

Modeling the Spread of COVID-19 with the Control of Mixed Vaccine Types during the Pandemic in Thailand
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
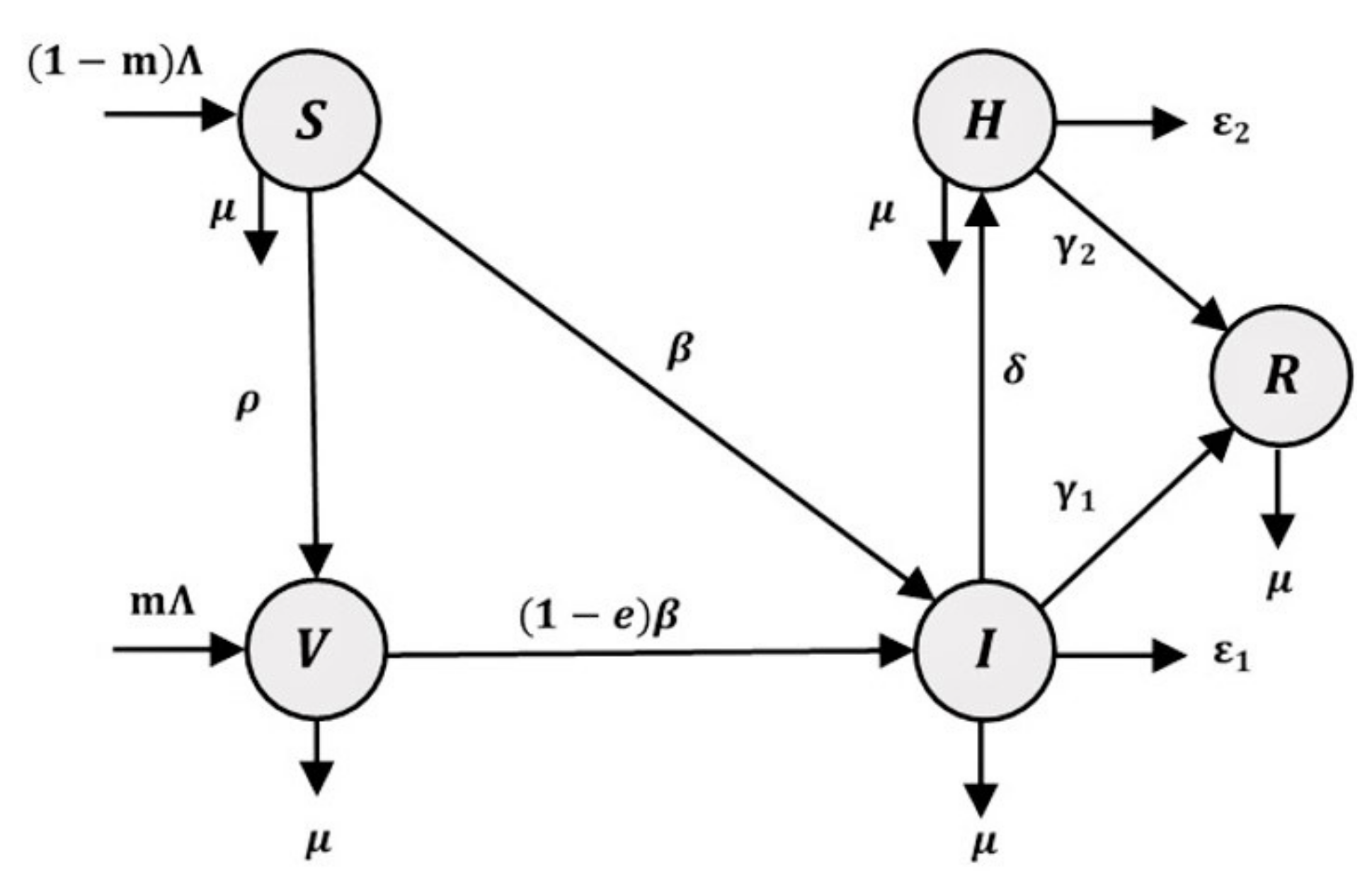
2.1. Mathematical Models
- is the number of people recruited from the population per day;
- is the proportion of vaccinated individuals;
