

Retrospective Modeling of the Omicron Epidemic in Shanghai, China: Exploring the Timing and Performance of Control Measures
 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. The Age-Structured and Vaccination-Stratified SEPASHRD Model
2.3. Parameter Settings and Initial States
2.4. Estimation of Parameters in the SEPASHRD Model
2.5. Simulation Study
2.6. Statistical Analysis
3. Results
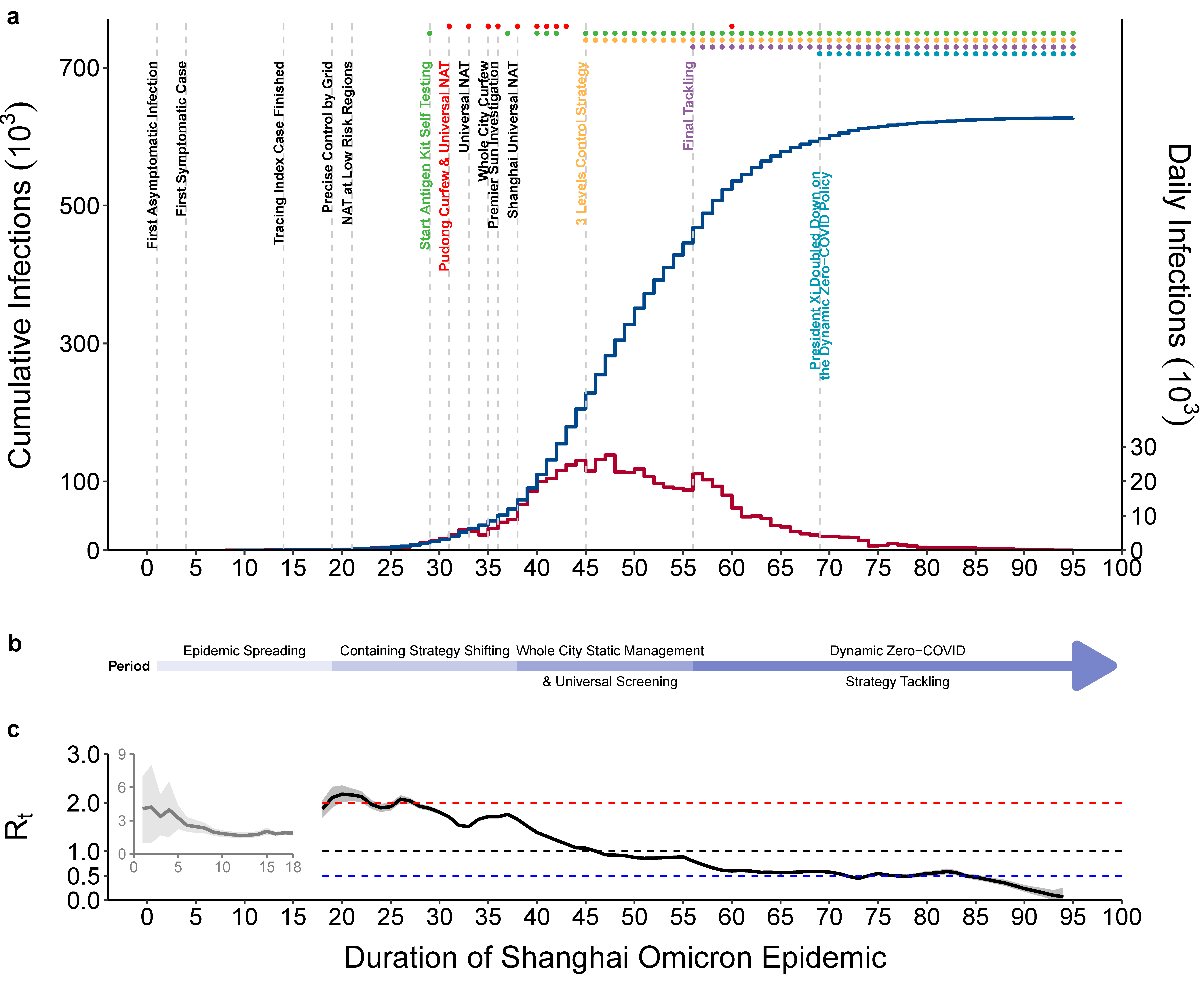
3.1. Brief Description of the Shanghai Omicron Epidemic
3.2. Model Design, Fitting, and Parameter Estimations
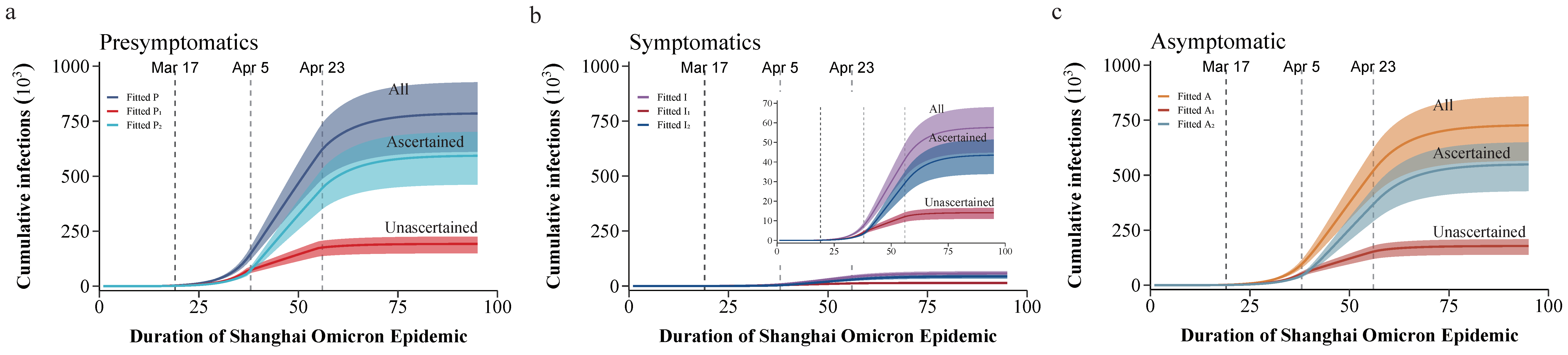
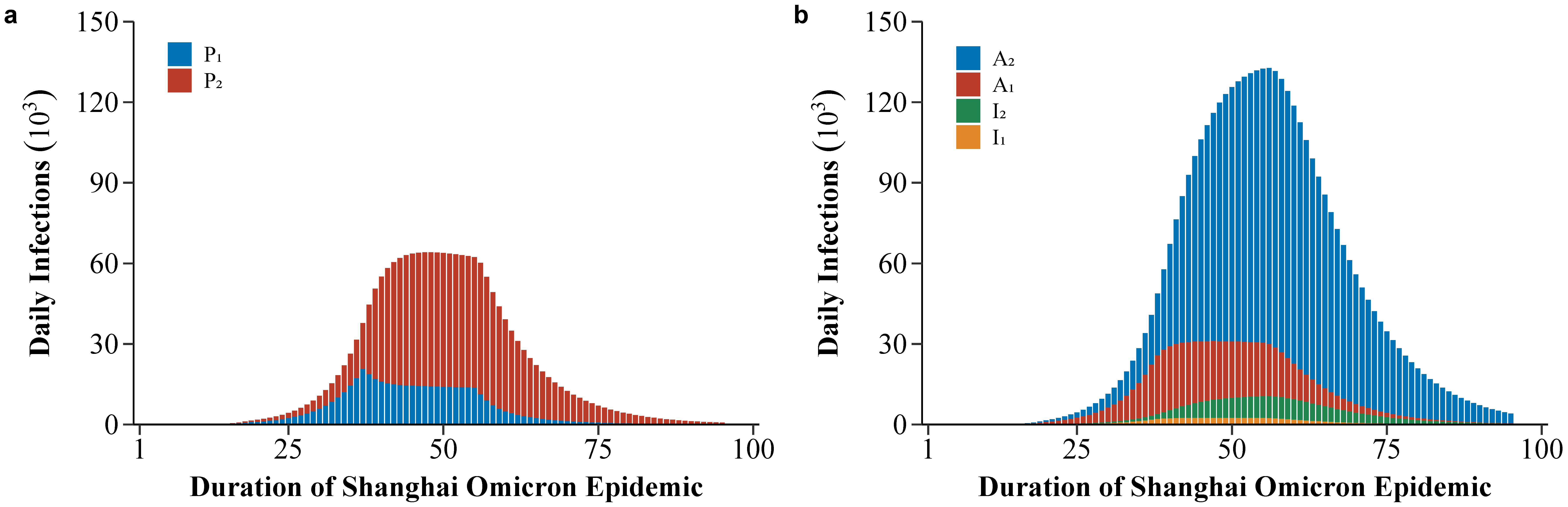
3.3. The Real Situation of the Shanghai Omicron Epidemic
3.4. Counterfactual Evaluation of Possible Control Strategies and Consequences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Peng, M. Outbreak of COVID-19: An emerging global pandemic threat. Biomed. Pharmacother. 2020, 129, 110499. [Google Scholar] [CrossRef]
- Chen, H.; Shi, L.; Zhang, Y.; Wang, X.; Sun, G. A cross-country core strategy comparison in China, Japan, Singapore and South Korea during the early COVID-19 pandemic. Glob. Health 2021, 17, 22. [Google Scholar] [CrossRef] [PubMed]
- Oliu-Barton, M.; Pradelski, B.S.R.; Aghion, P.; Artus, P.; Kickbusch, I.; Lazarus, J.V.; Sridhar, D.; Vanderslott, S. SARS-CoV-2 elimination, not mitigation, creates best outcomes for health, the economy, and civil liberties. Lancet 2021, 397, 2234–2236. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.Q.; Lv, L.; Chen, Y.; Chen, H.D.; Zhang, M.X.; Tung, T.H.; Zhu, J.S. The impact of the Omicron epidemic on the health behavior in Cape Town, South Africa. One Health 2022, 14, 100395. [Google Scholar] [CrossRef]
- Yuan, P.; Tan, Y.; Yang, L.; Aruffo, E.; Ogden, N.H.; Yang, G.; Lu, H.; Lin, Z.; Lin, W.; Ma, W.; et al. Assessing the mechanism of citywide test-trace-isolate Zero-COVID policy and exit strategy of COVID-19 pandemic. Infect. Dis. Poverty 2022, 11, 104. [Google Scholar] [CrossRef] [PubMed]
- Viana, R.; Moyo, S.; Amoako, D.G.; Tegally, H.; Scheepers, C.; Althaus, C.L.; Anyaneji, U.J.; Bester, P.A.; Boni, M.F.; Chand, M.; et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature 2022, 603, 679–686. [Google Scholar] [CrossRef]
