
Engaging the Private Health Service Delivery Sector for TB Care in India—Miles to Go!
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Efforts by NTEP for Private Sector Engagement
3.2. Mode of Providing Public Provision of Services to Private Sector
3.3. Other Models of Private Sector Engagement for TB Care Evolved in India
3.4. Outcomes of Private Sector Engagement
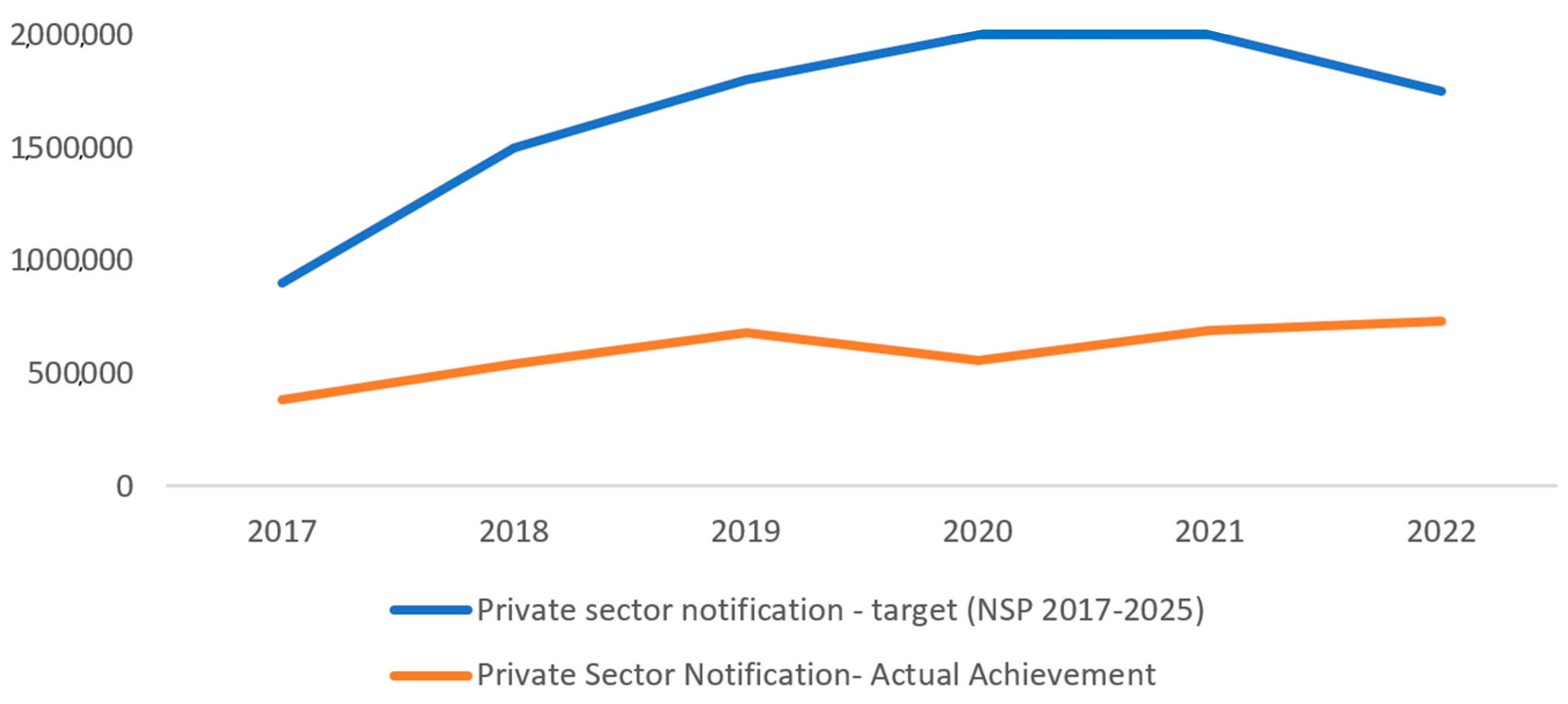
3.5. Achievements in Comparison to the NSP Targets
3.6. Critical Observations
- Notifications and ensuring public health actions for people with TB have not been converted into routine practice in the private sector. Most of the partnership models in the country were incentive-based or service-purchase models that were similar to a client–vendor relationship. Several models that have successfully increased private case notifications were difficult to sustain and expand due to a lesser emphasis on creating sustainable partnerships.