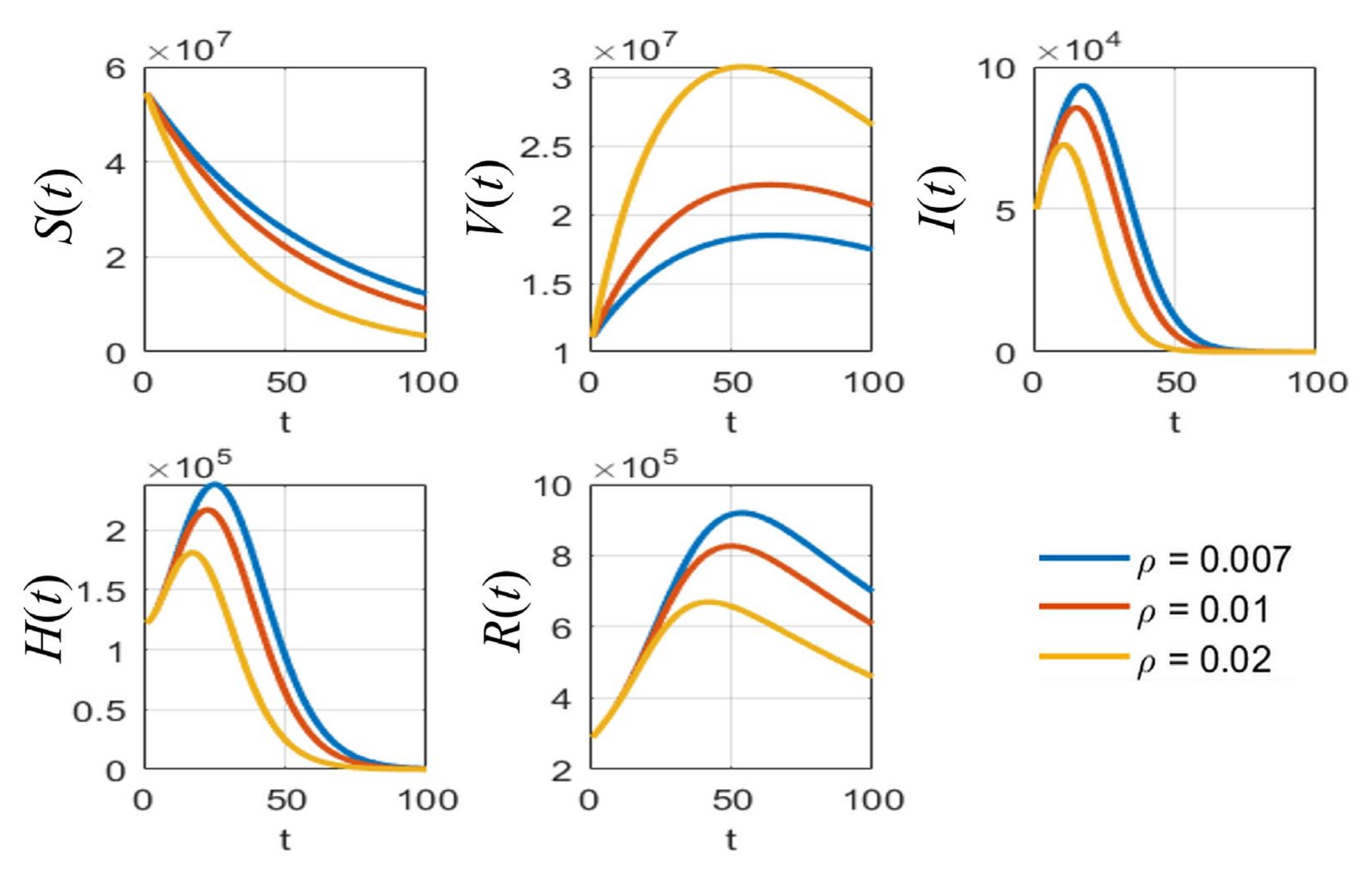
- is the vaccination rate per day;
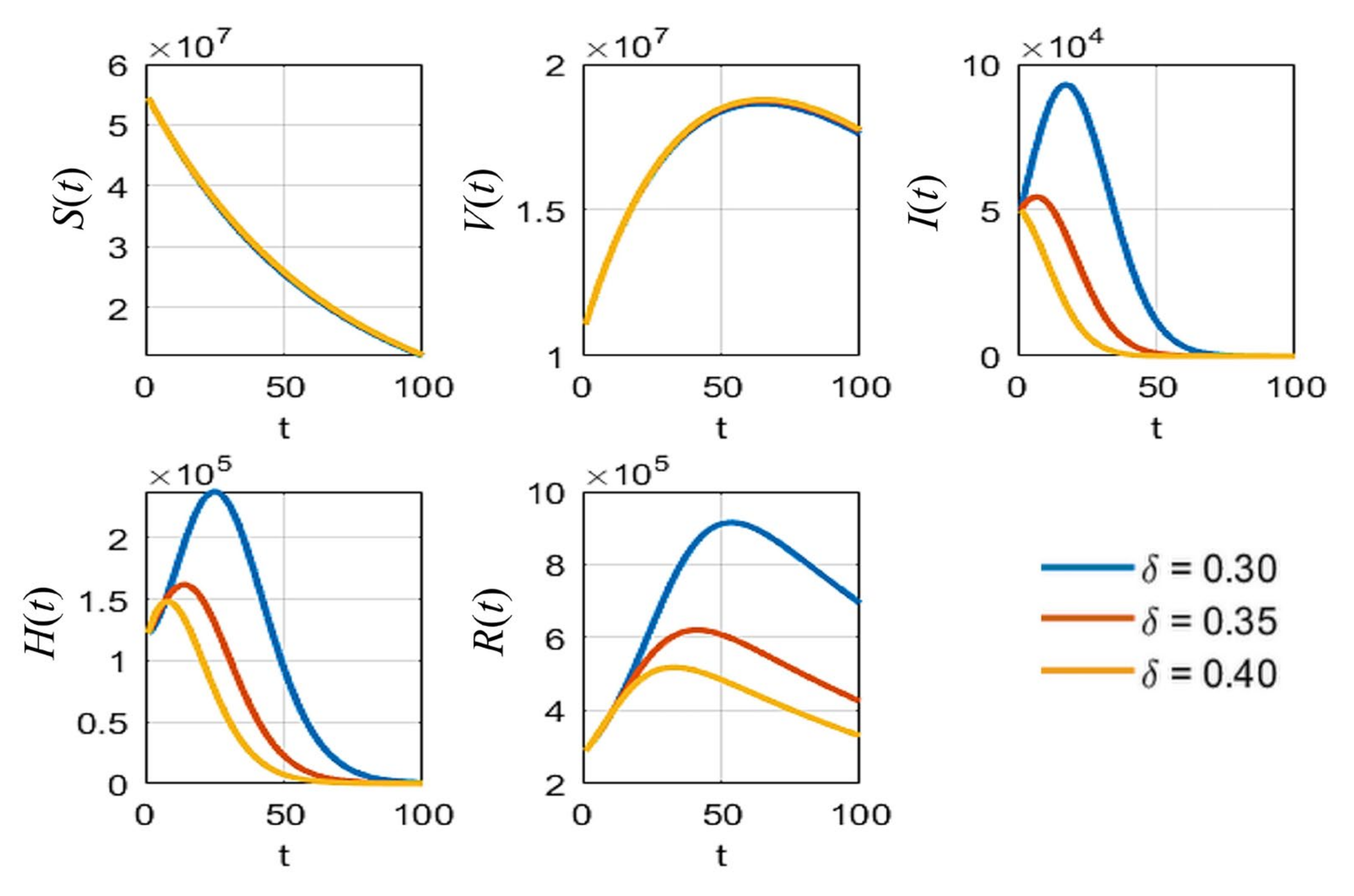
- is the vaccine efficacy or reduced rate of vaccination, the value of which varies depending on the type of vaccine;
- is the transmission rate, the value of which is defined by the probability of disease transmission in a single contact multiplied by the average number of contacts per person;