- Krueger, T.; Gogolewski, K.; Bodych, M.; Gambin, A.; Giordano, G.; Cuschieri, S.; Czypionka, T.; Perc, M.; Petelos, E.; Rosinska, M.; et al. Risk assessment of COVID-19 epidemic resurgence in relation to SARS-CoV-2 variants and vaccination passes. Commun. Med. 2022, 2, 23. [Google Scholar] [CrossRef]
- Guo, Y.; Han, J.; Zhang, Y.; He, J.; Yu, W.; Zhang, X.; Wu, J.; Zhang, S.; Kong, Y.; Guo, Y.; et al. SARS-CoV-2 Omicron Variant: Epidemiological Features, Biological Characteristics, and Clinical Significance. Front. Immunol. 2022, 13, 877101. [Google Scholar] [CrossRef]
- Team, C.C.-R. SARS-CoV-2 B.1.1.529 (Omicron) Variant—United States, December 1–8, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1731–1734. [Google Scholar] [CrossRef]
- Del Rio, C.; Omer, S.B.; Malani, P.N. Winter of Omicron-The Evolving COVID-19 Pandemic. JAMA 2022, 327, 319–320. [Google Scholar] [CrossRef]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and COVID-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, M.; Liang, W. Persevere in the Dynamic COVID-Zero Strategy in China to Gain a Precious Time Window for the Future. China CDC Wkly 2022, 4, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Akkiz, H. The Biological Functions and Clinical Significance of SARS-CoV-2 Variants of Corcern. Front. Med. 2022, 9, 849217. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Deng, X.; Yang, J.; Sun, K.; Liu, H.; Chen, Z.; Peng, C.; Chen, X.; Wu, Q.; Zou, J.; et al. Modeling transmission of SARS-CoV-2 Omicron in China. Nat. Med. 2022, 28, 1468–1475. [Google Scholar] [CrossRef]
- Modes, M.E.; Directo, M.P.; Melgar, M.; Johnson, L.R.; Yang, H.; Chaudhary, P.; Bartolini, S.; Kho, N.; Noble, P.W.; Isonaka, S.; et al. Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance—One Hospital, California, July 15–September 23, 2021, and December 21, 2021–January 27, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Christie, B. COVID-19: Early studies give hope omicron is milder than other variants. BMJ 2021, 375, n3144. [Google Scholar] [CrossRef]
