
Dengue Incidence Trends and Its Burden in Major Endemic Regions from 1990 to 2019

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Ethics Statement
2.2. Data Collection
2.3. Statistical Analysis
2.4. ARIMA Model
3. Results
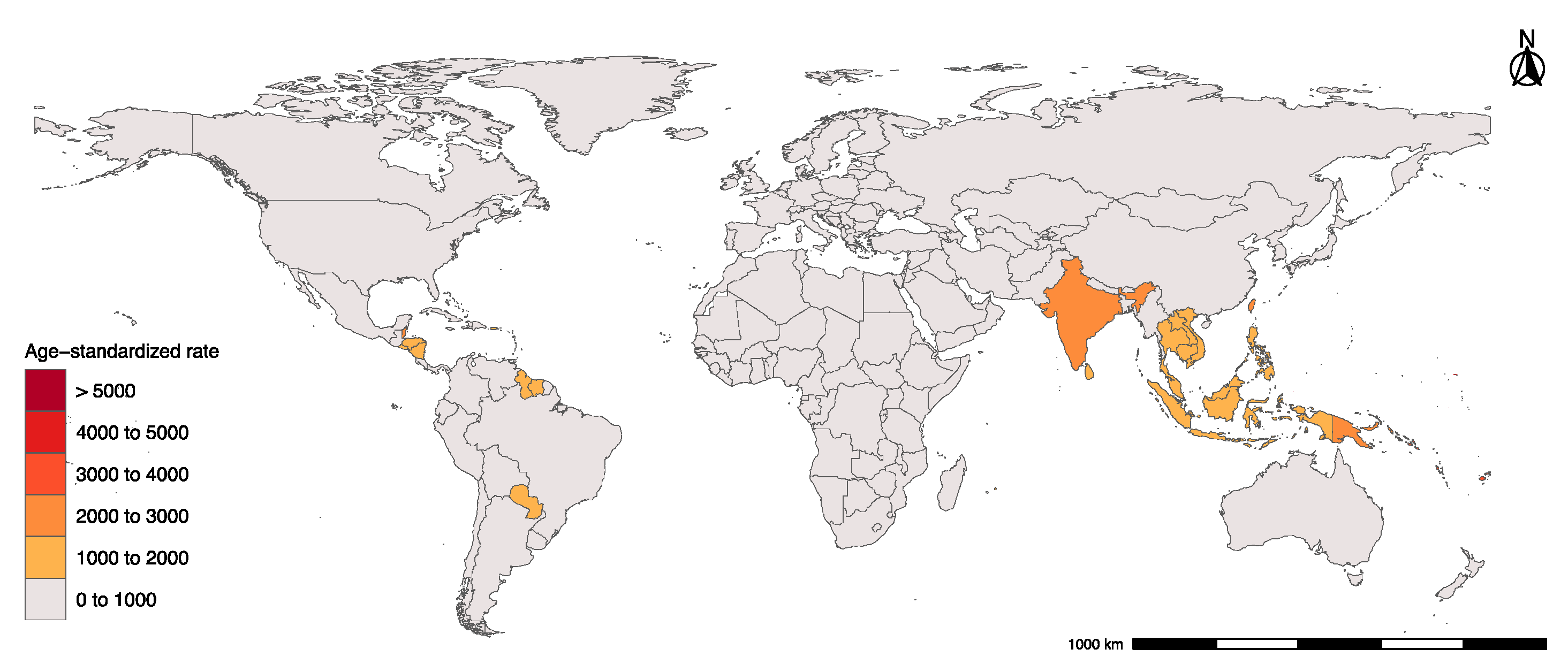
3.1. Global Dengue Incidence
3.2. Burden of Dengue in Three Major Endemic Regions
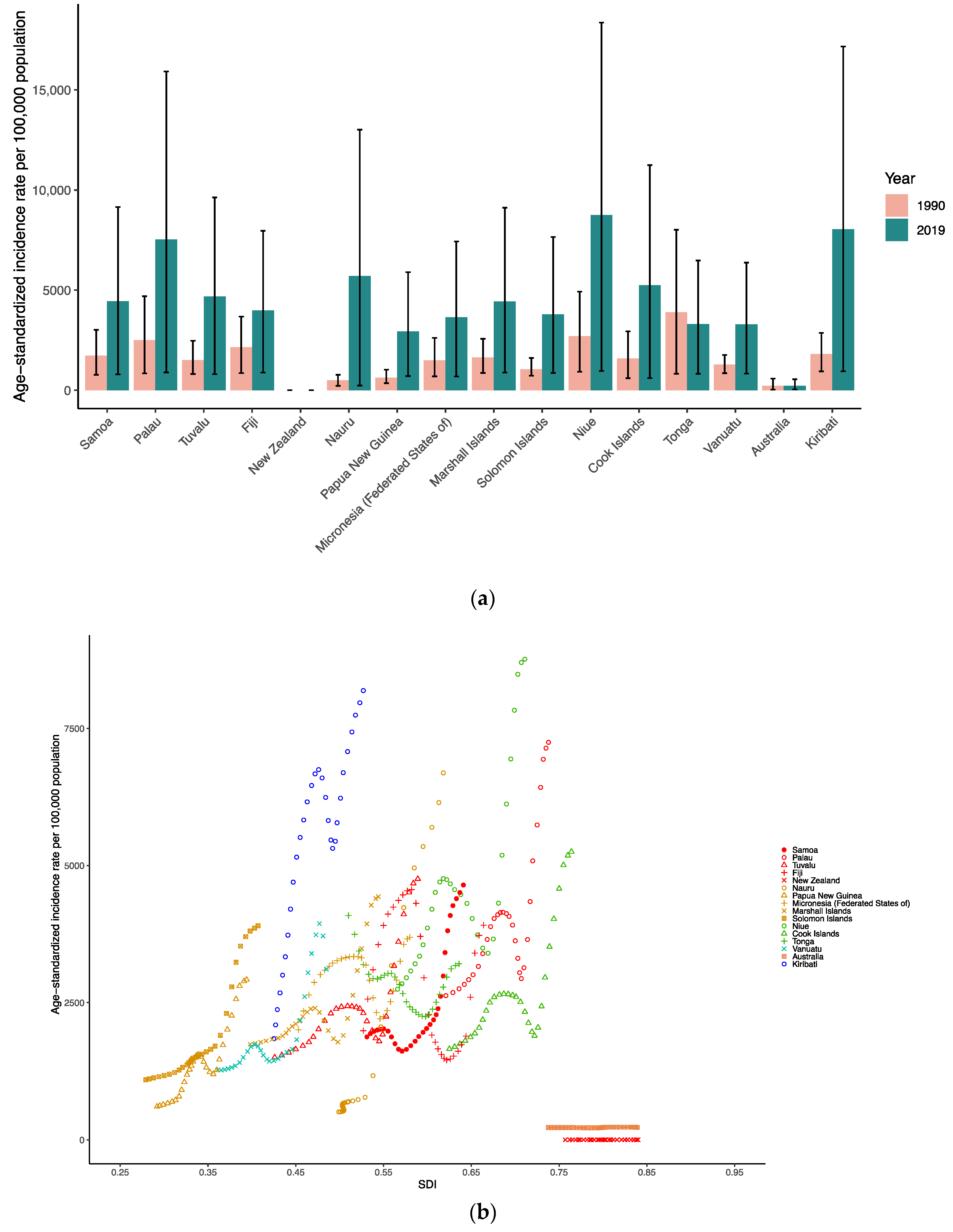
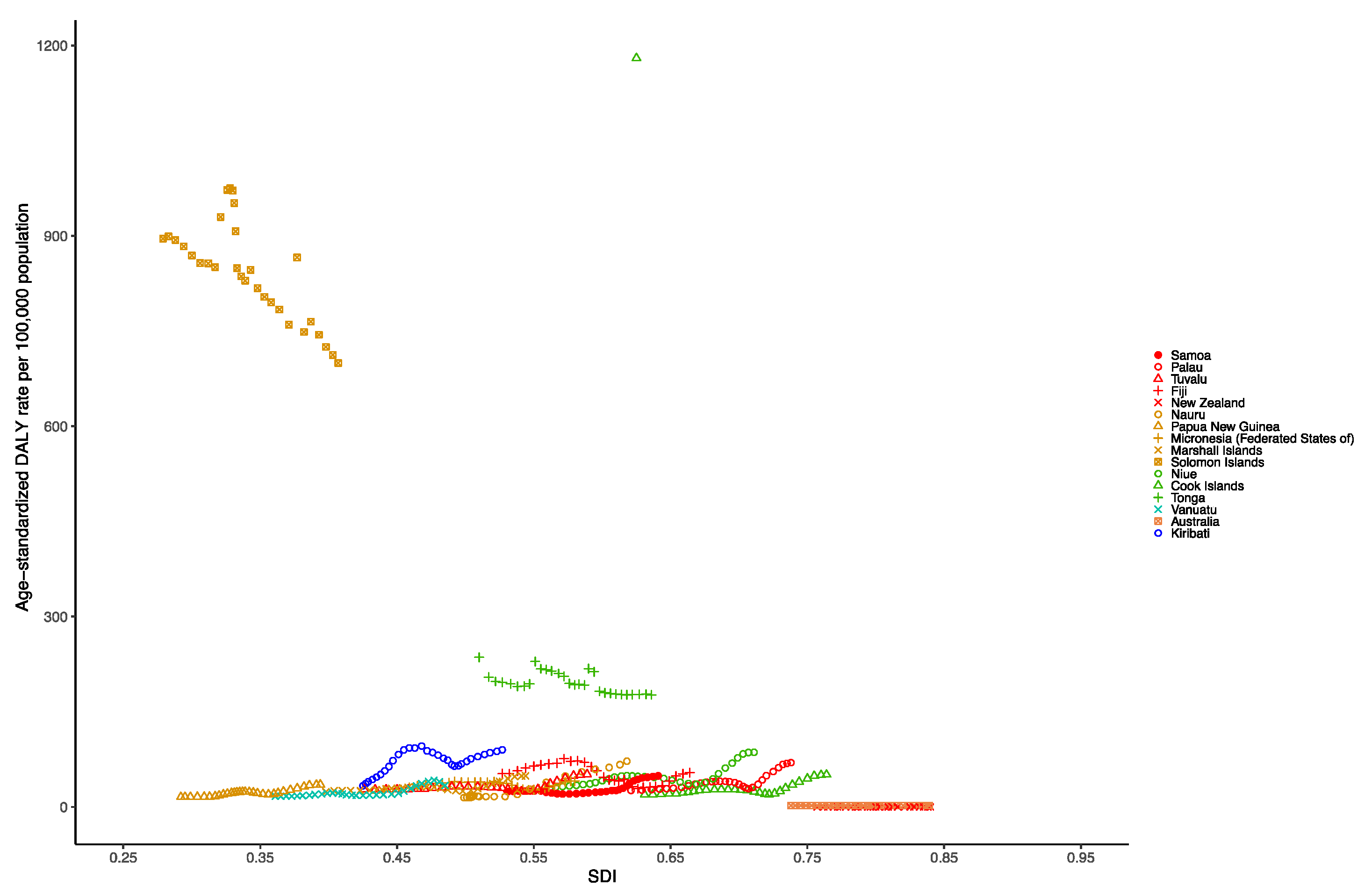
3.3. Oceania Dengue Burden
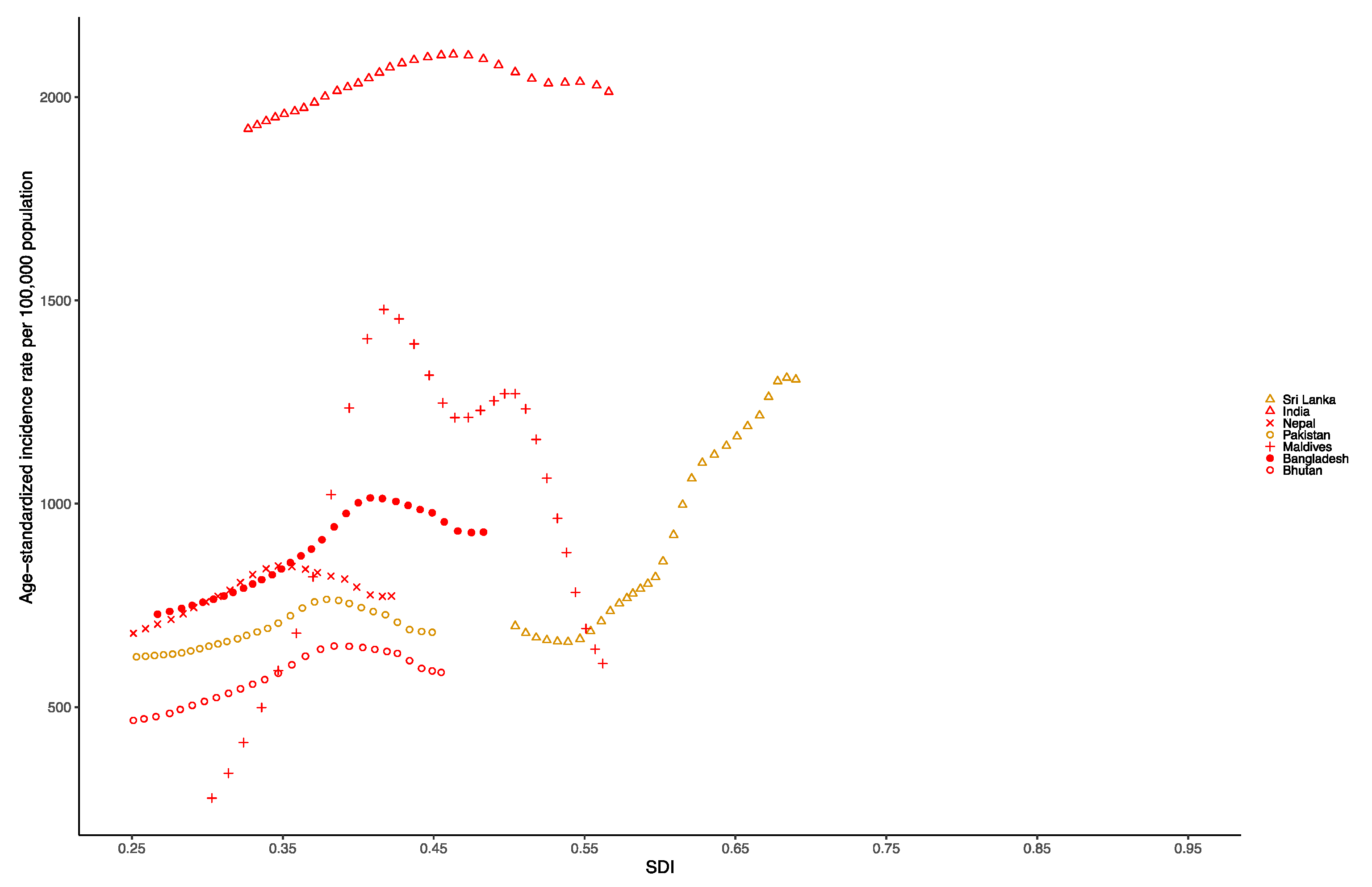
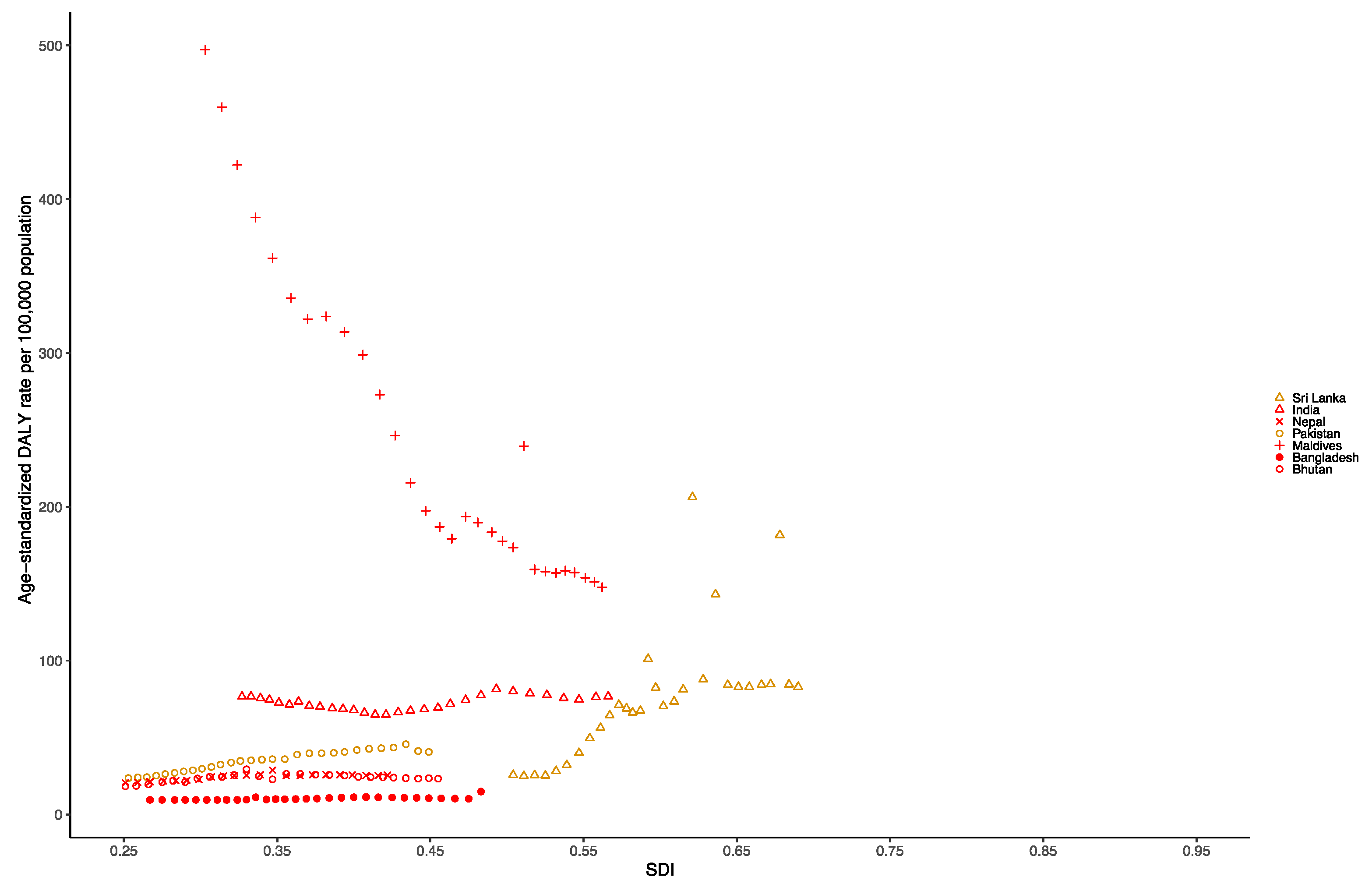
3.4. South Asia Dengue Burden
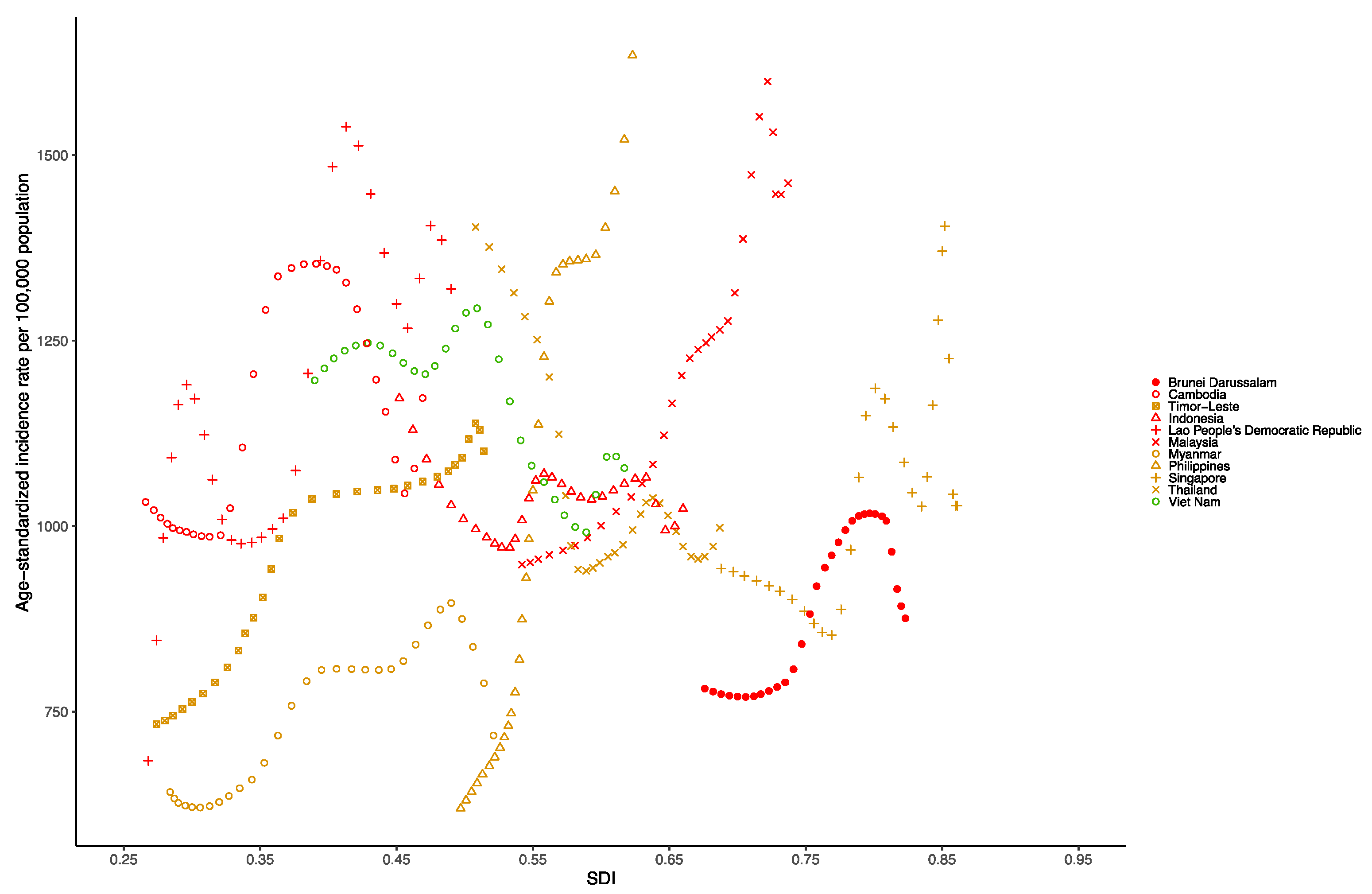
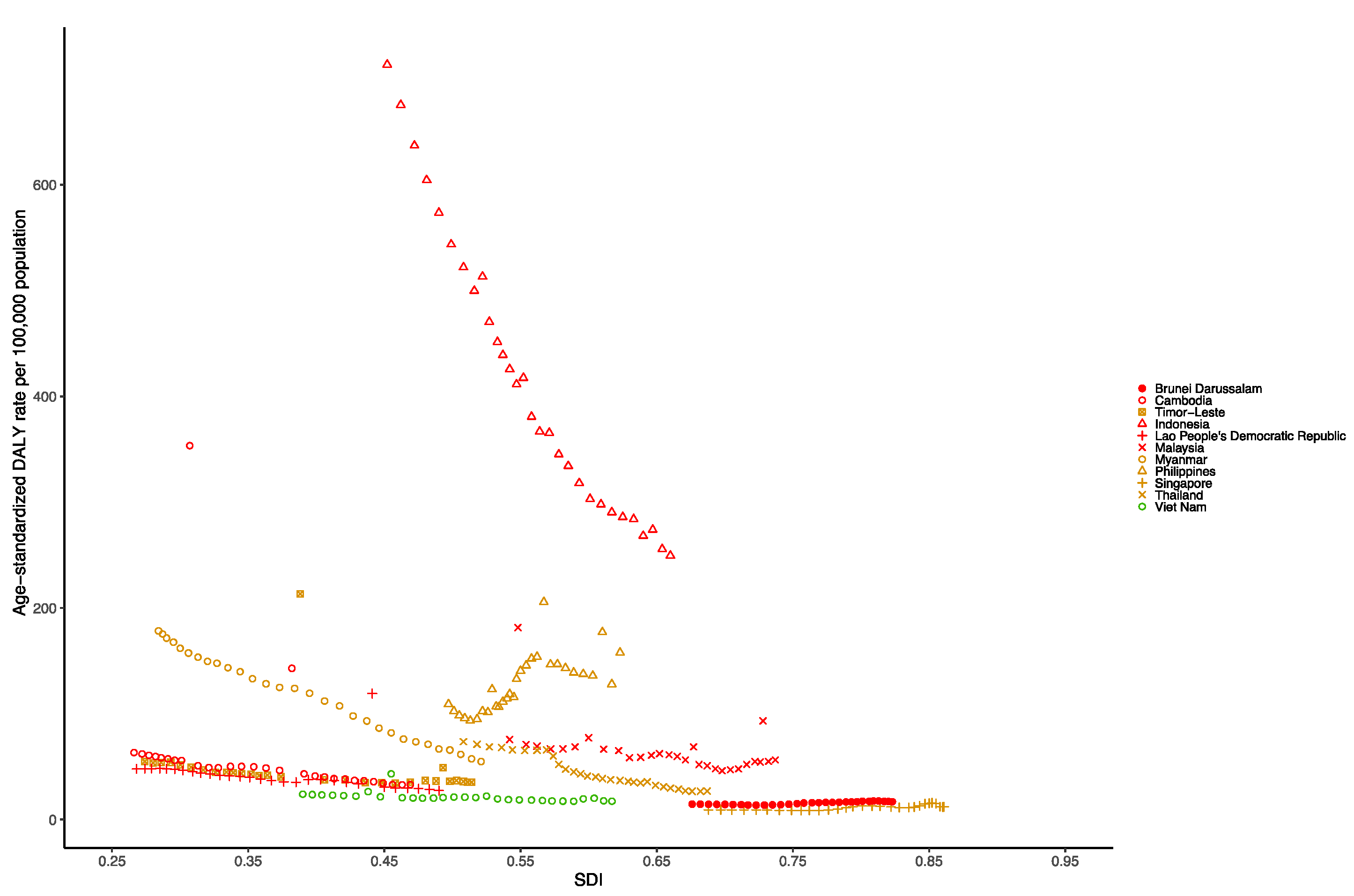
3.5. Southeast Asia Dengue Burden
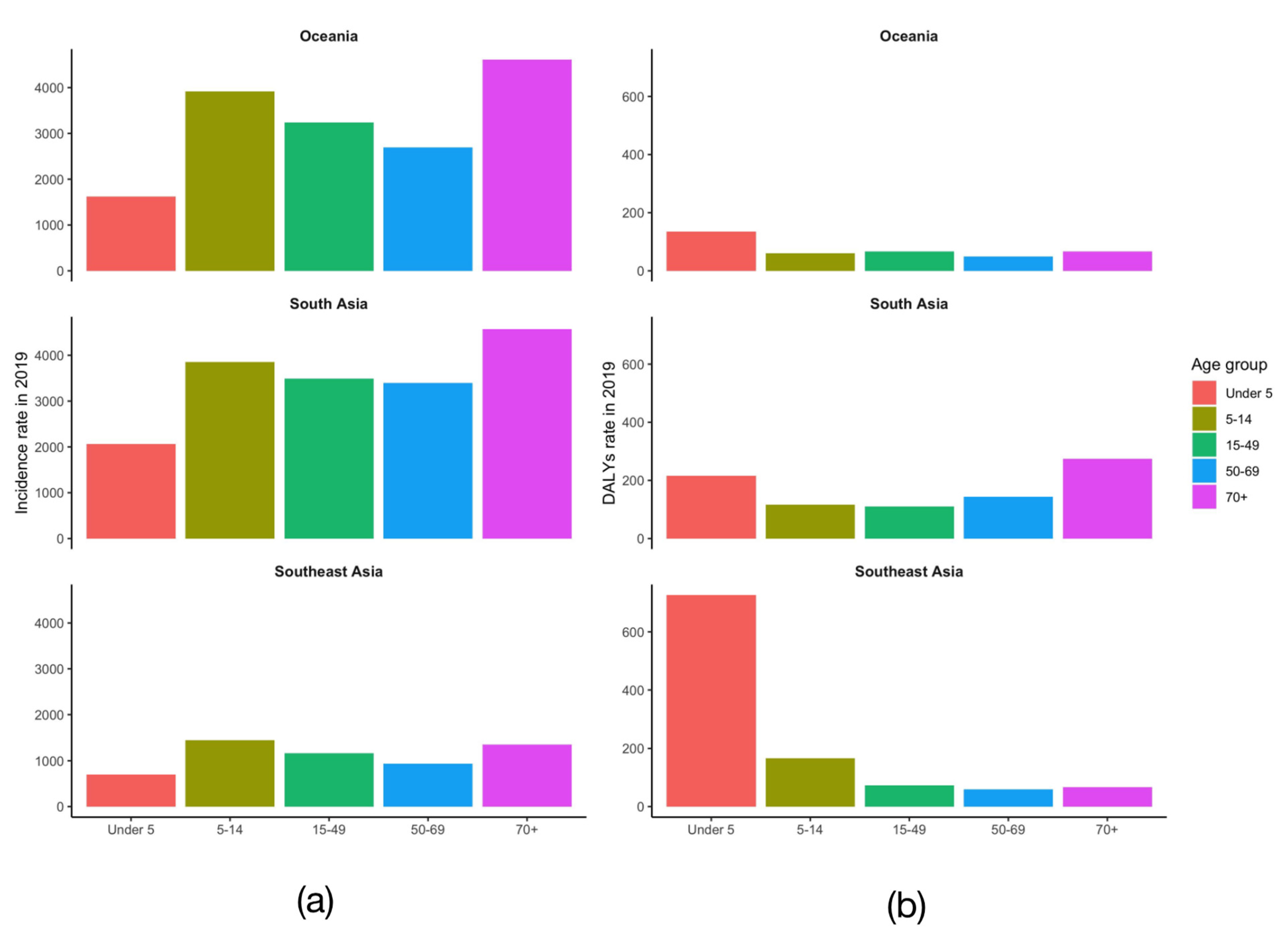
3.6. Age Distribution of Dengue Burden in Three Major Endemic Regions
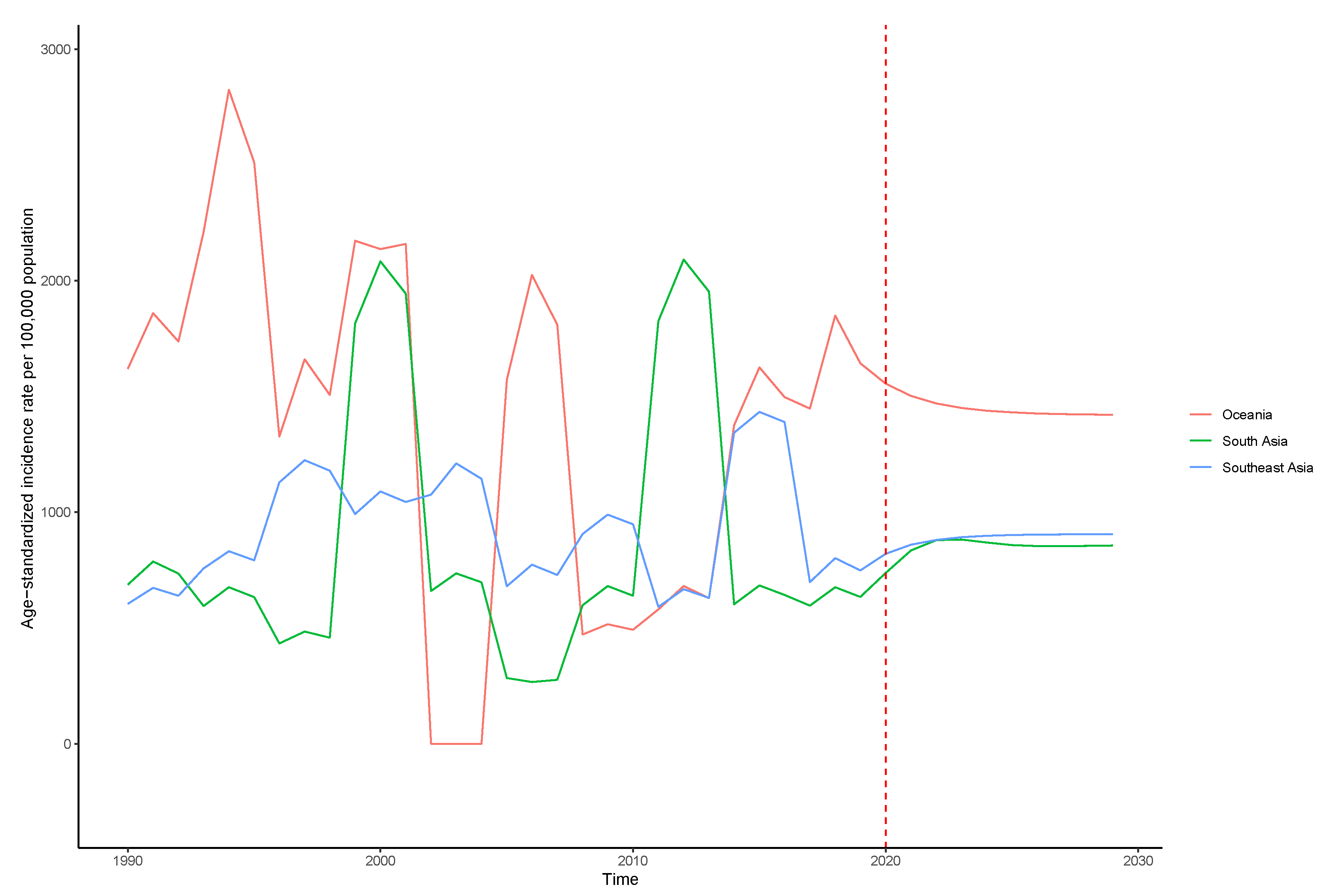