- are the recovery rates of infected individuals and hospitalized individuals, respectively;
- are the induced COVID-19 death rates of infected individuals and hospitalized individuals, respectively;
- is the rate of detection, which is the level of attention to the disease; and
- is the natural death rate, i.e., the rate of people who die without COVID-19 symptoms.
2.2. Model Analysis
2.2.1. The Nature of the Model Parameters
2.2.2. Equilibrium Points
- with , , , , , , and .
2.2.3. The Basic Reproduction Numbers
2.2.4. Stability of the Disease-Free Equilibrium Point
2.2.5. Stability of the Endemic Equilibrium Point
- ,
- and .
2.2.6. Sensitivity Analysis
2.3. Data Collection and Implementation
3. Results
3.1. Parameter Estimation and the Relationship between Ro, Transmission Rate, and Vaccine Efficacy
3.2. Simulation and Equilibrium Points
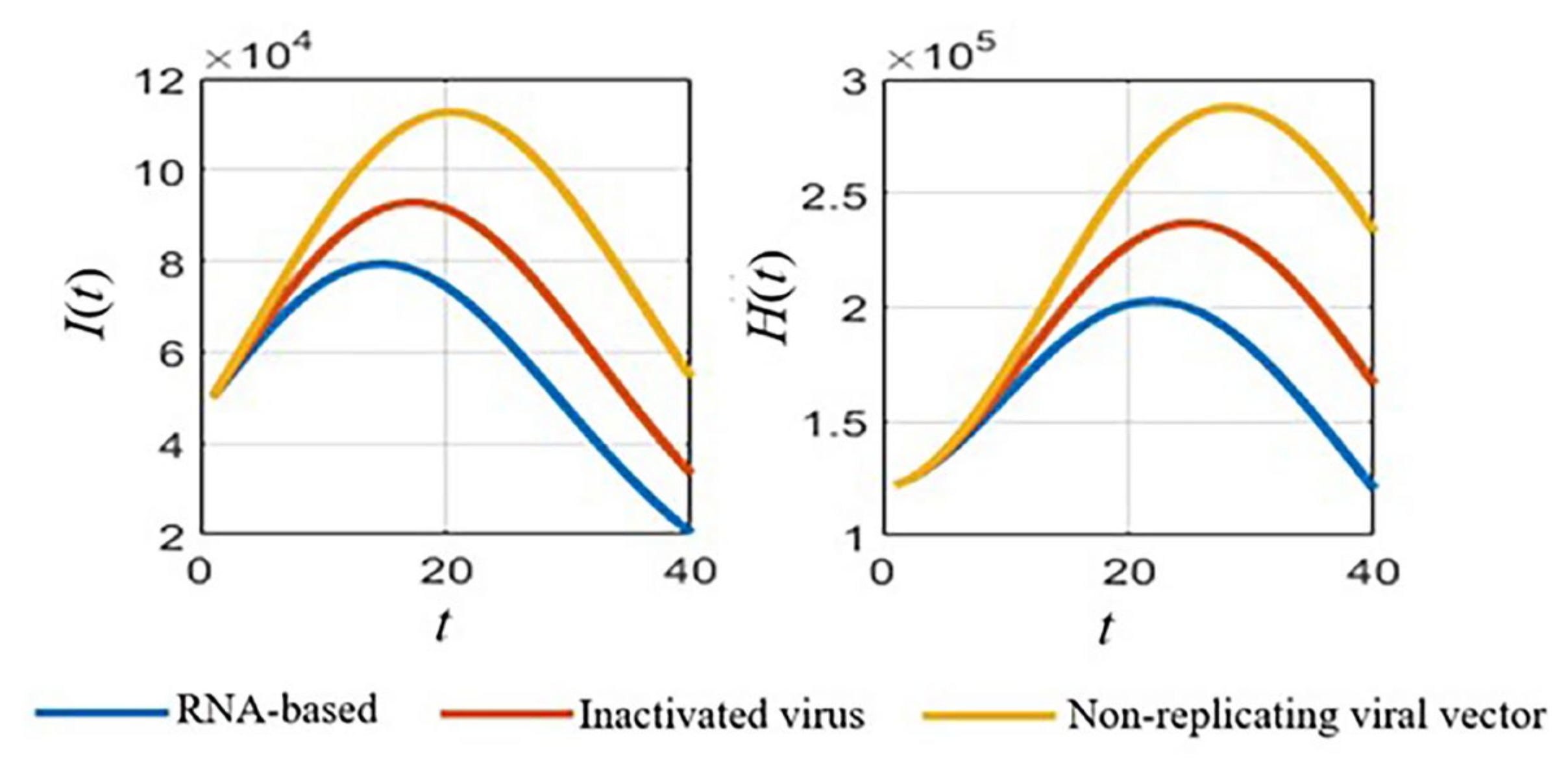
3.2.1. Simulations of the SVIHR Model with Different Types of Vaccine
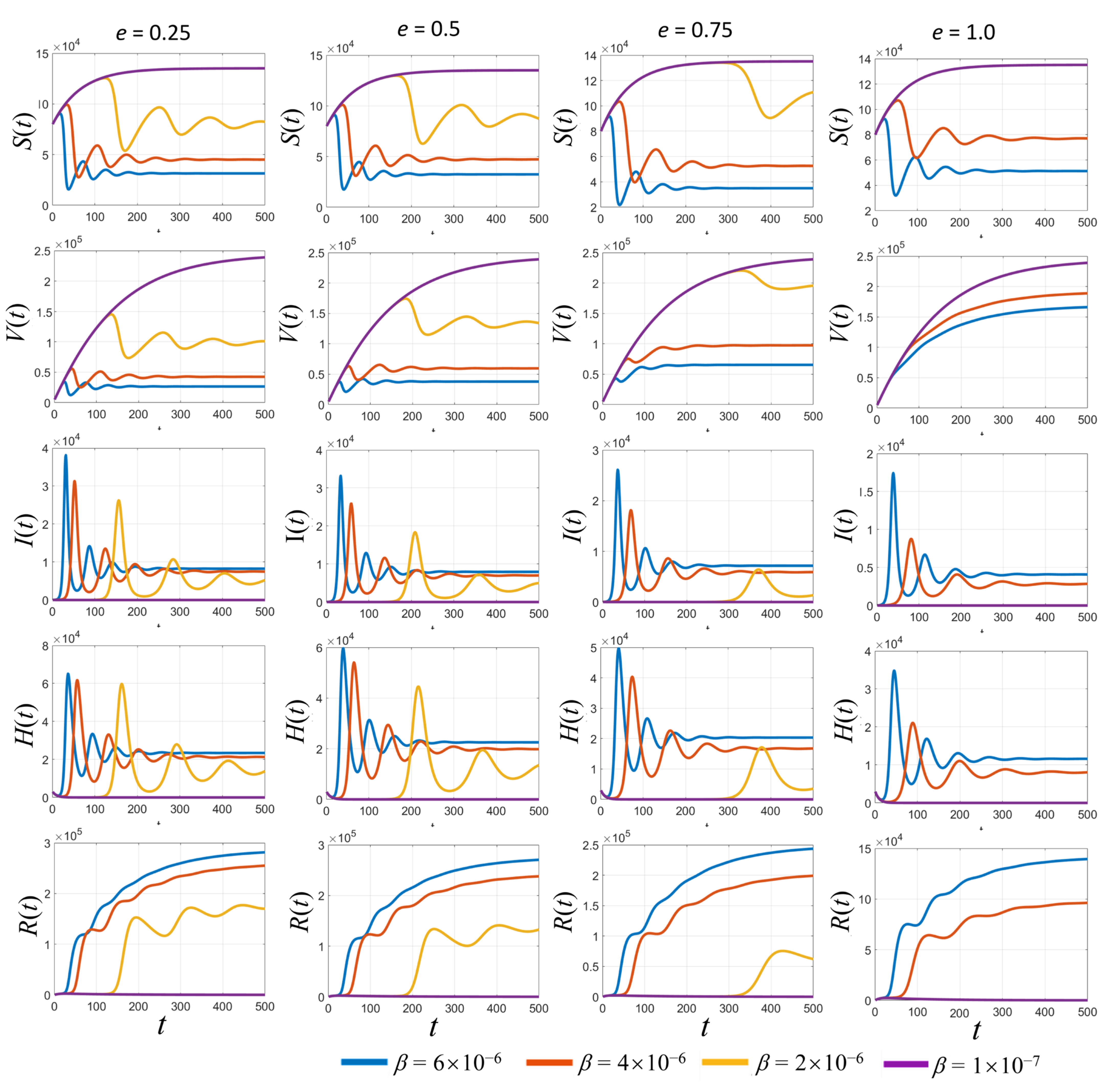
