
Weak Adoption and Performance of Hepatitis B Birth-Dose Vaccination Programs in Africa: Time to Consider Systems Complexity?—A Scoping Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives of the Review
- To describe current knowledge on the risk of HBV MTCT in the WHO Africa region;
- To describe the status of HBV MTCT mitigation strategies including hepatitis B birth-dose vaccination programs;
- To explore health systems’ capacity to support hepatitis B birth-dose vaccination programs in the WHO Africa region.
2.2. Methods
3. Results
3.1. Current Knowledge on the Risk of HBV MTCT in the WHO Africa Region
3.1.1. Growing Evidence on the Risk of HBV MTCT

3.1.2. HIV–HBV Co-Infection and the Increased Risk of HBV MTCT

| Study No. | Author, Year | Setting | Study Design | Study Period | Population and Population Size | Summary of Key Findings |
|---|---|---|---|---|---|---|
| 1 | Rashid et al., 2014 [12] | Tanzania | Cross-sectional | August–September 2010 | 310 Pregnant women |
|
| 2 | Bayo et al., 2014 [10] | Uganda | Cross-sectional | September 2012–January 2013 | 397 Pregnant women |
|
| 3 | Howell et al., 2014 [5] | Sub-Saharan Africa | Literature Review | Publications between 1995–2013 | 60,177 Pregnant women and women of childbearing age |
|
| 528 Mother–child pairs |
| |||||
| 4 | Sadoh et al., 2014 [6] | Nigeria | Literature Review | Period not specified. References range from 1988–2013 | Pregnant women and women of childbearing age |
|
| Mother–child pairs (Size of population not consistently reported) |
| |||||
| 5 | Umare et al., 2016 [9] | Ethiopia | Cross-sectional | March–May 2015 | 338 Pregnant women |
|
| 6 | Breakwell et al., 2017 [2] | WHO AFRO | Literature review | January 1995–October 2016 | Median range 269–2244 Pregnant women across 75 studies |
|
| WHO/UNICEF Monitoring data updated to year 2016 | 143 Mother–child pairs |
| ||||
| 7 | Chotun et al., 2017 [15] | South Africa | Prospective cohort | June–November 2014 | 134 Pregnant women |
|
| 4 Infants |
| |||||
| 8 | Kirbak et al., 2017 [11] | South Sudan | Cross-sectional | December 2012–March 2013 | 280 Pregnant women |
|
| 9 | Seremba et al., 2017 [49] | Uganda | Cross-sectional | July 2012–June 2014 | 612 Mothers |
|
| 606 Infants |
| |||||
| 10 | Sone et al., 2017 [7] | Cameroon | Prospective cross-sectional | 10-month period, year not specified. | 298 Pregnant women |
|
| Ethical clearance given in 2014 | 20 Infants |
| ||||
| 11 | Bittaye et al., 2019 [8] | The Gambia | Cross-sectional | May–July 2015 | 424 Pregnant women |
|
| 12 | Guingané et al., 2020 [13] | Burkina Faso | Prospective cohort | October 2014–February 2016 | 1580 Pregnant women |
|
| 40 Infants |
| |||||
| 13 | Thompson et al., 2021 [14] | Democratic Republic of Congo | Cohort | September 2018–February 2019 | 4016 Pregnant women |
