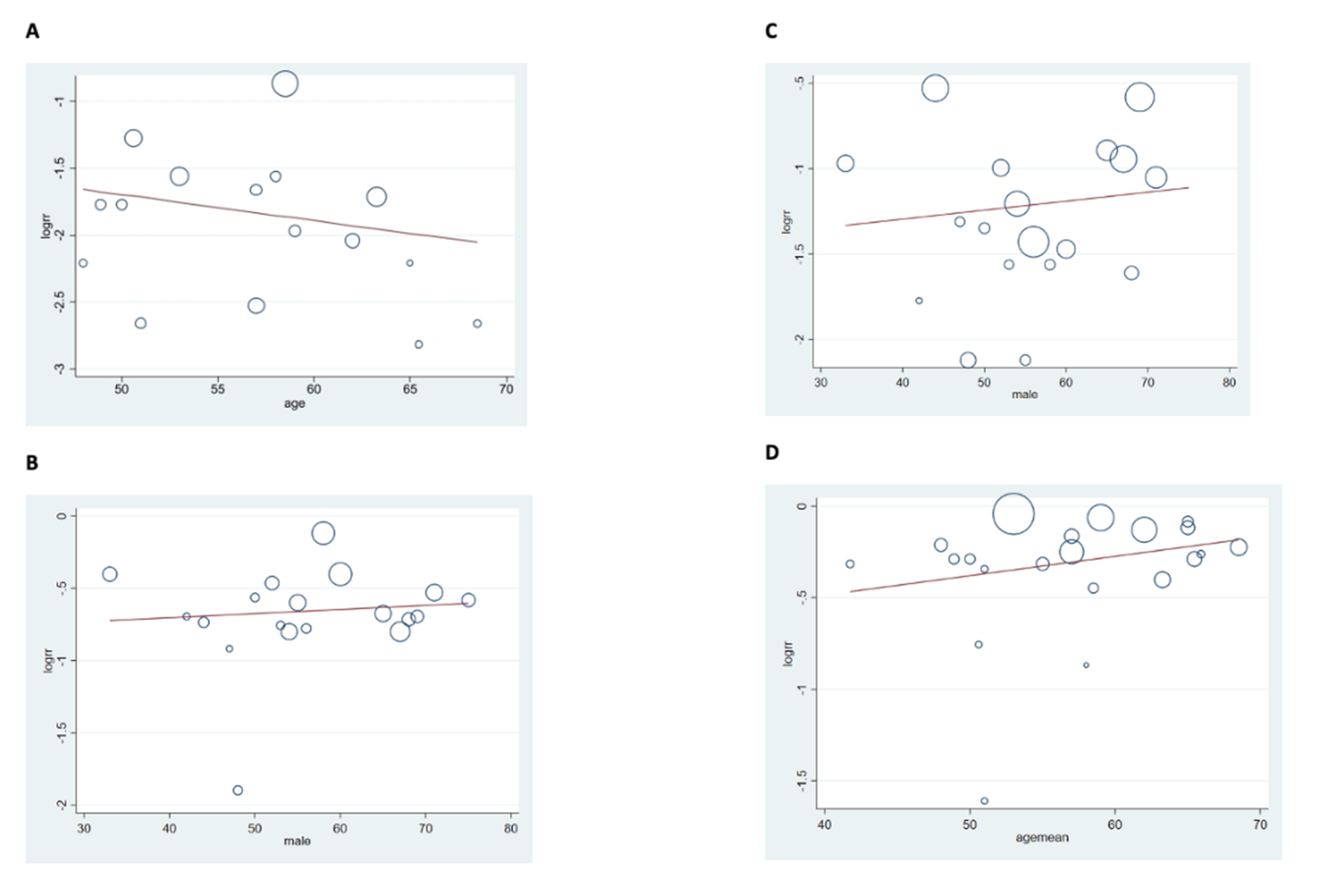
Regression Analysis
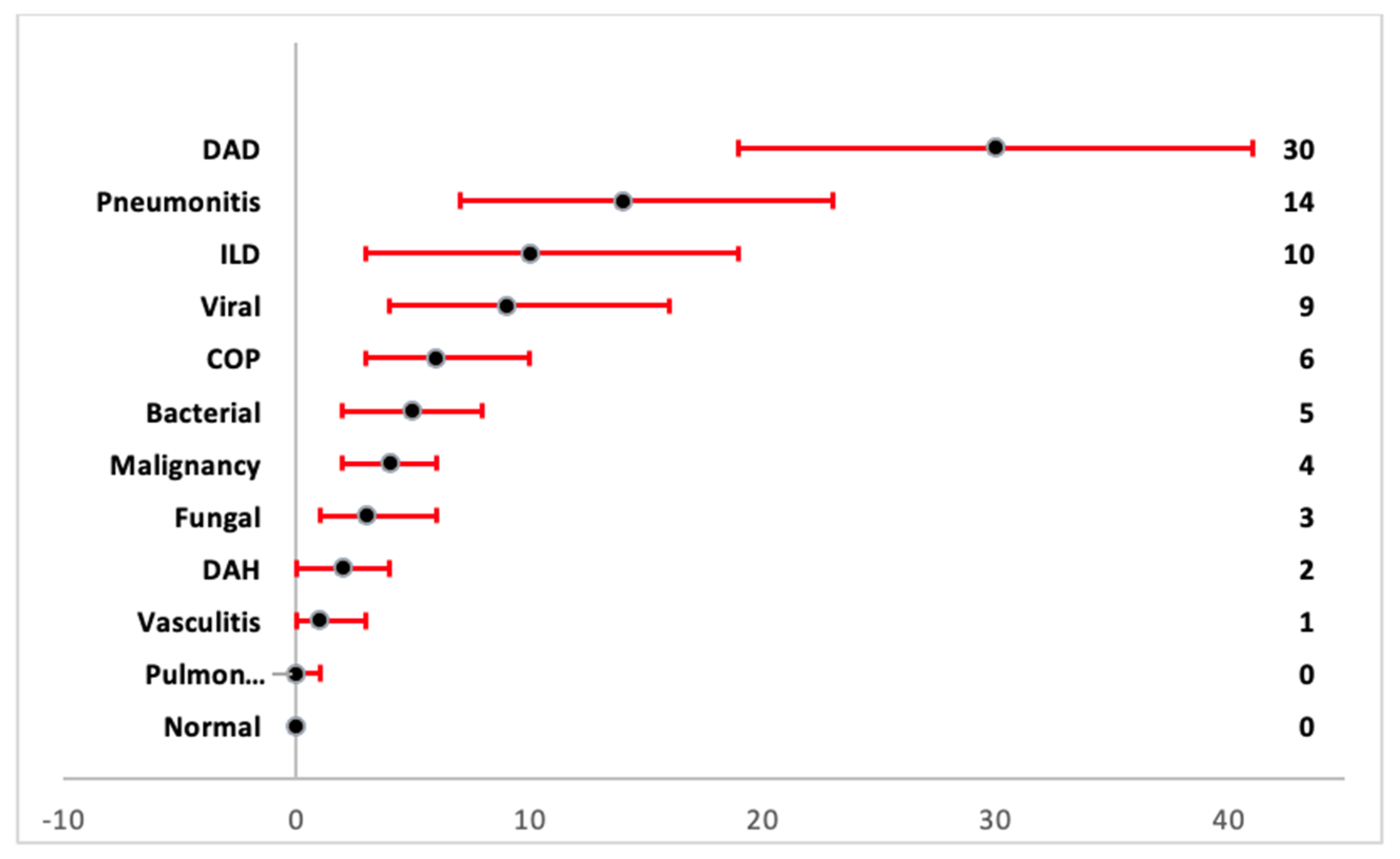
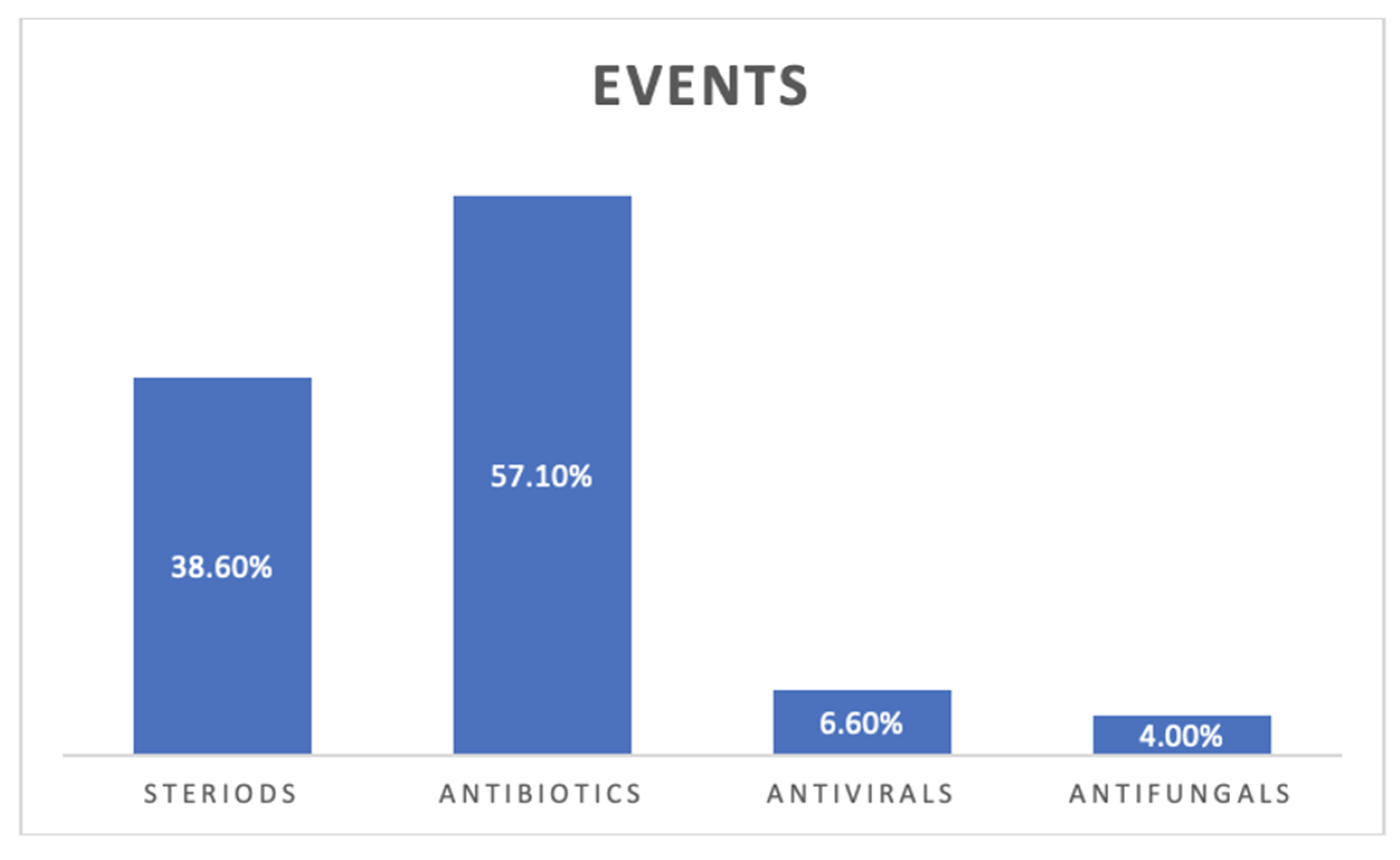
3.3.2. Pathologic Diagnosis
Quality of the Included Studies
4. Discussion
4.1. High Risk of Mortality with Lung Biopsy in ARDS
4.2. Pathological Diagnoses on Lung Biopsy and Change in Management
4.3. High Complication Rate with Lung Biopsy
5. Conclusions
Take Home Message
- Lung biopsy in ARDS patients leads to a change in management in 3/4 of patients.