3.2.2. Simulation of the SVIHR Model with Various Transmission Rates and Vaccine Efficacy
3.3. Sensitivity of Parameters and Impact on the Pandemic
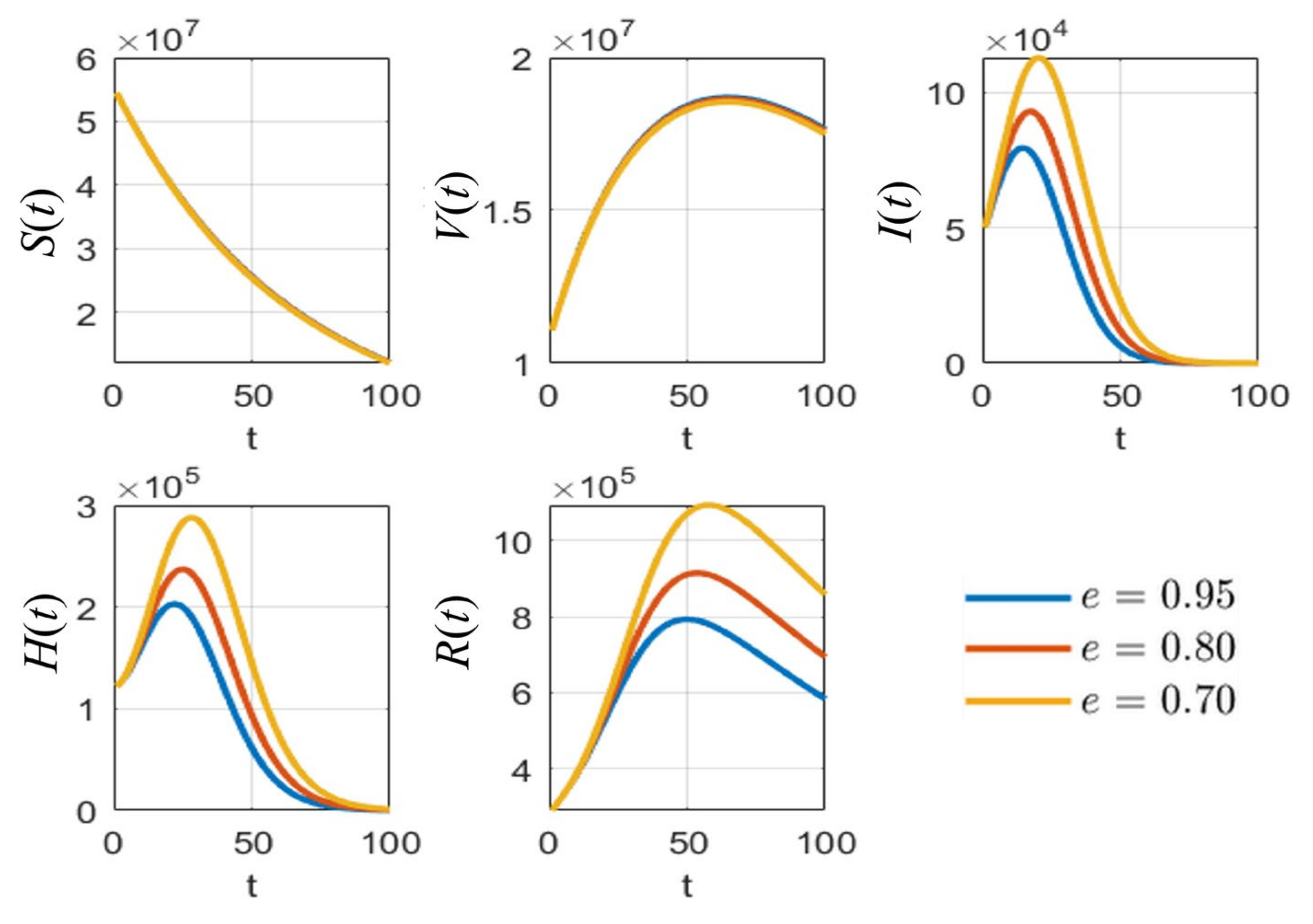
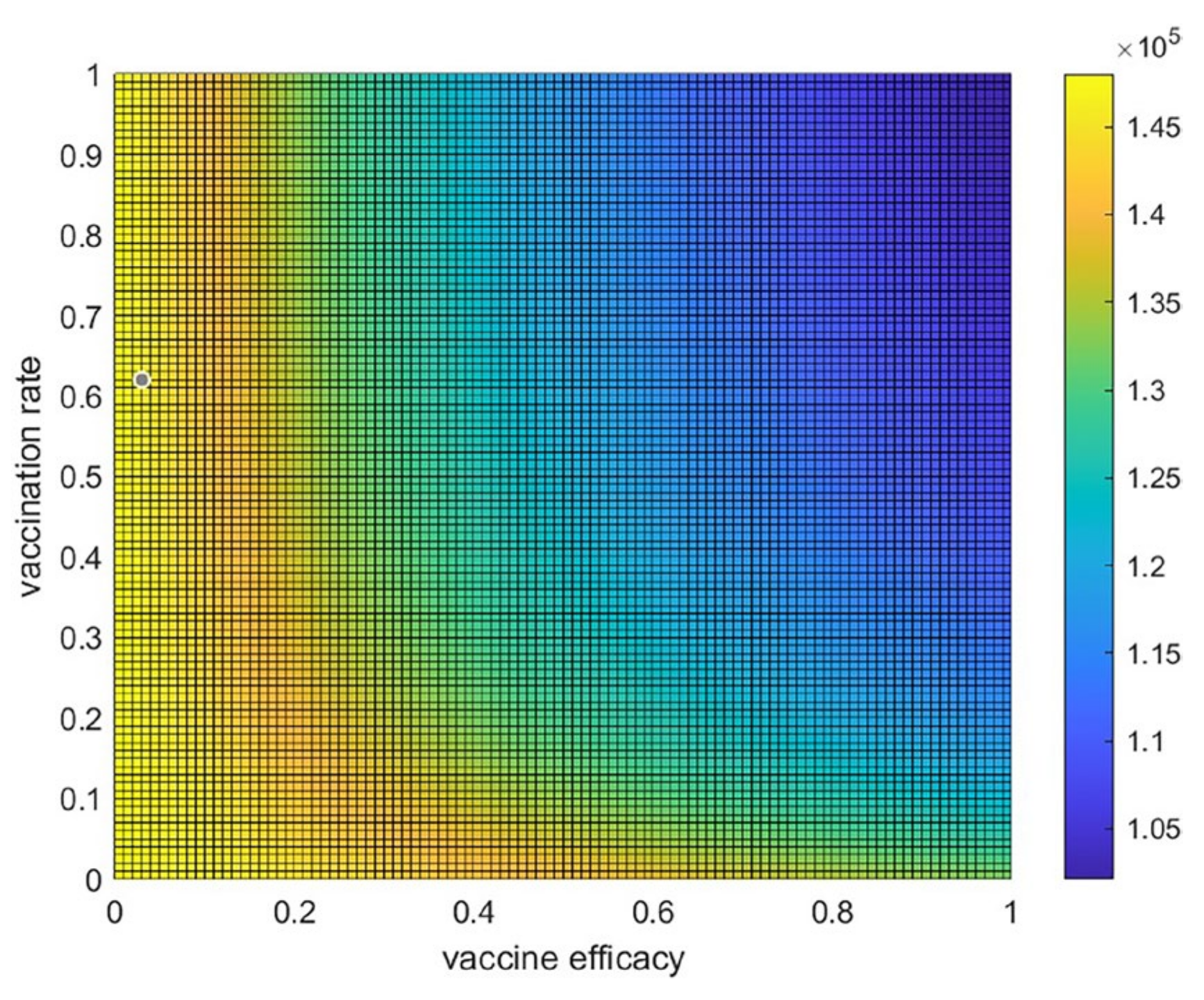
3.4. Trade-Off between Vaccine Efficacy and Vaccination Rate
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 28 July 2021).
