
Procedure for Handling and Storage of Onchocerca volvulus Microfilariae Obtained from Skin Snips for Downstream Genetic Work

 , ,
, ,  , , , , ,
, , , , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Design
2.1. Microfilariae Transfer for Genetic Analysis from a 2018 Epidemiological Study in the Maridi Health District of South Sudan without the Newly Developed Procedure
2.2. Microfilariae Transfer for Genetic Analysis from the Ongoing Trials in DRC with the New Procedures
3. Overview of the Procedure
- After counting, the procedure for transfer and storage of mf is designed to reduce researcher workload and fatigue-related human error as follows:
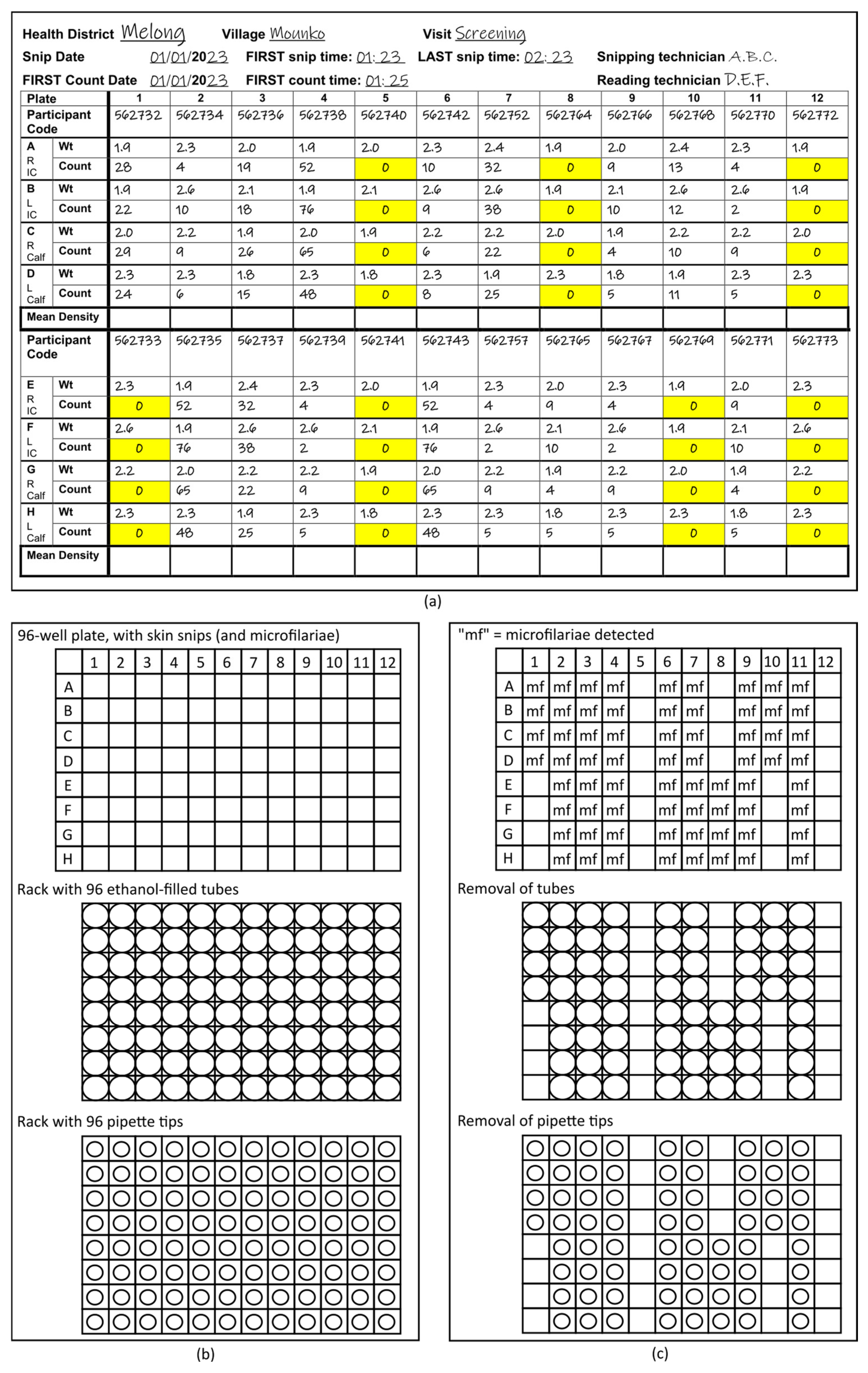
- Use of the “96-format” (12 columns and 8 rows) throughout the process. For the incubation of the mf in 0.9% saline before counting, the Source Record Forms (Figure 1a) on which the parasitologists record the number of mf counted microscopically in each well (Supplemental File: Source Record Forms for four or two skin snips per participant) and the racks with ethanol-filled tubes into which the mf are transferred. The 96-format is also taken into consideration by use of racks with 96 pipette tips and either 8-channel or 12-channel pipettes.
