


Liver Injury in Favipiravir-Treated COVID-19 Patients: Retrospective Single-Center Cohort Study


 , , , , and
, , , , and
Abstract
:1. Introduction
2. Research Design and Methods
2.1. Sample Size and Sample Selection
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographic Profile and General Information for All Patients under Study
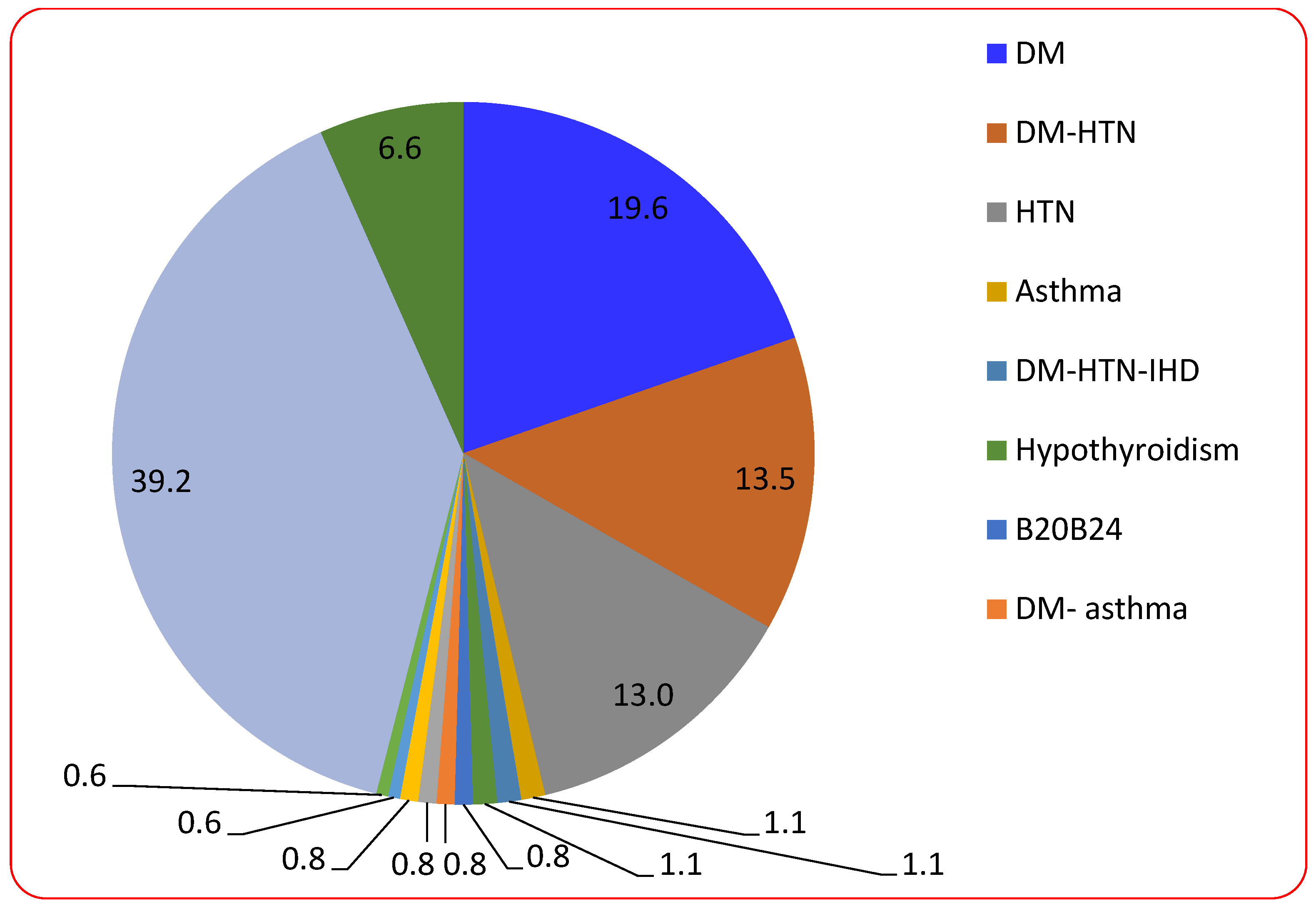
3.2. Description of Chronic Diseases of the Participating Patients
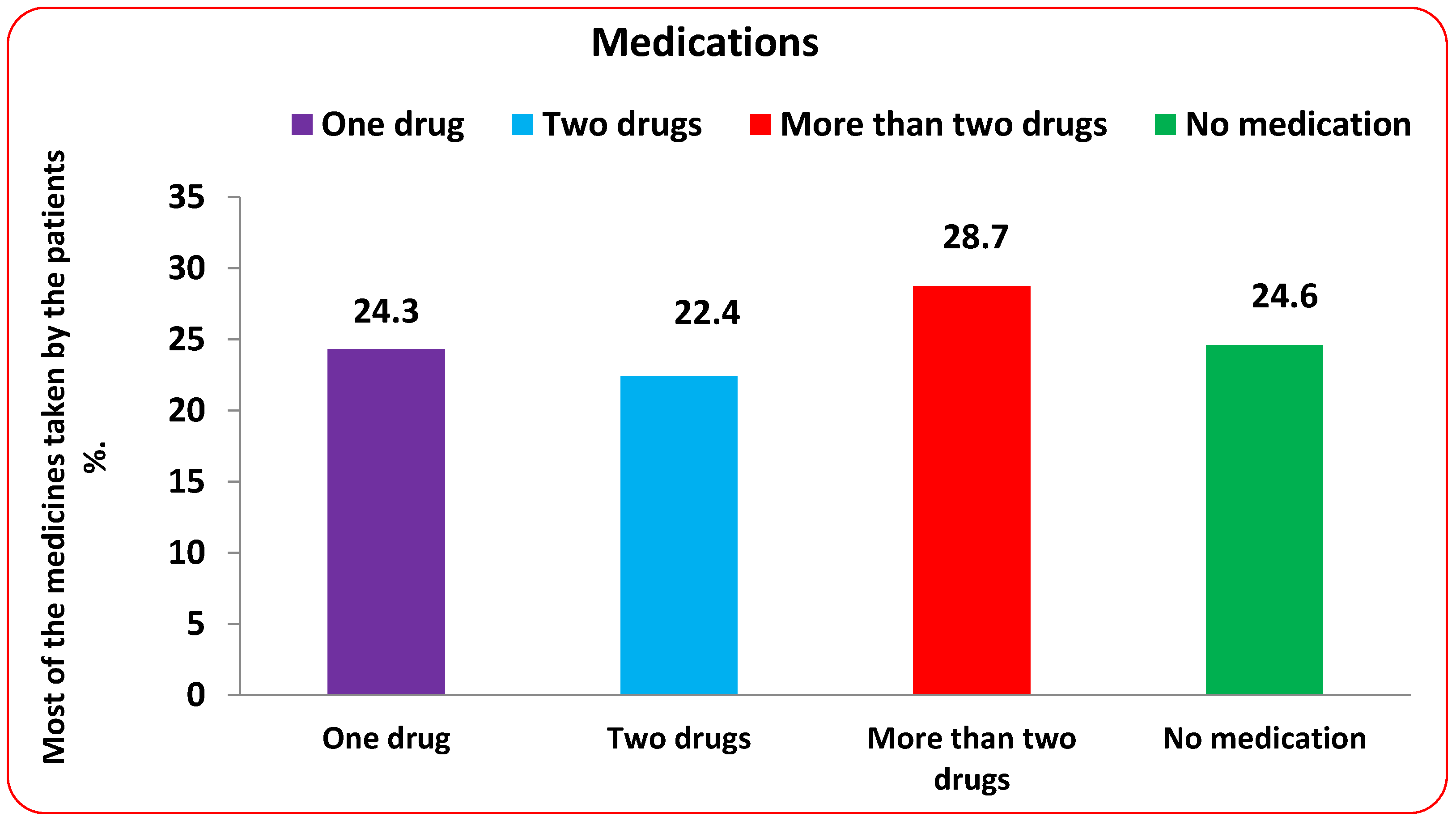
3.3. Most of the Medicines Are Taken by the Patients under Study
3.4. The Effect of Using Another Medication on Liver Enzymes
3.5. Comparison between Genders, Nationality, and Age Categories in Treated and Untreated with FPV
3.6. Pearson Correlation Coefficient between the Liver Functions (before and after FPV Treatment)
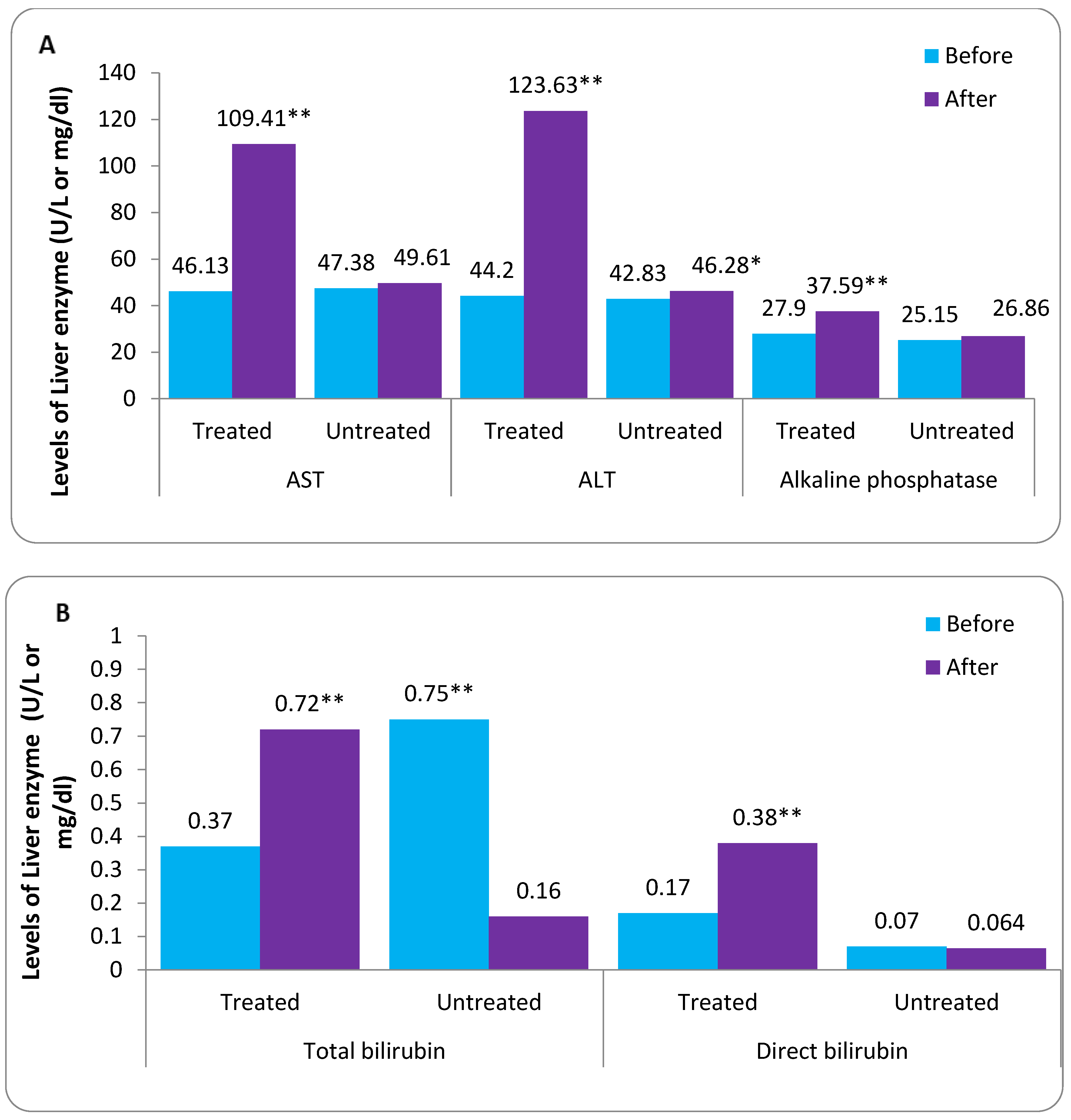
3.7. Comparison between before and after According to Treated and Untreated FPV Therapy
3.8. Comparison between Treated and Untreated after FPV Therapy
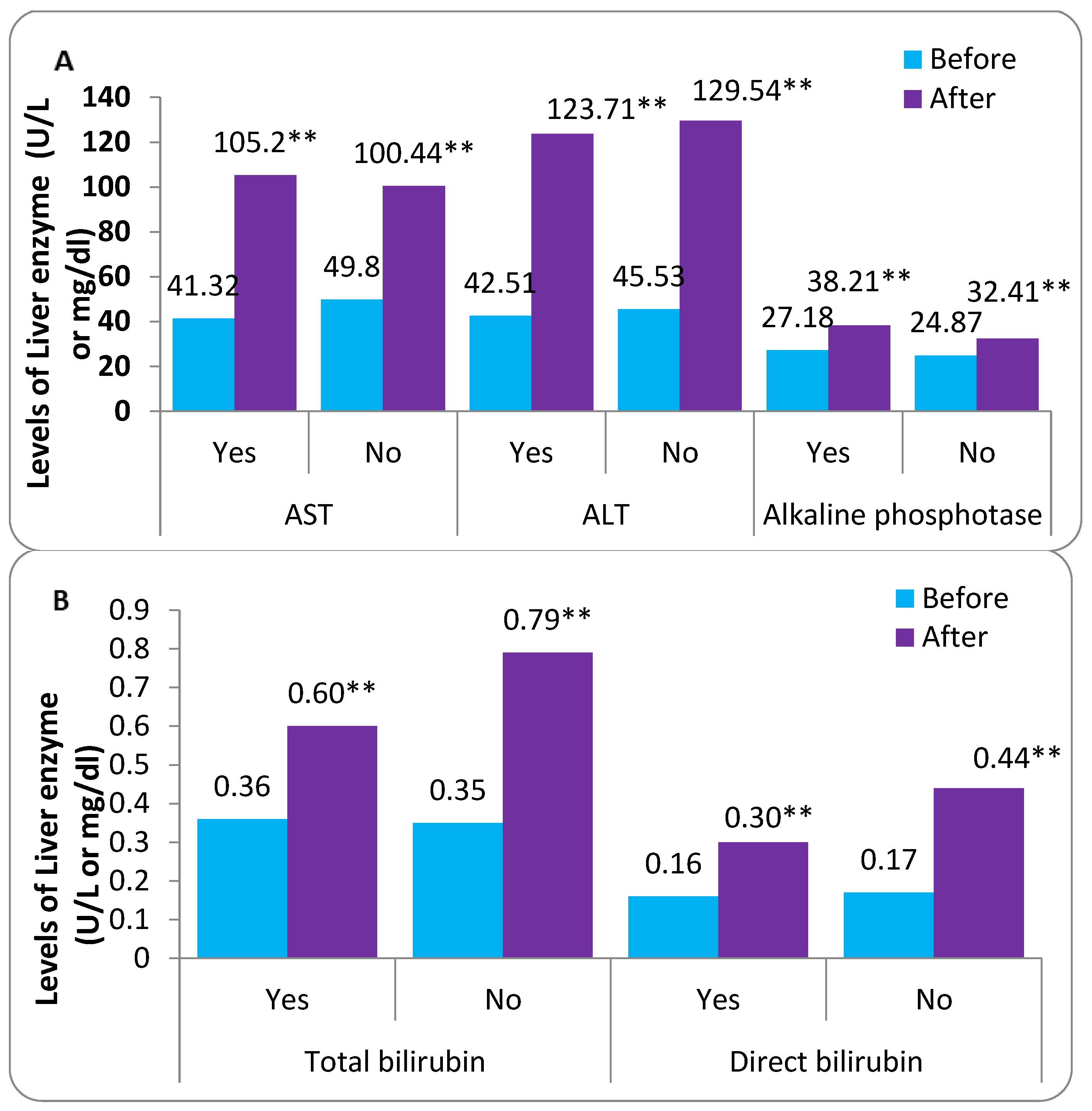
3.9. Comparison between Patients Who Were Treated with FVP Based on Chronic Disease
3.10. Comparison between Patients Treated and Untreated with FVP Based on Chronic Disease
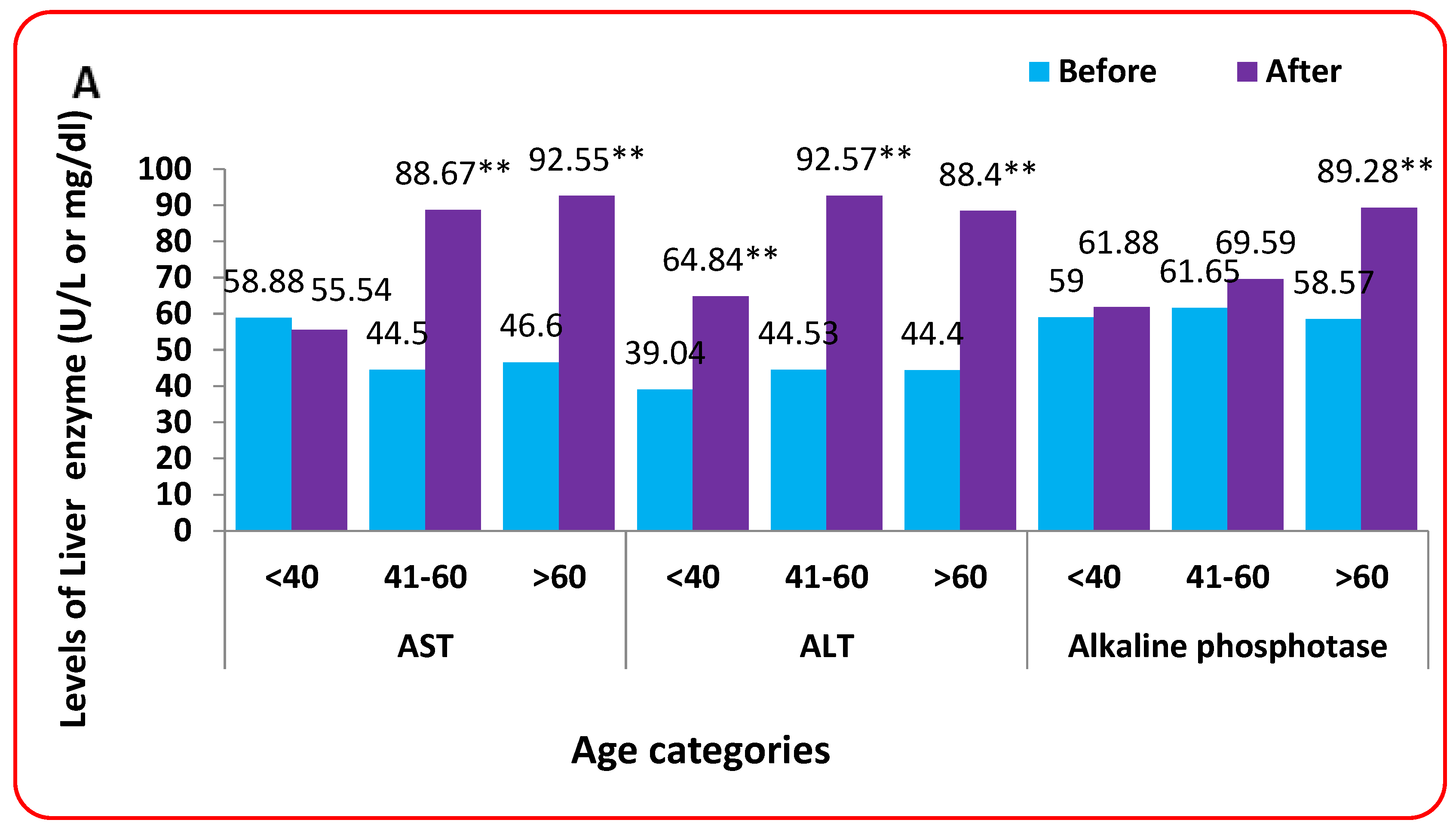
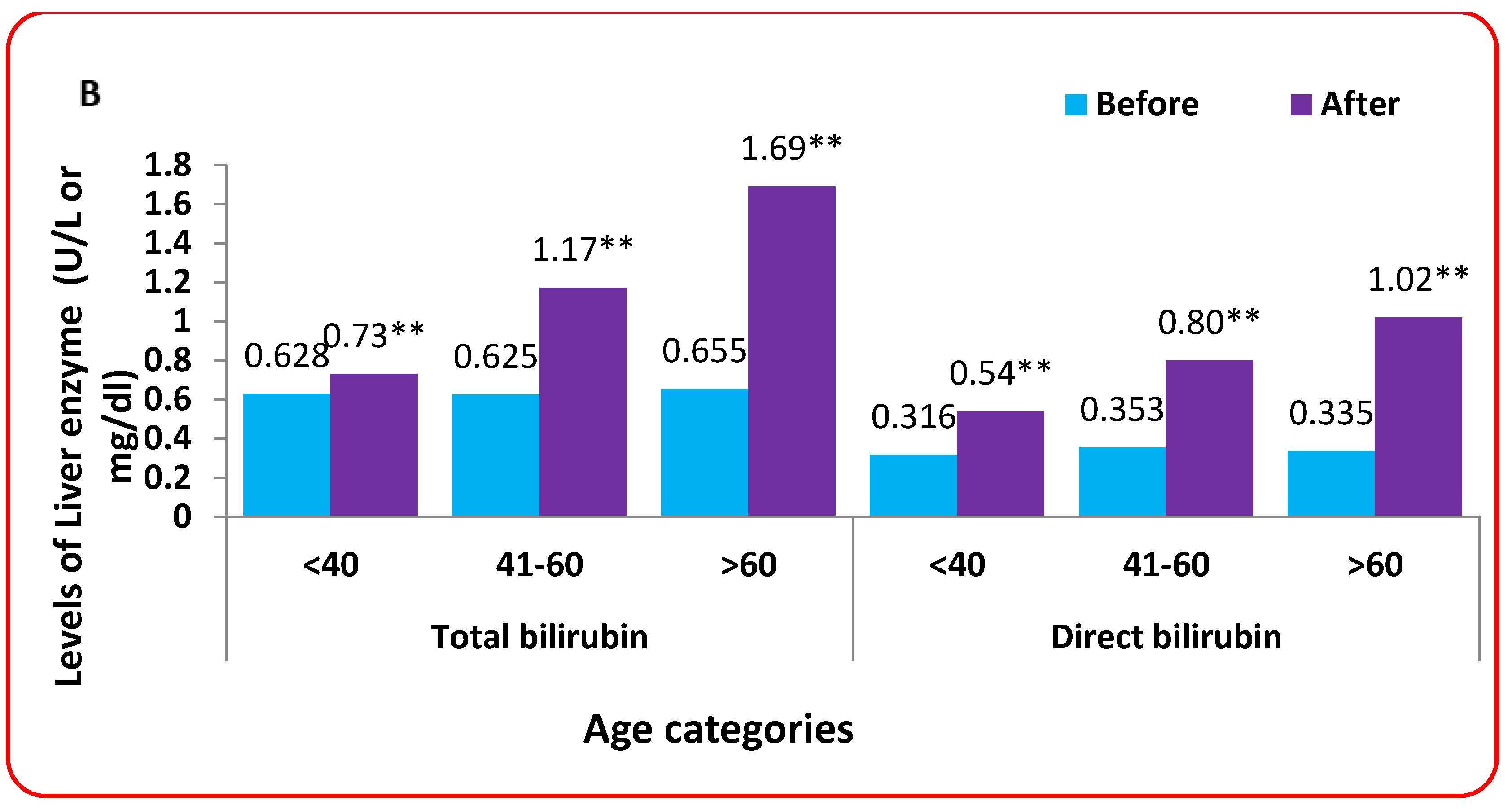
3.11. Effect of Age Categories on Liver Function
4. Discussion
5. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AST | aspartate transaminase |
| ADEs | adverse events |
| ALT | alanine transaminase |
| FVP | favipiravir |
| GGT | gamma-glutamyl transferase |
| ICU | intensive care unit |
References
- Sofi, M.S.; Hamid, A.; Bhat, S.U. SARS-CoV-2: A critical review of its history, pathogenesis, transmission, diagnosis and treatment. Biosaf. Health 2020, 2, 217–225. [Google Scholar] [CrossRef]
- Esakandari, H.; Nabi-Afjadi, M.; Fakkari-Afjadi, J.; Farahmandian, N.; Miresmaeili, S.-M.; Bahreini, E. A comprehensive review of COVID-19 characteristics. Biol. Proced. Online 2020, 22, 1–10. [Google Scholar] [CrossRef]
