
Very Prolonged Treatment with Albendazole of a Case of Disseminated Abdominal Cystic Echinococcosis
 ,
,
Abstract
:1. Introduction
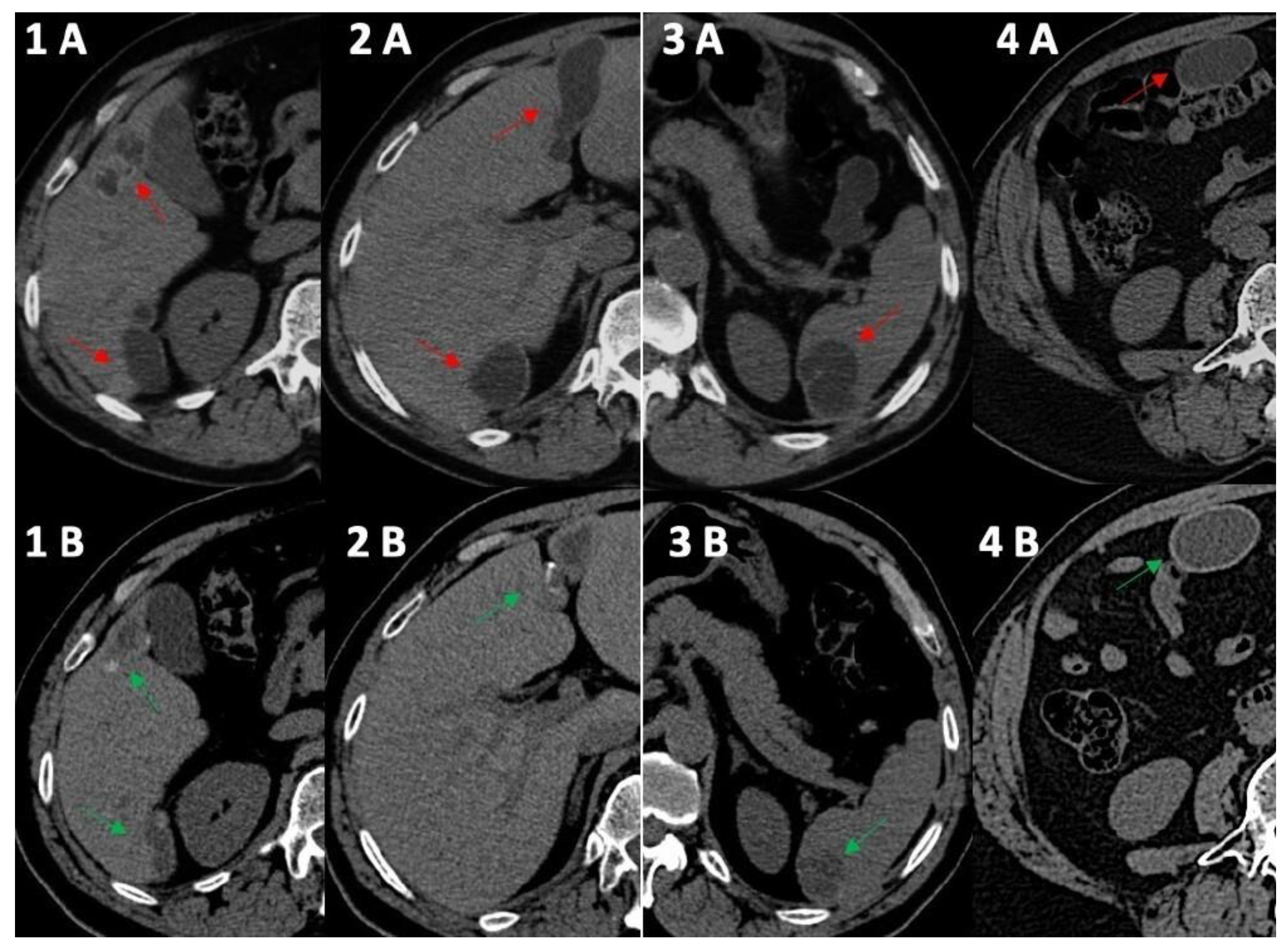
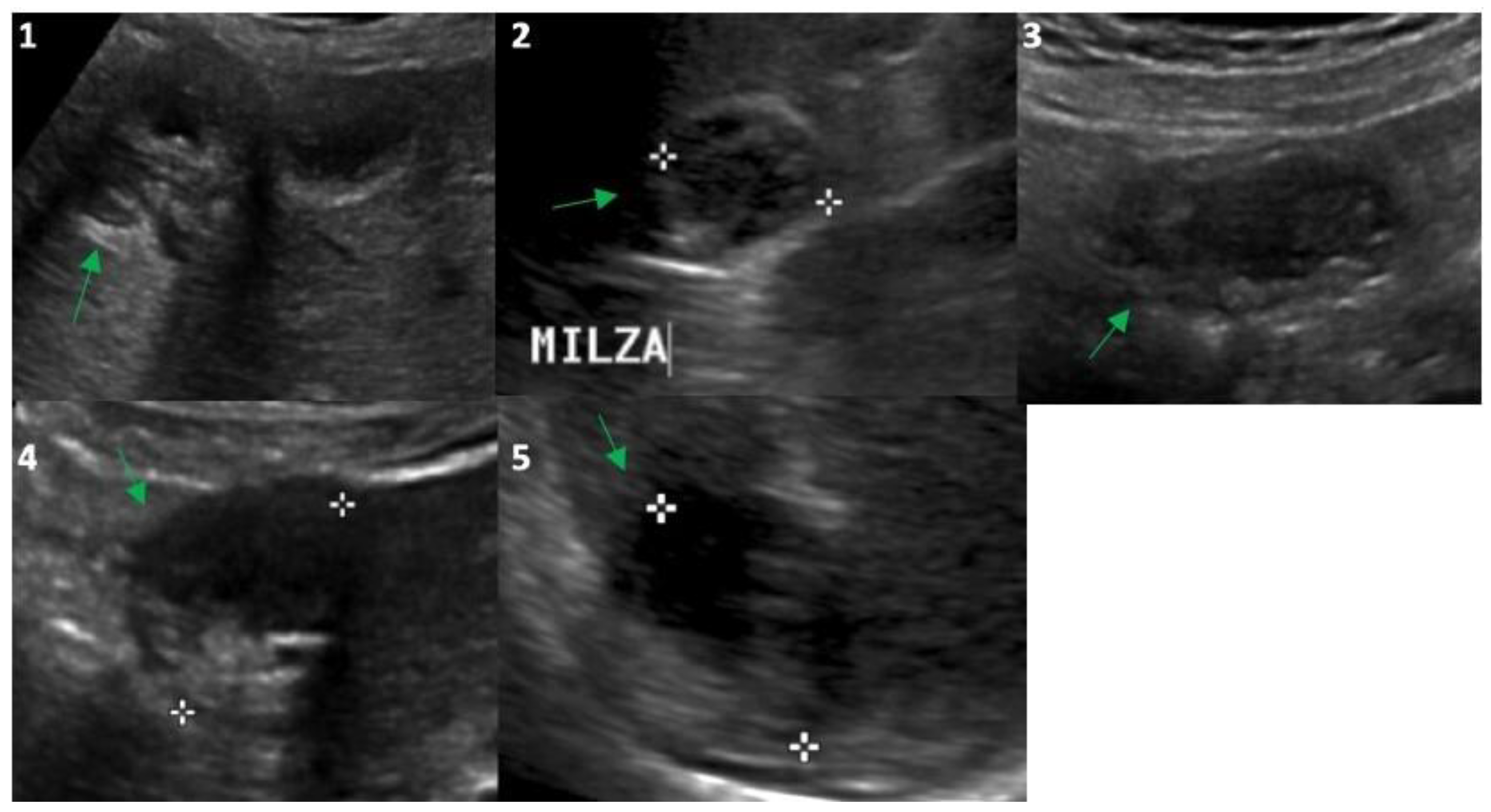
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agudelo Higuita, N.I.; Brunetti, E.; McCloskey, C. Cystic Echinococcosis. J. Clin. Microbiol. 2016, 54, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Deplazes, P.; Rinaldi, L.; Alvarez Rojas, C.A.; Torgerson, P.R.; Harandi, M.F.; Romig, T.; Antolova, D.; Schurer, J.M.; Lahmar, A.; Cringoli, G.; et al. Global Distribution of Alveolar and Cystic Echinococcosis. Adv. Parasitol. 2017, 95, 315–493. [Google Scholar] [CrossRef] [PubMed]
- Gabriele, F.; Bortoletti, G.; Conchedda, M.; Palmas, C.; Ecca, A.R. Idatidosi cistica umana in Italia: Un problema di salute pubblica? Passato e presente [Human cystic hydatidosis in Italy: A public health emergency? Past to present]. Parassitologia 2004, 46, 39–43. [Google Scholar] [PubMed]
- Majbar, M.A.; Souadka, A.; Sabbah, F.; Raiss, M.; Hrora, A.; Ahallat, M. Peritoneal echinococcosis: Anatomoclinical features and surgical treatment. World J. Surg. 2012, 36, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Teggi, A.; Lastilla, M.G.; De Rosa, F. Therapy of human hydatid disease with mebendazole and albendazole. Antimicrob. Agents Chemother. 1993, 37, 1679–1684. [Google Scholar] [CrossRef] [PubMed]
- Junghanss, T.; da Silva, A.M.; Horton, J.; Chiodini, P.L.; Brunetti, E. Clinical management of cystic echinococcosis: State of the art, problems, and perspectives. Am. J. Trop. Med. Hyg. 2008, 79, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Salinas, J.C.; Torcal, J.; Lozano, R.; Sousa, R.; Morandeira, A.; Cabezali, R. Intracystic infection of liver hydatidosis. Hepatogastroenterology 2000, 47, 1052–1055. [Google Scholar] [PubMed]
- Horton, R.J. Albendazole in treatment of human cystic echinococcosis14: 12 years of experience. Acta Trop. 1997, 64, 79–93. [Google Scholar] [CrossRef] [PubMed]