- Labelling of the 96-format racks, rather than individual tubes with mf, using positional information to associate wells in the 96-well plates in which the skin snips are incubated, corresponding metadata on the 96-format Source Record Form and the individual tubes in the 96-tube racks into which the mf are transferred from the 96-well plates (Figure 1b,c).
- Each rack used has a unique identifier or barcode. That barcode is entered into a label printer and printed in duplicate. Both printed labels are attached to the rack: one will remain on the rack, the other will be attached to the Source Record Form that includes the metadata for the mf to unambiguously link the samples that will be transferred to tubes in the rack with the Source Record Form.
- To reduce the probability of sample loss through the use of the following:
- Screw-top tubes, which reduce evaporation and accidental opening during handling and shipping.
- Racks with a lockable lid, which prevent tubes from falling out of place during transport. This is critical for a procedure that eliminates the workload and potential errors associated with labelling many tubes individually by associating tube position with metadata.
- To preserve resources.
4. Materials
4.1. Equipment
- 8-channel pipette (or 12-channel pipette), 20–200 µL volume.
- Tweezers.
- Uncapping tool (e.g., Azenta Screw Cap Remover) or flathead screwdriver, or other mechanism to facilitate unscrewing tubes.
- Label printer for duplicating rack barcode information (or generating barcode information if case racks without imprinted barcodes are used).
4.2. Consumables
- Nitrile or vinyl protective gloves.
- Permanent marker.
- 10 mL reagent reservoirs (“long containers”) designed for repeated filling of 8- (or 12-) channel pipettes.
- 1 mL screw-top tubes, slender enough for 8-channel pipette use (96-format) and suitable for cold storage. Tubes certified for use at freezing temperatures with external thread recommended (e.g., Azenta FluidX Next-Gen 1.0 mL jacket tube, 68-1003-11).
- 96-format tube racks (i.e., 8 × 12), with imprinted, human- (and possibly also machine-) readable barcodes, with a lockable lid (e.g., Azenta FluidX Next-Gen high-rise rack with standard lid lock, 66-51020) for ethanol-filled tubes.
- Additional 96-format tube racks for placing unused ethanol-filled tubes (see Detailed Procedure below).
- Biohazard container for the 96-well plates after mf transfer to the tubes.
- Biohazard container for used pipette tips.
- Racked pipette tips, 200 µL (96-format, i.e., 12 columns and 8 rows).
4.3. Solutions
- Ethanol, molecular grade, pure.
- 0.9% NaCl solution (approximately 10 mL per 96-well plate).
4.4. Counted Microfilariae and Associated Metadata
- 96-well plates with the skin snips and mf in 0.9% saline, after the mf have been counted and the designated staff has released the plate for mf transfer.
- Photocopy of completed Source Record Forms of a quality that ensures that all writing is readable (blank forms for studies that use two or four skin snips are available in the Supplemental File).
5. Detailed Procedure
5.1. Preparatory Work
- Pre-fill tubes with 500–600 μL ethanol (≥99.5%). Ensure caps are tight to reduce evaporation and reduce the risk of spilling.