- W.H.O. Coronavirus Disease (COVID-19). Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 1 January 2020).
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef]
- da Rosa Mesquita, R.; Francelino Silva Junior, L.C.; Santos Santana, F.M.; Farias de Oliveira, T.; Campos Alcântara, R.; Monteiro Arnozo, G.; Rodrigues da Silva Filho, E.; Galdino dos Santos, A.G.; Oliveira da Cunha, E.J.; Salgueiro de Aquino, S.H. Clinical manifestations of COVID-19 in the general population: Systematic review. Wien. Klin. Wochenschr. 2021, 133, 377–382. [Google Scholar] [CrossRef]
- Lam, S.; Lombardi, A.; Ouanounou, A. COVID-19: A review of the proposed pharmacological treatments. Eur. J. Pharmacol. 2020, 886, 173451. [Google Scholar] [CrossRef]
- Agrawal, U.; Raju, R.; Udwadia, Z.F. Favipiravir: A new and emerging antiviral option in COVID-19. Med. J. Armed Forces India 2020, 76, 370–376. [Google Scholar] [CrossRef]
- Wu, R.; Wang, L.; Kuo, H.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating COVID-19. Curr Pharm. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef]
- Zhao, L.; Zhong, W. Mechanism of action of favipiravir against SARS-CoV-2: Mutagenesis or chain termination? Innov. 2021, 2, 100165. [Google Scholar] [CrossRef]
- Furuta, Y.; Gowen, B.B.; Takahashi, K.; Shiraki, K.; Smee, D.F.; Barnard, D.L. Favipiravir (T-705), a novel viral RNA polymerase inhibitor. Antivir. Res. 2013, 100, 446–454. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.X.; Chen, X.P. Favipiravir: Pharmacokinetics and concerns about clinical trials for 2019-nCoV infection. Clin. Pharmacol. Ther. 2020, 108, 242–247. [Google Scholar] [CrossRef] [Green Version]
- Kaur, R.J.; Charan, J.; Dutta, S.; Sharma, P.; Bhardwaj, P.; Sharma, P.; Lugova, H.; Krishnapillai, A.; Islam, S.; Haque, M. Favipiravir use in COVID-19: Analysis of suspected adverse drug events reported in the WHO database. Infect. Drug Resist. 2020, 13, 4427. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, S.M.; Farhadi, T.; Velayati, A.A. A review on favipiravir: The properties, function, and usefulness to treat COVID-19. Expert Rev. Anti-Infect. Ther. 2021, 19, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Saudi, C.; Creatinine, C.; LFTs, C.X. Saudi MoH Protocol for Patients Suspected of/Confirmed with COVID-19. Supportive care and antiviral treatment of suspected or confirmed COVID-19 infection. In Coronavirus Diseases 19 (COVID-19) Guidelines. July 31st, Version 2.1; Ministry of Health: Riyad, Saudia Arabia, 2020. [Google Scholar]
- Lv, Y.; Huang, Z. Account of Deep Learning-Based Ultrasonic Image Feature in the Diagnosis of Severe Sepsis Complicated with Acute Kidney Injury. Comput. Math Methods Med. 2022, 2022, 8158634. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Kulkarni, A.; Sharma, M.; Rao, P.N.; Reddy, D.N. Favipiravir-induced liver injury in patients with coronavirus disease 2019. J. Clin. Transl. Hepatol. 2021, 9, 276. [Google Scholar] [CrossRef]
- Hassanipour, S.; Arab-Zozani, M.; Amani, B.; Heidarzad, F.; Fathalipour, M.; Martinez-de-Hoyo, R. The efficacy and safety of Favipiravir in treatment of COVID-19: A systematic review and meta-analysis of clinical trials. Sci. Rep. 2021, 11, 11022. [Google Scholar] [CrossRef]
- Sodeifian, F.; Seyedalhosseini, Z.S.; Kian, N.; Eftekhari, M.; Najari, S.; Mirsaeidi, M.; Farsi, Y.; Nasiri, M.J. Drug-Induced Liver Injury in COVID-19 Patients: A Systematic Review. Front. Med. 2021, 8, 1624. [Google Scholar] [CrossRef]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, evaluation, and treatment of coronavirus (COVID-19). In Statpearls [Internet]; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Yamazaki, S.; Suzuki, T.; Sayama, M.; Nakada, T.A.; Igari, H.; Ishii, I. Suspected cholestatic liver injury induced by favipiravir in a patient with COVID-19. J. Infect. Chemother. 2021, 27, 390–392. [Google Scholar] [CrossRef]
- Al-Shammari, A.H.; Shahadha, M.A.A. The effect of Favipiravir on liver enzyme among patients with mild to moderate COVID-19 infection: A prospective cohort study. J. Popul. Ther. Clin. Pharmacol. 2022, 29, 46–54. [Google Scholar]