- Wolff, G.B.; Oliu-Barton, M. Europe must come together to confront omicron. BMJ 2022, 376, o90. [Google Scholar] [CrossRef]
- Bershteyn, A.; Kim, H.Y.; Braithwaite, R.S. Real-Time Infectious Disease Modeling to Inform Emergency Public Health Decision Making. Annu. Rev. Public Health 2022, 43, 397–418. [Google Scholar] [CrossRef]
- Markovic, R.; Sterk, M.; Marhl, M.; Perc, M.; Gosak, M. Socio-demographic and health factors drive the epidemic progression and should guide vaccination strategies for best COVID-19 containment. Results Phys. 2021, 26, 104433. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, W.; Chen, S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet 2022, 399, 2011–2012. [Google Scholar] [CrossRef]
- Tian, H.; Liu, Y.; Li, Y.; Wu, C.H.; Chen, B.; Kraemer, M.U.G.; Li, B.; Cai, J.; Xu, B.; Yang, Q.; et al. An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China. Science 2020, 368, 638–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Chang, H.; Tian, H.; Zhu, Y.; Li, J.; Wei, Z.; Wang, Y.; Xia, A.; Ge, Y.; Liu, G.; et al. Epidemiological and clinical features of SARS-CoV-2 infection in children during the outbreak of Omicron variant in Shanghai, March 7–31, 2022. Influenza Other Respir. Viruses 2022, 16, 1059–1065. [Google Scholar] [CrossRef]
- Shao, J.; Fan, R.; Hu, J.; Zhang, T.; Lee, C.; Huang, X.; Wang, F.; Liang, H.; Jin, Y.; Jiang, Y.; et al. Clinical Progression and Outcome of Hospitalized Patients Infected with SARS-CoV-2 Omicron Variant in Shanghai, China. Vaccines 2022, 10, 1409. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Deng, X.; Fang, L.; Sun, K.; Wu, Y.; Che, T.; Zou, J.; Cai, J.; Liu, H.; Wang, Y.; et al. Epidemiological characteristics and transmission dynamics of the outbreak caused by the SARS-CoV-2 Omicron variant in Shanghai, China: A descriptive study. Lancet Reg. Health West. Pac. 2022, 29, 100592. [Google Scholar] [CrossRef]
- Chen, X.; Yan, X.; Sun, K.; Zheng, N.; Sun, R.; Zhou, J.; Deng, X.; Zhuang, T.; Cai, J.; Zhang, J.; et al. Estimation of disease burden and clinical severity of COVID-19 caused by Omicron BA.2 in Shanghai, February–June 2022. Emerg. Microbes Infect. 2022, 11, 2800–2807. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Cao, S.; Zhao, L.; Yan, Y.; Huang, J. Policy choices for Shanghai responding to challenges of Omicron. Front. Public Health 2022, 10, 927387. [Google Scholar] [CrossRef]