- The number and characteristics of private providers is not clearly understood by the NTEP. The private sector is highly fragmented, ranging from informal health care providers to corporate hospitals. It also consists of providers of variable quality. A uniform strategy for engagement might not be relevant to all parties. In many states of India, informal health care providers outnumber formal health care providers [32,33]. They include village practitioners, drug sellers, untrained allopathic providers, traditional healers, and faith healers. They are the most frequent first port of call for rural residents seeking health care [34,35,36]. Patients approaching an informal health care provider currently experience delays in the diagnosis of TB [37,38,39]. To address the issue of delays in the diagnosis and to find out all the ‘missing cases’, it is essential to engage these informal providers. Similarly, the Ayurveda, Unani, Siddha, Homeopathy (AYUSH) providers and chemists in India are among the first point of care in several part of the country. There are no major strategies by the NTEP to engage with such a diverse set of providers.
- Public sector staff have limited capacity and skills to engage with the private sector [40]. For successful engagement of the private sector, public sector staff require a thorough understanding of the private sector system and require skills for advocacy, marketing, and communication. There is no mechanism to systematically impart such knowledge and skills to NTEP staff.
- There are no formal stakeholder platforms where the ‘for-profit health sector’ is present, limiting the level of dialogue between the NTEP and the private sector for any policy discussions.
- Though there is regulation, its poor implementation is a major challenge. Effective enforcement of this regulation is highly uneven, limited to a few locations. The drug control department finds it difficult to implement the Schedule H1 regulation due to inadequate human resources, and chemists find it difficult to document in their busy schedules [2,41].
- There are around 2000 private medical laboratories accredited by the National Accreditation Board for Testing and Calibration Laboratories (NABL) [42]. However, the efforts to extend TB laboratory services in the private sector are limited. There are 75 NTEP-certified culture and DST labs in the public sector, whereas there are only 17 in the private sector [15].
- The coverage in PM-JAY is currently limited to the indoor management of patients with pleural, pericardial, and neuro-tuberculosis [21].
- There are only a few studies with any in-depth follow-up on the process of the partnership or any longitudinal study of a partnership.
4. Discussion
Suggestions for the Way Forward
- (1)
- Corporate/big hospitals: STEPS, which is envisioned as an equal partnership between the public and private sector for the benefit of society, where private hospitals establish systems to improve the quality of TB care, could be a good model for private hospitals [27]. PPSAs can support the establishing of STEPS in cities where private hospital concentration is higher. The NTEP can also advocate with the Insurance Regulatory and Development Authority of India (IRDAI), other private insurance agencies, and accreditation bodies such as the National Accreditation Board for Hospitals & Healthcare providers (NABH) to ensure that the patients getting treatment in private hospitals are being managed as per the STCI.
- (2)
- Individual medical practitioners: They require access to opportunities for skill up-gradation and support for referrals, provision for access to molecular tests, supply of restricted medicines, support for documentation, patient support, feedback, and social recognition of their work [40,44]. A participatory program where a PPSA offers free access to rapid diagnostics, drugs, support for the notification of patients, and patient support has found to be effective in engaging private practitioners in Chennai [44]. Professional medical associations could play a major role in the capacity building of general practitioners and improving the quality of care through normative forces and peer pressure. Electronic learning courses with flexible schedules and provisions for periodically updating their knowledge through an established communication channel could be attempted. Social marketing of NTEP drugs and diagnostics might be helpful in increasing the uptake of these.
- (3)
- Chemists: India has over 750,000 chemists and pharmacists who could be actively engaged in symptom screening, referral, and surveillance. Experiences from pharmacy engagement across the globe have revealed that establishing a system for simple screening among high-risk clients and a flexible referral mechanism at pharmacies is possible and has the potential to reduce the delay in diagnosis [45]. Chemists ‘associations and the Pharmacy Council of India need to be made stakeholders, and a system to train and update the knowledge of pharmacists needs to be established. Chemists also can play an important role in strengthening Schedule H1, which can help in identifying the right providers for engagement and strengthening surveillance. Schedule H1 has immense potential for identifying the right providers for engagement, strengthening the TB surveillance system, and improving the quality of care in the private sector. The NTEP needs to devise a strategy to strengthen Schedule H1 implementation by advocating with the drug control department and supporting them, establishing systems and tools for strengthening surveillance and collaborating with chemists individually and through their associations. Use of an API (application programming interface), which integrates billing software with Nikshay to generate real-time information of anti-TB drug sales, would have an immense potential to strengthen surveillance [43,46].