- Ou, S.M.; Lee, K.H.; Tsai, M.T.; Tseng, W.C.; Chu, Y.C.; Tarng, D.C. Artificial Intelligence for Risk Prediction of Rehospitalization with Acute Kidney Injury in Sepsis Survivors. J. Pers. Med. 2022, 12, 43. [Google Scholar] [CrossRef]
- Suh, J.I. Drug-induced liver injury. Yeungnam Univ. J. Med. 2020, 37, 2. [Google Scholar] [CrossRef]
- Carleton, H.M.; Haynes, F. Histological Technique; Oxford University Press: Oxford, UK, 1926; Volume 2. [Google Scholar]
- Ge, Z.-y.; Yang, L.-m.; Xia, J.-j.; Fu, X.-h.; Zhang, Y.-z. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J. Zhejiang Univ.-SCIENCE B 2020, 21, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cichoż-Lach, H.; Michalak, A. Liver injury in the era of COVID-19. World J Gastroenterol. 2021, 27, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, M.; Hamblin, M.R.; Rezaei, N. COVID-19: Transmission, prevention, and potential therapeutic opportunities. Clin. Chim. Acta 2020, 508, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Ghasemnejad-Berenji, M.; Pashapour, S. Favipiravir and COVID-19: A simplified summary. Drug Res. 2021, 71, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Nasir, M.; Perveen, R.; Murshed, M.; Nazneen, R.; Talha, K.A. Survival and biomarkers of COVID-19 patients treated with remdesivir and favipiravir in ICU during the peak of pandemic: A single center study in Bangladesh. J. Pharm. Res. Int. 2021, 32, 14–22. [Google Scholar] [CrossRef]
- Yang, R.X.; Zheng, R.D.; Fan, J.G. Etiology and management of liver injury in patients with COVID-19. World J. Gastroenterol. 2020, 26, 4753–4762. [Google Scholar] [CrossRef]
- Almoosa, Z.; Saad, M.; Qara, S.; Mustafa, M.; Mansour, A.; Alshab, D.; Alhashem, J.; Sajida, A.L.; Alkhalifah, S.; Mokhtar, A.L.; et al. Favipiravir versus standard of care in patients with severe COVID-19 infections: A retrospective comparative study. J. Infect. Public Health 2021, 14, 1247–1253. [Google Scholar] [CrossRef]
- Kawasuji, H.; Tsuji, Y.; Ogami, C.; Takegoshi, Y.; Kaneda, M.; Murai, Y.; Kimoto, K.; Ueno, A.; Miyajima, Y.; Fukui, Y.J.m. Association between high serum favipiravir concentrations and drug-induced liver injury. medRxiv 2021. [Google Scholar] [CrossRef]