- For each rack, print 2× labels with a unique alpha-numeric code. If the rack already has an imprinted code (i.e., pressed into the plastic frame), use the same alpha-numeric barcode as on the rack. Compare the printed barcode to the one imprinted on the rack to ensure they are identical and print new labels if they do not correspond. Stick one label on the rack itself (i.e., not on the lid). The other should be stuck on the outside of the rack such that it is easily detachable (it will be affixed to the Source Record Form in step 8). This step ensures that the label on the rack and the label on the Source Record Form will be identical in the case of a typo in the printed rack label relative to the imprinted rack barcode.
- Fill the long containers (reagent reservoirs) with NaCl (0.9%).
- Set the 8-channel (or 12-channel) pipette to 100 μL.
- Match the photocopies of the completed Source Record Form and the 96-well plates with the mf via the Plate Identifier on the top left corner of the Source Record Form.
5.2. Transfer of Microfilariae
- 1.
- Review the photocopy of the completed Source Record Form to identify any wells that have mf (Figure 1a).
- 2.
- Align the first 96-well plate with the mf to be transferred and the rack with 96 tubes into which the mf will be transferred. Unless the rack positions are labelled, a standard approach for ensuring that the racks are facing the same way across institutions working on the same project is important. With the brand of racks used in our study, the alpha-numeric, pre-printed barcode were oriented on the left side, while the pre-printed labels are on the front facing the laboratory staff. This ensures that the material in, e.g., plate well A1 (corresponding to the counts and participant code on the Source Record Form for well A1) is transferred to the first tube A1 in the upper left of the rack. This is key to eliminating the need for labelling individual tubes (Figure 1b).
- 3.
- Remove one of the detachable barcode labels from the rack and stick it to the Source Record Form copy.
- 4.
- Unlock the rack lid and place it face up on the counter.
- 5.
- Remove those tubes in the rack that correspond to positions in the 96-well plate with 0 mf and place them into empty racks for later use (Figure 1c).NB: This may result in entire columns or rows without tubes since the position of the tubes remaining in the rack must correspond exactly to the position of wells with mf in the 96-well plate. While this step increases workload for laboratory staff during mf transfer, it reduces waste of ethanol-filled tubes, shipping weight, and time required for filling tubes with ethanol for future mf transfers.NB: for the brand used in our study, the orange capping tool can be used to push tubes out from the bottom of the rack if needed.
- 6.
- Line up the 96-pipette tip rack with the 96-well plate and the 96-well tube rack (Figure 1b).
- 7.
- Remove those pipette tips that correspond to positions in the first column of wells of the 96 well plate without mf and place them into the tray (they will be later placed into an empty 96-pipette rack) (Figure 1b).
- 8.
- Starting with the wells in column 1, corresponding to wells A1–A8 in the 96-well plate (or the first column of wells in which at least one well includes mf), follow the procedure given below:
- a.
- Remove the screw tops of the tubes (using the orange capping tool, flathead screwdriver, or by hand) and place them in the rack lid.
- b.
- Equip the pipette with tips for each of the positions corresponding to wells containing mf.
- c.
- Pipette the contents of the wells gently up and down three or four times to ensure that mf are pipetted up.NB: It is important that this step is GENTLE. Sudden or jerky pipette plunger action will increase the risk of mf being sucked into the pipette channels, contaminating the pipette and leading to loss of mf.NB: Take care NOT to include the skin snip in the well. The pipette tip orifice should be too small to allow accidental pipetting of the skin snip, but attention needs to be paid to this and the fact that the skin snip may temporarily block the orifice.
- d.
- Transfer the contents into the corresponding tubes in the rack.
- e.
- Set the pipette volume to 50 µL.
- f.
- Pipette up 50 µL NaCl from the long container.
- g.
- Transfer the 50 µL NaCl into the wells from which the mf were just transferred.
- h.
- Pipette up and down gently three or four times to rinse the wells—following the notes above.
- i.
- Transfer the 50 µL to the corresponding tubes in the rack (final ethanol concentration in the tubes ≥74%).
- j.
