
Coinfection with Strongyloides and SARS-CoV-2: A Systematic Review
 , , , ,
, , , ,
Abstract
:1. Introduction
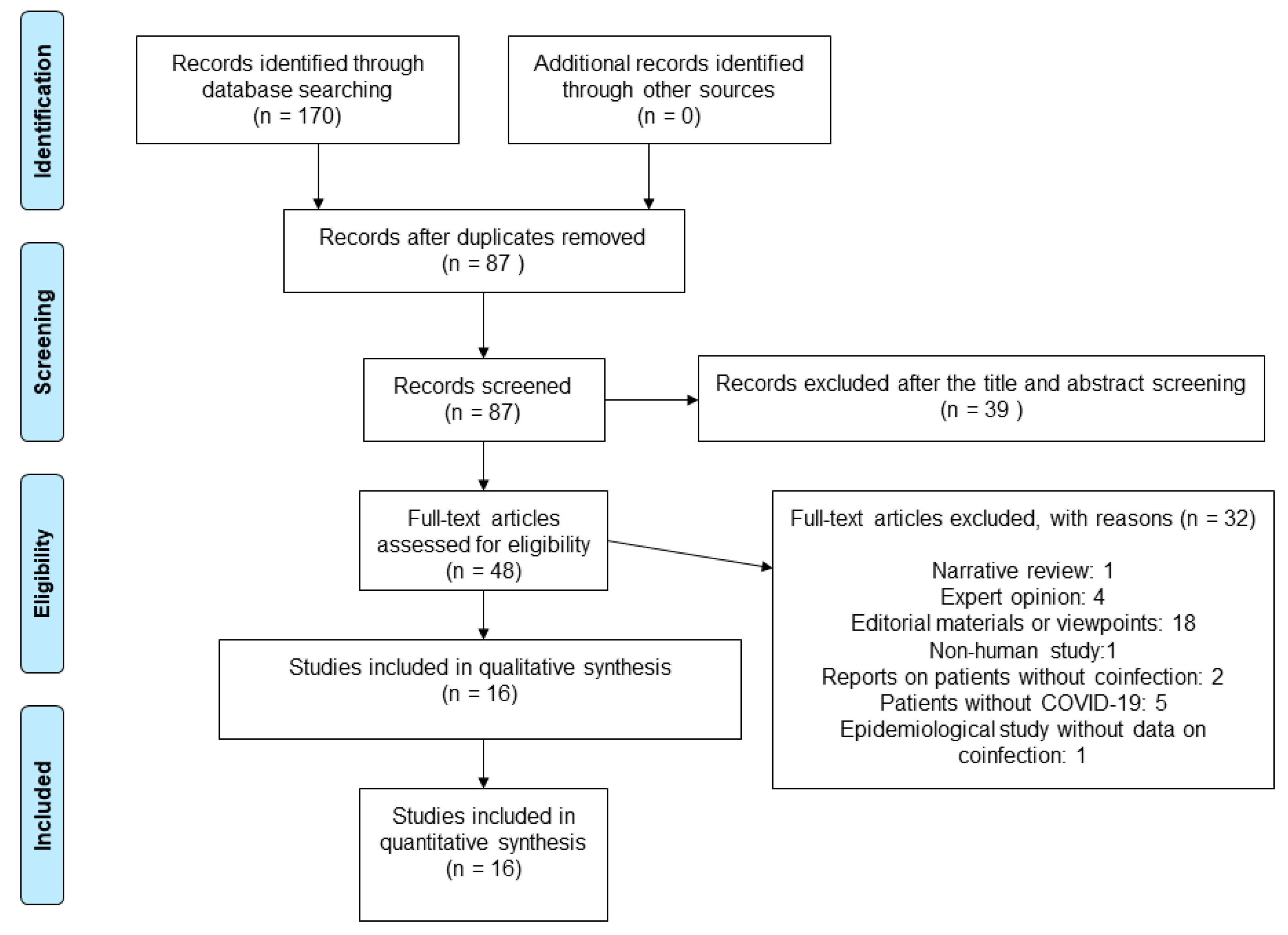
2. Materials and Methods
3. Results
3.1. Hyperinfection Syndrome (HS) and Disseminated Strongyloidiasis (DS)
3.2. Cutaneous Reactivation of Strongyloidiasis
3.3. Gastrointestinal Manifestations of Strongyloidiasis
3.4. Isolated Eosinophilia
3.5. Asymptomatic Strongyloidiasis
3.6. Laboratory Investigations
3.7. Time Interval between SARS-CoV-2 Infection and Strongyloides Manifestations
3.8. Strongyloidiasis Treatment and Outcomes
3.9. Case Causality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McKenna, M.L.; McAtee, S.; Bryan, P.E.; Jeun, R.; Ward, T.; Kraus, J.; Bottazzi, M.E.; Hotez, P.J.; Flowers, C.C.; Mejia, R. Human Intestinal Parasite Burden and Poor Sanitation in Rural Alabama. Am. J. Trop. Med. Hyg. 2017, 97, 1623–1628. [Google Scholar] [CrossRef]
- Buonfrate, D.; Bisanzio, D.; Giorli, G.; Odermatt, P.; Fürst, T.; Greenaway, C.; French, M.; Reithinger, R.; Gobbi, F.; Montresor, A.; et al. The Global Prevalence of Strongyloides stercoralis Infection. Pathogens 2020, 9, 468. [Google Scholar] [CrossRef] [PubMed]
- Olsen, A.; van Lieshout, L.; Marti, H.; Polderman, T.; Polman, K.; Steinmann, P.; Stothard, R.; Thybo, S.; Verweij, J.J.; Magnussen, P. Strongyloidiasis--the most neglected of the neglected tropical diseases? Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Muñoz, J.; Gobbi, F.; Van Den Ende, J.; Bisoffi, Z. Severe strongyloidiasis: A systematic review of case reports. BMC Infect Dis. 2013, 13, 78. [Google Scholar] [CrossRef]
- Corti, M. Strongyloides stercoralis in Immunosuppressed Patients. Arch. Clin. Infect. Dis. 2016, 11, e27510. [Google Scholar] [CrossRef]
- Luvira, V.; Siripoon, T.; Phiboonbanakit, D.; Somsri, K.; Watthanakulpanich, D.; Dekumyoy, P. Strongyloides stercoralis: A Neglected but Fatal Parasite. Trop. Med. Infect Dis. 2022, 7, 310. [Google Scholar] [CrossRef]