- Cai, M.; Em Karniadakis, G.; Li, C. Fractional SEIR model and data-driven predictions of COVID-19 dynamics of Omicron variant. Chaos 2022, 32, 071101. [Google Scholar] [CrossRef]
- Yang, H.; Nie, H.; Zhou, D.; Wang, Y.; Zuo, W. The Effect of Strict Lockdown on Omicron SARS-CoV-2 Variant Transmission in Shanghai. Vaccines 2022, 10, 1392. [Google Scholar] [CrossRef]
- Zhang, J.; Klepac, P.; Read, J.M.; Rosello, A.; Wang, X.; Lai, S.; Li, M.; Song, Y.; Wei, Q.; Jiang, H.; et al. Patterns of human social contact and contact with animals in Shanghai, China. Sci. Rep. 2019, 9, 15141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef]
- Du, Z.W.; Liu, C.F.; Wang, L.; Bai, Y.; Lau, E.H.Y.; Wu, P.; Cowling, B.J. Shorter serial intervals and incubation periods in SARS-CoV-2 variants than the SARS-CoV-2 ancestral strain. J. Travel Med. 2022, 29. [Google Scholar] [CrossRef] [PubMed]
- The State Council Information Office of the People’s Republic of China. Press Conference Held in Shanghai on Prevention and Control of COVID-19 Epidemic (180th). Available online: http://www.scio.gov.cn/xwfbh/gssxwfbh/xwfbh/shanghai/Document/1724361/1724361.htm (accessed on 11 May 2022).
- The Government of the Hong Kong Special Administrative Region. Hong Kong Vaccination Dashboard. Available online: https://www.covidvaccine.gov.hk/en/dashboard (accessed on 25 September 2022).
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Garrett, N.; Tapley, A.; Andriesen, J.; Seocharan, I.; Fisher, L.H.; Bunts, L.; Espy, N.; Wallis, C.L.; Randhawa, A.K.; Miner, M.D.; et al. High Asymptomatic Carriage With the Omicron Variant in South Africa. Clin. Infect. Dis. 2022, 75, e289–e292. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Jian, F.; Song, W.; Xiao, T.; Wang, L.; Du, S.; Wang, J.; Li, Q.; Chen, X.; et al. BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Nature 2022, 608, 593–602. [Google Scholar] [CrossRef]
