
The Role of Post-Bronchoscopy Sputum Examination in Screening for Active Tuberculosis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Definition, Collection of the Sputum, and Bronchoscopy BAL Technique
2.2. Data Collection
2.3. Statistical Analysis
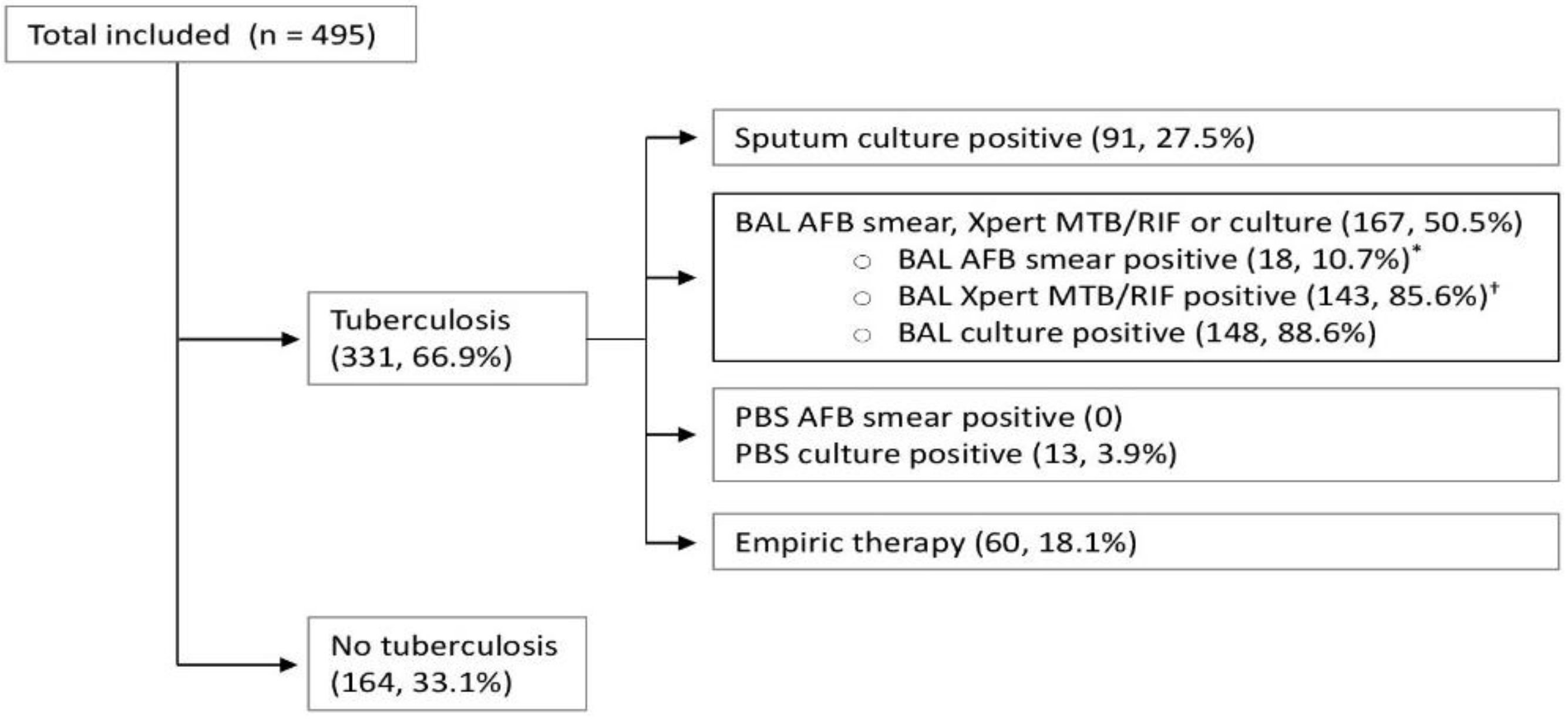
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Diagnostic Yield for Individual and Combinations of Tests for Confirmation of Active TB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2022. Available online: https://apps.who.int/iris/bitstream/handle/10665/363752/9789240061729-eng.pdf (accessed on 27 October 2022).
