
Toxoplasmosis: A Timeless Challenge for Pregnancy
Abstract
:1. Introduction
2. Materials and Methods
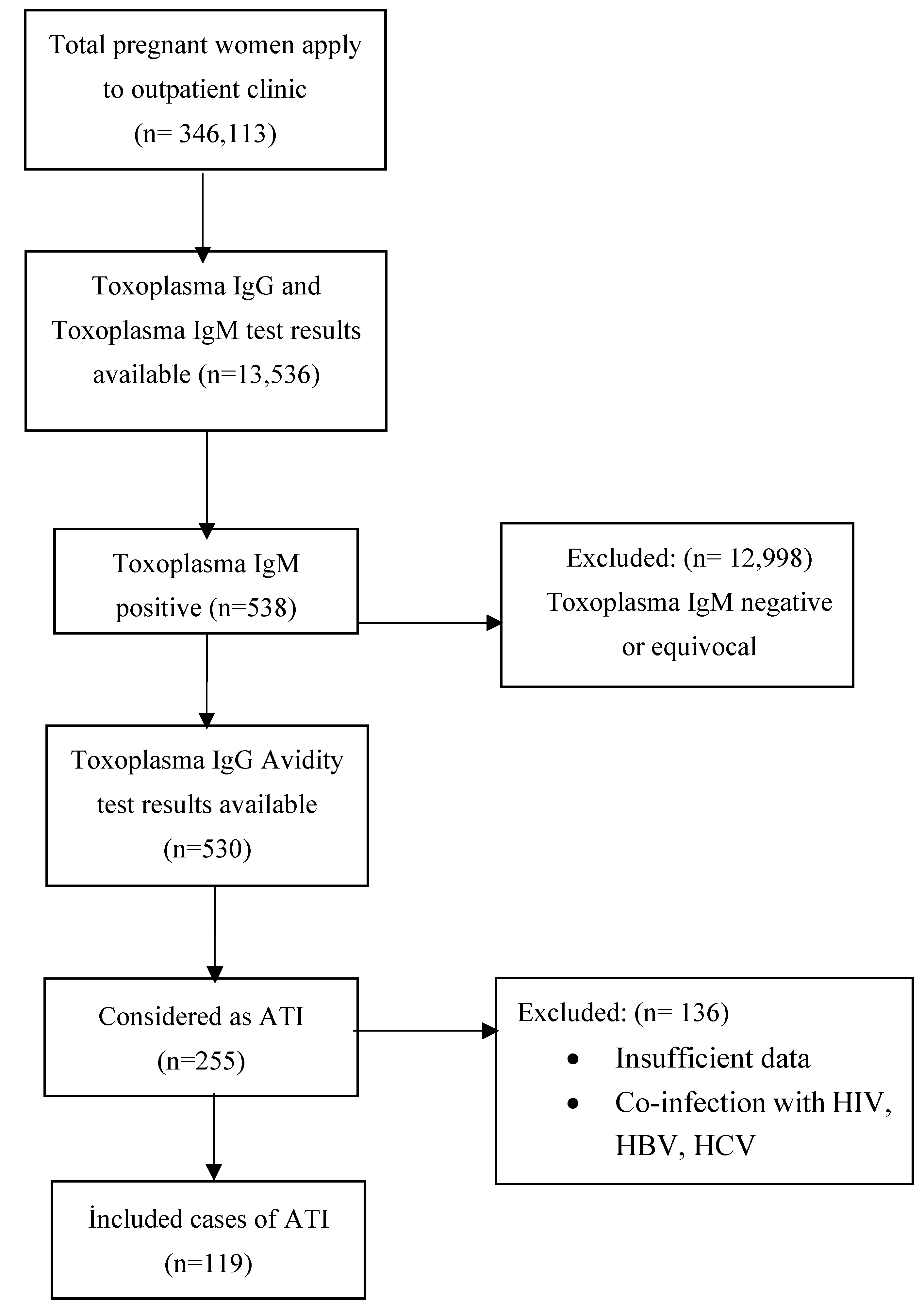
2.1. Patient Selection
- Patients who have a positive toxoplasma IgM and low IgG avidity results within each trimester;
- Patients who have a positive toxoplasma IgM and high or intermediate IgG avidity results after 16 weeks of pregnancy (in which acute past distinction cannot be made).
- Those who have toxoplasma IgM test positivity in the first 10 days after birth;
- Detection of increasing or persistent toxoplasma IgG titer in the first year of life without treatment;
- Detection of T. gondii DNA PCR or a positive toxoplasma IgM test for cerebrospinal fluid (CSF);
- Sabin-Feldman test positivity in blood or CSF (a titer of 1:16 is considered to be positive).