- Despite a change in management and pathology-directed treatment, there was significant mortality in ARDS patients who had a lung biopsy.
- High rates of complications from lung biopsy were observed in ARDS patients who had a lung biopsy.
- The decision for lung biopsy in ARDS patients should be individualized considering the complications and mortality rates.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment. JAMA 2018, 319, 698–710. [Google Scholar] [CrossRef] [PubMed]
- Saguil, A.; Fargo, M.V. Acute respiratory distress syndrome: Diagnosis and management. Am. Fam. Physician 2020, 101, 730–738. [Google Scholar] [PubMed]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA J. Am. Med. Assoc. 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E. Acute respiratory distress syndrome. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Thille, A.W.; Esteban, A.; Fernández-Segoviano, P.; Rodriguez, J.-M.; Aramburu, J.-A.; Peñuelas, O.; Cortés-Puch, I.; Cardinal-Fernández, P.; Lorente, J.A.; Frutos-Vivar, F. Comparison of the Berlin definition for acute respiratory distress syndrome with autopsy. Am. J. Respir. Crit. Care Med. 2013, 187, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef]
- Libby, L.J.; Gelbman, B.D.; Altorki, N.K.; Christos, P.J.; Libby, D.M. Surgical lung biopsy in adult respiratory distress syndrome: A meta-analysis. Ann. Thorac. Surg. 2014, 98, 1254–1260. [Google Scholar] [CrossRef]
- Papazian, L.; Thomas, P.; Bregeon, F.; Garbe, L.; Zandotti, C.; Saux, P.; Gaillat, F.; Drancourt, M.; Auffray, J.P.; Gouin, F. Open-lung biopsy in patients with acute respiratory distress syndrome. Anesthesiol. J. Am. Soc. Anesthesiol. 1998, 88, 935–944. [Google Scholar] [CrossRef]
- Villar, J. Dexamethasone treatment for the acute respiratory distress syndrome: A multicenter, randomized controlled trial. Lancet Respir. Med. 2020, 8, 267–276. [Google Scholar] [CrossRef]
- Meduri, G.U. Methylprednisolone infusion in early severe ARDS: Results of a randomized controlled trial. Chest 2007, 131, 954–963. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and me-ta-analyses: The PRISMA statement. PLoS Med. 2009, 21, 1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, K.C.; Tsai, Y.H.; Wu, Y.-K.; Chen, N.-H.; Hsieh, M.-J.; Huang, S.-F.; Huang, C.-C. Open lung biopsy in early-stage acute respiratory distress syndrome. Crit. Care 2006, 10, R106. [Google Scholar] [CrossRef] [Green Version]
- Soh, L.H.; Chian, C.F.; Su, W.L.; Yan, H.C.; Perng, W.C.; Wu, C.P. Role of open lung biopsy in patients with diffuse lung infiltrates and acute respiratory failure. J. Formos. Med. Assoc. 2005, 104, 17–21. [Google Scholar] [PubMed]
- Ortiz, G.; Garay, M.; Mendoza, D.; Cardinal-Fernández, P. Impact and safety of open lung biopsy in patients with acute respiratory distress syndrome (ARDS). Med. Intensiva 2019, 43, 139–146. [Google Scholar] [CrossRef]
- Philipponnet, C.; Cassagnes, L.; Pereira, B.; Kemeny, J.-L.; Devouassoux-Shisheboran, M.; Lautrette, A.; Guerin, C.; Souweine, B. Diagnostic yield and therapeutic impact of open lung biopsy in the critically ill patient. PLoS ONE 2018, 13, e0196795. [Google Scholar]