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis. Module 2: Screening—Systematic Screening for Tuberculosis Disease. Available online: https://apps.who.int/iris/bitstream/handle/10665/340255/9789240022676-eng.pdf (accessed on 27 October 2022).
- Uplekar, M.; Weil, D.; Lonnroth, K.; Jaramillo, E.; Lienhardt, C.; Dias, H.M.; Falzon, D.; Floyd, K.; Gargioni, G.; Getahun, H.; et al. WHO’s new end TB strategy. Lancet 2015, 385, 1799–1801. [Google Scholar] [CrossRef] [PubMed]
- Parsons, L.M.; Somoskövi, Á.; Gutierrez, C.; Lee, E.; Paramasivan, C.N.; Abimiku, A.; Spector, S.; Roscigno, G.; Nkengasong, J. Laboratory diagnosis of tuberculosis in resource-poor Countries: Challenges and opportunities. Clin. Microbiol. Rev. 2011, 24, 314–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haraka, F.; Kakolwa, M.; Schumacher, S.G.; Nathavitharana, R.R.; Denkinger, C.M.; Gagneux, S.; Reither, K.; Ross, A. Impact of the diagnostic test Xpert MTB/RIF on patient outcomes for tuberculosis. Cochrane Database Syst. Rev. 2021, 2021, CD012972. [Google Scholar] [CrossRef]
- Corbett, E.L.; Marston, B.; Churchyard, G.J.; de Cock, K.M. Tuberculosis in sub-Saharan Africa: Opportunities, challenges, and change in the era of antiretroviral treatment. Lancet 2006, 367, 926–937. [Google Scholar] [CrossRef] [PubMed]
- Boehme, C.C.; Nabeta, P.; Hillemann, D.; Nicol, M.P.; Shenai, S.; Krapp, F.; Allen, J.; Tahirli, R.; Blakemore, R.; Rustomjee, R.; et al. Rapid Molecular Detection of Tuberculosis and Rifampin Resistance. N. Engl. J. Med. 2010, 363, 1005–1015. [Google Scholar] [CrossRef] [Green Version]
- George, P.M.; Mehta, M.; Dhariwal, J.; Singanayagam, A.; Raphael, C.E.; Salmasi, M.; Connell, D.W.; Molyneaux, P.; Wickremasinghe, M.; Jepson, A.; et al. Post-bronchoscopy sputum: Improving the diagnostic yield in smear negative pulmonary TB. Respir. Med. 2011, 105, 1726–1731. [Google Scholar] [CrossRef] [Green Version]
- Lewinsohn, D.M.; Leonard, M.K.; Lobue, P.A.; Cohn, D.L.; Daley, C.L.; Desmond, E.; Keane, J.; Lewinsohn, D.A.; Loeffler, A.M.; Mazurek, G.H.; et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin. Infect. Dis. 2017, 64, e1–e33. [Google Scholar] [CrossRef]
- Wallace, J.M.; Deutsch, A.L.; Harrell, J.H.; Moser, K.M. Bronchoscopy and transbronchial biopsy in evaluation of patients with suspected active tuberculosis. Am. J. Med. 1981, 70, 1189–1194. [Google Scholar] [CrossRef]
- Sarkar, S.K.; Sharma, G.S.; Gupta, P.R.; Sharma, R.K. Fiberoptic bronchoscopy in the diagnosis of pulmonary tuberculosis. Tubercle 1980, 61, 97–99. [Google Scholar] [CrossRef]
- Park, J.H.; Jo, K.W.; Shim, T.S.; Kim, S.H. Diagnostic yield of post-bronchoscopy sputum for diagnosing pauci-bacillary pulmonary tuberculosis. Ann. Med. 2021, 53, 576–580. [Google Scholar] [CrossRef]
- L-Suwaidi, Z.A. Tuberculosis in Qatar. Int. J. Mycobacteriology 2015, 4, 124. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumb, R.; van Deun, A.; Bastian, I.; Fitz-Gerald, M. Laboratory Diagnosis of Tuberculosis by Sputum Microscopy; SA Pathology: Adelaide, Australia, 2013.