- Keiser, P.B.; Nutman, T.B. Strongyloides stercoralis in the Immunocompromised Population. Clin. Microbiol. Rev. 2004, 17, 208–217. [Google Scholar] [CrossRef]
- Czeresnia, J.M.; Weiss, L.M. Strongyloides stercoralis. Lung 2022, 200, 141–148. [Google Scholar] [CrossRef]
- Ghosh, K.; Ghosh, K. Strongyloides stercoralis septicaemia following steroid therapy for eosinophilia: Report of three cases. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 1163–1165. [Google Scholar] [CrossRef]
- Fardet, L.; Généreau, T.; Poirot, J.-L.; Guidet, B.; Kettaneh, A.; Cabane, J. Severe strongyloidiasis in corticosteroid-treated patients: Case series and literature review. J. Infect. 2007, 54, 18–27. [Google Scholar] [CrossRef]
- Wurtz, R.; Mirot, M.; Fronda, G.; Peters, C.; Kocka, F. Short report: Gastric infection by Strongyloides stercoralis. Am. J. Trop. Med. Hyg. 1994, 51, 339–340. [Google Scholar] [CrossRef]
- Mokhlesi, B.; Shulzhenko, O.; Garimella, P.S.; Kuma, L.; Monti, C. Pulmonary Strongyloidiasis: The Varied Clinical Presentations. Clin. Pulm. Med. 2004, 11, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Mejia, R.; Nutman, T.B. Screening, prevention, and treatment for hyperinfection syndrome and disseminated infections caused by Strongyloides stercoralis. Curr. Opin. Infect Dis. 2012, 25, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Meamar, A.R.; Rezaian, M.; Mohraz, M.; Hadighi, R.; Kia, E.B. Strongyloides stercoralis hyper-infection syndrome in HIV+/AIDS patients in Iran. Parasitol. Res. 2007, 101, 663–665. [Google Scholar] [CrossRef]
- Chordia, P.; Christopher, S.; Abraham, O.C.; Muliyil, J.; Kang, G.; Ajjampur, S. Risk factors for acquiring Strongyloides stercoralis infection among patients attending a tertiary hospital in south India. Indian J. Med. Microbiol. 2011, 29, 147–151. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 8 September 2022).