- (4)
- AYUSH: Systematic training and sensitization for referral, extending the specimen collection and transportation mechanisms, and treatment support need to be conducted for AYUSH practitioners. Integrated delivery models such as hub-and-spoke models, where an AYUSH practitioner refers a patient for treatment initiation to a modern medicine practitioner/private health facility/government health facility, could be attempted.
- (5)
- Informal health care providers: There is a growing recognition that it is essential to engage informal providers to reach out to all TB patients because of their significant presence in rural areas and also because they care for people in the lower socioeconomic strata who are disproportionately affected by the TB disease. The program needs to engage with the informal health care providers by educating them for symptom screening and referral, extending the specimen collection and transportation mechanisms, and empowering them as treatment supporters. There is limited experience of engaging informal health care providers for TB care [47,48]. Agencies with a deeper understanding of the community and its behavior need to be engaged to map the informal providers and systematically engage them. Enforcing the Schedule H1 regulations might help in reducing the number of unqualified practitioners prescribing anti-TB drugs.
- (6)
- Laboratory: The NTEP needs to proactively improve the access to diagnostics for patients reaching the private sector through certifying more private laboratories for TB tests such as the line probe assay and DST, scaling up various models such as cartridge/chip sharing and reagent rental, or subsidizing rates through the IPAQT mechanism. The strategic purchase of services from private laboratories could improve the utilization and acceptability of DST among the private sector doctors.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Global TB Report 2022. WHO. 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports (accessed on 10 January 2023).
- Government of India. Ministry of Health and Family Welfare (MOHFW). Central TB Division. National Strategic Plan for Tuberculosis Elimination 2017–2025. MOHFW. 2017. Available online: https://tbcindia.gov.in/WriteReadData/NSP%20Draft%2020.02.2017%201.pdf (accessed on 10 January 2023).
- Indian Council of Medical Research. National TB Prevalence Survey 2019–2021. ICMR. 2022. Available online: https://tbcindia.gov.in/showfile.php?lid=3659 (accessed on 10 January 2022).
- Arinaminpathy, N.; Batra, D.; Khaparde, S. The number of privately treated tuberculosis cases in India: An estimation from drug sales data. Lancet Infect. Dis. 2016, 16, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Arinaminpathy, N.; Batra, D.; Maheshwari, N. Tuberculosis treatment in the private healthcare sector in India: An analysis of recent trends and volumes using drug sales data. BMC Infect. Dis. 2019, 19, 539. [Google Scholar] [CrossRef] [PubMed]
- Stallworthy, G.; Dias, H.M.; Pai, M. Quality of tuberculosis care in the private health sector. J. Clin. Tuberc. Other Mycobact. Dis. 2020, 20, 100171. [Google Scholar] [CrossRef]
- Kwan, A.; Daniels, B.; Saria, V.; Satyanarayana, S.; Subbaraman, R.; McDowell, A.; Bergkvist, S.; Das, R.K.; Das, V.; Das, J.; et al. Variations in the quality of tuberculosis care in urban India: A cross-sectional, standardized patient study in two cities. PLoS Med. 2018, 15, e1002653. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Kwan, A.; Daniels, B.; Satyanarayana, S.; Subbaraman, R.; Bergkvist, S.; Das, R.K.; Das, V.; Pai, M. Use of standardised patients to assess quality of tuberculosis care: A pilot, cross-sectional study. Lancet Infect. Dis. 2015, 15, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Satyanarayana, S.; Subbaraman, R.; Shete, P.; Gore, G.; Das, J.; Cattamanchi, A.; Mayer, K.; Menzies, D.; Harries, A.D.; Hopewell, P.; et al. Quality of tuberculosis care in India: A systematic review. Int. J. Tuberc. Lung Dis. 2015, 19, 751–763. [Google Scholar] [CrossRef]
- World Health Organisation. The Private Health Sector: An Operational Definition. Geneva. 2020. Available online: https://www.who.int/docs/default-source/health-system-governance/private-health-sector-an-operational-definition.pdf (accessed on 20 January 2023).