- Mihmanli, M.; Idiz, U.O.; Kaya, C.; Demir, U.; Bostanci, O.; Omeroglu, S.; Bozkurt, E. Current status of diagnosis and treatment of hepatic echinococcosis. World J. Hepatol. 2016, 8, 1169–1181. [Google Scholar] [CrossRef] [PubMed]
- Collado-Aliaga, J.; Romero-Alegría, Á.; Alonso-Sardón, M.; López-Bernus, A.; Galindo-Pérez, I.; Muro, A.; Velasco-Tirado, V.; Muñoz Bellido, J.L.; Belhassen-García, M.; Pardo-Lledias, J. Eosinophilia and cystic echinococcosis: What is the relationship? Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 6–22. [Google Scholar] [CrossRef] [PubMed]
- Mirabile, E.; Solomon, N.; Fields, P.J.; Macpherson, C.N.L. Progress towards international adoption of the World Health Organization ultrasound classification of cystic echinococcosis. Acta Trop. 2019, 189, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Casulli, A. New global targets for NTDs in the WHO roadmap 2021–2030. PLoS Negl. Trop. Dis. 2021, 15, e0009373. [Google Scholar] [CrossRef]
- Mandal, S.; Mandal, M.D. Human cystic echinococcosis: Epidemiologic, zoonotic, clinical, diagnostic and therapeutic aspects. Asian Pac. J. Trop. Med. 2012, 5, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Obeid, M.; Mansour, S.; Damouny, M.; Farah, A.; Halloun, K.; Marjiyeh, R.; Ghalia, J.; Khuri, S. A conservative management of spontaneously ruptured liver hydatid cyst. Gastroenterol. Res. 2021, 14, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Zavoikin, V.D.; Zelya, O.P.; Tumolskaya, N.I. Clinical tolerance and efficacy of anti-parasitic treatment with albendazole in patients with alveolar echinococcosis: Long-term follow-up observation in 117 patients. Parasitol. Res. 2021, 120, 3603–3610. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, L.; Manciulli, T.; Cretu, C.M.; Giordani, M.T.; Angheben, A.; Bartoloni, A.; Zammarchi, L.; Bartalesi, F.; Richter, J.; Chiodini, P.; et al. Cystic echinococcosis of the bone: A European multicenter study. Am. J. Trop. Med. Hyg. 2019, 100, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Pedrosa, I.; Saíz, A.; Arrazola, J.; Ferreirós, J.; Pedrosa, C.S. Hydatid disease: Radiologic and pathologic features and complications. Radiographics 2000, 20, 795–817. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Year | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Month | Jul. | Mar. | Jul. | Oct. | Nov. | Oct. | Oct. | Oct. | Sep. | Gen. | May | Nov. |
| IgG anti-echinococcus (titers) | 1/6400 | 1/6400 | 1/6400 | 1/3200 | 1/3200 | 1/1600 | 1/1600 | 1/800 | 1/800 | 1/400 | - | 1/200 |
| ABZ cycles | 2 | - | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 1 |
| AST (U/L) | 140 | 198 | 58 | 19 | 27 | 23 | 28 | 22 | 26 | 24 | 16 | 20 |
| ALT (U/L) | 358 | 308 | 60 | 13 | 28 | 30 | 33 | 35 | 32 | 30 | 13 | 28 |
| GGT (U/L) | 179 | 268 | 101 | 32 | 19 | 29 | 27 | 32 | 30 | 28 | 25 | 34 |
| White blood cells (n/mmc) | 7920 | 7100 | 7430 | 7400 | 7500 | 10,100 | ||||||
| Eosinophils (%) | 2.7 | 3.5 | 4.6 | 2.6 | 1.6 | 1.0 | ||||||
| Hemoglobin (g/dL) | 12.7 | 12.0 | 12.2 | 12.4 | 12.3 | 12.5 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buscemi, C.; Randazzo, C.; Buscemi, P.; Caldarella, R.; Lombardo, M.; Buscemi, S. Very Prolonged Treatment with Albendazole of a Case of Disseminated Abdominal Cystic Echinococcosis. Trop. Med. Infect. Dis. 2023, 8, 449. https://doi.org/10.3390/tropicalmed8090449
Buscemi C, Randazzo C, Buscemi P, Caldarella R, Lombardo M, Buscemi S. Very Prolonged Treatment with Albendazole of a Case of Disseminated Abdominal Cystic Echinococcosis. Tropical Medicine and Infectious Disease. 2023; 8(9):449. https://doi.org/10.3390/tropicalmed8090449
Chicago/Turabian StyleBuscemi, Carola, Cristiana Randazzo, Paolo Buscemi, Rosalia Caldarella, Martina Lombardo, and Silvio Buscemi. 2023. "Very Prolonged Treatment with Albendazole of a Case of Disseminated Abdominal Cystic Echinococcosis" Tropical Medicine and Infectious Disease 8, no. 9: 449. https://doi.org/10.3390/tropicalmed8090449