- Lala, V.; Goyal, A.; Minter, D.A. Liver function tests. In StatPearls [Internet]; StatPearls Publishing: St. Petersburg, FL, USA, 2021. [Google Scholar]
- Marc, F.; Moldovan, C.; Hoza, A.; Restea, P.; Sachelarie, L.; Romila, L.E.; Suteu, C.; Farcas, D.M. Evaluation of hepatic biochemical parameters during antiviral treatment in COVID-19 patients. Biology 2021, 11, 13. [Google Scholar] [CrossRef]
- Alotaibi, M.; Ali, A.; Bakhshwin, D.; Alatawi, Y.; Alotaibi, S.; Alhifany, A.; Alharthi, B.; Alharthi, N.; Alyazidi, A.; Alharthi, Y.; et al. Effectiveness and Safety of Favipiravir Compared to Hydroxychloroquine for Management of Covid-19: A Retrospective Study. Int. J. Gen. Med. 2021, 14, 5597–5606. [Google Scholar] [CrossRef]
- Ara Perveen, R.; Nasir, M.; Murshed, M.M.; Naznin, R.; Ahmed, S.N. Remdesivir and Favipiravir Changes Hepato-Renal Profile in COVID-19 patients: A Cross Sectional Observation in Bangladesh. Int. J. Med. Sci. Clin. Invent. 2021, 8, 5196–5201. [Google Scholar] [CrossRef]
- Arshad, U.; Pertinez, H.; Box, H.; Tatham, L.; Rajoli, R.K.; Curley, P.; Neary, M.; Sharp, J.; Liptrott, N.J.; Valentijn, A.J.C.P.; et al. Prioritization of anti-SARS-Cov-2 drug repurposing opportunities based on plasma and target site concentrations derived from their established human pharmacokinetics. Clin. Pharmacol. Ther. 2020, 108, 775–790. [Google Scholar] [CrossRef] [PubMed]
- Tajiri, K.; Shimizu, Y. Liver physiology and liver diseases in the elderly. World J. Gastroenterol. 2013, 19, 8459. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K.; Samuel, K.; Vandeputte, M.; Hayes, P.C.; Plevris, J.N.J.P. SARS-CoV-2 infection and the liver. Pathogens 2020, 9, 430. [Google Scholar] [CrossRef]
- Zhang, C.; Shi, L.; Wang, F.-S. Liver injury in COVID-19: Management and challenges. Lancet Gastroenterol. Hepatol. 2020, 5, 428–430. [Google Scholar] [CrossRef]