- Covid, O.; Table, S.A. Ivermectin treatment for Strongyloides infection in patients with COVID-19. Can. Commun. Dis. Rep. 2021, 47, 316–321. [Google Scholar] [CrossRef] [PubMed]
- De Wilton, A.; Nabarro, L.E.; Godbole, G.S.; Chiodini, P.L.; Boyd, A.; Woods, K. Risk of Strongyloides Hyperinfection Syndrome when prescribing dexamethasone in severe COVID-19. Travel Med. Infect Dis. 2021, 40, 101981. [Google Scholar] [CrossRef]
- Shirley, D.A.; Moonah, S. COVID-19 and Corticosteroids: Unfamiliar but Potentially Fatal Infections That Can Arise following Short-Course Steroid Treatment. Am. J. Trop. Med. Hyg. 2021, 104, 790–793. [Google Scholar] [CrossRef]
- Olivera, M.J. Dexamethasone and COVID-19: Strategies in Low- and Middle-Income Countries to Tackle Steroid-Related Strongyloides Hyperinfection. Am. J. Trop. Med. Hyg. 2021, 104, 1611–1612. [Google Scholar] [CrossRef]
- Boggild, A.K.; Libman, M.; Greenaway, C.; McCarthy, A.E. CATMAT statement on disseminated strongyloidiasis: Prevention, assessment and management guidelines. Can. Commun. Dis. Rep. 2016, 42, 12–19. [Google Scholar] [CrossRef]
- Stauffer, W.M.; Alpern, J.D.; Walker, P.F. COVID-19 and Dexamethasone: A Potential Strategy to Avoid Steroid-Related Strongyloides Hyperinfection. JAMA 2020, 324, 623–624. [Google Scholar] [CrossRef] [PubMed]
- Rosca, E.C.; Heneghan, C.; Spencer, E.A.; Pluddemann, A.; Maltoni, S.; Gandini, S.; Onakpoya, I.; Evans, D.; Conly, J.M.; Jefferson, T. Coinfection with Strongyloides and SARS-CoV-2: Protocol for a systematic review. medRxiv 2023. [Google Scholar] [CrossRef]
- WHO. The Use of the WHO-UMC System for Standardised Case Causality Assessment. Available online: https://www.who.int/publications/m/item/WHO-causality-assessment (accessed on 9 September 2022).
- Alian, S.; Ahangarkani, F.; Boskabadi, S.J.; Kargar-Soleimanabad, S.; Delavarian, L.; Pakzad, A. Mucormycosis, one month after recovery from COVID-19: A case report. Ann. Med. Surg. 2022, 78, 103911. [Google Scholar] [CrossRef] [PubMed]
- Babazadeh, S.; Shokri-Shirvani, J.; Ranaee, M. Strongyloides Hyperinfection Syndrome Following Corticosteroid Therapy in a Patient with COVID-19 infection: A Case Report. Iran. J. Med. Microbiol. 2022, 16, 267–270. [Google Scholar] [CrossRef]
- Feria, L.; Torrado, M.; Anton-Vazquez, V. Reactivation of Strongyloides stercoralis in patients with SARS-CoV-2 pneumonia receiving dexamethasone. Med. Clin. 2022, 158, 242–243. [Google Scholar] [CrossRef] [PubMed]
- Gautam, D.; Gupta, A.; Meher, A.; Siddiqui, F.; Singhai, A. Corticosteroids in Covid-19 pandemic have the potential to unearth hidden burden of strongyloidiasis. IDCases 2021, 25, e01192. [Google Scholar] [CrossRef]
- Kim, J.M.; Sivasubramanian, G. Strongyloides Hyperinfection Syndrome among COVID-19 Patients Treated with Corticosteroids. Emerg. Infect Dis. 2022, 28, 1531–1533. [Google Scholar] [CrossRef]
- Lier, A.J.; Davis, M.W.; Topal, J.E. Antimicrobial Management of Disseminated Strongyloidiasis in a COVID-19 Patient. Am. J. Trop. Med. Hyg. 2020, 103, 2150. [Google Scholar] [CrossRef]
- Lorenzo, H.; Carbonell, C.; Vicente Santiago, M.B.; López-Bernus, A.; Pendones Ulerio, J.; Muñoz Bellido, J.L.; Muro, A.; Belhassen-García, M. Influence of the drugs used in migrant patients with severe acute respiratory syndrome coronavirus 2 and the development of symptomatic strongyloidiasis. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 440–445. [Google Scholar] [CrossRef]