|
| 88 Infants |
|
3.2. Status of HBV MTCT Mitigation Strategies in the WHO Africa Region
3.2.1. Barriers to Adopting Universal Hepatitis B Birth-Dose Vaccination Programs
3.2.2. Challenges Faced by Established Hepatitis B Birth-Dose Vaccination Programs
3.2.3. Poor Adherence to Timely Hepatitis B Birth-Dose Vaccination
3.3. Health Systems’ Capacity to Support Hepatitis B Birth-Dose Vaccination Programs in the WHO Africa Region
3.3.1. Conceptual Models for the Assessment of Health Systems’ Capacity
3.3.2. Complexity as a Characteristic of Hepatitis B Birth-Dose Vaccination Programs
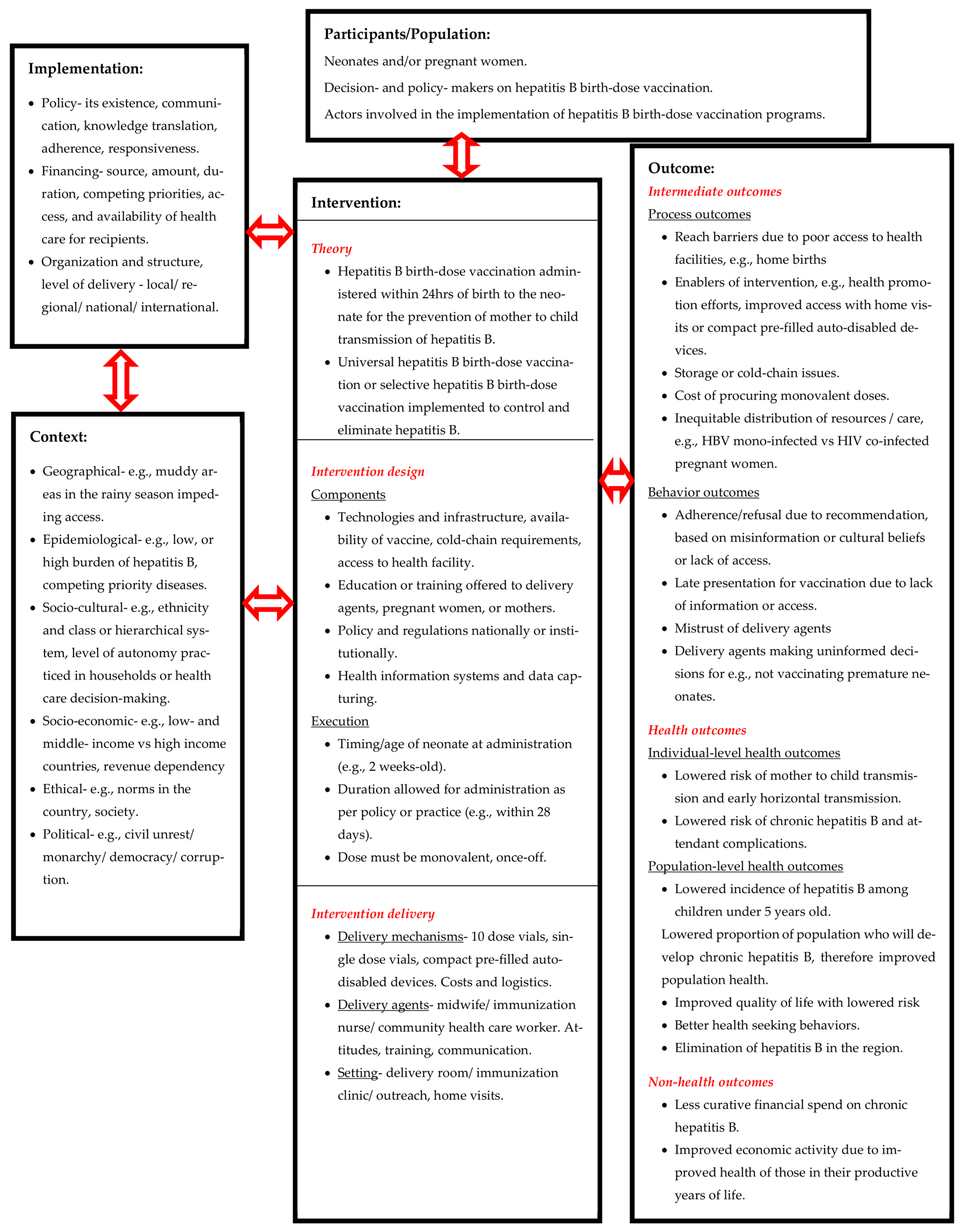
3.3.3. A Systems-Based Logic Model for Assessing Complexity within Hepatitis B Birth-Dose Vaccination Programs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Section | Item | PRISMA-ScR checklist item | Page number |
| Title | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1–21 |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 1–3 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 2–3 |
| Methods | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | N/A |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 3 |
| Information sources | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 3 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | 1–2 (Table S1) |
| Selection of sources of evidence | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 3 |
| Data charting process | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 3 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 3 |
| Critical appraisal of individual sources of evidence | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | N/A |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 3 |
| Results | |||
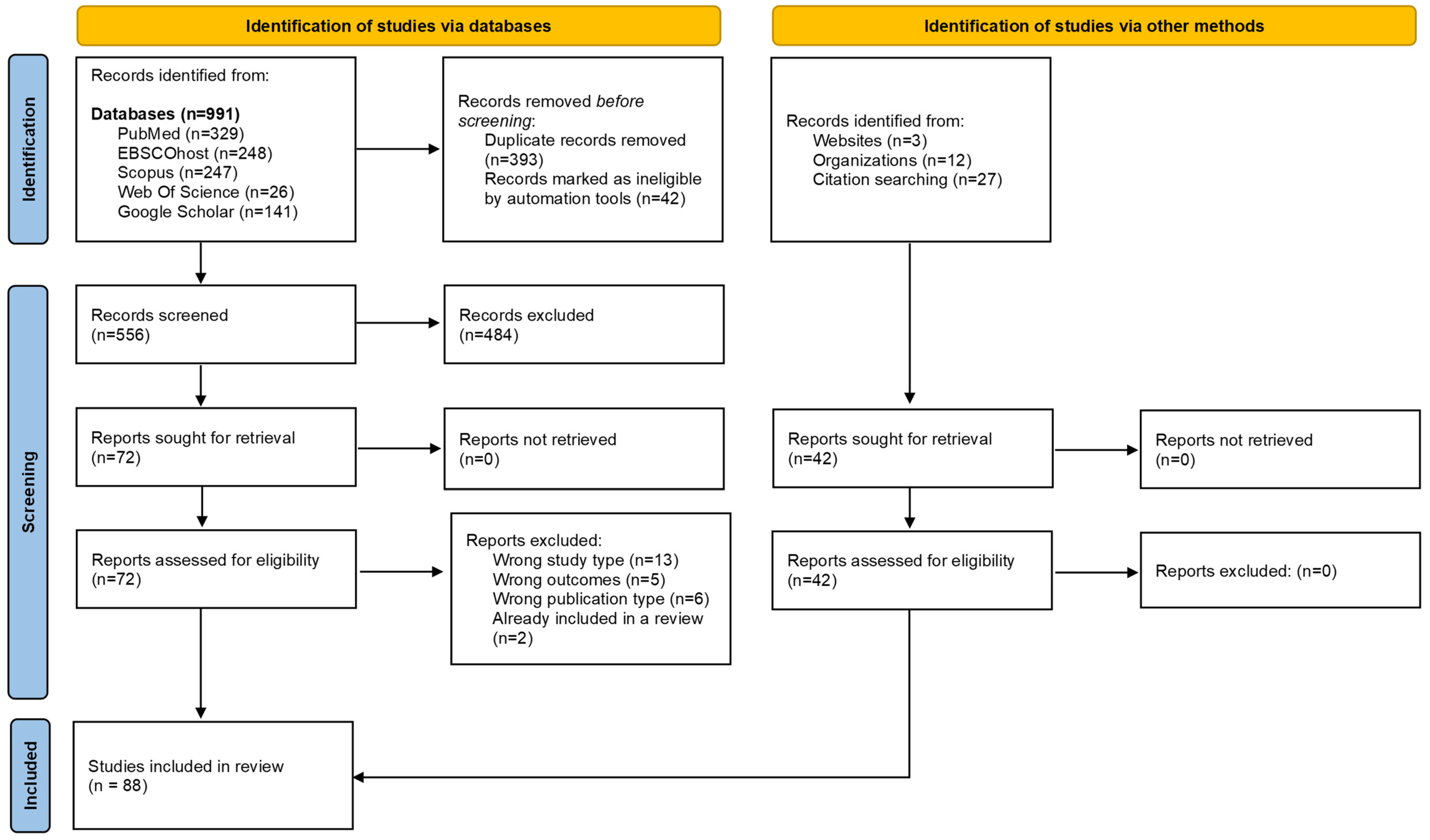
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 5 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 7–8 &3–19 (Table S2) |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | N/A |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 3–18 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 3–18 |
| Discussion | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 20–21 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 21 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 21 |
| Funding | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 21 |
References
- Dionne-Odom, J.; Njei, B.; Tita, A. Elimination of Vertical Transmission of Hepatitis B in Africa: A Review of Available Tools and New Opportunities. Clin. Ther. 2018, 40, 1255–1267. [Google Scholar] [CrossRef]
- Breakwell, L.; Tevi-Benissan, C.; Childs, L.; Mihigo, R.; Tohme, R. The Status of Hepatitis B Control in the African Region. Pan Afr. Med. J. 2017, 27, 17. [Google Scholar] [CrossRef]