2.2. Laboratory Analysis
2.3. Statistical analyses
2.4. Ethical Permission
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmed, M.; Sood, A.; Gupta, J. Toxoplasmosis in pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 255, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Kieffer, F.; Wallon, M. Congenital toxoplasmosis. In Handbook of Clinical Neurology, 3rd ed.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 112, pp. 1099–1101. [Google Scholar]
- Khan, K.; Khan, W. Congenital toxoplasmosis: An overview of the neurological and ocular manifestations. Parasitol. Int. 2018, 67, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Villard, O.; Cimon, B.; L’Ollivier, C.; Fricker-Hidalgo, H.; Godineau, N.; Houze, S.; Paris, L.; Pelloux, H.; Villena, I.; Candolfi, E. Serological diagnosis of Toxoplasma gondii infection: Recommendations from the French National Reference Center for Toxoplasmosis. Diagn. Microbiol. Infect. Dis. 2016, 84, 22–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiter-Owona, I.; Petersen, E.; Joynson, D.; Aspöck, H.; Dardé, M.L.; Disko, R.; Dreazen, O.; Dumon, H.; Grillo, R.; Gross, U.; et al. The past and present role of the Sabin-Feldman dye test in the serodiagnosis of toxoplasmosis. Bull. World Health Organ. 1999, 77, 929–935. [Google Scholar]
- Hampton, M.M. Congenital Toxoplasmosis: A Review. Neonatal Netw. 2015, 34, 274–278. [Google Scholar] [CrossRef]
- Molan, A.; Nosaka, K.; Hunter, M.; Wang, W. Global status of Toxoplasma gondii infection: Systematic review and prevalence snapshots. Trop Biomed 2019, 36, 898–925. [Google Scholar]
- Cabra-Bautista, G.; Paz-Córdoba, B.E.; Henao-Pabón, T.; Bravo, A.M.; Florez, I.D.; Delgado-Noguera, M.; Calvache, J.A. Quality of clinical practice guidelines for gestational and congenital toxoplasmosis: A systematic review of the literature. J. Eval. Clin. Pract. 2022, 28, 218–224. [Google Scholar] [CrossRef]
- El Bissati, K.; Levigne, P.; Lykins, J.; Adlaoui, E.B.; Barkat, A.; Berraho, A.; Laboudi, M.; El Mansouri, B.; Ibrahimi, A.; Rhajaoui, M.; et al. Global initiative for congenital toxoplasmosis: An observational and international comparative clinical analysis. Emerg. Microbes Infect. 2018, 7, 165. [Google Scholar] [CrossRef] [Green Version]
- Dubey, J.P.; Murata, F.H.A.; Cerqueira-Cézar, C.K.; Kwok, O.C.H.; Villena, I. Congenital toxoplasmosis in humans: An update of worldwide rate of congenital infections. Parasitology 2021, 148, 1406–1416. [Google Scholar] [CrossRef]
- Kolören, Z.; Dubey, J.P. A review of toxoplasmosis in humans and animals in Turkey. Parasitology 2020, 147, 12–28. [Google Scholar] [CrossRef]
- Ulusan Bağcı, Ö.; Bayındır Bilman, F.; Baran, N.; Peker, B.O.; Pektaş, B.; Aksoy Gökmen, A.; Er, H.H.; Kaya, S. Retrospective Evaluation of Toxoplasma Serology in Patients Admitted to a Training and Research Hospital Between 2017–2021. Turk. Parazitol. Derg. 2022, 46, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Tekay, F.; Ozbek, E. The seroprevalence of Toxoplasma gondii in women from Sanliurfa, a province with a high raw meatball consumption. Turk. Parazitol. Derg. 2007, 31, 176–179. [Google Scholar]
- SYROCOT (Systematic Review on Congenital Toxoplasmosis) Study Group; Thiébaut, R.; Leproust, S.; Chêne, G.; Gilbert, R. Effectiveness of prenatal treatment for congenital toxoplasmosis: A meta-analysis of individual patients’ data. Lancet 2007, 369, 115–122. [Google Scholar]
- Dunn, D.; Wallon, M.; Peyron, F.; Petersen, E.; Peckham, C.; Gilbert, R. Mother-to-child transmission of toxoplasmosis: Risk estimates for clinical counselling. Lancet 1999, 353, 1829–1833. [Google Scholar] [CrossRef]