- Marchese, V.; Crosato, V.; Gulletta, M.; Castelnuovo, F.; Cristini, G.; Matteelli, A.; Castelli, F. Strongyloides infection manifested during immunosuppressive therapy for SARS-CoV-2 pneumonia. Infection 2021, 49, 539–542. [Google Scholar] [CrossRef]
- Babazadeh, S.; Shokri-Shirvani, J.; Ranaee, M. Strongyloides stercoralis prophylaxis with ivermectin in COVID-19 patients. Eur. J. Hosp. Pharmacy. Sci. Pract. 2021, 28, A115–A116. [Google Scholar] [CrossRef]
- Nakandakari Gomez, M.D.; Marín Macedo, H.; Seminario Vilca, R. IgA (Henoch Schönlein Purpura) Vasculitis In A Pediatric Patient With COVID-19 And Strongyloidiasis. Rev. Fac. Med. Hum. 2021, 21, 199–205. [Google Scholar] [CrossRef]
- Núñez-Gómez, L.; Comeche, B.; Subirats, M. Strongyloidiasis: An Important Coinfection in the COVID-19 Era. Am. J. Trop. Med. Hyg. 2021, 105, 1134–1135. [Google Scholar] [CrossRef]
- O’Dowling, A.; Gillis, A. Strongyloides Hyperinfection Syndrome in a Patient with Asymptomatic COVID-19 Infection. Ir. Med. J. 2022, 115, 591. [Google Scholar] [PubMed]
- Patel, A.; Bender, W.; Gonzalez, E.; Williamson, M. A case of disseminated strongyloidiasis during treatment for COVID-19. Chest 2021, 160, A278. [Google Scholar] [CrossRef]
- Pintos-Pascual, I.; López-Dosil, M.; Castillo-Núñez, C.; Múñez-Rubio, E. Eosinophilia and abdominal pain after severe pneumonia due to COVID 19. Enferm. Infecc. Microbiol. Clin. 2021, 39, 478–480. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Singh, U.S. Coinfection with Strongyloides and Ascaris in a COVID-19-positive male presenting with acute abdomen: A case report. Future Microbiol. 2022, 17, 1099–1105. [Google Scholar] [CrossRef]
- Stylemans, D.; Van Cauwelaert, S.; D’Haenens, A.; Slabbynck, H. COVID-19-Associated Eosinopenia in a Patient With Chronic Eosinophilia Due to Chronic Strongyloidiasis. Infect Dis. Clin. Pract. (Baltim Md) 2021, 29, e305–e306. [Google Scholar] [CrossRef]
- Nucci, M.; Portugal, R.; Pulcheri, W.; Spector, N.; Ferreira, S.B.; de Castro, M.B.; Noe, R.; de Oliveira, H.P. Strongyloidiasis in patients with hematologic malignancies. Clin. Infect Dis. 1995, 21, 675–677. [Google Scholar] [CrossRef]
- Brigandi, R.A.; Rotman, H.L.; Leon, O.; Nolan, T.J.; Schad, G.A.; Abraham, D. Strongyloides stercoralis host-adapted third-stage larvae are the target of eosinophil-associated immune-mediated killing in mice. J. Parasitol. 1998, 84, 440–445. [Google Scholar] [CrossRef]
- Genta, R.M. Dysregulation of strongyloidiasis: A new hypothesis. Clin. Microbiol. Rev. 1992, 5, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Corti, M.; Villafañe, M.F.; Trione, N.; Risso, D.; Abuín, J.C.; Palmieri, O. [Infection due to Strongyloides stercoralis: Epidemiological, clinical, diagnosis findings and outcome in 30 patients]. Rev. Chil. Infectol. 2011, 28, 217–222. [Google Scholar] [CrossRef]
- Tanaka, M.; Hirabayashi, Y.; Gatanaga, H.; Aizawa, S.; Hachiya, A.; Takahashi, Y.; Tashiro, E.; Kohsaka, T.; Oyamada, M.; Ida, S.; et al. Reduction in interleukin-2-producing cells but not Th1 to Th2 shift in moderate and advanced stages of human immunodeficiency virus type-1-infection: Direct analysis of intracellular cytokine concentrations in CD4+ CD8− T cells. Scand. J. Immunol. 1999, 50, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Montes, M.; Sanchez, C.; Verdonck, K.; Lake, J.E.; Gonzalez, E.; Lopez, G.; Terashima, A.; Nolan, T.; Lewis, D.E.; Gotuzzo, E.; et al. Regulatory T cell expansion in HTLV-1 and strongyloidiasis co-infection is associated with reduced IL-5 responses to Strongyloides stercoralis antigen. PLoS Negl. Trop. Dis. 2009, 3, e456. [Google Scholar] [CrossRef]