- Tamandjou Tchuem, C.R.; Andersson, M.I.; Wiysonge, C.S.; Mufenda, J.; Preiser, W.; Cleary, S. Prevention of Hepatitis B Mother-to-Child Transmission in Namibia: A Cost-Effectiveness Analysis. Vaccine 2021, 39, 3141–3151. [Google Scholar] [CrossRef]
- Chotun, N.; Nel, E.; Cotton, M.F.; Preiser, W.; Andersson, M.I. Hepatitis B Virus Infection in HIV-Exposed Infants in the Western Cape, South Africa. Vaccine 2015, 33, 4618–4622. [Google Scholar] [CrossRef]
- Howell, J.; Lemoine, M.; Thursz, M. Prevention of Materno-Foetal Transmission of Hepatitis B in Sub-Saharan Africa: The Evidence, Current Practice and Future Challenges. J. Viral Hepat. 2014, 21, 381–396. [Google Scholar] [CrossRef]
- Sadoh, A.; Sadoh, W. Does Nigeria Need the Birth Dose of the Hepatitis B Vaccine? Niger. J. Paediatr. 2014, 41, 104–109. [Google Scholar] [CrossRef]
- Sone, L.; Voufo, R.; Dimodi, H.; Kengne, M.; Gueguim, C.; Nnanga, N.; Oben, J.; Ngondi, J. Prevalence and Identification of Serum Markers Associated with Vertical Transmission of Hepatitis B in Pregnant Women in Yaounde, Cameroon. Int. J. MCH AIDS 2017, 6, 69–74. [Google Scholar] [CrossRef]
- Bittaye, M.; Idoko, P.; Ekele, B.A.; Obed, S.A.; Nyan, O. Hepatitis B Virus Sero-Prevalence amongst Pregnant Women in the Gambia. BMC Infect. Dis. 2019, 19, 259. [Google Scholar] [CrossRef]
- Umare, A.; Seyoum, B.; Gobena, T.; Haile Mariyam, T. Hepatitis B Virus Infections and Associated Factors among Pregnant Women Attending Antenatal Care Clinic at Deder Hospital, Eastern Ethiopia. PLoS ONE 2016, 11, e0166936. [Google Scholar] [CrossRef]
- Bayo, P.; Ochola, E.; Oleo, C.; Mwaka, A.D. High Prevalence of Hepatitis B Virus Infection among Pregnant Women Attending Antenatal Care: A Cross-Sectional Study in Two Hospitals in Northern Uganda. BMJ Open 2014, 4, e005889. [Google Scholar] [CrossRef]
- Kirbak, A.L.S.; Ng’ang’a, Z.; Omolo, J.; Idris, H.; Usman, A.; Mbabazi, W.B. Sero-Prevalence for Hepatitis B Virus among Pregnant Women Attending Antenatal Clinic in Juba Teaching Hospital, Republic of South Sudan. Pan Afr. Med. J. 2017, 26, 72. [Google Scholar] [CrossRef] [PubMed]
- Rashid, S.; Kilewo, C.; Aboud, S. Seroprevalence of Hepatitis B Virus Infection among Antenatal Clinic Attendees at a Tertiary Hospital in Dar Es Salaam, Tanzania. Tanzan. J. Health Res. 2014, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guingané, A.N.; Bougouma, A.; Sombié, R.; King, R.; Nagot, N.; Meda, N.; Van de Perre, P.; Tuaillon, E. Identifying Gaps across the Cascade of Care for the Prevention of HBV Mother-to-child Transmission in Burkina Faso: Findings from the Real World. Liver Int. 2020, 40, 2367–2376. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.; Morgan, C.E.; Ngimbi, P.; Mwandagalirwa, K.; Ravelomanana, N.L.R.; Tabala, M.; Fathy, M.; Kawende, B.; Muwonga, J.; Misingi, P.; et al. Arresting Vertical Transmission of Hepatitis B Virus (AVERT-HBV) in Pregnant Women and Their Neonates in the Democratic Republic of the Congo: A Feasibility Study. Lancet Glob. Health 2021, 9, e1600–e1609. [Google Scholar] [CrossRef] [PubMed]