- Inspect the wells to confirm that the skin biopsy is still in there. For any well without a visible skin biopsy inspect the corresponding tube in the rack for the skin snip and remove with tweezers if necessary.
- k.
- Eject the pipette tips into the biowaste container.
- l.
- Re-cap the tubes in the column, ensuring that each tube is firmly closed.
- 9.
- Repeat this step for all non-empty columns 2–12.
- 10.
- Replace the lid on the rack and lock it.
- 11.
- Discard the 96-well plate into the designated biowaste container.
5.3. Storage of Consumables for Re-Use
- Place the ethanol-tubes not needed for preservation of mf (because their position corresponded to a well without mf) into EMPTY tube racks. Once all positions in the rack have been filled, the tube rack can be used for transfer of mf as per Section 5.1.
- Place all pipette tips not used (because their position corresponded to a well without mf) into an empty pipette tip rack. Once all positions in the rack have been filled, the rack can be used for future transfer of mf as per Section 5.1.
6. Methods for Comparison of Suitability of Microfilariae Samples Transferred without and with Our New Procedure for Genetic Analysis
6.1. Picking of Microfilariae
6.2. DNA Extraction, Amplification, and Sequencing
6.2.1. DNA Extraction
- Lysis buffer was prepared using 10 mM Tris-HCl pH 8.0, 1 mM EDTA pH 8.0, and 1% Tween®20 (Sigma-Aldrich, Burlington, MA, USA), with 300 µg/mL proteinase K added just prior to use. Lysis buffer can be stored at 8 °C for no more than 24 h before use.
- Wells each containing a single mf in lysis buffer were incubated at 55 °C for 2 h, followed by heat inactivating the solution at 80 °C or 85 °C for 20 min.
6.2.2. Detection of DNA in the Crude Lysate Using qPCR
- Primers were used to target a 67 bp region of the mitochondrial genome [22]: forward primer, SP-Ov-mt-10062 (5′-ttg att caa tat cag gga cgt a-3′); reverse primer, ASP-Ov-mt-10062 (5′-att ggt gac caa taa cct tca-3′). As a positive control, an oligonucleotide of the mitochondrial (mt) target sequence was synthesized (5′-ttg att caa tat cag gga cgt ata ttt cgt caa tct gag ttg act ttg aag gtt att ggt cac caa t-3′). For a 66 bp region of the nuclear genome: SP_Ov_OM4_4192352 (5′-tta gag gcc ctt tcg cag t-3′) and ASP_Ov_OM4_4192352 (5′-cag cac tga tcc cgg taa at-3′) with corresponding oligonucleotide as a positive control (5′-tta gag gcc ctt tcg cag tcc ttt tag tta cat tct tca aca gtg aat tta ccg gga tca gtg ctg-3′).
- The qPCR reactions were performed with a final volume of 10 µL containing 5 µL of SsoAdvanced Universal SYBR Green master mix (Bio-Rad Laboratories, South Granville, NSW, Australia), 2 µL of nuclease free water, 0.5 µL each of 10 µM forward and reverse primers, and 2 µL of 1:5 diluted microfilarial lysates.
- In each qPCR run, water was used as a negative control, and the synthesized oligonucleotide was used as a standard. Each of the diluted lysates was run in duplicate, and the standards in triplicate.
- qPCR assays were run on a CFX Real-Time System (Bio-Rad Laboratories, Hercules, CA, USA), with an initial denaturing step of 3 min at 98 °C followed by 40 cycles of (98 °C 10 s, 54 °C 15 s, 72 °C 15 s, read plate) including melt curve analysis at 65 °C to 95 °C for 5 s with an increment of 0.2 °C for 5 s.