- Boardman, N.J.; Moore, T.; Freiman, J.; Tagliaferri, G.; McMurray, D.; Elson, D.; Lederman, E. Pulmonary Tuberculosis Disease among Immigrant Detainees: Rapid Disease Detection, High Prevalence of Asymptomatic Disease, and Implications for Tuberculosis Prevention. Clin. Infect. Dis. 2021, 73, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Mathez, C.; Bangala, Y.; Bady, P.; Zellweger, J.P. Active screening for pulmonary tuberculosis by chest x-ray among immigrants at the Swiss border. Swiss Med. Wkly. 2007, 137, 649–654. [Google Scholar] [CrossRef]
- Khawbung, J.L.; Nath, D.; Chakraborty, S. Drug resistant Tuberculosis: A review. Comp. Immunol. Microbiol. Infect. Dis. 2021, 74, 101574. [Google Scholar] [CrossRef]
- Danek, S.J.; Bower, J.S. Diagnosis of pulmonary tuberculosis by flexible fiberoptic bronchoscopy. Am. Rev. Respir. Dis. 1979, 119, 677–679. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.S.; Sun, A.J.M.; Hoheisel, G.B. Bronchoscopic aspiration and bronchoalveolar lavage in the diagnosis of sputum smear-negative pulmonary tuberculosis. Lung 1990, 168, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Tamura, A.; Shimada, M.; Matsui, Y.; Kawashima, M.; Suzuki, J.; Ariga, H.; Ohshima, N.; Masuda, K.; Matsui, H.; Nagai, H.; et al. The value of fiberoptic bronchoscopy in culture-positive pulmonary tuberculosis patients whose pre-bronchoscopic sputum specimens were negative both for smear and PCR analyses. Intern. Med. 2010, 49, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Chawla, R.; Pant, K.; Jaggi, O.P.; Chandrashekhar, S.; Thukral, S.S. Fibreoptic bronchoscopy in smear-negative pulmonary tuberculosis. Eur. Respir. J. 1988, 1, 804–806. [Google Scholar] [CrossRef]
- Bouton, T.C.; Jacobson, K.R. Symptom Screens Are Not Sufficient: The Fight against Tuberculosis Needs Better Weapons. Clin. Infect. Dis. 2021, 73, 121–123. [Google Scholar] [CrossRef]
- Drain, P.K.; Bajema, K.L.; Dowdy, D.; Dheda, K.; Naidoo, K.; Schumacher, S.G.; Ma, S.; Meermeier, E.; Lewinsohn, D.M.; Sherman, D.R. Incipient and subclinical tuberculosis: A clinical review of early stages and progression of infection. Clin. Microbiol. Rev. 2018, 31, e00021-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, D.J.; Lewis, W.P.; Barnes, P.F. Yield of bronchoscopy for the diagnosis of tuberculosis in patients with human immunodeficiency virus infection. Chest 1992, 102, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Aderaye, G.; Gegziabher, H.; Aseffa, A.; Worku, A.; Lindquist, L. Comparison of acid-fast stain and culture for Mycobacterium tuberculosis in pre- and post-bronchoscopy sputum and bronchoalveolar lavage in HIV-infected patients with atypical chest X-ray in Ethiopia. Ann. Thorac. Med. 2007, 2, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.A.; Wright, A. The World Health Organization/International Union against Tuberculosis and Lung Disease Global Project on Surveillance for anti-tuberculosis drug resistance: A model for other infectious diseases. Clin. Infect. Dis. 2005, 41, S258–S262. [Google Scholar] [CrossRef]