- Cattaneo, C.; Pagliarini, E.; Mambrini, S.P.; Tortorici, E.; Mene, R.; Torlasco, C.; Perger, E.; Parati, G.; Bertoli, S. Changes in smell and taste perception related to COVID-19 infection: A case-control study. Sci. Rep. 2022, 12, 8192. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Dashtbali, M.; Mirzaie, M. A compartmental model that predicts the effect of social distancing and vaccination on controlling COVID-19. Sci. Rep. 2021, 11, 8191. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Costa Clemens, S.A.; Weckx, L.; Clemens, R.; Almeida Mendes, A.V.; Ramos Souza, A.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; de Moraes Pinto, M.I.; Gonzalez, I.G.S.; et al. Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): A phase 4, non-inferiority, single blind, randomised study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Shay, D.K.; Gee, J.; Su, J.R.; Myers, T.R.; Marquez, P.; Liu, R.; Zhang, B.; Licata, C.; Clark, T.A.; Shimabukuro, T.T. Safety Monitoring of the Janssen (Johnson & Johnson) COVID-19 Vaccine—United States, March-April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 680–684. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.N.M.; May, B.P.; Ung, T.T.; Nguyen, M.K.; Nguyen, T.T.T.; Dinh, V.L.; Doan, C.C.; Tran, T.V.; Khong, H.; Nguyen, T.T.T.; et al. Preclinical Immune Response and Safety Evaluation of the Protein Subunit Vaccine Nanocovax for COVID-19. Front. Immunol. 2021, 12, 4856. [Google Scholar] [CrossRef]
- Ministry of Public Health. COVID-19 Situation Reports. Available online: https://ddc.moph.go.th/viralpneumonia/eng/situation.php (accessed on 28 July 2021).
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.L.J. An Introduction to Stochastic Processes with Applications to Biology; Pearson Education: Hoboken, NJ, USA, 2003. [Google Scholar]
- Allen, S.L.J. An Introduction to Stochastic Epidemic Models: Mathematical Epidemiology; Springer: Berlin/Heidelberg, Germany, 2008; pp. 81–130. [Google Scholar]
- Hethcote, H.W. Three Basic Epidemiological Models. In Applied Mathematical Ecology; Springer: Berlin/Heidelberg, Germany, 1989; pp. 119–144. [Google Scholar] [CrossRef]
- Giordano, G.; Colaneri, M.; Di Filippo, A.; Blanchini, F.; Bolzern, P.; De Nicolao, G.; Sacchi, P.; Colaneri, P.; Bruno, R. Modeling vaccination rollouts, SARS-CoV-2 variants and the requirement for non-pharmaceutical interventions in Italy. Nat. Med. 2021, 27, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Husniah, H.; Ruhanda, R.; Supriatna, A.K.; Biswas, M.H.A. SEIR Mathematical Model of Convalescent Plasma Transfusion to Reduce COVID-19 Disease Transmission. Mathematics 2021, 9, 2857. [Google Scholar] [CrossRef]
- Prathumwan, D.; Trachoo, K.; Chaiya, I. Mathematical Modeling for Prediction Dynamics of the Coronavirus Disease 2019 (COVID-19) Pandemic, Quarantine Control Measures. Symmetry 2020, 12, 1404. [Google Scholar] [CrossRef]
- Intarapanya, T.; Suratanee, A.; Pattaradilokrat, S.; Plaimas, K. Modeling the spread of COVID-19 as a consequence of undocumented immigration toward the reduction of daily hospitalization: Case reports from Thailand. PLoS ONE 2022, 17, e0273558. [Google Scholar] [CrossRef]
- Jabal, K.A.; Wiegler, K.B.; Edelstein, M. Convalescent plasma from people vaccinated after COVID-19 infection. Lancet Microbe 2021, 2, e171–e172. [Google Scholar] [CrossRef]
- Nagoba, B.; Gavkare, A.; Jamadar, N.; Mumbre, S.; Selkar, S. Positive aspects, negative aspects and limitations of plasma therapy with special reference to COVID-19. J. Infect. Public Health 2020, 13, 1818–1822. [Google Scholar] [CrossRef] [PubMed]
- Diagne, M.L.; Rwezaura, H.; Tchoumi, S.Y.; Tchuenche, J.M. A Mathematical Model of COVID-19 with Vaccination and Treatment. Comput. Math. Methods Med. 2021, 2021, 1250129. [Google Scholar] [CrossRef]
- Leung, N.H.L. Transmissibility and transmission of respiratory viruses. Nat. Rev. Microbiol. 2021, 19, 528–545. [Google Scholar] [CrossRef]
- Van den Driessche, P.; Watmough, J. Reproduction numbers and sub-threshold endemic equilibria for compartmental models of disease transmission. Math. Biosci. 2002, 180, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Bodson, M. Explaining the Routh–Hurwitz Criterion: A Tutorial Presentation [Focus on Education]. IEEE Control Syst. Mag. 2020, 40, 45–51. [Google Scholar] [CrossRef]
- Chitnis, N.; Hyman, J.M.; Cushing, J.M. Determining important parameters in the spread of malaria through the sensitivity analysis of a mathematical model. Bull. Math. Biol. 2008, 70, 1272–1296. [Google Scholar] [CrossRef] [PubMed]
- Thailand Death Rate 2015–2020. United Nations—World Population Prospects. Available online: https://population.un.org/wpp/ (accessed on 9 February 2022).