7. Results
7.1. Sample Receipt and Tube Identification and Assignment to Metadata
7.2. qPCR Assessment of DNA Extractions
8. Discussion
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Open Access Statement
Disclaimer
References
- Remme, J.H.F.; Boatin, B.; Boussinesq, M. Helminthic diseases: Onchocerciasis and loiasis. In The International Encyclopedia of Public Health, 2nd ed.; Quah, S.R., Cockerham, W.C., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2017; Volume 3, pp. 576–587. [Google Scholar]
- Basáñez, M.G.; Pion, S.D.; Churcher, T.S.; Breitling, L.P.; Little, M.P.; Boussinesq, M. River blindness: A success story under threat? PLoS Med. 2006, 3, e371. [Google Scholar] [CrossRef] [PubMed]
- Awadzi, K.; Opoku, N.O.; Attah, S.K.; Lazdins-Helds, J.; Kuesel, A.C. A randomized, single-ascending-dose, ivermectin-controlled, double-blind study of moxidectin in Onchocerca volvulus infection. PLoS Negl. Trop. Dis. 2014, 8, e2953. [Google Scholar] [CrossRef]
- Chesnais, C.B.; Nana-Djeunga, H.C.; Njamnshi, A.K.; Lenou-Nanga, C.G.; Boulle, C.; Bissek, A.Z.; Kamgno, J.; Colebunders, R.; Boussinesq, M. The temporal relationship between onchocerciasis and epilepsy: A population-based cohort study. Lancet Infect. Dis. 2018, 18, 1278–1286. [Google Scholar] [CrossRef]
- Fodjo, J.N.S.; Mandro, M.; Mukendi, D.; Tepage, F.; Menon, S.; Nakato, S.; Nyisi, F.; Abhafule, G.; Wonya’rossi, D.; Anyolito, A.; et al. Onchocerciasis-associated epilepsy in the Democratic Republic of Congo: Clinical description and relationship with microfilarial density. PLoS Negl. Trop. Dis. 2019, 13, e0007300. [Google Scholar] [CrossRef]
- Frempong, K.K.; Walker, M.; Cheke, R.A.; Tetevi, E.J.; Gyan, E.T.; Owusu, E.O.; Wilson, M.D.; Boakye, D.A.; Taylor, M.J.; Biritwum, N.K.; et al. Does increasing treatment frequency address suboptimal responses to ivermectin for the control and elimination of River blindness? Clin. Infect. Dis. 2016, 62, 1338–1347. [Google Scholar] [CrossRef]
- Theile, E.A.; Cama, V.A.; Lakwo, T.; Mekasha, S.; Abanyie, F.; Sleshi, M.; Kebede, A.; Cantey, P.T. Detection of Onchocerca volvulus in skin snips by microscopy and real-time polymerase chain reaction: Implications for monitoring and evaluation activities. Am. J. Trop. Med. Hyg. 2016, 94, 906–911. [Google Scholar] [CrossRef]
- Lagatie, O.; Merino, M.; Batsa Debrah, L.; Debrah, A.Y.; Stuyver, L.J. An isothermal DNA amplification method for detection of Onchocerca volvulus infection in skin biopsies. Parasit. Vectors 2016, 9, 624. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for Stopping Mass Drug Administration and Verifying Elimination of Human Onchocerciasis: Criteria and Procedures; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization; African Programme for Onchocerciasis Control. Conceptual and Operational Framework of Onchocerciasis Elimination with Ivermectin Treatment; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization; African Programme for Onchocerciasis Control. Report of the Consultative Meetings on Strategic Options and Alternative Treatment Strategies for Accelerating Onchocerciasis Elimination in Africa; World Health Organization: Geneva, Switzerland, 2015; p. 55. [Google Scholar]