- Gerard, L.; Bidoul, T.; Castanares-Zapatero, D.; Wittebole, X.; Lacroix, V.; Froidure, A.; Hoton, D.; Laterre, P.-F. Open Lung Biopsy in Nonresolving Acute Respiratory Distress Syndrome Commonly Identifies Corticosteroid-Sensitive Pathologies, Associated with Better Outcome. Crit. Care Med. 2018, 46, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Almotairi, A.; Biswas, S.; Shahin, J. The role of open lung biopsy in critically ill patients with hypoxic respiratory failure: A retrospective cohort study. Can. Respir. J. 2016, 2016, 8715024. [Google Scholar] [CrossRef] [Green Version]
- Guerin, C.; Bayle, F.; Leray, V.; Debord, S.; Stoian, A.; Yonis, H.; Roudaut, J.B.; Bourdin, G.; Devouassoux-Shisheboran, M.; Bucher, E.; et al. Open lung biopsy in nonresolving ARDS frequently identifies diffuse alveolar damage regardless of the severity stage and may have implications for patient management. Intensive Care Med. 2015, 41, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, O.E.; Daeze, C.; Benoit, D.; Praet, M.; Vermassen, E.; Decruyenaere, M. Diagnostic potential of open lung biopsy in mechanically ventilated patients with diffuse pulmonary infiltrates of unclear aetiology. Anaesth. Intensive Care 2013, 41, 610–617. [Google Scholar] [CrossRef] [Green Version]
- Melo, N.; Figueiredo, S.; Morais, A.; Moura, C.S.; Pinho, P.; Bastos, P.; Oliveira, T. Open lung biopsy in patients on mechanical ventilation with suspected diffuse lung disease. Rev. Port. Pneumol. Engl. Ed. 2009, 15, 597–611. [Google Scholar] [CrossRef] [Green Version]
- Charbonney, E.; Robert, J.; Pache, J.-C.; Chevrolet, J.-C.; Eggimann, P. Impact of bedside open lung biopsies on the management of mechanically ventilated immunocompromised patients with acute respiratory distress syndrome of unknown etiology. J. Crit. Care 2009, 24, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Baumann, H.J.; Kluge, S.; Balke, L.; Yekebas, E.; Izbicki, J.R.; Amthor, M.; Kreymann, G.; Meyer, A. Yield and safety of bedside open lung biopsy in mechanically ventilated patients with acute lung injury or acute respiratory distress syndrome. Surgery 2008, 143, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.; Ahmed, R.; Ahmed, Q.; Rahman, M.U.; Yamani, N. Risks and benefits of open-lung biopsy in the mechanically ventilated critically ill population: A cohort study and literature review. Med. Sci. Monit. 2007, 13, CR365–CR371. [Google Scholar]
- Lim, S.Y.; Suh, G.Y.; Choi, J.C.; Koh, W.J.; Lim, S.Y.; Han, J.; Lee, K.S.; Shim, Y.M.; Chung, M.P.; Kim, H.; et al. Usefulness of open lung biopsy in mechanically ventilated patients with undiagnosed diffuse pulmonary infiltrates: Influence of comorbidities and organ dysfunction. Crit. Care 2007, 11, R93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papazian, L.; Doddoli, C.; Chetaille, B.; Gernez, Y.; Thirion, X.; Roch, A.; Donati, Y.; Bonnety, M.; Zandotti, C.; Thomas, P. A contributive result of open-lung biopsy improves survival in acute respiratory distress syndrome patients. Crit. Care Med. 2007, 35, 755–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbas, C.S.V.; Capelozzi, V.L.; Hoelz, C.; Magaldi, R.B.; Sandeville, M.L.; Werebe, E.; Filho, L.O.A.; Knobel, E. Impact of open lung biopsy on refractory acute respiratory failure. J. Bras. Pneumol. 2006, 32, 418–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapala, M.M.; Yuk, J.; Ahmed, N. Open lung biopsy yields diagnostically specific information that alters management in patients with ards: 79. Crit. Care Med. 2005, 33, A20. [Google Scholar] [CrossRef]