- Malekmohammad, M.; Marjani, M.; Tabarsi, P.; Baghaei, P.; Sadr, Z.; Naghan, P.A.; Mansouri, D.; Masjedi, M.R.; Velayati, A.A. Diagnostic yield of post-bronchoscopy sputum smear in pulmonary tuberculosis. Scand. J. Infect. Dis. 2012, 44, 369–373. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 495) | Active Tuberculosis (n = 331) | No Active Tuberculosis (n = 164) | p Value | |
|---|---|---|---|---|
| Age—years | 31 (26–38) | 30 (26–37) | 34 (29–41.5) | <0.001 |
| Male sex | 329 (66.5%) | 226 (68.3%) | 103 (62.8%) | 0.23 |
| Nationality by WHO region of origin | 0.13 | |||
| African Region | 66 (13.3%) | 53 (16%) | 13 (7.9%) | |
| Eastern Mediterranean region | 36 (7.3%) | 23 (7%) | 13 (7.9%) | |
| European region | 2 (0.4%) | 1 (0.3%) | 1 (0.6%) | |
| Region of America | 1 (0.2%) | 1 (0.3%) | 0 | |
| South-East Asia | 266 (53.7%) | 171 (51.7%) | 95 (57.9%) | |
| Western Pacific Region | 124 (25.1%) | 82 (24.8%) | 42 (25.6%) | |
| Craft and manual worker | 428 (86.5%) | 287 (86.7%) | 141 (86%) | 0.89 |
| Arrived in Qatar within the preceding 6 months | 414 (83.6%) | 272 (82.2%) | 142 (86.6%) | 0.25 |
| Smoker | 201 (40.6%) | 149 (45%) | 52 (31.7%) | 0.005 |
| Diabetes | 44 (8.9%) | 31 (9.4%) | 13 (7.9%) | 0.74 |
| Hypertension | 15 (3%) | 8 (2.4%) | 7 (4.3%) | 0.27 |
| Chronic lung disease | 5 (1%) | 3 (0.9%) | 2 (1.2%) | 0.67 |
| Malignancy | 2 (0.4%) | 1 (0.3%) | 1 (0.6%) | 0.55 |
| Chronic kidney disease | 63 (12.7%) | 43 (13%) | 20 (12.2%) | 0.89 |
| Human immunodeficiency virus infection | 2 (0.4%) | 2 (0.6%) | 0 | >0.999 |
| Tuberculosis symptoms | 197 (39.8%) | 132 (39.9%) | 65 (39.6%) | >0.999 |
| Fever | 102 (20.6%) | 70 (21.2%) | 32 (19.5%) | 0.72 |
| Weight loss | 81 (16.4%) | 61 (18.4%) | 20 (12.2%) | 0.093 |
| Cough | 160 (32.3%) | 96 (29%) | 64 (39%) | 0.032 |
| Night sweats | 30 (6.1%) | 25 (7.6%) | 5 (3.1%) | 0.07 |
| History of previous tuberculosis | 28 (5.7%) | 11 (3.3%) | 17 (10.4%) | 0.003 |
| Family history of tuberculosis | 37 (7.5%) | 29 (8.76%) | 8 (4.88%) | 0.15 |
| Bilateral radiological abnormalities | 259 (52.3%) | 164 (49.6%) | 95 (57.9%) | 0.086 |
| Apical radiological abnormalities | 235 (47.5%) | 175 (52.9%) | 60 (36.6%) | <0.001 |
| TST > 5 mm * | 159 (32.12%) | 106 (32.02%) | 53 (32.32%) | 0.43 |
| QuantiFERON TB Gold positive † | 228 (46.1%) | 175 (52.9%) | 53 (32.32%) | <0.001 |
| TST > 5 mm or QuantiFERON TB Gold positive | 356 (71.9%) | 263 (79.5%) | 93 (56.7%) | <0.001 |
