
Application of Sonographic Assessments of the Rate of Proximal Progression to Monitor Protobothrops mucrosquamatus Bite-Related Local Envenomation: A Prospective Observational Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment and Characteristics
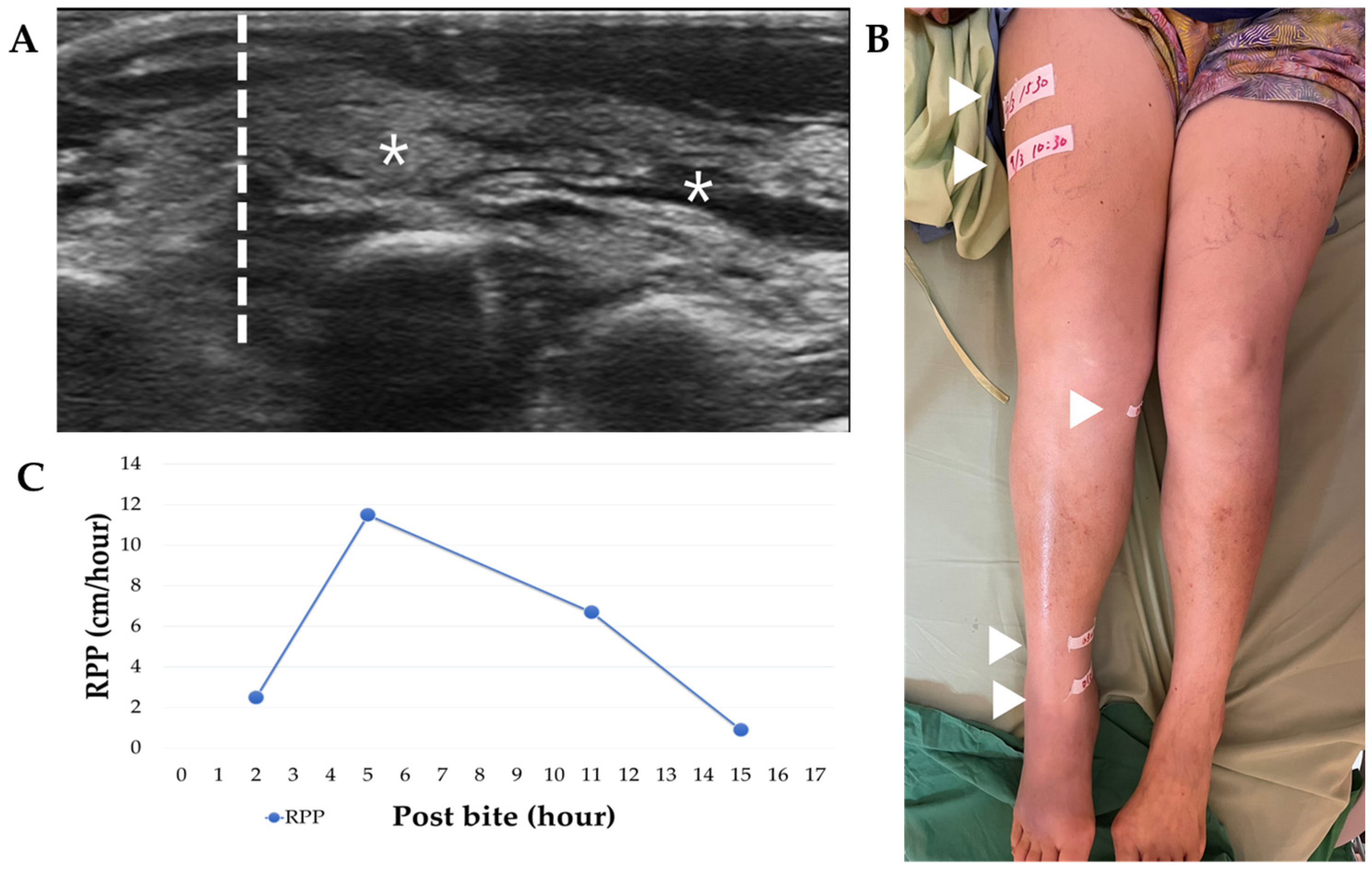