- Porto, A.F.; Neva, F.A.; Bittencourt, H.; Lisboa, W.; Thompson, R.; Alcântara, L.; Carvalho, E.M. HTLV-1 decreases Th2 type of immune response in patients with strongyloidiasis. Parasite Immunol. 2001, 23, 503–507. [Google Scholar] [CrossRef]
- Grove, D.I. Human strongyloidiasis. Adv. Parasitol. 1996, 38, 251–309. [Google Scholar] [CrossRef]
- Xie, G.; Ding, F.; Han, L.; Yin, D.; Lu, H.; Zhang, M. The role of peripheral blood eosinophil counts in COVID-19 patients. Allergy 2021, 76, 471–482. [Google Scholar] [CrossRef]
- Cortés-Vieyra, R.; Gutiérrez-Castellanos, S.; Álvarez-Aguilar, C.; Baizabal-Aguirre, V.M.; Nuñez-Anita, R.E.; Rocha-López, A.G.; Gómez-García, A. Behavior of Eosinophil Counts in Recovered and Deceased COVID-19 Patients over the Course of the Disease. Viruses 2021, 13, 1675. [Google Scholar] [CrossRef]
- Padigel, U.M.; Hess, J.A.; Lee, J.J.; Lok, J.B.; Nolan, T.J.; Schad, G.A.; Abraham, D. Eosinophils act as antigen-presenting cells to induce immunity to Strongyloides stercoralis in mice. J. Infect Dis. 2007, 196, 1844–1851. [Google Scholar] [CrossRef]
- Galioto, A.M.; Hess, J.A.; Nolan, T.J.; Schad, G.A.; Lee, J.J.; Abraham, D. Role of eosinophils and neutrophils in innate and adaptive protective immunity to larval strongyloides stercoralis in mice. Infect Immun. 2006, 74, 5730–5738. [Google Scholar] [CrossRef]
- Geri, G.; Rabbat, A.; Mayaux, J.; Zafrani, L.; Chalumeau-Lemoine, L.; Guidet, B.; Azoulay, E.; Pène, F. Strongyloides stercoralis hyperinfection syndrome: A case series and a review of the literature. Infection 2015, 43, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Adedayo, O.; Grell, G.; Bellot, P. Hyperinfective strongyloidiasis in the medical ward: Review of 27 cases in 5 years. South Med. J. 2002, 95, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Litachevsky, V.; Peretz, S.; Schwartz, I. [Clinical-pathologic conference (cpc)—Pulmonary insufficiency in Myasthenia Gravis patient]. Harefuah 2013, 152, 344–347, 368. [Google Scholar] [PubMed]
- Ribeiro, L.C.; Rodrigues Junior, E.N.; Silva, M.D.; Takiuchi, A.; Fontes, C.J. [Purpura in patient with disseminated strongiloidiasis]. Rev. Soc. Bras. Med. Trop. 2005, 38, 255–257. [Google Scholar] [CrossRef]
- Requena-Méndez, A.; Buonfrate, D.; Gomez-Junyent, J.; Zammarchi, L.; Bisoffi, Z.; Muñoz, J. Evidence-Based Guidelines for Screening and Management of Strongyloidiasis in Non-Endemic Countries. Am. J. Trop. Med. Hyg. 2017, 97, 645–652. [Google Scholar] [CrossRef]
- Brotherton, H.; Usuf, E.; Nadjm, B.; Forrest, K.; Bojang, K.; Samateh, A.L.; Bittaye, M.; Roberts, C.A.; d’Alessandro, U.; Roca, A. Dexamethasone for COVID-19: Data needed from randomised clinical trials in Africa. Lancet Glob. Health 2020, 8, e1125–e1126. [Google Scholar] [CrossRef]
- Rodríguez-Guardado, A.; Álvarez-Martínez, M.J.; Flores, M.D.; Sulleiro, E.; Torrús-Tendero, D.; Velasco, M.; Membrillo, F.J. Screening for strongyloidiasis in Spain in the context of the SARS-CoV-2 pandemic: Results of a survey on diagnosis and treatment. Enferm. Infecc. Microbiol. Clin. 2022. [Google Scholar] [CrossRef]


{kind=link}