- Sauerbrey, M.; Rakers, L.J.; Richards, F.O. Progress toward elimination of onchocerciasis in the Americas. Int. Health 2018, 10, i71–i78. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Elimination of human onchocerciasis: Progress report, 2021. Wkly. Epidemiol. Rec. 2022, 97, 591–598. [Google Scholar]
- Noma, M.; Zouré, H.G.; Tekle, A.H.; Enyong, P.A.; Nwoke, B.E.; Remme, J.H. The geographic distribution of onchocerciasis in the 20 participating countries of the African Programme for Onchocerciasis Control: (1) priority areas for ivermectin treatment. Parasit. Vectors 2014, 7, 325. [Google Scholar] [CrossRef]
- Zouré, H.G.; Noma, M.; Tekle, A.H.; Amazigo, U.V.; Diggle, P.J.; Giorgi, E.; Remme, J.H. The geographic distribution of onchocerciasis in the 20 participating countries of the African Programme for Onchocerciasis Control: (2) pre-control endemicity levels and estimated number infected. Parasit. Vectors 2014, 7, 326. [Google Scholar] [CrossRef] [PubMed]
- Diawara, L.; Traore, M.O.; Badji, A.; Bissan, Y.; Doumbia, K.; Goita, S.F.; Konate, L.; Mounkoro, K.; Sarr, M.D.; Seck, A.F.; et al. Feasibility of onchocerciasis elimination with ivermectin treatment in endemic foci in Africa: First evidence from studies in Mali and Senegal. PLoS Negl. Trop. Dis. 2009, 3, e497. [Google Scholar] [CrossRef] [PubMed]
- Tekle, A.H.; Zouré, H.G.; Noma, M.; Boussinesq, M.; Coffeng, L.E.; Stolk, W.A.; Remme, J.H. Progress towards onchocerciasis elimination in the participating countries of the African Programme for Onchocerciasis Control: Epidemiological evaluation results. Infect. Dis. Poverty 2016, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Traore, M.O.; Sarr, M.D.; Badji, A.; Bissan, Y.; Diawara, L.; Doumbia, K.; Goita, S.F.; Konate, L.; Mounkoro, K.; Seck, A.F.; et al. Proof-of-principle of onchocerciasis elimination with ivermectin treatment in endemic foci in Africa: Final results of a study in Mali and Senegal. PLoS Negl. Trop. Dis. 2012, 6, e1825. [Google Scholar] [CrossRef] [PubMed]
- Crawford, K.E.; Hedtke, S.M.; Kuesel, A.C.; Doyle, S.D.; Armoo, S.; Osei-Atweneboana, M.; Grant, W.N. Genome-based tools for onchocerciasis elimination: Utility of the mitochondrial genome for delineating Onchocerca volvulus transmission zones. bioRxiv 2019. [Google Scholar] [CrossRef]
- Shrestha, H.; McCulloch, K.; Chisholm, R.H.; Armoo, S.; Vierigh, F.; Sirwani, N.; Crawford, K.E.; Osei-Ateweneboana, M.Y.; Grant, W.N.; Hedtke, S.M. Synthesizing environmental, epidemiological, and genetic data to understand the persistence of onchocerciasis transmission in the ecological transition region of Ghana. medRxiv 2023. [Google Scholar] [CrossRef]
- Choi, Y.J.; Tyagi, R.; McNulty, S.N.; Rosa, B.A.; Ozersky, P.; Martin, J.; Hallsworth-Pepin, K.; Unnasch, T.R.; Norice, C.T.; Nutman, T.B.; et al. Genomic diversity in Onchocerca volvulus and its Wolbachia endosymbiont. Nat. Microbiol. 2016, 2, 16207. [Google Scholar] [CrossRef]
- Hedtke, S.M.; Choi, Y.-J.; Kode, A.; Chalasani, G.C.; Sirwani, N.; Jada, S.R.; Hotterbeekx, A.; Mandro, M.; Siewe Fodjo, J.N.; Amombo, G.N.; et al. Assessing intensity of infection and genetic diversity of onchocerciasis using mitochondrial genome sequencing of single microfilariae. Pathogens 2023, 12, 971. [Google Scholar] [CrossRef]