- Monteiro, A.S.; Addor, G.; Nigri, D.H.; Franco, C.A.B. Open lung biopsy in patients on mechanical ventilation and presenting diffuse pulmonary infiltrate. J. Bras. Pneumol. 2005, 31, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.R.; Karmpaliotis, D.; Ayas, N.T.; Mark, E.J.; Wain, J.; Thompson, B.T.; Malhotra, A. The role of open-lung biopsy in ARDS. Chest 2004, 125, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Flabouris, A.; Myburgh, J. The utility of open lung biopsy in patients requiring mechanical ventilation. Chest 1999, 115, 811–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, R.; McGuire, G. Evaluation of open lung biopsy in critically ill, ventilator dependent intensive care unit patients. Can. Respir. J. 1997, 4, 246–250. [Google Scholar] [CrossRef] [Green Version]
- Canver, C.C.; Mentzer, R.M., Jr. The role of open lung biopsy in early and late survival of ventilator-dependent patients with diffuse idiopathic lung disease. J. Cardiovasc. Surg. 1994, 35, 151–155. [Google Scholar]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyazaki, Y.; Tateishi, T.; Akashi, T.; Ohtani, Y.; Inase, N.; Yoshizawa, Y. Clinical predictors and histologic appearance of acute exacerbations in chronic hypersensitivity pneumonitis. Chest 2008, 134, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Horita, N.; Hashimoto, S.; Miyazawa, N.; Fujita, H.; Kojima, R.; Inoue, M.; Ueda, A.; Ishigatsubo, Y.; Kaneko, T. Impact of Corticosteroids on Mortality in Patients with Acute Respiratory Distress Syndrome: A Systematic Review and Meta-analysis. Intern. Med. 2015, 54, 1473–1479. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, J.P.; Fogarty, A.W.; McKeever, T.M.; Hubbard, R.B. In-Hospital Mortality after Surgical Lung Biopsy for Interstitial Lung Disease in the United States. 2000 to 2011. Am. J. Respir. Crit. Care Med. 2016, 193, 1161–1167. [Google Scholar] [CrossRef]
- Castro, C.Y. ARDS and diffuse alveolar damage: A pathologist’s perspective. Semin. Thorac. Cardiovasc. Surg. 2006, 18, 13–19. [Google Scholar] [CrossRef]
- Wong, A.K.; Walkey, A.J. Open lung biopsy among critically ill, mechanically ventilated patients. A meta analysis. Ann. Am. Thorac. Soc. 2015, 12, 1226–1230. [Google Scholar] [CrossRef] [Green Version]
- Bensard, D.D.; McIntyre, R.C., Jr.; Waring, B.J.; Simon, J.S. Comparison of video thoracoscopic lung biopsy to open lung biopsy in the diagnosis of interstitial lung disease. Chest 1993, 103, 765. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Type | n | Age (Mean ± SD) | Males n (%) | PaO2/FiO2 (mmHg) Mean ± SD | PEEP (cm H2O), Mean ± SD |
|---|---|---|---|---|---|---|---|
| Ortiz 2018 [14] | Columbia | Retrospective | 15 | 42 ± 18 | 7 (47) | 121 ± 0 | 13 ± 0 |
| Philipponnet 2018 [15] | France | Retrospective | 46 | 69 ± 5 | 33 (71) | 180 ± 89 | - |