| Study | Age | Gender | Underlying Diseases | Strongyloides Infection Manifestation | Strongyloides Infection Diagnosis | COVID-19 Diagnosis | Laboratory Findings | COVID-19 Treatment | Strongyloides Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Alian 2022 [25] | 73 | Female | Chronic kidney disease, diabetes mellitus, hypertension, dyslipidemia. | Mucormycosis. No strongyloidiasis manifestations. | Stool analysis | N/R | Lymphocytes decreased | Dexamethasone (8 mg daily) Remdesevir. | N/R | Death |
| Babazadeh 2022 [26] | 70 | Male | Mitral valve replacement, atrial fibrillation, heart failure. | HS | Histopathologic examination (gastric and duodenal mucosae) | N/R | Lymphocytes normal Eosinophils increased | Dexamethasone (6 mg/day iv, 10 days). | Ivermectin (200 μg/kg for 7 days) Albendazole (400 mg every 12 h for 10 days) | Remission of symptoms |
| Feria 2022, case 1 [27] | 44 | Male | Smoking, hypertension, obesity. | Cutaneous reactivation | Serology for S. stercoralis IgG (ELISA) | N/R | Eosinophils normal | Dexamethasone (6 mg/day, 7 days). | Ivermectin (200 mcg/kg/day for 2 days) | Resolution of the skin condition |
| Feria 2022, case 2 [27] | 74 | Female | Pyrazolone allergy, hypertension, dyslipidemia, chronic kidney disease, disseminated tuberculosis correctly treated. | Cutaneous reactivation | Serology for S. stercoralis IgG (ELISA) | N/R | Lymphocytes normal Eosinophils decreased | Dexamethasone (6 mg/day, 10 days). | Ivermectin (200 mcg/kg/day for 2 days) | Resolution of the skin condition |
| Gautam 2021 [28] | 53 | Male | N/R | HS | Stool microscopic examination Koga agar plate | N/R | Eosinophils normal | Methylprednisolone (60 mg iv, twice a day for 5 days). | Ivermectin Albendazole | Recovery |
| Kim 2022 [29] | 63 | Male | Diabetes mellitus, alcohol use disorder. | HS | Microscopic examination of the bronchoalveolar lavage fluid Serology for S. stercoralis IgG Stool microscopic examination | RT-PCR | Lymphocytes decreased Eosinophiles decreased | Dexamethasone (6 mg/d for 10 days); Baricitinib (10 mg/day, for 5 days) Remdesivir (100 mg/day, for 5 days). | Oral ivermectin (200 μg/kg for 14 days) | Death |
| Lier 2020 [30] | 68 | Male | Hypertension, diabetes mellitus complicated by peripheral neuropathy. | DS | Sputum culture Gram and iodine stains Strongyloides serum antibody Stool analysis | RT-PCR | Lymphocytes normal Eosinophils decreased | Methylprednisolone (40 mg iv every 8 h, 3 courses) Tocilizumab (once, iv at 8 mg/kg) Hydroxychloroquine (400 mg oral twice daily loading dose, then 200 mg oral twice daily for 5 days). | Ivermectin (200 μg/kg daily). Albendazole (400 mg orally every 12 h, a 2-week course | Improvement. Transferred to a skilled nursing facility |
| Lorenzo 2022, Patient 1 [31] | 37 | Female | Obesity, diabetes mellitus, dyslipidemia, previous strongyloidiasis (digestive symptoms, no cutaneous manifestations). | None | Serology for S. stercoralis IgG (ELISA) | RT-PCR | Eosinophils normal | Dexamethasone (6 mg once daily for 10 days). | N/R | Recovery |
| Lorenzo 2022, Patient 2 [31] | 47 | Female | Chagas disease, previous strongyloidiasis (digestive symptoms, asthma, no cutaneous manifestations). | None | Serology for S. stercoralis IgG (ELISA) | RT-PCR | Eosinophils normal | Dexamethasone (6 mg once daily, for 10 days) Remdesivir. | N/R | Recovery |