- Chotun, N.; Preiser, W.; van Rensburg, C.J.; Fernandez, P.; Theron, G.B.; Glebe, D.; Andersson, M.I. Point-of-Care Screening for Hepatitis B Virus Infection in Pregnant Women at an Antenatal Clinic: A South African Experience. PLoS ONE 2017, 12, e0181267. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization; Annex, W. 1. Key Data at a Glance. In Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- United Nations Children’s Fund Global and Regional Trends. Available online: https://data.unicef.org/topic/hivaids/global-regional-trends/ (accessed on 15 August 2023).
- Andersson, M.I.; Maponga, T.G.; Ijaz, S.; Barnes, J.; Theron, G.B.; Meredith, S.A.; Preiser, W.; Tedder, R.S. The Epidemiology of Hepatitis B Virus Infection in HIV-Infected and HIV-Uninfected Pregnant Women in the Western Cape, South Africa. Vaccine 2013, 31, 5579–5584. [Google Scholar] [CrossRef]
- Maponga, T.G.; Matteau Matsha, R.; Morin, S.; Scheibe, A.; Swan, T.; Andrieux-Meyer, I.; Spearman, C.W.; Klein, M.B.; Rockstroh, J.K. Highlights from the 3rd International HIV/Viral Hepatitis Co-Infection Meeting-HIV/Viral Hepatitis: Improving Diagnosis, Antiviral Therapy and Access. Hepatol. Med. Policy 2017, 2, 8. [Google Scholar] [CrossRef]
- United Nations Children’s Fund Immunization Coverage Estimates Data Visualization. Available online: https://data.unicef.org/resources/immunization-coverage-estimates-data-visualization/ (accessed on 15 August 2023).
- Anderson, S.; Harper, L.M.; Dionne-Odom, J.; Halle-Ekane, G.; Tita, A.T.N.; Dionne-Odom, J.; Halle-Ekane, G. A Decision Analytic Model for Prevention of Hepatitis B Virus Infection in Sub-Saharan Africa Using Birth-Dose Vaccination. Int. J. Gynecol. Obstet. 2018, 141, 126–132. [Google Scholar] [CrossRef]
- Diale, Q.; Pattinson, R.; Chokoe, R.; Masenyetse, L.; Mayaphi, S. Antenatal Screening for Hepatitis B Virus in HIV-Infected and Uninfected Pregnant Women in the Tshwane District of South Africa. S. Afr. Med. J. 2016, 106, 97–100. [Google Scholar] [CrossRef]
- World Health Organization. Hepatitis B Vaccines: WHO Position Paper, July 2017—Recommendations. Vaccine 2019, 37, 223–225. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016; ISBN 9789241503501. [Google Scholar]
- de Villiers, M.J.; Nayagam, S.; Hallett, T.B. The Impact of the Timely Birth Dose Vaccine on the Global Elimination of Hepatitis B. Nat. Commun. 2021, 12, 6223. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 15 August 2022).