3.7. Prediction of the Incidence Trend of Dengue in Major Endemic Regions-Time Series Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Packierisamy, P.R.; Ng, C.-W.; Dahlui, M.; Inbaraj, J.; Balan, V.K.; Halasa, Y.A.; Shepard, D.S. Cost of Dengue Vector Control Activities in Malaysia. Am. J. Trop. Med. Hyg. 2015, 93, 1020–1027. [Google Scholar] [CrossRef]
- Guzman, M.G.; Harris, E. Dengue. Lancet 2015, 385, 453–465. [Google Scholar] [CrossRef]
- Katzelnick, L.C.; Coloma, J.; Harris, E. Dengue: Knowledge Gaps, Unmet Needs, and Research Priorities. Lancet Infect. Dis. 2017, 17, e88–e100. [Google Scholar] [CrossRef]
- Sang, S.; Wang, S.; Lu, L.; Bi, P.; Lv, M.; Liu, Q. The Epidemiological Characteristics and Dynamic Transmission of Dengue in China, 2013. PLoS Negl. Trop. Dis. 2016, 10, e0005095. [Google Scholar] [CrossRef]
- O’Driscoll, M.; Imai, N.; Ferguson, N.M.; Hadinegoro, S.R.; Satari, H.I.; Tam, C.C.; Dorigatti, I. Spatiotemporal Variability in Dengue Transmission Intensity in Jakarta, Indonesia. PLoS Negl. Trop. Dis. 2020, 14, e0008102. [Google Scholar] [CrossRef]
- Sarmiento-Senior, D.; Matiz, M.I.; Jaramillo-Gómez, J.F.; Olano, V.A.; Vargas, S.L.; Alexander, N.; Lenhart, A.; Stenström, T.A.; Overgaard, H.J. Knowledge, Attitudes, and Practices about Dengue among Pupils from Rural Schools in an Endemic Area in Colombia. Biomedica 2019, 39, 478–490. [Google Scholar] [CrossRef]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The Global Distribution and Burden of Dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- Tatem, A.J.; Hay, S.I.; Rogers, D.J. Global Traffic and Disease Vector Dispersal. Proc. Natl. Acad. Sci. USA 2006, 103, 6242–6247. [Google Scholar] [CrossRef]