| Hemoglobin counts gm/dL | 13.9 (12.9–15.1) | 13.8 (12.7–15.1) | 14.3 (13.1–15.3) | 0.039 |
| Peripheral white cell count (×109/L) | 7.7 (6.4–9.4) | 7.6 (6.4–9.1) | 8 (6.3–9.9) | 0.22 |
| Platelet count (109/L) | 296 (252–349) | 297 (255–349) | 291 (241–350) | 0.33 |
| C-reactive protein (mg/L) | 5.6 (1.8–44.6) | 11 (2–50) | 3 (0.9–9.4) | 0.032 |
| Alanine transaminase (U/L) | 18 (13–27) | 17.8 (13–26.7) | 20.9 (14.3–28) | 0.016 |
| Number (%) with Positive Results for M. tuberculosis | Sensitivity (95% CI) | Negative Predictive Value (95% CI) | Negative Likelihood Ratio (95% CI) | |
|---|---|---|---|---|
| Expectorate sputum culture | 91 (18.4%) | 27.5% (22.7–32.3) | 40.6% (35.8–45.4) | 0.73 (0.68–0.77) |
| BAL AFB smear | 35 (7.1%) | 10.6% (7.2–13.9) | 35.7% (31.3–40.0) | 0.89 (0.86–0.93) |
| BAL Xpert MTB/RIF | 213 (43%) | 64.4% (59.2–69.5) | 58.2% (52.4–63.9) | 0.36 (0.31–0.41) |
| BAL culture | 225 (45.5%) | 68.0% (62.9–73.0) | 60.7% (54.9–66.6) | 0.32 (0.27–0.37) |
| BAL AFB smear, Xpert MTB/RIF, or culture | 245 (49.5%) | 74.0% (69.3–78.7) | 65.6% (59.7–71.5) | 0.26 (0.22–0.31) |
| Post-bronchoscopy sputum AFB smear | 18 (3.6%) | 5.4% (3.0–7.9) | 34.4% (30.1–38.6) | 0.95 (0.92–0.97) |
| Post-bronchoscopy sputum culture | 131 (26.5%) | 39.6% (34.3–44.8) | 45.1% (39.9–50.2) | 0.60 (0.55–0.66) |
| Post-bronchoscopy sputum AFB smear or culture | 132 (26.7%) | 39.9% (34.6–45.2) | 45.2% (40.1–50.3) | 0.60 (0.55–0.66) |
| Expectorated sputum or BAL AFB smear, culture, or Xpert MTB/RIF | 258 (52.1%) | 77.9% (73.5–82.4) | 69.2% (63.3–75.1) | 0.22 (0.18–0.27) |
| Expectorated sputum, BAL or post-bronchoscopy sputum AFB smear, culture, or Xpert MTB/RIF | 271 (54.7%) | 81.9% (77.7–86) | 73.2% (67.4–79) | 0.18 (0.14–0.23) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, G.A.; Goravey, W.; Howady, F.S.; Ali, M.; Alshurafa, A.; Abdalhadi, A.M.; Hajmusa, M.; Daghfal, J.; Khal, A.A.; Maslamani, M.A.; et al. The Role of Post-Bronchoscopy Sputum Examination in Screening for Active Tuberculosis. Trop. Med. Infect. Dis. 2023, 8, 13. https://doi.org/10.3390/tropicalmed8010013
Ali GA, Goravey W, Howady FS, Ali M, Alshurafa A, Abdalhadi AM, Hajmusa M, Daghfal J, Khal AA, Maslamani MA, et al. The Role of Post-Bronchoscopy Sputum Examination in Screening for Active Tuberculosis. Tropical Medicine and Infectious Disease. 2023; 8(1):13. https://doi.org/10.3390/tropicalmed8010013
Chicago/Turabian StyleAli, Gawahir A., Wael Goravey, Faraj S. Howady, Maisa Ali, Awni Alshurafa, Ahmed M. Abdalhadi, Muhammed Hajmusa, Joanne Daghfal, Abdullatif Al Khal, Muna Al Maslamani, and et al. 2023. "The Role of Post-Bronchoscopy Sputum Examination in Screening for Active Tuberculosis" Tropical Medicine and Infectious Disease 8, no. 1: 13. https://doi.org/10.3390/tropicalmed8010013