- Doyle, S.R.; Bourguinat, C.; Nana-Djeunga, H.C.; Kengne-Ouafo, J.A.; Pion, S.D.S.; Bopda, J.; Kamgno, J.; Wanji, S.; Che, H.; Kuesel, A.C.; et al. Genome-wide analysis of ivermectin response by Onchocerca volvulus reveals that genetic drift and soft selective sweeps contribute to loss of drug sensitivity. PLoS Negl. Trop. Dis. 2017, 11, e0005816. [Google Scholar] [CrossRef]
- Hedtke, S.M.; Kuesel, A.C.; Crawford, K.E.; Graves, P.M.; Boussinesq, M.; Lau, C.L.; Boakye, D.A.; Grant, W.N. Genomic epidemiology in filarial nematodes: Transforming the basis for elimination program decisions. Front. Genet. 2020, 10, 1282. [Google Scholar] [CrossRef]
- Arnott, A.; Barry, A.E.; Reeder, J.C. Understanding the population genetics of Plasmodium vivax is essential for malaria control and elimination. Malar. J. 2012, 11, 14. [Google Scholar] [CrossRef]
- Dalmat, R.; Naughton, B.; Kwan-Gett, T.S.; Slyker, J.; Stuckey, E.M. Use cases for genetic epidemiology in malaria elimination. Malar. J. 2019, 18, 163. [Google Scholar] [CrossRef]
- Noviyanti, R.; Miotto, O.; Barry, A.; Marfurt, J.; Siegel, S.; Nguyen, T.-N.; Quang, H.H.; Anggraeni, N.D.; Laihad, F.; Liu, Y.; et al. Implementing parasite genotyping into national surveillance frameworks: Feedback from control programmes and researchers in the Asia-Pacific region. Malar. J. 2020, 19, 271. [Google Scholar] [CrossRef] [PubMed]
- Michalski, M.L.; Griffiths, K.G.; Williams, S.A.; Kaplan, R.M.; Moorhead, A.R. The NIH-NIAID Filariasis Research Reagent Resource Center. PLoS Negl. Trop. Dis. 2011, 5, e1261. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Onchocerciasis: Diagnostic Target Product Profile to Support Preventative Chemotherapy; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Biamonte, M.A.; Cantey, P.T.; Coulibaly, Y.I.; Gass, K.M.; Hamill, L.C.; Hanna, C.; Lammie, P.J.; Kamgno, J.; Nutman, T.B.; Oguttu, D.W.; et al. Onchocerciasis: Target product profiles of in vitro diagnostics to support onchocerciasis elimination mapping and mass drug administration stopping decisions. PLoS Negl. Trop. Dis. 2022, 16, e0010682. [Google Scholar] [CrossRef] [PubMed]
- Shey, R.A.; Ghogomu, S.M.; Shintouo, C.M.; Nkemngo, F.N.; Nebangwa, D.N.; Esoh, K.; Yaah, N.E.; Manka’aFri, M.; Nguve, J.E.; Ngwese, R.A.; et al. Computational design and preliminary serological analysis of a novel multi-epitope vaccine candidate against onchocerciasis and related filarial diseases. Pathogens 2021, 10, 99. [Google Scholar] [CrossRef] [PubMed]
- Lustigman, S.; Makepeace, B.L.; Klei, T.R.; Babayan, S.A.; Hotez, P.; Abraham, D.; Bottazzi, M.E. Onchocerca volvulus: The road from basic biology to a vaccine. Trends Parasitol. 2018, 34, 64–79. [Google Scholar] [CrossRef]
- Zhan, B.; Bottazzi, M.E.; Hotez, P.J.; Lustigman, S. Advancing a human onchocerciasis vaccine from antigen discovery to efficacy studies against natural infection of cattle with Onchocerca ochengi. Front. Cell. Infect. Microbiol. 2022, 12, 869039. [Google Scholar] [CrossRef]
- Abd-Elfarag, G.; Carter, J.Y.; Raimon, S.; Sebit, W.; Suliman, A.; Fodjo, J.N.S.; Olore, P.C.; Biel, K.P.; Ojok, M.; Logora, M.Y.; et al. Persons with onchocerciasis-associated epilepsy and nodding seizures have a more severe form of epilepsy with more cognitive impairment and higher levels of Onchocerca volvulus infection. Epileptic Disord. 2020, 22, 301–308. [Google Scholar] [CrossRef]