- Idris, F.; Ting, D.H.R.; Alonso, S. An Update on Dengue Vaccine Development, Challenges, and Future Perspectives. Expert Opin. Drug Discov. 2021, 16, 47–58. [Google Scholar] [CrossRef]
- Getahun, A.; Batikawai, A.; Nand, D.; Khan, S.; Sahukhan, A.; Faktaufon, D. Dengue in Fiji: Epidemiology of the 2014 DENV-3 Outbreak. West. Pac. Surveill. Response J. 2019, 10, 31–38. [Google Scholar] [CrossRef]
- Costa, G.B.; Smithyman, R.; O’Neill, S.L.; Moreira, L.A. How to Engage Communities on a Large Scale? Lessons from World Mosquito Program in Rio de Janeiro, Brazil. Gates Open Res. 2020, 4, 109. [Google Scholar] [CrossRef]
- Suarez, G.P.; Udiani, O.; Allan, B.F.; Price, C.; Ryan, S.J.; Lofgren, E.; Coman, A.; Stone, C.M.; Gallos, L.K.; Fefferman, N.H. A Generic Arboviral Model Framework for Exploring Trade-Offs between Vector Control and Environmental Concerns. J. Theor. Biol. 2020, 490, 110161. [Google Scholar] [CrossRef]