- Huang, L. Adjusted control rate closely associated with the epidemiologic evolution of the recent COVID-19 wave in Shanghai, with 94.3% of all new cases being asymptomatic on first diagnosis. J. Infect. 2022, 85, e89–e91. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, F.; Cui, J.; Peng, Z.; Chang, Z.; Lai, S.; Chen, Q.; Wang, L.; Gao, G.F.; Feng, Z. Comprehensive large-scale nucleic acid-testing strategies support China’s sustained containment of COVID-19. Nat. Med. 2021, 27, 740–742. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Wu, Z.; Li, Z.; Zhang, Y.; McGoogan, J.M.; Li, Q.; Dong, X.; Ren, R.; Feng, L.; Qi, X.; et al. One Hundred Days of Coronavirus Disease 2019 Prevention and Control in China. Clin. Infect. Dis. 2021, 72, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Sun, K.; Feng, Z.; Yi, L.; Wu, Y.; Liu, H.; Wang, Q.; Ajelli, M.; Viboud, C.; Yu, H. Assessing the feasibility of sustaining SARS-CoV-2 local containment in China in the era of highly transmissible variants. medRxiv 2022, 20, 442. [Google Scholar] [CrossRef]
- Chen, Q.; Rodewald, L.; Lai, S.; Gao, G.F. Rapid and sustained containment of COVID-19 is achievable and worthwhile: Implications for pandemic response. BMJ 2021, 375, e066169. [Google Scholar] [CrossRef]
- Hao, X.; Cheng, S.; Wu, D.; Wu, T.; Lin, X.; Wang, C. Reconstruction of the full transmission dynamics of COVID-19 in Wuhan. Nature 2020, 584, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Elliot, A.J.; Harcourt, S.E.; Hughes, H.E.; Loveridge, P.; Morbey, R.A.; Smith, S.; Soriano, A.; Bains, A.; Smith, G.E.; Edeghere, O.; et al. The COVID-19 pandemic: A new challenge for syndromic surveillance. Epidemiol. Infect. 2020, 148, e122. [Google Scholar] [CrossRef]
- Lash, R.R.; Moonan, P.K.; Byers, B.L.; Bonacci, R.A.; Bonner, K.E.; Donahue, M.; Donovan, C.V.; Grome, H.N.; Janssen, J.M.; Magleby, R.; et al. COVID-19 Case Investigation and Contact Tracing in the US, 2020. JAMA Netw. Open 2021, 4, e2115850. [Google Scholar] [CrossRef] [PubMed]
- Shanghai Finance Bureau. Shanghai’s General Public Budget Revenue and Expenditure from January to July 2022. Available online: http://czj.sh.gov.cn/zys_8908/czsj_9054/dfczsz/20220831/xxfbinfo0000010287.html (accessed on 27 September 2022).