| Gerard 2018 [16] | Belgium | Retrospective | 51 | 65 ± 7 | 28 (55) | 128 ± 0 | 9 ± 2 |
| Almotairi 2016 [17] | Canada | Retrospective | 76 | 63 ± 4 | 41 (54) | 136 ± 24 | - |
| Guerin 2015 [18] | France | Retrospective | 83 | 64 ± 6 | 35 (56) | - | - |
| Depuydt 2013 [19] | Belgium | Retrospective | 60 | 62 ± 14 | 36 (60) | 189 ± 0 | 8 ± 1 |
| Melo 2009 [20] | Portugal | Retrospective | 19 | 58 ± 16 | 10 (53) | 171 ± 0 | 9 ± 0 |
| Charbonney 2009 [21] | Switzerland | Retrospective | 19 | 50 ± 5 | 11 (58) | 119 ± 34 | 6 ± 3 |
| Baumann 2008 [22] | Germany | Retrospective | 27 | 48 ± 14 | 12 (44) | 188 ±109 | - |
| Arabi 2007 [23] | Saudi Arabia | Retrospective | 14 | 51 ± 19 | 7 (50) | 150 ± 60 | 8 ± 4 |
| Lim 2007 [24] | South Korea | Retrospective | 36 | 59 ± 0 | 25 (69) | 159 ± 0 | 11 ± 4 |
| Papazian 2007 [25] | France | Prospective | 100 | 57 ± 17 | 67 (67) | 129 ± 14 | 10 ± 3 |
| Barbas 2006 [26] | Brazil | Retrospective | 12 | 65 ± 14 | 5 (42) | 157 ± 0 | - |
| Kao 2006 [12] | Taiwan | Retrospective | 41 | 55 ± 17 | 28 (68) | 116 ± 43 | 11 ± 3 |
| Soh 2005 [13] | Taiwan | Retrospective | 32 | 51 ± 22 | 24 (75) | 163 ± 90 | - |
| Kapala 2005 [27] | Brazil | Retrospective | 13 | 66 ± 0 | - | - | - |
| Monteiro 2005 [28] | Brazil | Retrospective | 24 | 65 ± 0 | 12 (50) | - | - |
| Patel 2004 [29] | USA | Retrospective | 57 | 53 ± 18 | 36 (65) | 145 ± 61 | 10 ± 4 |
| Flabouris 1999 [30] | Australia | Retrospective | 24 | 49 ±16 | 8 (33) | 161 ± 0 | - |
| Papazian 1998 [8] | France | Prospective | 36 | 59 ± 15 | - | 122 ± 37 | 10 ± 0 |
| Hughes 1997 [31] | Canada | Retrospective | 27 | 57 ± 0 | 14 (52) | - | - |
| Canver 1994 [32] | USA | Retrospective | 92 | 51 ± 5 | 13 (48) | - | 9 ± 1 |
| Univariate: Coefficient of Variation (p) | Multivariate: Coefficient of Variation (p) | |||||
|---|---|---|---|---|---|---|
| Age | Male | Study Type | Age | Male | Study Type | |
| Air-leak | 0.98 (0.5) | 1.01 (0.2) | 0.57 (0.1) | 0.97 (0.3) | 1.02 (0.76) | 0.36 (0.06) |
| Morality | 1.02 (0.1) | 1.00 (0.6) | 0.89 (0.6) | 1.01 (0.1) | 1.00 (0.9) | 0.85 (0.6) |
| Complications | 0.98 (0.4) | 1.00 (0.6) | 0.87 (0.7) | 0.98 (0.3) | 1.01 (0.5) | 1.20 (0.7) |
| CIM | 1.01 (0.2) | 1.00 (0.9) | 1.18 (0.4) | 1.01 (0.3) | 1.00 (0.7) | 1.11 (0.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mir, T.; Regmi, N.; Saydain, G.; Kaul, V.; Soubani, A.O.; Qureshi, W.T. Outcome and Post-Surgical Lung Biopsy Change in Management of ARDS: A Proportional Prevalence Meta-Analysis. Adv. Respir. Med. 2022, 90, 267-278. https://doi.org/10.3390/arm90040036
Mir T, Regmi N, Saydain G, Kaul V, Soubani AO, Qureshi WT. Outcome and Post-Surgical Lung Biopsy Change in Management of ARDS: A Proportional Prevalence Meta-Analysis. Advances in Respiratory Medicine. 2022; 90(4):267-278. https://doi.org/10.3390/arm90040036
Chicago/Turabian StyleMir, Tanveer, Neelambuj Regmi, Ghulam Saydain, Viren Kaul, Ayman O. Soubani, and Waqas T. Qureshi. 2022. "Outcome and Post-Surgical Lung Biopsy Change in Management of ARDS: A Proportional Prevalence Meta-Analysis" Advances in Respiratory Medicine 90, no. 4: 267-278. https://doi.org/10.3390/arm90040036