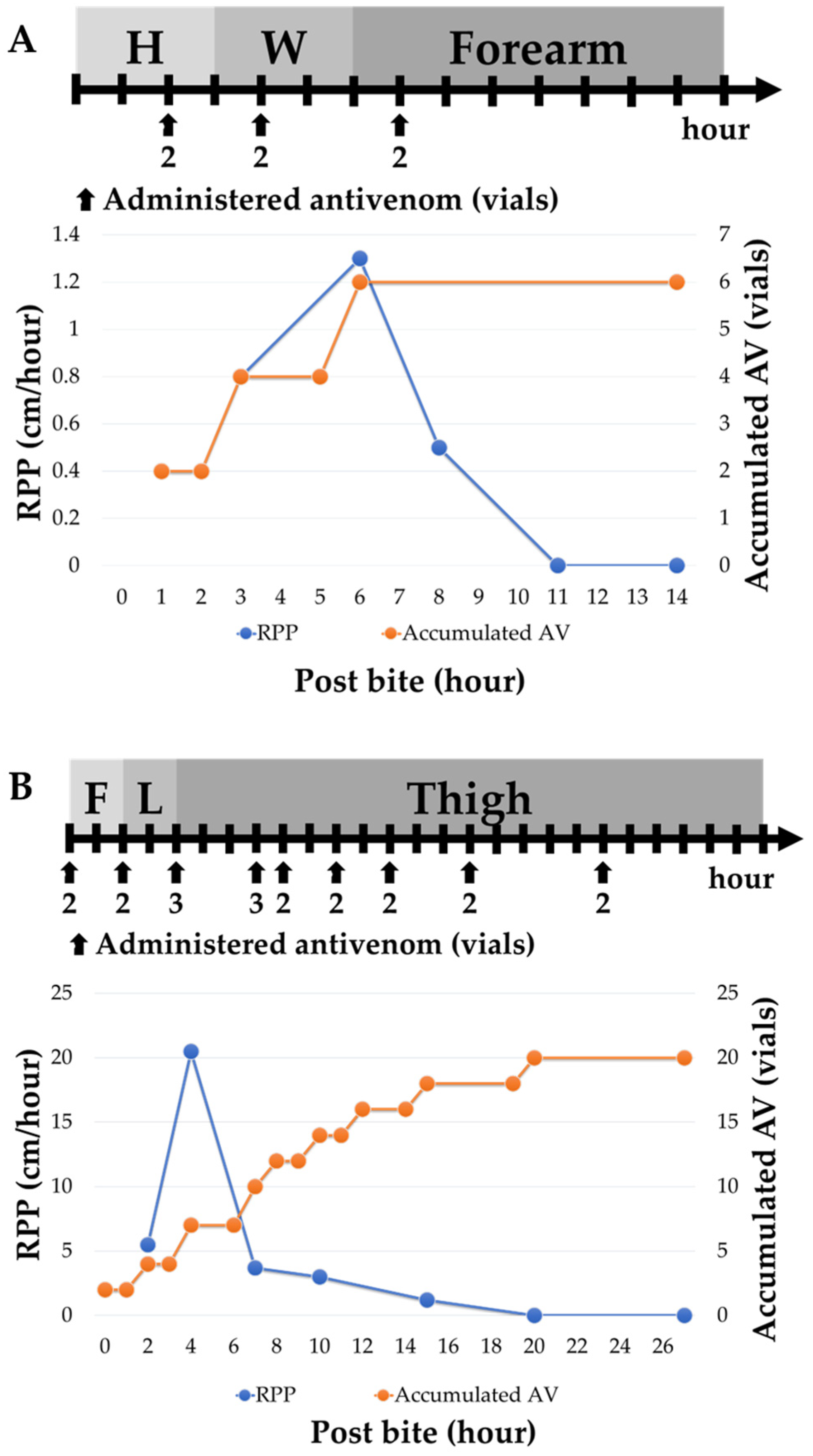
2.2. Patient Management: Antivenom Administration and POCUS Monitoring
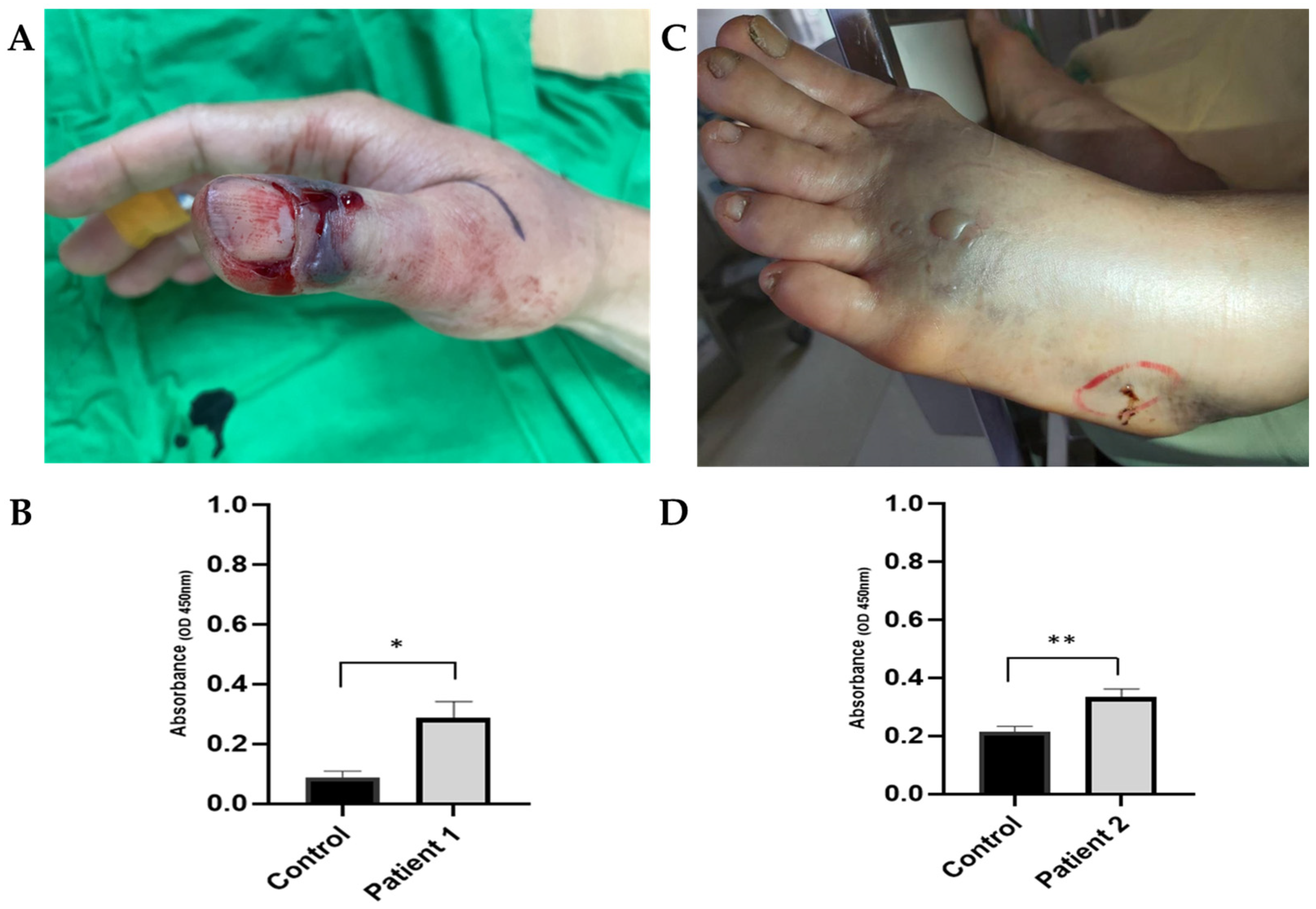
2.3. Toxin analysis: Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Recruited Patients
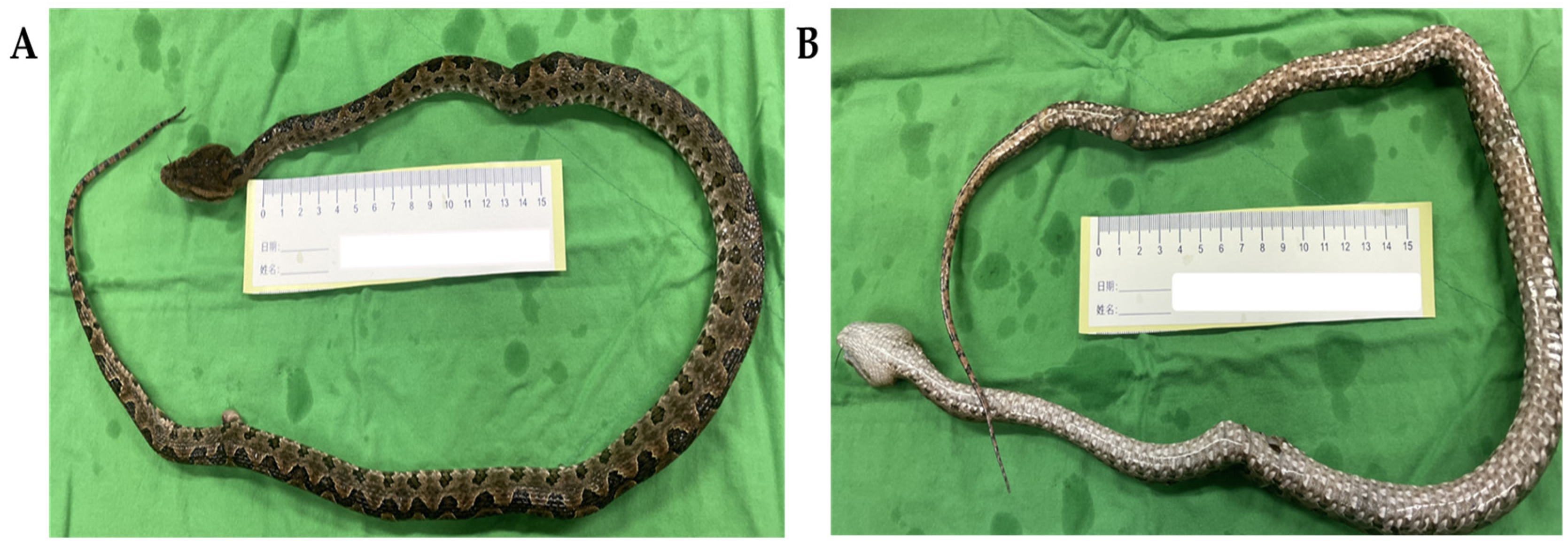
3.2. Characteristics of the Patients Bitten by P. mucrosquamatus
3.3. Different Types of Clinical Management Based on the RPP
3.4. Surgery for Patients Bitten by P. mucrosquamatus
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mao, Y.-C.; Hung, D.-Z. Epidemiology of Snake Envenomation in Taiwan. In Clinical Toxinology in Asia Pacific and Africa, 1st ed.; Gopalakrishnakone, P., Ed.; Springer: Heidelberg, Germany; New York, NY, USA; Dordrecht, The Netherlands; London, UK, 2015; pp. 3–22. [Google Scholar]
- Chung, K.-F.; Shao, K.-T. Checklist of Taiwanese Species. Available online: https://taibnet.sinica.edu.tw/home.php? (accessed on 1 January 2003).