- World Health Organization Regional Office for Africa. Prevention, Care and Treatment of Viral Hepatitis in the African Region: Framework for Action, 2016–2020; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Kabore, J. Hepatitis B Birth Dose (HepB BD) Vaccination in the WHO African Region. In Proceedings of the Building a Community of Practice to Assist hepB Birth Dose Introduction in African Countries, Online, 17–18 March 2021; Coalition for Global Hepatitis Elimination: Decatur, GA, USA, 2021. [Google Scholar]
- Njuguna, H. HepB-BD and Infant HepB3 Coverage Status in Africa. In Proceedings of the Hepatitis B Birth Dose in the African Region: Bridging Ccience and Advocacy to Eliminate Mother-to-Child Transmission of HBV, Online, 22 August 2022. [Google Scholar]
- Mounier-Jack, S.; Griffiths, U.K.; Closser, S.; Burchett, H.; Marchal, B. Measuring the Health Systems Impact of Disease Control Programmes: A Critical Reflection on the WHO Building Blocks Framework. BMC Public Health 2014, 14, 278. [Google Scholar] [CrossRef] [PubMed]
- Travis, P.; Bennet, S.; Haines, A.; Pang, T.; Bhutta, Z.; Hyder, A.; Pielemeier, N.; Mills, A.; Evans, T. Overcoming Health-Systems Constraints to Achieve the Millenium Development Goals. Lancet 2004, 364, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Shiell, A.; Hawe, P.; Gold, L. Complex Interventions or Complex Systems? Implications for Health Economic Evaluation. BMJ 2008, 336, 1281. [Google Scholar] [CrossRef]
- de Savigny, D.; Adam, T. (Eds.) Systems Thinking for Health Systems Strengthening; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Langlois, E.V.; Daniels, K.; Akl, E.A. (Eds.) Evidence Synthesis for Health Policy and System: A Method Guide; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241514552. [Google Scholar]
- Petticrew, M. When Are Complex Interventions “Complex”? When Are Simple Interventions “Simple”? Eur. J. Public Health 2011, 21, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Mitchie, S.; Nazareth, I.; Petticrew, M. Developing and Evaluating Complex Interventions: The New Medical Research Council Guidance. BMJ 2008, 337, 979–983. [Google Scholar] [CrossRef]
- Petticrew, M.; Anderson, L.; Elder, R.; Grimshaw, J.; Hopkins, D.; Hahn, R.; Krause, L.; Kristjansson, E.; Mercer, S.; Sipe, T.; et al. Complex Interventions and Their Implications for Systematic Reviews: A Pragmatic Approach. J. Clin. Epidemiol. 2013, 66, 1209–1214. [Google Scholar] [CrossRef]
- Hawe, P.; Shiell, A.; Riley, T. Theorising Interventions as Events in Systems. Am. J. Community Psychol. 2009, 43, 267–276. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. (Eds.) JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020; ISBN 978-0-6488488-0-6. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Reiswig, J. Mendeley. J. Med. Libr. Assoc. 2010, 98, 193–194. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Bottomley, C.; Njie, R.; Mendy, M. The Association between Maternal Hepatitis B e Antigen Status, as a Proxy for Perinatal Transmission, and the Risk of Hepatitis B e Antigenaemia in Gambian Children. BMC Public Health 2014, 14, 532. [Google Scholar] [CrossRef] [PubMed]
- Keane, E.; Funk, A.L.; Shimakawa, Y. Systematic Review with Meta-Analysis: The Risk of Mother-to-Child Transmission of Hepatitis B Virus Infection in Sub-Saharan Africa. Aliment. Pharmacol. Ther. 2016, 44, 1005–1017. [Google Scholar] [CrossRef]
- Ekra, D.; Herbinger, K.-H.; Konate, S.; Leblond, A.; Fretz, C.; Cilote, V.; Douai, C.; Da Silva, A.; Gessner, B.D.; Chauvin, P. A Non-Randomized Vaccine Effectiveness Trial of Accelerated Infant Hepatitis B Immunization Schedules with a First Dose at Birth or Age 6 Weeks in Côte d’Ivoire. Vaccine 2008, 26, 2753–2761. [Google Scholar] [CrossRef] [PubMed]
- Tamandjou Tchuem, C.R.; Maponga, T.G.; Chotun, N.; Preiser, W.; Andersson, M.I. Is Hepatitis B Birth Dose Vaccine Needed in Africa? Pan Afr. Med. J. 2017, 27, 18. [Google Scholar] [CrossRef]
