
Assessing the Incidence of Snakebites in Rural Gabon—A Community-Based, Cross-Sectional Pilot Survey

 , , , and
, , , and 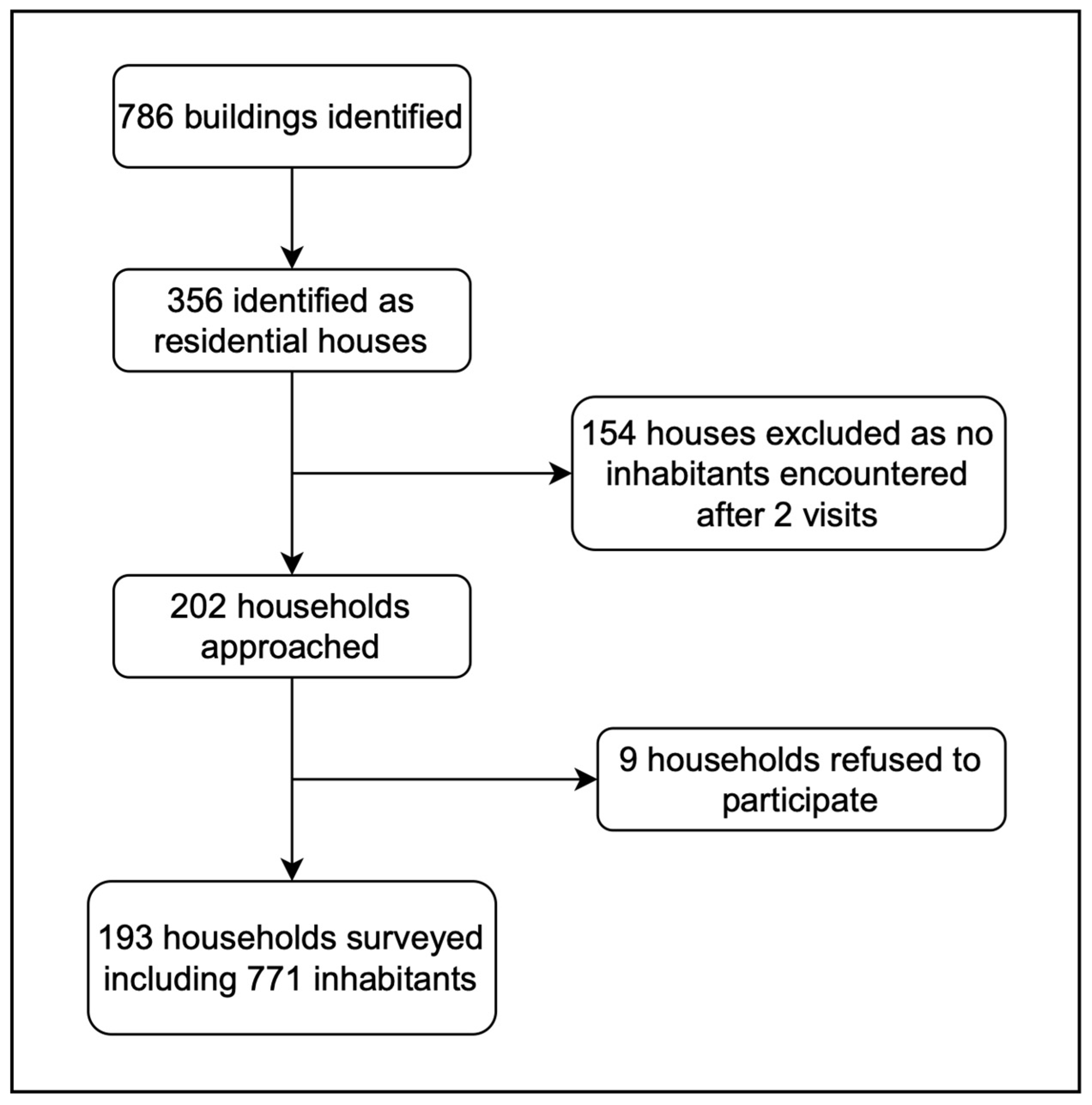{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Study Population
2.2. Prevalence of Snakebites and Risk Factors
3. Discussion
4. Materials and Methods
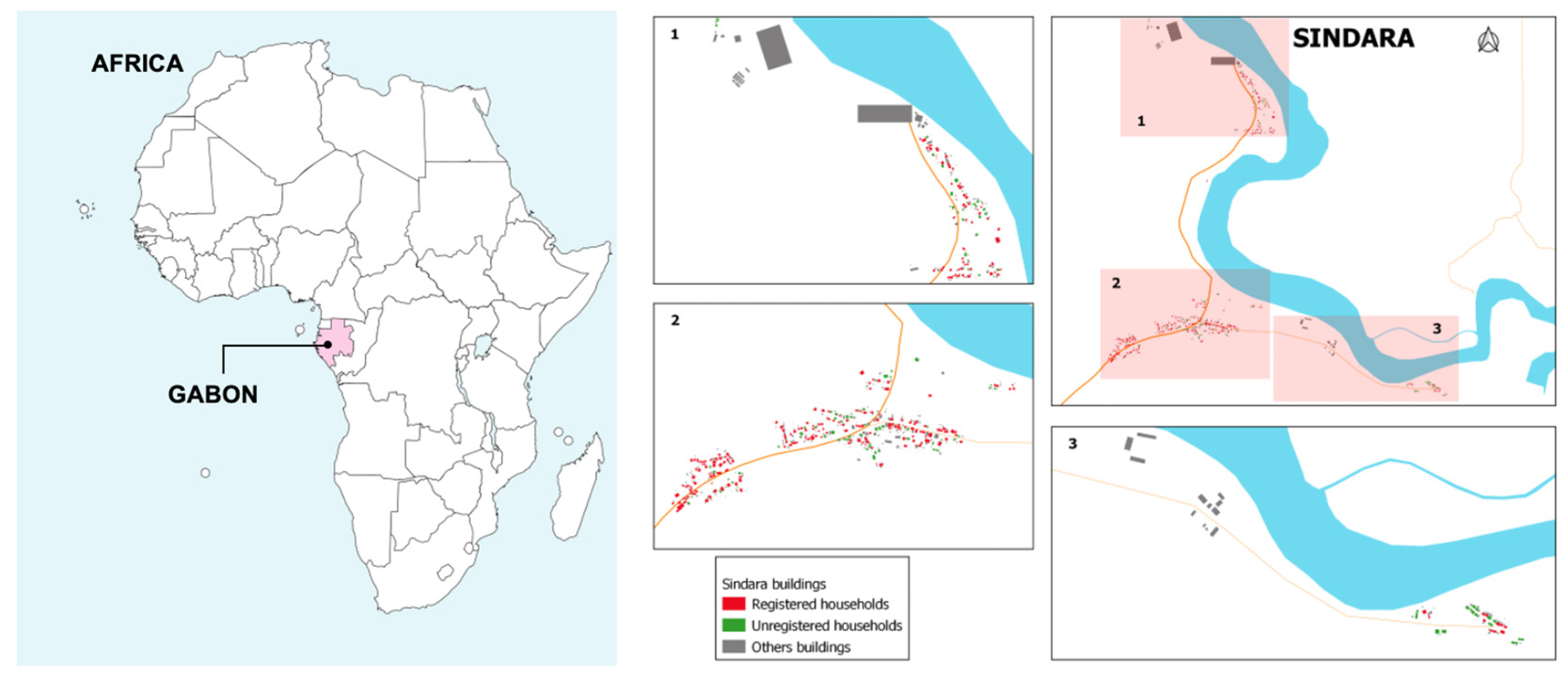
4.1. Study Setting
4.2. Study Design and Procedures
Demographic and Health Surveillance System
4.3. Questionnaire Design
4.4. Data Collection
4.5. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Snakebite Envenoming. Available online: https://www.who.int/news-room/fact-sheets/detail/snakebite-envenoming (accessed on 25 March 2023).
- Chippaux, J.P. Snake-bites: Appraisal of the global situation. Bull. World Health Organ. 1998, 76, 515–524. [Google Scholar] [PubMed]
- Kasturiratne, A.; Wickremasinghe, A.R.; de Silva, N.; Gunawardena, N.K.; Pathmeswaran, A.; Premaratna, R.; Savioli, L.; Lalloo, D.G.; de Silva, H.J. The global burden of snakebite: A literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS Med. 2008, 5, e218. [Google Scholar] [CrossRef] [PubMed]
- Maurice, M.; Veronique, M.; Ebong, E.; Laura, N.; Chutame, C. The Assessment of Human-Snake Interaction and its Outcome in the City of Kumba. Int. J. For. Anim. Fish. Res. 2018, 2, 74–83. [Google Scholar] [CrossRef]
- Pauwels, O. Slippery Customers; Royal Belgian Institute of Natural Sciences: Brussels, Belgium, 2009. [Google Scholar]
- Tchoua, R.; Raouf, A.O.; Ogandaga, A.; Mouloungui, C.; Loussou, J.B.; Kombila, M.; Nsafu, D.N. Analysis of snake bite envenomations in Gabon. Bull. Soc. Pathol. Exot. 2002, 95, 188–190. [Google Scholar] [PubMed]
- Aron, M.B.; Kachimanga, C.; Kreuels, B.; Mailosi, B.; Sambani, C.; Matanje, B.L.; Blessmann, J.; Chunga, M.; Momba, G.; Ndarama, E.; et al. Health care workers’ knowledge on identification, management and treatment of snakebite cases in rural Malawi: A descriptive study. PLoS Negl. Trop. Dis. 2022, 16, e0010841. [Google Scholar] [CrossRef] [PubMed]