- Cieslak, K.P.; Baur, O.; Verheij, J.; Bennink, R.J.; van Gulik, T.M. Liver function declines with increased age. Hpb 2016, 18, 691–696. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (N = 362) | % | |
|---|---|---|
| Gender | ||
| Male | 275 | 76.0% |
| Female | 87 | 24.0% |
| Nationality | ||
| Saudi | 98 | 27.1% |
| Non-Saudi | 264 | 72.9% |
| Age | ||
| ADULT < 40 | 66 | 18.2% |
| MIDDLE AGE 40–60 | 204 | 56.4% |
| ELDERLY > 60 | 92 | 25.4% |
| Mean (±SD) | 51.29 (±10.43) | |
| Min–Max | 24–67 | |
| Treated with FVP | ||
| Yes | 181 | 50.0% |
| No | 181 | 50.0% |
| Medication | Mean ± SD | Mode | Median | t | sig | |
|---|---|---|---|---|---|---|
| AST. B | Received drugs (n = 274) | 46.99 ± 27.35 | 45 | 43 | −1.086 | 0.278 |
| NA (n = 88) | 50.69 ± 28.88 | 32 | 41 | |||
| AST.A | Received drugs | 69.10 ± 93.51 | 50 | 50 | −1.935 | 0.054 |
| NA | 103.17 ± 240.16 | 29 | 44 | |||
| ALT.B | Received drugs | 42.47 ± 25.83 | 20 | 36 | −0.062 | 0.950 |
| NA | 42.67 ± 26.28 | 29 | 36 | |||
| ALT.A | Received drugs | 83.31 ± 163.69 | 35 | 54 | −0.336 | 0.737 |
| NA | 89.70 ± 121.23 | 28 | 51 | |||
| Alkaline phosphatase. B | Received drugs | 27.59 ± 40.41 | 63 | 63 | 0.915 | 0.361 |
| NA | 23.16 ± 35.76 | 58 | 58 | |||
| Alkaline phosphatase. A | Received drugs | 34.19 ± 49.04 | 63 | 64 | 1.411 | 0.159 |
| NA | 26.00 ± 40.49 | 8 | 61 | |||
| Total bilirubin.B | Received drugs | 0.66 ± 6.15 | 0.31 | 0.50 | 0.609 | 0.543 |
| NA | 0.25 ± 0.40 | 0.36 | 0.48 | |||
| Total bilirubin. A | Received drugs | 0.44 ± 0.96 | 0.45 | 0.46 | −0.128 | 0.898 |
| NA | 0.45 ± 1.12 | 0.49 | 0.52 | |||
| Directbilirubin. B | Received drugs | 0.13 ± 0.19 | 0.20 | 0.26 | 1.513 | 0.131 |
| NA | 0.09 ± 0.22 | 0.15 | 0.22 | |||
| Directbilirubin. A | Received drugs | 0.21 ± 0.54 | 0.21 | 0.26 | −0.414 | 0.679 |
| NA | 0.24 ± 0.74 | 0.13 | 0.25 |
| AST | ALT | Alkaline Phosphates | Total Bilirubin | Direct Bilirubin | ||
|---|---|---|---|---|---|---|
| AST | r | 1 | 0.440 ** | 0.106 | 0.075 | 0.240 ** |
| p-value | 0.0001 | 0.155 | 0.320 | 0.001 | ||
| ALT | r | 0.369 ** | 1 | 0.235 ** | 0.244 ** | 0.292 ** |