- World Health Organisation. Engaging the Private Health Service Delivery Sector through Governance in Mixed Health Systems: Strategy Report of the WHO Advisory Group on the Governance of the Private Sector for Universal Health Coverage; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/activities/strengthening-private-sector-engagement-for-uhc (accessed on 3 February 2023).
- Government of India. Ministry of Health and Family Welfare. National Health Policy 2017. GoI. 2017. Available online: https://www.nhp.gov.in/nhpfiles/national_health_policy_2017.pdf (accessed on 10 January 2023).
- World Health Organization (WHO) Country Office for India. Standards for TB Care in India. WHO. 2014. Available online: https://apps.who.int/iris/bitstream/handle/10665/208894/stci_book.pdf (accessed on 1 January 2023).
- Government of India. Ministry of Health and Family Welfare. National Tuberculosis Elimination Programme. NIKSHAY. Available online: https://www.nikshay.in/ (accessed on 1 January 2023).
- Ministry of Health and Family Welfare. India TB Report 2022. CTD. Available online: https://tbcindia.gov.in/WriteReadData/IndiaTBReport2022/TBAnnaulReport2022.pdf (accessed on 10 January 2023).
- Government of India. Ministry of Health and Family Welfare. Direct Benet Transfer Manual for National Tuberculosis Elimination Programme. Available online: https://tbcindia.gov.in/WriteReadData/l892s/23294204DBTManualForNTEP.pdf (accessed on 1 January 2023).
- Government of India. Ministry of Health and Family Welfare. Notification of TB Cases. Government of India. 2012. Available online: https://tbcindia.gov.in/WriteReadData/l892s/8249592141TB%20Notification%20Govt%20%20Order%20dated%2007%2005%202012.pdf (accessed on 1 January 2023).
- Government of India. Ministry of Health and Family Welfare. Gazette of India Notification G.S.R. 588(E). 2013. Drugs and Cosmetics (Fourth Amendment) Rules/2013. Available online: https://thehealthmaster.com/wp-content/uploads/2020/10/GSR-No.-588E-Dt-30-08-2013-Schedule-H1-Drugs-DC-fourth-Amendment-Rules-2013.pdf (accessed on 1 January 2023).
- National Pharmaceuticals Pricing Authority. Compendium of Ceiling Prices of Scheduled Drugs as on 10.08.2022. NPPA. Available online: https://www.nppaindia.nic.in/wp-content/uploads/2022/09/Compendium-Prices-2022.pdf (accessed on 10 January 2022).
- Government of India. Ministry of Health & Family Welfare. Guidance Document on Partnerships. 2019. Available online: https://tbcindia.gov.in/WriteReadData/l892s/9531588006Guidance%20Doucument%20on%20Partnerships%20RNTCP%202019.pdf (accessed on 10 January 2022).
- National Health Authority. Ayushman Bharat Pradan Mantri Jan Arogya Yojana. Available online: https://setu.pmjay.gov.in/setu/ (accessed on 10 January 2023).
- Initiative for Promoting Affordable and Quality TB Tests (IPAQT). 2023. Available online: https://healthmarketinnovations.org/program/initiative-promoting-affordable-and-quality-tb-tests-ipaqt (accessed on 10 January 2023).
- Government of India. Ministry of Health & Family Welfare, National Tuberculosis Elimination Programme (NTEP). Universal Access to TB Care (UATBC): Concurrent Assessment Report. NTEP. 2016. Available online: https://tbcindia.gov.in/index1.php?sublinkid=4711&level=3&lid=3265&lang=1 (accessed on 10 January 2023).
- Deo, S.; Jindal, P.; Gupta, D.; Khaparde, S.; Rade, K.; Sachdeva, K.S.; Vadera, B.; Shah, D.; Patel, K.; Dave, P.; et al. What would it cost to scale-up private sector engagement efforts for tuberculosis care? Evidence from three pilot programs in India. PLoS ONE 2019, 14, e0214928. [Google Scholar] [CrossRef]
- Project JEET. Available online: https://www.projectjeet.in/ (accessed on 9 January 2023).