- World Health Organization. Global Compliance with Hepatitis B Vaccine Birth Dose and Factors Related to Timely Schedule. A Review; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Seremba, E.; Van Geertruyden, J.P.; Ssenyonga, R.; Opio, C.K.; Kaducu, J.M.; Sempa, J.B.; Colebunders, R.; Ocama, P. Early Childhood Transmission of Hepatitis B Prior to the First Hepatitis B Vaccine Dose Is Rare among Babies Born to HIV-Infected and Non-HIV Infected Mothers in Gulu, Uganda. Vaccine 2017, 35, 2937–2942. [Google Scholar] [CrossRef]
- Ott, J.J.; Stevens, G.A.; Groeger, J.; Wiersma, S.T. Global Epidemiology of Hepatitis B Virus Infection: New Estimates of Age-Specific HBsAg Seroprevalence and Endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Platt, L.; French, C.E.; McGowan, C.R.; Sabin, K.; Gower, E.; Trickey, A.; McDonald, B.; Ong, J.; Stone, J.; Easterbrook, P.; et al. Prevalence and Burden of HBV Co-infection among People Living with HIV: A Global Systematic Review and Meta-analysis. J. Viral Hepat. 2020, 27, 294–315. [Google Scholar] [CrossRef]
- Sichone, V.; Vwalika, B. Prevalence of Hepatitis B Virus, HIV and HBV Coinfection and Associated Factors in Pregnant Women Attending Antenatal Care at the University Teaching Hospital, Lusaka, Zambia. Med. J. Zamb. 2019, 46, 10–18. [Google Scholar] [CrossRef]
- Gueye, S.; Diop-Ndiaye, H.; Lo, G.; Guindo, I.; Dia, A.; Sow-Sall, A.; Gaye-Diallo, A.; Mboup, S.; Toure-Kane, C. HBV Carriage in Children Born From HIV-Seropositive Mothers in Senegal: The Need of Birth-Dose HBV Vaccination. J. Med. Virol. 2016, 88, 815–819. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy; World Health Organization: Geneva, Switzerland, 2020; ISBN 9789240002708.
- Terrault, N.A.; Bzowej, N.H.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H. AASLD Guidelines for Treatment of Chronic Hepatitis B. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef] [PubMed]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.A.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the Management of Hepatitis B Virus Infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed]
- Jooste, P.; van Zyl, A.; Adland, E.; Daniels, S.; Hattingh, L.; Brits, A.; Wareing, S.; Goedhals, D.; Jeffery, K.; Andersson, M.; et al. Screening, Characterisation and Prevention of Hepatitis B Virus (HBV) Co-Infection in HIV-Positive Children in South Africa. J. Clin. Virol. 2016, 85, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Hipgrave, D.B.; Maynard, J.E.; Biggs, B.-A. Improving Birth Dose Coverage of Hepatitis B Vaccine. Bull. World Health Organ. 2006, 84, 65–71. [Google Scholar] [CrossRef]
- Dadari, I.K.; Zgibor, J.C. How the Use of Vaccines Outside the Cold Chain or in Controlled Temperature Chain Contributes to Improving Immunization Coverage in Low- and Middle-Income Countries (LMICs): A Scoping Review of the Literature. J. Glob. Health 2021, 11, 4004. [Google Scholar] [CrossRef]
- Bassoum, O.; Kimura, M.; Dia, A.T.; Lemoine, M.; Shimakawa, Y. Coverage and Timeliness of Birth Dose Vaccination in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Vaccines 2020, 8, 301. [Google Scholar] [CrossRef]
- World Health Organization. Hepatitis B Vaccination Coverage. Available online: https://immunizationdata.who.int/pages/coverage/HEPB.html (accessed on 15 August 2023).
- World Health Organization. Global Hepatitis Report 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Sanou, A.M.; Ilboudo, A.K.; Meda, Z.C.; Togozia, A.; Coulibaly, A.; Sagna Tani, A.C.; Dramane, K.; Tarnagda, Z. Hepatitis B Vaccination in Burkina Faso: Prevalence of HBsAg Carriage and Immune Response in Children in the Western Region. J. Infect. Dev. Ctries. 2018, 12, 1002–1008. [Google Scholar] [CrossRef]
- Apiung, T.; Ndanu, T.A.; Mingle, J.A.A.; Sagoe, K.W.C. Hepatitis B Virus Surface Antigen and Antibody Markers in Children at a Major Paediatric Hospital after the Pentavalent DTP-HBV-Hib Vaccination. Ghana Med. J. 2017, 51, 13–19. [Google Scholar] [CrossRef]
- Metodi, J.; Aboud, S.; Mpembeni, R.; Munubhi, E. Immunity to Hepatitis B Vaccine in Tanzanian Under-5 Children. Ann. Trop. Paediatr. 2010, 30, 129–136. [Google Scholar] [CrossRef]