- Ho, C.-H.; Mao, Y.-C.; Tsai, Y.-D.; Lin, C.-S.; Liu, S.-H.; Chiang, L.-C.; Hung, Y.; Tsai, S.-H. Descriptive study of snakebite patients in Northern Taiwan: 2009 to 2016. J. Med. Sci. 2019, 39, 114–120. [Google Scholar] [CrossRef]
- Mao, Y.C.; Liu, P.Y.; Chiang, L.C.; Lee, C.H.; Lai, C.S.; Lai, K.L.; Lin, W.L.; Su, H.Y.; Ho, C.H.; Doan, U.V.; et al. Clinical manifestations and treatments of Protobothrops mucrosquamatus bite and associated factors for wound necrosis and subsequent debridement and finger or toe amputation surgery. Clin. Toxicol. 2020, 59, 28–37. [Google Scholar] [CrossRef]
- Liu, C.C.; Wu, C.J.; Hsiao, Y.C.; Yang, Y.H.; Liu, K.L.; Huang, G.J.; Hsieh, C.H.; Chen, C.K.; Liaw, G.W. Snake venom proteome of Protobothrops mucrosquamatus in Taiwan: Delaying venom-induced lethality in a rodent model by inhibition of phospholipase A2 activity with varespladib. J. Proteom. 2021, 234, 104084–104093. [Google Scholar] [CrossRef] [PubMed]
- Chiang, L.-C.; Chien, K.-Y.; Su, H.-Y.; Chen, Y.-C.; Mao, Y.-C.; Wu, W.-G. Comparison of Protein Variation in Protobothrops mucrosquamatus Venom between Northern and Southeast Taiwan and Association with Human Envenoming Effects. Toxins 2022, 14, 643. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, J.M.; Rucavado, A.; Escalante, T. Snake Venom Metalloproteinases Biological Roles and Participation in the Pathophysiology of Envenomation. In Handbook of Venoms and Toxins of Reptiles; Mackessy, S.P., Mackessy, S.P., Eds.; CRC Press Inc.: London, UK, 2009; pp. 115–139. [Google Scholar]
- Doley, R.; Zhou, X.; Kini, R.M. Snake Venom Phospholipase A2 Enzymes. In Handbook of Venoms and Toxins of Reptiles, 1st ed.; Mackessy, S.P., Mackessy, S.P., Eds.; CRC Press Inc.: London, UK, 2009; p. 528. [Google Scholar]
- Mao, Y.-C.; Hung, D.-Z. Management of Snake Envenomation in Taiwan. In Clinical Toxinology in Asia Pacific and Africa, 1st ed.; Gopalakrishnakone, P., Ed.; Springer: Heidelberg, Germany; New York, NY, USA; Dordrecht, The Netherlands; London, UK, 2015; pp. 23–52. [Google Scholar]
- Ming-Yi, L.; Ruey-Jen, H. Toxoids and Antivenoms of Venomous Snakes in Taiwan. J. Toxicol. Toxin Rev. 1997, 16, 163–175. [Google Scholar] [CrossRef]
- Mao, Y.C.; Liu, P.Y.; Chiang, L.C.; Lai, C.S.; Lai, K.L.; Ho, C.H.; Wang, T.H.; Yang, C.C. Naja atra snakebite in Taiwan. Clin. Toxicol. 2017, 56, 273–280. [Google Scholar] [CrossRef]
- Blaylock, R.S. Antibiotic use and infection in snakebite victims. S. Afr. Med. J. 1999, 89, 874–876. [Google Scholar]
- Ho, C.H.; Ismail, A.K.; Liu, S.H.; Tzeng, Y.S.; Li, L.Y.; Pai, F.C.; Hong, C.W.; Mao, Y.C.; Chiang, L.C.; Lin, C.S.; et al. The role of a point-of-care ultrasound protocol in facilitating clinical decisions for snakebite envenomation in Taiwan: A pilot study. Clin. Toxicol. 2021, 59, 794–800. [Google Scholar] [CrossRef]
- Ismail, A.K. Snakebite and Envenomation Management in Malaysia. Toxinol. Clin. Toxinol. Asia Pac. Africa 2015, 2, 71–102. [Google Scholar]