- Donadono, V.; Saccone, G.; Maruotti, G.M.; Berghella, V.; Migliorini, S.; Esposito, G.; Sirico, A.; Tagliaferri, S.; Ward, A.; Mazzarelli, L.L.; et al. Incidence of toxoplasmosis in pregnancy in Campania: A population-based study on screening, treatment, and outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 316–321. [Google Scholar] [CrossRef]
- Findal, G.; Helbig, A.; Haugen, G.; Jenum, P.A.; Stray-Pedersen, B. Management of suspected primary Toxoplasma gondii infection in pregnant women in Norway: Twenty years of experience of amniocentesis in a low-prevalence population. BMC Pregnancy Childbirth 2017, 17, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotop, A.; Hlobil, H.; Gross, U. Efficacy of rapid treatment initiation following primary Toxoplasma gondii infection during pregnancy. Clin. Infect. Dis. 2012, 54, 1545–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, E.; Meroni, V.; Vasconcelos-Santos, D.V.; Mandelbrot, L.; Peyron, F. Congenital toxoplasmosis: Should we still care about screening? Food Waterborne Parasitol. 2022, 11, e00162. [Google Scholar] [CrossRef]
- Wallon, M.; Peyron, F.; Cornu, C.; Vinault, S.; Abrahamowicz, M.; Kopp, C.B.; Binquet, C. Congenital toxoplasma infection: Monthly prenatal screening decreases transmission rate and improves clinical outcome at age 3 years. Clin. Infect. Dis. 2013, 56, 1223–1231. [Google Scholar] [CrossRef] [Green Version]
- Villena, I.; Ancelle, T.; Delmas, C.; Garcia, P.; Brezin, A.P.; Thulliez, P.; Wallon, M.; King, L.; Goulet, V. Toxosurv network and National Reference Centre for Toxoplasmosis. Congenital toxoplasmosis in France in 2007: First results from a national surveillance system. Eurosurveillance 2010, 15, 19600. [Google Scholar] [CrossRef] [Green Version]
- Prusa, A.R.; Kasper, D.C.; Pollak, A.; Olischar, M.; Gleiss, A.; Hayde, M. Amniocentesis for the detection of congenital toxoplasmosis: Results from the nationwide Austrian prenatal screening program. Clin. Microbiol. Infect. 2015, 21, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallon, M.; Kodjikian, L.; Binquet, C.; Garweg, J.; Fleury, J.; Quantin, C.; Peyron, F. Long-term ocular prognosis in 327 children with congenital toxoplasmosis. Pediatrics 2004, 113, 1567–1572. [Google Scholar] [CrossRef]
- Buonsenso, D.; Pata, D.; Turriziani, C.A.; Iademarco, M.; De Santis, M.; Masini, L.; Conti, G.; Molle, F.; Baldascino, A.; Acampora, A.; et al. Spyramicine and Trimethoprim-Sulfamethoxazole Combination to Prevent Mother-To-Fetus Transmission of Toxoplasma gondii Infection in Pregnant Women: A 28-Years Single-center Experience. Pediatr. Infect. Dis. J. 2022, 41, e223–e227. [Google Scholar] [CrossRef] [PubMed]
- Bartholo, B.B.G.R.; Monteiro, D.L.M.; Rodrigues, N.C.P.; Trajano, A.J.B.; de Jesus, N.R.; Cardoso, F.F.O.; de Souza, F.M.; Werner, H.; Araujo Júnior, E. Treatment of Acute Toxoplasmosis in Pregnancy: Influence in the Mother-to-Child Transmission. J. Obstet. Gynaecol. Can. 2020, 42, 1505–1510. [Google Scholar] [CrossRef]
- Avci, M.E.; Arslan, F.; Çiftçi, Ş.; Ekiz, A.; Tüten, A.; Yildirim, G.; Madazli, R. Role of spiramycin in prevention of fetal toxoplasmosis. J. Matern. Fetal Neonatal Med. 2016, 29, 2073–2076. [Google Scholar] [CrossRef] [PubMed]
- Freeman, K.; Tan, H.K.; Prusa, A.; Petersen, E.; Buffolano, W.; Malm, G.; Cortina-Borja, M.; Gilbert, R. European Multicentre Study on Congenital Toxoplasmosis. Predictors of retinochoroiditis in children with congenital toxoplasmosis: European, prospective cohort study. Pediatrics 2008, 121, e1215–e1222. [Google Scholar] [CrossRef]


{kind=link}