- Breakwell, L.; Marke, D.; Kaiser, R.; Tejada-Strop, A.; Pauly, M.D.; Jabbi, S.; Yambasu, S.; Kabore, H.J.; Stewart, B.; Sesay, T.; et al. Assessing the Impact of the Routine Childhood Hepatitis B Immunization Program and the Need for Hepatitis B Vaccine Birth Dose in Sierra Leone, 2018. Vaccine 2022, 40, 2741–2748. [Google Scholar] [CrossRef] [PubMed]
- Klingler, C.; Thoumi, A.I.; Mrithinjayam, V.S. Cost-Effectiveness Analysis of an Additional Birth Dose of Hepatitis B Vaccine to Prevent Perinatal Transmission in a Medical Setting in Mozambique. Vaccine 2012, 31, 252–259. [Google Scholar] [CrossRef]
- Gosset, A. Introducing Birth-Dose Hepatitis B Vaccination Would Be Cost Effective in Burkina Faso. PharmacoEcon Outcomes News 2021, 883, 21–24. [Google Scholar] [CrossRef]
- Gosset, A.; Nishimwe, M.L.; Diallo, M.Y.; Deroo, L.; Diallo, A.; Ba, E.H.; Carrieri, P.M.; Sokhna, C.; Vray, M.; Shimakawa, Y.; et al. The Costs of Introducing the Hepatitis B Birth Dose Vaccine into the National Immunization Programme in Senegal (NéoVac Study). Vaccines 2021, 9, 521. [Google Scholar] [CrossRef]
- Memirie, S.T.; Desalegn, H.; Naizgi, M.; Nigus, M.; Taddesse, L.; Tadesse, Y.; Tessema, F.; Zelalem, M.; Girma, T. Introduction of Birth Dose of Hepatitis B Virus Vaccine to the Immunization Program in Ethiopia: An Economic Evaluation. Cost Eff. Resour. Alloc. 2020, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Reardon, J.M.; O’Connor, S.M.; Njau, J.D.; Lam, E.K.; Staton, C.A.; Cookson, S.T. Cost-Effectiveness of Birth-Dose Hepatitis B Vaccination among Refugee Populations in the African Region: A Series of Case Studies. Confl. Health 2019, 13, 5. [Google Scholar] [CrossRef]
- Hagan, J.E.; Carvalho, E.; Souza, V.; Queresma Dos Anjos, M.; Abimbola, T.O.; Pallas, S.W.; Tevi Benissan, M.C.; Shendale, S.; Hennessey, K.; Patel, M.K. Selective Hepatitis B Birth-Dose Vaccination in São Tomé and Príncipe: A Program Assessment and Cost-Effectiveness Study. Am. J. Trop. Med. Hyg. 2019, 101, 891–898. [Google Scholar] [CrossRef]
- Moturi, E.; Tevi-Benissan, C.; Hagan, J.E.; Shendale, S.; Mayenga, D.; Murokora, D.; Patel, M.; Hennessey, K.; Mihigo, R. Implementing a Birth Dose of Hepatitis B Vaccine in Africa: Findings from Assessments in 5 Countries. J. Immunol. Sci. 2018, 5, 31–40. [Google Scholar] [CrossRef]
- Okenwa, U.J.; Dairo, M.D.; Uba, B.; Ajumobi, O. Maternal Reasons for Non-Receipt of Valid Hepatitis B Birth Dose among Mother-Infant Pairs Attending Routine Immunization Clinics, South-East, Nigeria. Vaccine 2019, 37, 6894–6899. [Google Scholar] [CrossRef]
- Nankya-Mutyoba, J.N.; Surkan, P.J.; Makumbi, F.; Aizire, J.; Kirk, G.D.; Ocama, P.; Atuyambe, L.M. Hepatitis B Birth Dose Vaccination for Newborns in Uganda: A Qualitative Inquiry on Pregnant Women’s Perceptions, Barriers and Preferences. J. Virus Erad. 2021, 7, 100039. [Google Scholar] [CrossRef]
- Miyahara, R.; Jasseh, M.; Gomez, P.; Shimakawa, Y.; Greenwood, B.; Keita, K.; Ceesay, S.; D’Alessandro, U.; Roca, A. Barriers to Timely Administration of Birth Dose Vaccines in The Gambia, West Africa. Vaccine 2016, 34, 3335–3341. [Google Scholar] [CrossRef] [PubMed]
- Boisson, A.; Goel, V.; Yotebieng, M.; Parr, J.B.; Fried, B.; Thompson, P. Implementation Approaches for Introducing and Overcoming Barriers to Hepatitis B Birth-Dose Vaccine in Sub-Saharan Africa. Glob. Health Sci. Pract. 2022, 10, e2100277. [Google Scholar] [CrossRef] [PubMed]
- Périères, L.; Marcellin, F.; Lo, G.; Protopopescu, C.; Ba, E.H.; Coste, M.; Kane, C.T.; Maradan, G.; Diallo, A.; Sokhna, C.; et al. Hepatitis B Vaccination in Senegalese Children: Coverage, Timeliness, and Sociodemographic Determinants of Non-Adherence to Immunisation Schedules (ANRS 12356 AmBASS Survey). Vaccines 2021, 9, 510. [Google Scholar] [CrossRef] [PubMed]