- Balakrishnan, S.; Rakesh, P.S.; Sunilkumar, M.; Sankar, B.; Ramachandran, R.; Ameer, K.A.; Gopi, R.; Nair, P. STEPS: A Solution for Ensuring Standards of TB Care for Patients Reaching Private Hospitals in India. Glob. Health Sci. Pract. 2021, 9, 286–295. [Google Scholar] [CrossRef]
- Rakesh, P.S.; Balakrishnan, S.; Sunilkumar, M.; Alexander, K.G.; Vijayan, S.; Roddawar, V.; Pramod Kumar, P.P.; Kailash, J.; Kunoor, A.; Rajiv, M.; et al. STEPS—A patient centric and low-cost solution to ensure standards of TB care to patients reaching private sector in India. BMC Health Serv. Res. 2022, 22, 2. [Google Scholar] [CrossRef] [PubMed]
- Central TB Division. Management of Patients Seeking Care in Private Sector. National Medical College Task Force on NTEP. 25 November 2022. Kolkota. Available online: https://www.slideshare.net/rivubasu94/management-of-patients-seeking-care-in-private-sector (accessed on 3 February 2023).
- Ministry of Health and Family Welfare. India TB Report 2018–2023. CTD. Available online: https://tbcindia.gov.in/index1.php?lang=1&level=1&sublinkid=4160&lid=2807 (accessed on 10 April 2023).
- Chandra, A.; Kumar, R.; Kant, S.; Parthasarathy, R.; Krishnan, A. Direct and indirect patient costs of tuberculosis care in India. Trop. Med. Int. Health. 2020, 25, 803–812. [Google Scholar] [CrossRef]
- GBD 2019 Universal Health Coverage Collaborators. Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1250–1284. [Google Scholar] [CrossRef]
- Priya, R.; Singh, R.; Das, S. Health Implications of Diverse Visions of Urban Spaces: Bridging the Formal-Informal Divide. Front. Public Health 2019, 7, 239. [Google Scholar] [CrossRef]
- Gautham, M.; Shyamprasad, K.M.; Singh, R.; Zachariah, A.; Singh, R.; Bloom, G. Informal rural healthcare providers in North and South India. Health Policy Plan. 2013, 29, i20–i29. [Google Scholar] [CrossRef]
- Kapoor, S.K.; Raman, A.V.; Sachdeva, K.S.; Satyanarayana, S. How Did the TB Patients Reach DOTS Services in Delhi? A Study of Patient Treatment Seeking Behavior. PLoS ONE 2012, 7, e42458. [Google Scholar] [CrossRef] [PubMed]
- Mistry, N.; Rangan, S.; Dholakia, Y.; Lobo, E.; Shah, S.; Patil, A. Durations and Delays in Care Seeking, Diagnosis and Treatment Initiation in Uncomplicated Pulmonary Tuberculosis Patients in Mumbai, India. PLoS ONE 2016, 11, e0152287. [Google Scholar]
- Mistry, N.; Lobo, E.; Shah, S.; Rangan, S.; Dholakia, Y. Pulmonary tuberculosis in Patna, India: Durations, delays, and health care seeking behaviour among patients identified through household surveys. J. Epidemiol. Glob. Health 2017, 7, 241–248. [Google Scholar] [CrossRef]
- Bronner Murrison, L.; Ananthakrishnan, R.; Swaminathan, A.; Auguesteen, S.; Krishnan, N.; Pai, M.; Dowdy, D.W. How do patients access the private sector in Chennai, India? An evaluation of delays in tuberculosis diagnosis. Int. J. Tuberc. Lung Dis. 2016, 20, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Thapa, P.; Hall, J.J.; Jayasuriya, R.; Mukherjee, P.S.; Beek, K.; Das, D.K.; Mandal, T.; Narasimhan, P. What are the tuberculosis care practices of informal healthcare providers? A cross-sectional study from Eastern India. Health Policy Plan. 2022, 37, 1158–1166. [Google Scholar] [CrossRef]
- Thapa, P.; Jayasuriya, R.; Hall, J.J.; Mukherjee, P.S.; Beek, K.; Briggs, N.; Kr Das, D.; Mandal, T.; Narasimhan, P. Are informal healthcare providers knowledgeable in tuberculosis care? A cross-sectional survey using vignettes in West Bengal, India. Int. Health 2022. [Google Scholar] [CrossRef] [PubMed]
- Nair, S.; Philip, S.; Varma, R.P.; Rakesh, P.S. Barriers for involvement of private doctors in RNTCP—Qualitative study from Kerala. India J. Fam. Med. Prim. Care 2019, 8, 160–165. [Google Scholar]
- World Health Organization (WHO). Engaging Private Health Care Providers in TB Care and Prevention: A Landscape Analysis. WHO. 2021. Available online: https://cdn.who.int/media/docs/default-source/hq-tuberculosis/engaging-private-health-care-providers-in-tb-care-and-prevention-a-landscape-analysis-2020-update.pdf (accessed on 1 October 2021).