- Dusabimana, A.; Tsebeni Wafula, S.; Raimon, S.J.; Fodjo, J.N.S.; Bhwana, D.; Tepage, F.; Abd-Elfarag, G.; Hotterbeekx, A.; Abrams, S.; Colebunders, R. Effect of ivermectin treatment on the frequency of seizures in persons with epilepsy infected with Onchocerca volvulus. Pathogens 2020, 10, 21. [Google Scholar] [CrossRef]
- Dusabimana, A.; Bhwana, D.; Raimon, S.; Mmbando, B.P.; Hotterbeekx, A.; Tepage, F.; Mandro, M.; Siewe Fodjo, J.N.; Abrams, S.; Colebunders, R. Ivermectin treatment response in Onchocerca volvulus infected persons with epilepsy: A three-country short cohort study. Pathogens 2020, 9, 617. [Google Scholar] [CrossRef] [PubMed]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Burns, M.; Valdivia, H. Modelling the limit of detection in real-time quantitative PCR. Eur. Food Res. Technol. 2008, 226, 1513–1524. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008. [Google Scholar]
- Marquina, D.; Buczek, M.; Ronquist, F.; Lukasik, P. The effect of ethanol concentration on the morphological and molecular preservation of insects for biodiversity studies. PeerJ 2021, 9, e10799. [Google Scholar] [CrossRef] [PubMed]
- Carew, M.E.; Metzeling, L.; St Clair, R.; Hoffmann, A.A. Detecting invertebrate species in archived collections using next-generation sequencing. Mol. Ecol. Resour. 2017, 17, 915–930. [Google Scholar] [CrossRef]
- Fobi, G.; Yameogo, L.; Noma, M.; Aholou, Y.; Koroma, J.B.; Zoure, H.M.; Ukety, T.; Lusamba-Dikassa, P.S.; Mwikisa, C.; Boakye, D.A.; et al. Managing the fight against onchocerciasis in Africa: APOC experience. PLoS Negl. Trop. Dis. 2015, 9, e0003542. [Google Scholar] [CrossRef]
- Coffeng, L.E.; Stolk, W.A.; Zoure, H.G.; Veerman, J.L.; Agblewonu, K.B.; Murdoch, M.E.; Noma, M.; Fobi, G.; Richardus, J.H.; Bundy, D.A.; et al. African programme for onchocerciasis control 1995–2015: Updated health impact estimates based on new disability weights. PLoS Negl. Trop. Dis. 2014, 8, e2759. [Google Scholar] [CrossRef]
- Boussinesq, M.; Fobi, G.; Kuesel, A.C. Alternative treatment strategies to accelerate the elimination of onchocerciasis. Int. Health 2018, 10, i40–i48. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hedtke, S.M.; Kode, A.; Ukety, T.O.; Mande, J.L.; Abhafule, G.M.; Raciu, A.A.; Uvon, C.B.; Jada, S.R.; Hotterbeekx, A.; Siewe Fodjo, J.N.; et al. Procedure for Handling and Storage of Onchocerca volvulus Microfilariae Obtained from Skin Snips for Downstream Genetic Work. Trop. Med. Infect. Dis. 2023, 8, 445. https://doi.org/10.3390/tropicalmed8090445
Hedtke SM, Kode A, Ukety TO, Mande JL, Abhafule GM, Raciu AA, Uvon CB, Jada SR, Hotterbeekx A, Siewe Fodjo JN, et al. Procedure for Handling and Storage of Onchocerca volvulus Microfilariae Obtained from Skin Snips for Downstream Genetic Work. Tropical Medicine and Infectious Disease. 2023; 8(9):445. https://doi.org/10.3390/tropicalmed8090445
Chicago/Turabian StyleHedtke, Shannon M., Anusha Kode, Tony O. Ukety, Jöel L. Mande, Germain M. Abhafule, Anuarite A. Raciu, Claude B. Uvon, Stephen R. Jada, An Hotterbeekx, Joseph Nelson Siewe Fodjo, and et al. 2023. "Procedure for Handling and Storage of Onchocerca volvulus Microfilariae Obtained from Skin Snips for Downstream Genetic Work" Tropical Medicine and Infectious Disease 8, no. 9: 445. https://doi.org/10.3390/tropicalmed8090445