- Musah, Y.; Ameade, E.P.K.; Attuquayefio, D.K.; Holbech, L.H. Epidemiology, ecology and human perceptions of snakebites in a savanna community of northern Ghana. PLoS Negl. Trop. Dis. 2019, 13, e0007221. [Google Scholar] [CrossRef] [PubMed]
- Pandey, D.P.; Subedi Pandey, G.; Sapkota, S.; Dangol, D.R.; Devkota, N.R. Attitudes, knowledge and practices of traditional snakebite healers in Nepal: Implications for prevention and control of snakebite. Trans. R. Soc. Trop. Med. Hyg. 2022, 117, 219–228. [Google Scholar] [CrossRef] [PubMed]
- WHO. Snakebite Envenoming: A Strategy for Prevention and Control; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Roberts, N.L.S.; Johnson, E.K.; Zeng, S.M.; Hamilton, E.B.; Abdoli, A.; Alahdab, F.; Alipour, V.; Ancuceanu, R.; Andrei, C.L.; Anvari, D.; et al. Global mortality of snakebite envenoming between 1990 and 2019. Nat. Commun. 2022, 13, 6160. [Google Scholar] [CrossRef]
- Chippaux, J.P.; Rage-Andrieux, V.; Le Mener-Delore, V.; Charrondiere, M.; Sagot, P.; Lang, J. Epidemiology of snake envenomations in northern Cameroon. Bull. Soc. Pathol. Exot. 2002, 95, 184–187. [Google Scholar]
- Chippaux, J.P. Estimate of the burden of snakebites in sub-Saharan Africa: A meta-analytic approach. Toxicon 2011, 57, 586–599. [Google Scholar] [CrossRef] [PubMed]
- Fita, D.S.; Costa Neto, E.M.; Schiavetti, A. ‘Offensive’ snakes: Cultural beliefs and practices related to snakebites in a Brazilian rural settlement. J. Ethnobiol. Ethnomed. 2010, 6, 13. [Google Scholar] [CrossRef] [PubMed]
- Steinhorst, J.; Tianyi, F.L.; Habib, A.G.; Oluoch, G.O.; Lalloo, D.G.; Stienstra, Y. Uniting behind a common goal: Collaboration between traditional healers and allopathic health care workers to improve rural snakebite care. Toxicon X 2022, 16, 100140. [Google Scholar] [CrossRef] [PubMed]