- National Accreditation Board for Testing and Calibration Laboratories (NABL). Directory of Accredited Medical Laboratories. NABL India. Available online: https://nabl-india.org/accredited-cab-directory/ (accessed on 10 February 2023).
- Ps, R.; Balakrishnan, S.; Ramachandran, R.; Nandhan, S.; Samuel, N.I.; Pp, P.; Aloysius, S. Using a Pharmacy-Based Surveillance System to Improve Standards for TB Care in Kerala, India. Glob. Health Sci. Pract. 2021, 9, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, R.; Richardson, M.D.; van den Hof, S.; Rangaswamy, R.; Thiagesan, R.; Auguesteen, S.; Kamp, N. Successfully Engaging Private Providers to Improve Diagnosis, Notification, and Treatment of TB and Drug-Resistant TB: The EQUIP Public-Private Model in Chennai, India. Glob. Health Sci. Pract. 2019, 7, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Bigio, J.; Aquilera Vasquez, N.; Huria, L.; Pande, T.; Creswell, J.; Ananthakrishnan, R.; Bimba, J.S.; Cuevas, L.E.; Vo, L.; Bakker, M.I.; et al. Engaging pharmacies in tuberculosis control: Operational lessons from 19 case detection interventions in high-burden countries. BMJ Glob. Health 2022, 7, e008661. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.; Deepak, K.G.; Verma, G.; Chaubey, S.; Kumar, L.; Klinton, J.; Raj, S.; Jha, P.; Vijayan, S. Engaging private pharmacies to help end TB in India. Int. J. Tuberc. Lung Dis. 2022, 26, 457–459. [Google Scholar] [CrossRef]
- Kelamane, S.; Satyanarayana, S.; Nagaraja, S.B.; Panibatla, V.; Dasari, R.; Rajeesham, K.A.; Kamineni, V. Engaging Informal Private Health Care Providers for TB Case Detection: Experiences from RIPEND Project in India. Tuberc. Res. Treat. 2021, 2021, 9579167. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Pattanaik, S.; Choudhury, R.; Nanda, P.; Sahu, S.; Panigrahi, R.; Padhi, B.K.; Sahoo, K.C.; Mishra, P.R.; Panigrahi, P.; et al. Impact of involvement of non-formal health providers on TB case notification among migrant slum-dwelling populations in Odisha, India. PLoS ONE 2018, 13, e0196067. [Google Scholar] [CrossRef]
- Central TB Division. Training Modules (5–9) for Programme Managers & Medical Officers. New Delhi. July 2020. Available online: https://tbcindia.gov.in/WriteReadData/NTEPTrainingModules5to9.pdf (accessed on 3 February 2023).