- Zhang, A.Z.; Enns, E.A. Optimal timing and effectiveness of COVID-19 outbreak responses in China: A modelling study. BMC Public Health 2022, 22, 679. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Wang, W.; Gao, L.; Wang, Y.; Luo, K.; Ren, L.; Zhan, Z.; Chen, X.; Zhao, S.; Huang, Y.; et al. Transmission heterogeneities, kinetics, and controllability of SARS-CoV-2. Science 2021, 371, eabe2424. [Google Scholar] [CrossRef]
- Zhang, J.; Litvinova, M.; Liang, Y.; Wang, Y.; Wang, W.; Zhao, S.; Wu, Q.; Merler, S.; Viboud, C.; Vespignani, A.; et al. Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China. Science 2020, 368, 1481–1486. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- McMenamin, M.E.; Nealon, J.; Lin, Y.; Wong, J.Y.; Cheung, J.K.; Lau, E.H.Y.; Wu, P.; Leung, G.M.; Cowling, B.J. Vaccine effectiveness of one, two, and three doses of BNT162b2 and CoronaVac against COVID-19 in Hong Kong: A population-based observational study. Lancet Infect. Dis. 2022, 22, 1435–1443. [Google Scholar] [CrossRef]
- Li, R.; Metcalf, C.J.E.; Stenseth, N.C.; Bjornstad, O.N. A general model for the demographic signatures of the transition from pandemic emergence to endemicity. Sci. Adv. 2021, 7, eabf9040. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lou, L.; Zhang, L.; Guan, J.; Ning, X.; Nie, M.; Wei, Y.; Chen, F. Retrospective Modeling of the Omicron Epidemic in Shanghai, China: Exploring the Timing and Performance of Control Measures. Trop. Med. Infect. Dis. 2023, 8, 39. https://doi.org/10.3390/tropicalmed8010039
Lou L, Zhang L, Guan J, Ning X, Nie M, Wei Y, Chen F. Retrospective Modeling of the Omicron Epidemic in Shanghai, China: Exploring the Timing and Performance of Control Measures. Tropical Medicine and Infectious Disease. 2023; 8(1):39. https://doi.org/10.3390/tropicalmed8010039
Chicago/Turabian StyleLou, Lishu, Longyao Zhang, Jinxing Guan, Xiao Ning, Mengli Nie, Yongyue Wei, and Feng Chen. 2023. "Retrospective Modeling of the Omicron Epidemic in Shanghai, China: Exploring the Timing and Performance of Control Measures" Tropical Medicine and Infectious Disease 8, no. 1: 39. https://doi.org/10.3390/tropicalmed8010039