| p value | 0.000 | 0.002 | 0.001 | 0.000 | ||
| Alkaline phosphates | r | 0.899 | 0.286 | 1 | 0.187 * | 0.233 ** |
| p value | 0.009 | 0.080 | 0.012 | 0.002 | ||
| Total bilirubin | r | 0.259 ** | 0.116 | −0.023 | 1 | 0.526 ** |
| p value | 0.000 | 0.120 | 0.754 | 0.000 | ||
| Direct bilirubin | r | 0.325 ** | 0.129 | −0.073 | 0.891 ** | 1 |
| p value | 0.000 | 0.087 | 0.334 | 0.000 | ||
| Variables | Before | After | % Change | 95% Confidence Interval | Paired. t-Test | p Values | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| AST | Treated | 46.13 ± 4.49 | 109.41 ± 6.76 | 137.18% | −92.11 | 34.43 | 4.32 | <0.001 ** |
| Untreated | 47.38 ± 2.64 | 49.61 ± 3.58 | 4.71% | 0.34 | 8.11 | 1.15 | 0.132 ** | |
| ALT | Treated | 44.20 ± 5.21 | 123.63 ± 9.68 | 172% | −109.84 | −49.02 | 5.15 | <0.001 ** |
| Untreated | 42.83 ± 6.53 | 46.28 ± 7.81 | 8.05% | −9.14 | −1.75 | 1.61 | 0.061 * | |
| Alkaline phosphatase | Treated | 27.90 ± 4.29 | 37.59 ± 5.29 | 34.73% | −13.86 | −5.52 | 4.58 | <0.001 ** |
| Untreated | 25.15 ± 6.42 | 26.86 ± 8.29 | 6.80% | −2.81 | −0.59 | 1.24 | 0.360 | |
| Total bilirubin | Treated | 0.37 ± 0.33 | 0.72 ± 0.37 | 94.59% | −0.54 | −0.17 | 3.83 | <0.001 ** |
| Untreated | 0.75 ± 0.51 | 0.16 ± 0.15 | 78.67% | −0.52 | 1.69 | 1.05 | 0.295 | |
| Direct bilirubin | Treated | 0.17 ± 0.21 | 0.38 ± 0.24 | 123.53% | −0.32 | −0.11 | 4.03 | <0.001 ** |
| Untreated | 0.07 ± 0.01 | 0.064 ± 0.11 | 8.57% | −0.001 | 0.02 | 1.73 | 0.085 | |
| Variables | Untreated | Treated | % Change | 95% Confidence Interval | Unpaired t-Test | p Values | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| AST (5–34 U/L) | 45.38 ± 7.24 | 109.41 ± 6.76 | 141.1% | 35.02 | 93.01 | 4.34 | <0.001 ** |
| ALT (5–55 U/L) | 46.28 ± 7.81 | 123.63 ± 9.68 | 167.13% | 46.36 | 108.32 | 4.91 | <0.001 ** |
| Alkaline phosphatase (40–150 U/L) | 26.86 ± 8.29 | 37.59 ± 5.29 | 39.95% | 1.01 | 20.45 | 2.17 | 0.031 ** |
| Total bilirubin (0.2–1.2 mg/dL) | 0.16 ± 0.15 | 0.72 ± 0.37 | 350.0% | 0.36 | 0.76 | 5.57 | <0.001 ** |
| Direct bilirubin (0.1 to 1.2 mg/dL) | 0.24 ± 0.11 | 0.38 ± 0.24 | 58.33% | 0.19 | 0.43 | 5.22 | <0.001 ** |