{kind=link}
| Domains of Engagement | Strategies (Year of Initiation) | Description |
|---|---|---|
| Policy and dialogue | National Health Policy (NHP) 2017 | NHP mentions about enabling the private sector contribution to make the health care systems more effective, efficient, rational, safe, affordable, and ethical [12]. |
| National Strategic Plan (NSP) for TB elimination from 2017 to 2025 | NSP highlights the need for private sector engagement as an important component to eliminate TB [2]. | |
| Standards of TB Care in India (STCI) | STCI mentions 26 standards that every citizen should receive irrespective of the sector of treatment [13]. | |
| Information Exchange | Ni-kshay (2012) | Ni-kshay is the real-time case-based web-based management information system of NTEP [14]. Private providers can directly log in to the system using their user credentials and notify TB and report outcomes. In total, 172,068 private hospitals were registered in Ni-kshay, out of which 36,346 notified at least one patient in 2021 [15]. |
| Incentive for TB notification and outcome reporting (2019) | NTEP provides INR 500 as an incentive to the private provider to notify each TB patient and another INR 500 to report the treatment outcome [16]. | |
| Ni-kshay Sampark (2018) | Ni-kshay sampark is the national call center, which supports the private sector with notification and treatment adherence support. The program currently runs a 100-seat call center and supports 14 languages [15]. | |
| Regulatory Measures | Mandatory TB notification (2012) | The Government of India has issued directives making TB notification mandatory and promulgated another directive penalizing failure to notify [17]. |
| Enforcement of Schedule H1 regulation (2014) | Anti-TB medicines are included in Schedule H1 and can only be sold on prescription from a registered medical practitioner, and details of the prescriber, the patient, and the drug sold need to be maintained by the chemists [18]. This is intended to prevent the indiscriminate use of the drug. | |
| Price ceiling of anti-TB drugs | The National Pharmaceutical Pricing Authority (NPPA) has imposed a ceiling price for anti-TB drugs to be sold in the market [19]. | |
| Public Provision of Services | Free drugs and diagnostics (2017) | The NTEP has provisions for supplying free, quality-assured anti-TB drugs and free tests such as molecular tests and drug susceptibility tests to the patients reaching the private sector [2]. |
| Nikshay Poshan Yojana (2018) | The NTEP provides INR 500 per month to all TB patients, irrespective of sector, during the treatment period as a direct benefit transfer [15]. | |
| Support in contact investigations, treatment adherence, and preventive therapy (2017) | Directly and through various agencies, the NTEP provides support for contact investigations and treatment adherence to all patients reaching private sector [2]. | |
| Training and capacity building | Directly and through various agencies, the NTEP provides training and capacity building for the health workforce in the private sector. | |
| Financing | National Partnership Guidelines (2019) | In 2001, the first guidelines on partnerships on engagement of non-governmental organizations (NGO) and private providers (revisions in 2008, 2014, and 2019) [20]. To increase the capacity of states for strategic purchase of services, multi-disciplinary technical support units have been formed in nine high priority States. |
| Pradhan Mantri Jan Arogya Yojana (PM-JAY) | PM-JAY is a health insurance scheme that provides cashless cover of INR 500,000 per annum (USD 6700) to the eligible disadvantaged households for inpatient treatment at empaneled private hospitals for listed conditions which include management of patients with pleural, pericardial, and neuro-tuberculosis [21]. | |
| Subsidy | The Initiative for Promoting Affordable and Quality Tests (IPAQT) in India provides over 130 accredited laboratories with concessionary pricing in exchange for their case notification to the NTP and passing on the price reductions to patients for WHO-endorsed TB tests [22]. |
| 2017 | 2018 | 2019 | 2020 | 2021 | |
|---|---|---|---|---|---|
| TB Notification from the private sector | 383,784 | 542,390 | 678,895 | 556,582 | 689,129 |
| Proportion of TB notification from private out of the total notification | 21% | 25% | 28% | 31% | 32% |
| Proportion of TB patients notified from private who knew their HIV status | NA | NA | 55% | 85% | 92% |
| Proportion of notified TB patients from private offered universal drug susceptibility testing | NA | 6% | 28% | 48% | 39.4% |
| Treatment success rate of TB patients in the private sector | 38% | 35% | 71% | 79% | 82% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suseela, R.P.; Shannawaz, M. Engaging the Private Health Service Delivery Sector for TB Care in India—Miles to Go! Trop. Med. Infect. Dis. 2023, 8, 265. https://doi.org/10.3390/tropicalmed8050265
Suseela RP, Shannawaz M. Engaging the Private Health Service Delivery Sector for TB Care in India—Miles to Go! Tropical Medicine and Infectious Disease. 2023; 8(5):265. https://doi.org/10.3390/tropicalmed8050265
Chicago/Turabian StyleSuseela, Rakesh P., and Mohd Shannawaz. 2023. "Engaging the Private Health Service Delivery Sector for TB Care in India—Miles to Go!" Tropical Medicine and Infectious Disease 8, no. 5: 265. https://doi.org/10.3390/tropicalmed8050265