| Lorenzo 2022, Patient 3 [31] | 33 | Female | Previous strongyloidiasis (digestive symptoms, asthma, no cutaneous manifestations). | Eosinophilia | Serology for S. stercoralis IgG (ELISA) | RT-PCR | Eosinophils increased | Dexamethasone (6 mg once daily, for 10 days) Remdesivir. | N/R | Recovery |
| Lorenzo 2022, Patient 4 [31] | 38 | Male | Previous strongyloidiasis (asthma, no cutaneous manifestations). | None | Serology for S. stercoralis IgG (ELISA) | RT-PCR | Eosinophils normal | Azithromycin Hydroxychloroquine Lopinavir/ritonavir. | N/R | Recovery |
| Lorenzo 2022, Patient 5 [31] | 22 | Male | Crohn disease, previous strongyloidiasis (digestive symptoms, no cutaneous manifestations). | None | Serology for S. stercoralis IgG (ELISA) | RT-PCR | Eosinophils normal | Azithromycin Hydroxychloroquine Lopinavir/ritonavir. | N/R | Recovery |
| Lorenzo 2022, Patient 6 [31] | 69 | Female | Trigeminal neuralgia. | None | Serology for S. stercoralis IgG (ELISA) | RT-PCR | Eosinophils normal | Azithromycin Hydroxychloroquine Lopinavir/ritonavir. | N/R | Recovery |
| Lorenzo 2022, Patient 7 [31] | 27 | Female | Vitiligo, previous strongyloidiasis (digestive symptoms, no cutaneous manifestations). | None | Serology for S. stercoralis IgG (ELISA) | RT-PCR | Eosinophils normal | None. | N/R | Recovery |
| Marchese 2021 [32] | 59 | Female | Still’s disease, hypertension, repeated episodes of diffuse itching in the last 10 years, treated with topical steroids with partial improvement. | Digestive symptoms. | Stool examination IFAT serology | RT-PCR | Eosinophils increased | Hydroxychloroquine Lopinavir/ritonavir Dexamethasone (20 mg/day for 5 days, followed by 10 mg/day for other 6 days) Tocilizumab 8 mg/kg, 2 doses, 12 h apart. | Ivermectin (200 mcg/kg, oral, 4 days) | Improvement |
| Martinez 2021, 3/35 (9%) cases [33] | Average: 42.84 ± 11.38 years (among 35 patients) | 52% of women (among 35 patients) | N/R | None | Serology for S. stercoralis | N/R | Eosinophils normal | Among 35 cases: 83% dexamethasone 6 mg/24 h, 14% methylprednisolone bolus 250 mg, 12% tocilizumab 400 mg, and 3% no immunosuppressive treatment. | Prophylactic: ivermectin 6 mg/8 h for 2 days. | No Strongyloides infection manifestations |
| Nakandakaria 2021 [34] | 4 | Female | The parents were tested positive and treated for COVID-19 a month earlier. | None | Stool examination | COVID-19 Rapid Test (IgM, IgG) | Eosinophils increased | N/R | Ivermectin (1 drop/kg/day for 2 days) Metronidazole (40 mg/kg/day every 8 h). | Recovery |
| Nunez-Gomez 2021 [35] | 45 | Male | Several episodes of suspected allergic reactions with rash and angioedema. The last episode occurred in 2018, and the trigger remained undetermined. | Cutaneous reactivation | Serology for S. stercoralis Stool Mueller-Hinton agar plate culture | N/R | N/R | Dexamethasone (6 mg/day, for 12 days) | Ivermectin (200 mg/kg, for 14 days). | Improvement |
| O’Dowling 2022 [36] | 60 | Female | No significant past medical history. | HS | Serology for S. stercoralis Pathological analysis of the small bowel specimen | N/R | N/R | None | Ivermectin (2 doses). | Improvement |
| Patel 2021 [37] | 72 | Male | N/R | DS | Stool microscopic examination Bronchoalveolar lavage Gram-stain | RT-PCR | Eosinophils increased | Dexamethasone | Ivermectin. | Improvement |
| Pintos-Pascual 2021 [38] | 70 | Male | Hypertension | Digestive reactivation | Fresh stool analysis Serological test | RT-PCR | Lymphocytes decreased Eosinophils normal | Methylprednisolone (250 mg boluses, for 5 days, followed by dose tapering, ending treatment at one month) Tocilizumab (day 6 to day 13). Anakinra (on days 10–13 and 19–24). | Albendazole (400 mg/12 h for 3 days) Ivermectin. | Resolution of symptoms |