| Parameters | Chronic Disease | Before (n = 181) | After (n = 181) | t-Test | Sig |
|---|---|---|---|---|---|
| AST (5–34 U/L) | Yes (n = 222) | 45.11 | 76.11 | 2.87 | 0.004 ** |
| No (n = 140) | 50.34 | 71.25 | 2.901 | 0.004 ** | |
| t-test | 2.44 | 0.65 | |||
| Sig | 0.015 ** | 0.948 | |||
| ALT (5–55 U/L) | Yes | 42.45 | 85.52 | 3.53 | <0.001 ** |
| No | 42.18 | 86.63 | 5.975 | <0.001 ** | |
| t-test | 0.05 | 0.260 | |||
| Sig | 0.956 | 0.795 | |||
| Alkaline phosphatase (40–150 U/L) | Yes | 27.54 | 34.24 | 4.18 | <0.001 ** |
| No | 22.99 | 27.13 | 3.075 | 0.003 ** | |
| t-test | 1.167 | 1.45 | |||
| Sig | 0.550 | 0.421 | |||
| Total bilirubin (0.2–1.2 mg/dL) | Yes | 0.76 | 0.39 | 0.763 | 0.04 ** |
| No | 0.26 | 0.46 | 2.31 | 0.023 ** | |
| t-test | 0.842 | 1.141 | |||
| Sig | 0.400 | 0.842 | |||
| Direct bilirubin (0.1 to 1.2) | Yes | 0.13 | 0.19 | 2.454 | 0.015 ** |
| No | 0.11 | 0.24 | 2.861 | <0.001 ** | |
| t-test | 0.843 | 1.16 | |||
| Sig | 0.400 | 0.247 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almutairi, A.O.; El-Readi, M.Z.; Althubiti, M.; Alhindi, Y.Z.; Ayoub, N.; Alzahrani, A.R.; Al-Ghamdi, S.S.; Eid, S.Y. Liver Injury in Favipiravir-Treated COVID-19 Patients: Retrospective Single-Center Cohort Study. Trop. Med. Infect. Dis. 2023, 8, 129. https://doi.org/10.3390/tropicalmed8020129
Almutairi AO, El-Readi MZ, Althubiti M, Alhindi YZ, Ayoub N, Alzahrani AR, Al-Ghamdi SS, Eid SY. Liver Injury in Favipiravir-Treated COVID-19 Patients: Retrospective Single-Center Cohort Study. Tropical Medicine and Infectious Disease. 2023; 8(2):129. https://doi.org/10.3390/tropicalmed8020129
Chicago/Turabian StyleAlmutairi, Amal Oweid, Mahmoud Zaki El-Readi, Mohammad Althubiti, Yosra Zakariyya Alhindi, Nahla Ayoub, Abdullah R. Alzahrani, Saeed S. Al-Ghamdi, and Safaa Yehia Eid. 2023. "Liver Injury in Favipiravir-Treated COVID-19 Patients: Retrospective Single-Center Cohort Study" Tropical Medicine and Infectious Disease 8, no. 2: 129. https://doi.org/10.3390/tropicalmed8020129