- Olakunde, B.O.; Adeyinka, D.A.; Olakunde, O.A.; Ogundipe, T.; Oladunni, F.; Ezeanolue, E.E. The Coverage of Hepatitis B Birth Dose Vaccination in Nigeria: Does the Place of Delivery Matter? Trans. R. Soc. Trop. Med. Hyg. 2021, 116, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Allison, R.D.; Patel, M.K.; Tohme, R.A. Hepatitis B Vaccine Birth Dose Coverage Correlates Worldwide with Rates of Institutional Deliveries and Skilled Attendance at Birth. Vaccine 2017, 35, 4094–4098. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, A.; Akmatov, M.K.; Krause, G. Hepatitis B Vaccination Timing: Results from Demographic Health Surveys in 47 Countries. Bull. World Health Organ. 2017, 95, 199–209G. [Google Scholar] [CrossRef]
- Maponga, T.G.; Nwankwo, C.; Matthews, P.C. Sustainable Development Goals for HBV Elimination in South Africa: Challenges, Progress, and the Road Ahead. S. Afr. Gastroenterol. Rev. 2019, 17, 15–25. [Google Scholar] [CrossRef]
- Immunization Vaccines and Biologicals. Practices to Improve Coverage of the Hepatitis B Birth Dose Vaccine; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Cheung, C.K. Proportion of Children Born to Infected Mothers at Risk of Contracting Hepatitis B, and Associated Risk Factors for Inadequate Hepatitis B Timely Birth Dose Vaccination: Analysis of the São Tomé and Príncipe Demographic Health Survey Program Data, 2008–2009; Uppsala Universitet: Uppsala, Sweden, 2017. [Google Scholar]
- Kruk, M.; Freedman, L.P. Assessing Health System Performance in Developing Countries: A Review of the Literature. Health Policy 2008, 85, 263–276. [Google Scholar] [CrossRef]
- Samb, B.; Evans, T.; Dybul, M.; Atun, R.; Moatti, J.P.; Nishtar, S.; Wright, A.; Celletti, F.; Hsu, J.; Kim, J.Y.; et al. An Assessment of Interactions between Global Health Initiatives and Country Health Systems. Lancet 2009, 373, 2137–2169. [Google Scholar] [CrossRef]
- World Health Organization. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Arah, O.A.; Klazinga, N.S.; Delnoij, D.M.J.; Ten Asbroek, A.H.A.; Custers, T. Conceptual Frameworks for Health Systems Performance: A Quest for Effectiveness, Quality, and Improvement. Int. J. Qual. Health Care 2003, 15, 377–398. [Google Scholar] [CrossRef]
- Murray, C.J.; Frenk, A.J. A Framework for Assessing the Performance of Health Systems. Bull. World Health Organ. 2000, 78, 717–731. [Google Scholar] [PubMed]
- Van Olmen, J.; Criel, B.; Bhojani, U.; Marchal, B.; Van Belle, S.; Chenge, F.; Hoeree, T.; Pirard, M.; Van Damme, W.; Kegels, G. The Health System Dynamics Framework: The Introduction of an Analytical Model for Health System Analysis and Its Application to Two Case-Studies. Health Cult. Soc. 2012, 2, 1–21. [Google Scholar] [CrossRef]
- Rohwer, A.; Pfadenhauer, L.; Burns, J.; Brereton, L.; Gerhardus, A.; Booth, A.; Oortwijn, W.; Rehfuess, E. Series: Clinical Epidemiology in South Africa. Paper 3: Logic Models Help Make Sense of Complexity in Systematic Reviews and Health Technology Assessments. J. Clin. Epidemiol. 2017, 83, 37–47. [Google Scholar] [CrossRef]
- Amponsah-Dacosta, E.; Kagina, B.M.; Olivier, J. Health Systems Constraints and Facilitators of Human Papillomavirus Immunization Programmes in Sub-Saharan Africa: A Systematic Review. Health Policy Plan. 2020, 35, 701–717. [Google Scholar] [CrossRef] [PubMed]
- Shen, A.K.; Fields, R.; McQuestion, M. The Future of Routine Immunization in the Developing World: Challenges and Opportunities. Glob. Health Sci. Pract. 2014, 2, 381–394. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solomon-Rakiep, T.; Olivier, J.; Amponsah-Dacosta, E. Weak Adoption and Performance of Hepatitis B Birth-Dose Vaccination Programs in Africa: Time to Consider Systems Complexity?—A Scoping Review. Trop. Med. Infect. Dis. 2023, 8, 474. https://doi.org/10.3390/tropicalmed8100474
Solomon-Rakiep T, Olivier J, Amponsah-Dacosta E. Weak Adoption and Performance of Hepatitis B Birth-Dose Vaccination Programs in Africa: Time to Consider Systems Complexity?—A Scoping Review. Tropical Medicine and Infectious Disease. 2023; 8(10):474. https://doi.org/10.3390/tropicalmed8100474
Chicago/Turabian StyleSolomon-Rakiep, Tasneem, Jill Olivier, and Edina Amponsah-Dacosta. 2023. "Weak Adoption and Performance of Hepatitis B Birth-Dose Vaccination Programs in Africa: Time to Consider Systems Complexity?—A Scoping Review" Tropical Medicine and Infectious Disease 8, no. 10: 474. https://doi.org/10.3390/tropicalmed8100474