| Singh 2021 [39] | 58 | Male | Diabetes, rheumatoid arthritis. | Unclear. Ascariasis—S. stercoralis coinfection | Stool microscopic examination | RT-PCR | Lymphocytes decreased Eosinophils increased | Methylprednisolone Aztreonam Hydroxychloroquine Favipiravir/remedesvir Azithromycin | Ivermectin (200 μg/kg/day, 2 weeks) Albendazole (400 mg every 12 h, 2 weeks)—for Ascariasis coinfection. | Improvement |
| Stylemans 2021 [40] | 59 | Male | Diabetes, smoking, chronic eosinophilia for 7 years. | Eosinophilia | Serology for S. stercoralis Molecular diagnosis of S. stercoralis in fresh fecal samples using RT-PCR | RT-PCR | Eosinophils normal | Anakinra Methylprednisolone (80 mg, tapered over 1 month; from day 49 quick tapering from 16 mg to stop over 7 days). | Ivermectin (single dose) | Recovery |
| Study | Certain | Probable/Likely | Possible | Unlikely | Conditional/Unclassified | Unassessable/Unclassifiable |
|---|---|---|---|---|---|---|
| Alian 2022 [25] | No | No | No | No | No | Yes |
| Babazadeh 2022 [26] | No | Yes | No | No | No | No |
| Feria 2022 case 1 [27] | No | Yes | No | No | No | No |
| Feria 2022 case 2 [27] | No | Yes | No | No | No | No |
| Gautam 2021 [28] | No | No | Yes | No | No | No |
| Kim 2022 [29] | No | Yes | No | No | No | No |
| Lier 2022 [30] | Yes | No | No | No | No | No |
| Lorenzo 2022 patient 1 [31] | No | No | No | No | No | Yes |
| Lorenzo 2022 patient 2 [31] | No | No | No | No | No | Yes |
| Lorenzo 2022 patient 3 [31] | No | No | No | No | No | Yes |
| Lorenzo 2022 patient 4 [31] | No | No | No | No | No | Yes |
| Lorenzo 2022 patient 5 [31] | No | No | No | No | No | Yes |
| Lorenzo 2022 patient 6 [31] | No | No | No | No | No | Yes |
| Lorenzo 2022 patient 7 [31] | No | No | No | No | No | Yes |
| Marchese 2021 [32] | No | No | Yes | No | No | No |
| Martinez 2021 [33] | No | No | No | No | No | Yes |
| Nakandakaria 2021 [34] | No | No | No | Yes | No | No |
| Nunez-Gomez 2021 [35] | No | No | Yes | No | No | No |
| O’Dowling 2022 [36] | No | No | No | Yes | No | No |
| Patel 2021 [37] | No | No | Yes | No | No | No |
| Pintos-Pascual 2021 [38] | No | Yes | No | No | No | No |
| Singh 2021 [39] | No | No | No | No | No | Yes |
| Stylemans 2021 [40] | No | No | Yes | No | No | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosca, E.C.; Heneghan, C.; Spencer, E.A.; Plüddemann, A.; Maltoni, S.; Gandini, S.; Onakpoya, I.J.; Evans, D.; Conly, J.M.; Jefferson, T. Coinfection with Strongyloides and SARS-CoV-2: A Systematic Review. Trop. Med. Infect. Dis. 2023, 8, 248. https://doi.org/10.3390/tropicalmed8050248
Rosca EC, Heneghan C, Spencer EA, Plüddemann A, Maltoni S, Gandini S, Onakpoya IJ, Evans D, Conly JM, Jefferson T. Coinfection with Strongyloides and SARS-CoV-2: A Systematic Review. Tropical Medicine and Infectious Disease. 2023; 8(5):248. https://doi.org/10.3390/tropicalmed8050248
Chicago/Turabian StyleRosca, Elena C., Carl Heneghan, Elizabeth A. Spencer, Annette Plüddemann, Susanna Maltoni, Sara Gandini, Igho J. Onakpoya, David Evans, John M. Conly, and Tom Jefferson. 2023. "Coinfection with Strongyloides and SARS-CoV-2: A Systematic Review" Tropical Medicine and Infectious Disease 8, no. 5: 248. https://doi.org/10.3390/tropicalmed8050248