- Theakston, R.D.; Warrell, D.A. Antivenoms: A list of hyperimmune sera currently available for the treatment of envenoming by bites and stings. Toxicon Off. J. Int. Soc. Toxinol. 1991, 29, 1419–1470. [Google Scholar] [CrossRef]
- Chieh-Fan, C.; Tzeng-Jih, L.; Wen-Chi, H.; Hua-Wei, Y. Appropriate antivenom doses for six types of envenomations caused by snakes in taiwan. J. Venom. Anim. Toxins Incl. Trop. Dis. 2009, 15, 479–490. [Google Scholar] [CrossRef]
- Liu, J.; He, Q.; Wang, W.; Zhou, B.; Li, B.; Zhang, Y.; Luo, C.; Chen, D.; Tang, J.; Yu, X. Preparation and neutralization efficacy of IgY antibodies raised against Deinagkistrodon acutus venom. J. Venom. Anim. Toxins Incl. Trop. Dis. 2017, 23, 22. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Dong, W.; Kong, T. Preparation and characterization of immunoglobulin yolk against the venom of Naja naja atra. Indian J. Exp. Biol. 2010, 48, 778–785. [Google Scholar] [PubMed]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Hung, D.-Z.; Chen, W.-K. Antivenin-related Serum Sickness. J. Chin. Med. Assoc. 2010, 73, 540–542. [Google Scholar] [CrossRef]
- LoVecchio, F.; Klemens, J.; Roundy, E.B.; Klemens, A. Serum sickness following administration of Antivenin (Crotalidae) Polyvalent in 181 cases of presumed rattlesnake envenomation. Wilderness Environ. Med. 2003, 14, 220–221. [Google Scholar] [CrossRef]
- Sawai, Y.; Tseng, C.S. Snakebites on Taiwan. Snake 1969, 1, 9. [Google Scholar]
- Chen, C.-K.; Lin, C.-C.; Shih, F.-Y.; Chaou, C.-H.; Lin, J.C.-C.; Lai, T.-I.; Tseng, C.-Y.; Fang, C.-C. Population-based study of venomous snakebite in Taiwan. J. Acute Med. 2015, 5, 38–42. [Google Scholar] [CrossRef]
- Lin, C.-C.; Shih, C.-P.; Wang, C.-C.; Ouyang, C.-H.; Liu, C.-C.; Yu, J.-S.; Lo, C.-H. The Clinical Usefulness of Taiwan Bivalent Freeze-Dried Hemorrhagic Antivenom in Protobothrops mucrosquamatus- and Viridovipera stejnegeri-Envenomed Patients. Toxins 2022, 14, 794. [Google Scholar] [CrossRef]
- Ralph, R.; Faiz, M.A.; Sharma, S.K.; Ribeiro, I.; Chappuis, F. Managing snakebite. BMJ 2022, 376, e057926. [Google Scholar] [CrossRef]
- Ho, C.-H.; Chiang, L.-C.; Mao, Y.-C.; Lan, K.-C.; Tsai, S.-H.; Shih, Y.-J.; Tzeng, Y.-S.; Lin, C.-S.; Lin, W.-L.; Fang, W.-H.; et al. Analysis of the Necrosis-Inducing Components of the Venom of Naja atra and Assessment of the Neutralization Ability of Freeze-Dried Antivenom. Toxins 2021, 13, 619. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.C.; Wu, C.J.; Chou, T.Y.; Liaw, G.W.; Hsiao, Y.C.; Chu, L.J.; Lee, C.H.; Wang, P.J.; Hsieh, C.H.; Chen, C.K.; et al. Development of a Monoclonal scFv against Cytotoxin to Neutralize Cytolytic Activity Induced by Naja atra Venom on Myoblast C2C12 Cells. Toxins 2022, 14, 459. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.C.; Chou, Y.S.; Chen, C.Y.; Liu, K.L.; Huang, G.J.; Yu, J.S.; Wu, C.J.; Liaw, G.W.; Hsieh, C.H.; Chen, C.K. Pathogenesis of local necrosis induced by Naja atra venom: Assessment of the neutralization ability of Taiwanese freeze-dried neurotoxic antivenom in animal models. PLoS Negl. Trop. Dis. 2020, 14, e0008054–e0008074. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.W.; Liu, B.S.; Chien, K.Y.; Chiang, L.C.; Huang, S.Y.; Sung, W.C.; Wu, W.G. Cobra venom proteome and glycome determined from individual snakes of Naja atra reveal medically important dynamic range and systematic geographic variation. J Proteom. 2015, 128, 92–104. [Google Scholar] [CrossRef]
- Cichutek, K.; Epstein, J.; Griffiths, E.; Hindawi, S.; Jivapaisarnpong, T.; Klein, H.; Minor, P.; Moftah, F.; Reddy, V.R.; Slamet, L.S.; et al. WHO Expert Committee on Biological Standardization, Sixty-Seventh Report; WHO Technical Report Series no. 1004; World Health Organization: Geneva, Switzerland, 2017; pp. 321–322. [Google Scholar]
- Lawley, T.J.; Bielory, L.; Gascon, P.; Yancey, K.B.; Young, N.S.; Frank, M.M. A prospective clinical and immunologic analysis of patients with serum sickness. N. Engl. J. Med. 1984, 311, 1407–1413. [Google Scholar] [CrossRef]
- Ryan, N.M.; Downes, M.A.; Isbister, G.K. Clinical features of serum sickness after Australian snake antivenom. Toxicon Off. J. Int. Soc. Toxinol. 2015, 108, 181–183. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group I | Group II | Group II | ||||
|---|---|---|---|---|---|---|
| p-Value | IIA | IIB | p-Value | |||
| Patients [persons, percentage (%)] | 7 (24) | 22 (76) | 11 (50) | 11 (50) | ||
| Severe swelling condition (Blaylock category) | <0.0001 | 0.59 | ||||
| Minimal | 7 (100) | 0 | 0 | 0 | ||
| Mild | 0 | 17 (77) | 9 (81) | 8 (73) | ||
| Moderate | 0 | 4 (18) | 2 (19) | 2 (18) | ||
| Severe | 0 | 1 (5) | 0 | 1 (9) | ||
| Gross | 0 | 0 | 0 | 0 | ||
| Gender | 0.06 | 0.08 | ||||
| Male | 6 (86) | 10 (45) | 3 (27) | 7 (64) | ||
| Age (year-old) | 0.65 | 0.21 | ||||
| Median | 59.00 | 57.50 | 60.00 | 55.00 | ||
| Range | 25–65 | 5–82 | 30–82 | 5–76 | ||
| Identify methods | 0.54 | 0.67 | ||||
| Snake body | 2 (29) | 7 (32) | 4 (36) | 3 (27) | ||
| Photo picture | 5 (71) | 12 (55) | 5 (45) | 7 (64) | ||
| Toxin analysis | 0 | 3 (14) | 2 (18) | 1 (9) | ||
| Encountered season | 0.63 | 0.12 | ||||
| Winter (12–2) | 0 | 2 (9) | 1 (9) | 1 (9) | ||
| Spring (3–5) | 2 (29) | 3 (14) | 0 | 3 (27) | ||
| Summer (6–8) | 1 (14) | 6 (27) | 5 (45) | 1 (9) | ||
| Fall (9–11) | 4 (57) | 11 (50) | 5 (45) | 6 (55) | ||
| Bite site | 0.44 | 0.34 | ||||
| finger | 0 | 2 (9) | 1 (9) | 1 (9) | ||
| hand | 4 (57) | 3 (14) | 1 (9) | 2 (18) | ||
| forearm | 0 | 1 (5) | 0 | 1 (9) | ||
| toe | 1 (14) | 4 (18) | 2 (18) | 2 (18) | ||
| foot | 2 (29) | 10 (45) | 5 (45) | 5 (45) | ||
| lower leg | 0 | 2 (9) | 2 (18) | 0 | ||
| Clinical presentation | 0.06 | 1 | ||||
| Fever | 0 | 0 | 0 | 0 | ||
| Local cyanosis | 7 (100) | 22 (100) | 11 (100) | 11 (100) | ||