| Age, years, median (min-max) | 26 (18–40) |
| Gestational age at presentation | |
| ≤12 weeks (first trimester), n (%) | 60 (50.4) |
| 13–27 weeks (second trimester), n (%) | 46 (38.7) |
| ≥28 weeks (third trimester), n (%) | 13 (10.9) |
| Gravity, median (min-max) | 3 (1–10) |
| Parity, median (min-max) | 1 (0–8) |
| Fetal USG examination | |
| Normal, n (%) | 114 (95.8) |
| Abnormal, n (%) | 5 (4.2) |
| Type of delivery | |
| Normal vaginal, n (%) | 71 (59.6) |
| Cesarean section, n (%) | 36 (30.3) |
| Voluntarily termination, n (%) | 3 (2.5) |
| Missed abortion, n (%) | 2 (1.7) |
| Ongoing pregnancy, n (%) | 7 (5.9) |
| Week of pregnancy at diagnosis, median (min-max) | 12 (5–38) |
| Week of pregnancy at delivery, median (min-max) | 38 (17–40) |
| Toxoplasma IgM, median (min-max) | 2.06 (1.01–27.56) |
| Toxoplasma IgG, median (min-max) | 293 (2–650) |
| Toxoplasma IgG avidity | |
| Low avidity (<50%), n (%) | 98 (82.4) |
| Intermediate avidity (50–50.9%), n (%) | 8 (6.7) |
| High avidity (≥60%), n (%) | 13 (10.9) |
| Toxoplasma PCR in amniotic fluid | |
| Not done, n (%) | 95 (79.8) |
| Done—PCR negative, n (%) | 23 (19.3) |
| Done—PCR positive, n (%) | 1 (0.8) |
| Treatment | |
| Spiramycin, n (%) | 103 (86.6) |
| Rejected treatment, n (%) | 16 (13.4) |
| Treatment duration, week, median (min-max) | 17 (2–33) |
| Newborn abnormalities | |
| Absent, n (%) | 96 (80.7) |
| Present, n (%) | 5 (4.2) |
| Unknown, n (%) | 18 (15.1) |
| CHİLD-1 | CHİLD-2 | CHİLD-3 | CHİLD-4 | |
|---|---|---|---|---|
| Maternal Characteristics | ||||
| Week of Pregnancy at Diagnosis | 37 | 38 | 37 | 29 |
| Week of Pregnancy at Delivery | 39 | 38 | 38 | 29 |
| Intrauterine Amniocentesis | Not Done | Not Done | Not Done | Not Done |
| Intrauterine Treatment | No | No | No | No |
| Type of Delivery | C/S | Vaginal | Vaginal | C/S |
| Toxoplasma IgM | Negative | Positive | Positive | Positive |
| Toxoplasma IgG | Positive | Positive | Positive | Positive |
| Toxoplasma IgG Avidity | Low | Low | No Data | Low |
| Fetal Characteristics | ||||
| Gender | Female | Male | Male | Male |
| Fetal USG Findings | Macrocephaly Hydrocephalus | Not Done | Not Done | Heavy IUGR |
| Birth Weight | 2800 | 2950 | 2500 | 650 |
| Apgar Score | 6/8 | 9/10 | No Data | No Data |
| Toxoplasma IgM | Negative | Positive | Positive | Not Adjusted |
| Toxoplasma IgG | Positive | Positive | Negative | Not Adjusted |
| Sabin-Feldman | 1/1024 (Blood) | 1/1024 (Blood) | 1/64 (CSF) | Not Adjusted |
| BOS Toxo PCR | Negative | No Data | Negative | Not Adjusted |
| Clinical Findings of Toxoplasmosis | Chorioretinite Hydrocephalıs | Toxoplasma scar Cerebellar hypoplasia Arachnoid cyst | Microcephaly | Not Adjusted |
| Treatment | Primetamine Sulfadiazine Leucoverine IV Steroid | Primetamine Leucoverine Clindamycin | Primetamine Sulfadiazine Leucoverine | No Treatment |
| Outcome | Alive | Alive | Alive | Ex |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damar Çakırca, T.; Can, İ.N.; Deniz, M.; Torun, A.; Akçabay, Ç.; Güzelçiçek, A. Toxoplasmosis: A Timeless Challenge for Pregnancy. Trop. Med. Infect. Dis. 2023, 8, 63. https://doi.org/10.3390/tropicalmed8010063
Damar Çakırca T, Can İN, Deniz M, Torun A, Akçabay Ç, Güzelçiçek A. Toxoplasmosis: A Timeless Challenge for Pregnancy. Tropical Medicine and Infectious Disease. 2023; 8(1):63. https://doi.org/10.3390/tropicalmed8010063
Chicago/Turabian StyleDamar Çakırca, Tuba, İlkay Nur Can, Melis Deniz, Ayşe Torun, Çiğdem Akçabay, and Ahmet Güzelçiçek. 2023. "Toxoplasmosis: A Timeless Challenge for Pregnancy" Tropical Medicine and Infectious Disease 8, no. 1: 63. https://doi.org/10.3390/tropicalmed8010063