- Hannah Ritchie, E.M.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Our World Data 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 9 February 2022).
- Higazy, M. Novel fractional order SIDARTHE mathematical model of COVID-19 pandemic. Chaos Solitons Fractals 2020, 138, 110007. [Google Scholar] [CrossRef] [PubMed]
- Arshad, S.; Khalid, S.; Javed, S.; Amin, N.; Nawaz, F. Modeling the impact of the vaccine on the COVID-19 epidemic transmission via fractional derivative. Eur. Phys. J. Plus 2022, 137, 802. [Google Scholar] [CrossRef]
- Algarni, A.D.; Ben Hamed, A.; Hamdi, M.; Elmannai, H.; Meshoul, S. Mathematical COVID-19 model with vaccination: A case study in Saudi Arabia. PeerJ Comput. Sci. 2022, 8, e959. [Google Scholar] [CrossRef]
- Acuna-Zegarra, M.A.; Diaz-Infante, S.; Baca-Carrasco, D.; Olmos-Liceaga, D. COVID-19 optimal vaccination policies: A modeling study on efficacy, natural and vaccine-induced immunity responses. Math. Biosci. 2021, 337, 108614. [Google Scholar] [CrossRef]
- Aruffo, E.; Yuan, P.; Tan, Y.; Gatov, E.; Moyles, I.; Belair, J.; Watmough, J.; Collier, S.; Arino, J.; Zhu, H. Mathematical modelling of vaccination rollout and NPIs lifting on COVID-19 transmission with VOC: A case study in Toronto, Canada. BMC Public Health 2022, 22, 1349. [Google Scholar] [CrossRef] [PubMed]
- Paul, A.K.; Kuddus, M.A. Mathematical analysis of a COVID-19 model with double dose vaccination in Bangladesh. Results Phys. 2022, 35, 105392. [Google Scholar] [CrossRef]
- Peter, O.J.; Panigoro, H.S.; Abidemi, A.; Ojo, M.M.; Oguntolu, F.A. Mathematical Model of COVID-19 Pandemic with Double Dose Vaccination. Acta Biotheor. 2023, 71, 9. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vaccine Types | Vaccine Efficacy (e) | Reference |
|---|---|---|
| RNA-based | 0.9572 | [8] |
| Non-replicating viral vector | 0.7103 | [8] |
| Inactivated virus | 0.8350 | [8] |
| Average | 0.8324 |
| Parameter | Value | Reference |
|---|---|---|
| 3000 individuals/day | Assumed | |
| 0.3235 | [31] | |
| 0.007117 | [14] | |
| Estimated | ||
| 0.09673 | [14] | |
| Estimated | ||
| 0.001069 | [14] | |
| 0.3 | [19] | |
| 0.0079 | [30] |
| Parameters | Sensitivity Index |
|---|---|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Intarapanya, T.; Suratanee, A.; Pattaradilokrat, S.; Plaimas, K. Modeling the Spread of COVID-19 with the Control of Mixed Vaccine Types during the Pandemic in Thailand. Trop. Med. Infect. Dis. 2023, 8, 175. https://doi.org/10.3390/tropicalmed8030175
Intarapanya T, Suratanee A, Pattaradilokrat S, Plaimas K. Modeling the Spread of COVID-19 with the Control of Mixed Vaccine Types during the Pandemic in Thailand. Tropical Medicine and Infectious Disease. 2023; 8(3):175. https://doi.org/10.3390/tropicalmed8030175
Chicago/Turabian StyleIntarapanya, Tanatorn, Apichat Suratanee, Sittiporn Pattaradilokrat, and Kitiporn Plaimas. 2023. "Modeling the Spread of COVID-19 with the Control of Mixed Vaccine Types during the Pandemic in Thailand" Tropical Medicine and Infectious Disease 8, no. 3: 175. https://doi.org/10.3390/tropicalmed8030175