| Progressed swelling | 0 | 22 (100) | 11 (100) | 11 (100) | ||
| Wound necrosis | 0 | 2 (9) | 1 (9) | 1 (9) | ||
| Bullae/ Blister | 0 | 2 (9) | 1 (9) | 1 (9) | ||
| Laboratory results | ||||||
| WBC [normal range: 4500–11,000 cells/μL] | 0.12 | 0.06 | ||||
| WBC (>11,000) | 0 | 6 (27) | 5 (45) | 1 (9) | ||
| WBC (<11,000) | 7 (100) | 16 (73) | 6 (55) | 10 (91) | ||
| PLT [normal range: 150,000–400,000 cells/μL] | 0.41 | 0.14 | ||||
| PLT (<150,000) | 0 | 2 (9) | 2 (18) | 0 | ||
| PLT (>150,000) | 7 (100) | 20 (81) | 9 (82) | 11 (100) | ||
| CK [normal range: 39–308 U/L] | 0.44 | 0.73 | ||||
| CK (>1000) | 0 | 2 (9%) | 1 (14) | 1 (9) | ||
| CK (<1000) | 5 (71) | 16 (73) | 6 (86) | 10 (91) | ||
| Kindo grade renal function (eGFR, mL/min/1.73 m2) | 0.38 | 0.17 | ||||
| Grade 1 (>90) | 4 (57) | 10 (45) | 3 (27) | 7 (64) | ||
| Grade 2 (60–89) | 3 (43) | 7 (32) | 4 (36) | 3 (27) | ||
| Grade 3 (30–59) | 0 | 5 (23) | 4 (36) | 1 (9) | ||
| Grade 4 (15–29) | 0 | 0) | 0 | 0 | ||
| Grade 5 (<15) | 0 | 0 | 0 | 0 | ||
| Administered antivenom (vials) | <0.0001 | <0.001 | ||||
| Median | 2.00 | 9.50 | 6.00 | 12.00 | ||
| Range | 1–4 | 4–22 | 4–10 | 8–22 | ||
| ED-LOS (hours) | <0.0001 | 0.03 | ||||
| Median | 8.00 | 24.50 | 21.00 | 27.50 | ||
| Range | 3–18 | 13–61 | 13–36 | 15.5–61 | ||
| Disposition | 0.22 | 0.33 | ||||
| ED discharge | 7 (100) | 18 (82) | 8 (73) | 10 (91) | ||
| admission and surgery | 0 | 2 (9) | 1 (9) | 1 (9) | ||
| admission without surgery | 0 | 2 (9) | 2 (18) | 0 | ||
| Complete remission days | <0.001 | 0.06 | ||||
| Median | 2.00 | 10.00 | 7.00 | 12.00 | ||
| Range | 1–2 | 1–49 | 1–25 | 6–49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, F.-C.; Ismail, A.K.; Mao, Y.-C.; Hsu, C.-H.; Chiang, L.-C.; Shih, C.-C.; Tzeng, Y.-S.; Lin, C.-S.; Liu, S.-H.; Ho, C.-H. Application of Sonographic Assessments of the Rate of Proximal Progression to Monitor Protobothrops mucrosquamatus Bite-Related Local Envenomation: A Prospective Observational Study. Trop. Med. Infect. Dis. 2023, 8, 246. https://doi.org/10.3390/tropicalmed8050246
Chen F-C, Ismail AK, Mao Y-C, Hsu C-H, Chiang L-C, Shih C-C, Tzeng Y-S, Lin C-S, Liu S-H, Ho C-H. Application of Sonographic Assessments of the Rate of Proximal Progression to Monitor Protobothrops mucrosquamatus Bite-Related Local Envenomation: A Prospective Observational Study. Tropical Medicine and Infectious Disease. 2023; 8(5):246. https://doi.org/10.3390/tropicalmed8050246
Chicago/Turabian StyleChen, Feng-Chen, Ahmad Khaldun Ismail, Yan-Chiao Mao, Chih-Hsiung Hsu, Liao-Chun Chiang, Chang-Chih Shih, Yuan-Sheng Tzeng, Chin-Sheng Lin, Shing-Hwa Liu, and Cheng-Hsuan Ho. 2023. "Application of Sonographic Assessments of the Rate of Proximal Progression to Monitor Protobothrops mucrosquamatus Bite-Related Local Envenomation: A Prospective Observational Study" Tropical Medicine and Infectious Disease 8, no. 5: 246. https://doi.org/10.3390/tropicalmed8050246