- World Bank Group. Climate Knowledge Portal: Country Gabon. Available online: https://climateknowledgeportal.worldbank.org/country/gabon/climate-data-historical (accessed on 23 August 2022).
- Manego, R.Z.; Mombo-Ngoma, G.; Witte, M.; Held, J.; Gmeiner, M.; Gebru, T.; Tazemda, B.; Mischlinger, J.; Groger, M.; Lell, B.; et al. Demography, maternal health and the epidemiology of malaria and other major infectious diseases in the rural department Tsamba-Magotsi, Ngounie Province, in central African Gabon. BMC Public Health 2017, 17, 130. [Google Scholar] [CrossRef] [PubMed]
- Vongphoumy, I.; Phongmany, P.; Sydala, S.; Prasith, N.; Reintjes, R.; Blessmann, J. Snakebites in Two Rural Districts in Lao PDR: Community-Based Surveys Disclose High Incidence of an Invisible Public Health Problem. PLoS Negl. Trop. Dis. 2015, 9, e0003887. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davi, S.D.; Lumeka, A.; Hildebrandt, T.R.; Endamne, L.R.; Otchague, C.; Okwu, D.G.; Artus, R.; Hunstig, F.; Manego, R.Z.; Blessmann, J.; et al. Assessing the Incidence of Snakebites in Rural Gabon—A Community-Based, Cross-Sectional Pilot Survey. Trop. Med. Infect. Dis. 2024, 9, 68. https://doi.org/10.3390/tropicalmed9040068
Davi SD, Lumeka A, Hildebrandt TR, Endamne LR, Otchague C, Okwu DG, Artus R, Hunstig F, Manego RZ, Blessmann J, et al. Assessing the Incidence of Snakebites in Rural Gabon—A Community-Based, Cross-Sectional Pilot Survey. Tropical Medicine and Infectious Disease. 2024; 9(4):68. https://doi.org/10.3390/tropicalmed9040068
Chicago/Turabian StyleDavi, Saskia Dede, Anita Lumeka, Teite Rebecca Hildebrandt, Lilian Rene Endamne, Cedric Otchague, Dearie Glory Okwu, Rica Artus, Friederike Hunstig, Rella Zoleko Manego, Jörg Blessmann, and et al. 2024. "Assessing the Incidence of Snakebites in Rural Gabon—A Community-Based, Cross-Sectional Pilot Survey" Tropical Medicine and Infectious Disease 9, no. 4: 68. https://doi.org/10.3390/tropicalmed9040068