- Hapuarachchi, H.C.; Koo, C.; Rajarethinam, J.; Chong, C.-S.; Lin, C.; Yap, G.; Liu, L.; Lai, Y.-L.; Ooi, P.L.; Cutter, J.; et al. Epidemic Resurgence of Dengue Fever in Singapore in 2013-2014: A Virological and Entomological Perspective. BMC Infect. Dis. 2016, 16, 300. [Google Scholar] [CrossRef]
- Ler, T.S.; Ang, L.W.; Yap, G.S.L.; Ng, L.C.; Tai, J.C.; James, L.; Goh, K.T. Epidemiological Characteristics of the 2005 and 2007 Dengue Epidemics in Singapore—Similarities and Distinctions. West. Pac. Surveill. Response J. 2011, 2, 24–29. [Google Scholar] [CrossRef]
- Koh, B.K.W.; Ng, L.C.; Kita, Y.; Tang, C.S.; Ang, L.W.; Wong, K.Y.; James, L.; Goh, K.T. The 2005 Dengue Epidemic in Singapore: Epidemiology, Prevention and Control. Ann. Acad. Med. Singap. 2008, 37, 538–545. [Google Scholar]
- Struchiner, C.J.; Rocklöv, J.; Wilder-Smith, A.; Massad, E. Increasing Dengue Incidence in Singapore over the Past 40 Years: Population Growth, Climate and Mobility. PLoS ONE 2015, 10, e0136286. [Google Scholar] [CrossRef]
- Low, S.-L.; Lam, S.; Wong, W.-Y.; Teo, D.; Ng, L.-C.; Tan, L.-K. Dengue Seroprevalence of Healthy Adults in Singapore: Serosurvey among Blood Donors, 2009. Am. J. Trop. Med. Hyg. 2015, 93, 40–45. [Google Scholar] [CrossRef]
- Halasa, Y.A.; Zambrano, B.; Shepard, D.S.; Dayan, G.H.; Coudeville, L. Economic Impact of Dengue Illness in the Americas. Am. J. Trop. Med. Hyg. 2011, 84, 200–207. [Google Scholar] [CrossRef]
- Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A. Economic and Disease Burden of Dengue in Southeast Asia. PLoS Negl. Trop. Dis. 2013, 7, e2055. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Coffeng, L.E.; Brady, O.J.; Hay, S.I.; Bedi, N.; Bensenor, I.M.; Castañeda-Orjuela, C.A.; et al. The Global Burden of Dengue: An Analysis from the Global Burden of Disease Study 2013. Lancet Infect. Dis. 2016, 16, 712–723. [Google Scholar] [CrossRef]
- Zeng, Z.; Zhan, J.; Chen, L.; Chen, H.; Cheng, S. Global, Regional, and National Dengue Burden from 1990 to 2017: A Systematic Analysis Based on the Global Burden of Disease Study 2017. eClinicalMedicine 2021, 32, 100712. [Google Scholar] [CrossRef]
- GBD 2016 Neurology Collaborators. Global, Regional, and National Burden of Neurological Disorders, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef]
- Weng, R.X.; Fu, H.L.; Zhang, C.L.; Ye, J.B.; Hong, F.C.; Chen, X.S.; Cai, Y.M. Time Series Analysis and Forecasting of Chlamydia Trachomatis Incidence Using Surveillance Data from 2008 to 2019 in Shenzhen, China. Epidemiol. Infect. 2020, 148, e76. [Google Scholar] [CrossRef]
- Beatty, M.E.; Beutels, P.; Meltzer, M.I.; Shepard, D.S.; Hombach, J.; Hutubessy, R.; Dessis, D.; Coudeville, L.; Dervaux, B.; Wichmann, O.; et al. Health Economics of Dengue: A Systematic Literature Review and Expert Panel’s Assessment. Am. J. Trop. Med. Hyg. 2011, 84, 473–488. [Google Scholar] [CrossRef]
- Mavian, C.; Dulcey, M.; Munoz, O.; Salemi, M.; Vittor, A.Y.; Capua, I. Islands as Hotspots for Emerging Mosquito-Borne Viruses: A One-Health Perspective. Viruses 2019, 11, 11. [Google Scholar] [CrossRef]
- Cao-Lormeau, V.-M. Tropical Islands as New Hubs for Emerging Arboviruses. Emerg. Infect. Dis. 2016, 22, 913–915. [Google Scholar] [CrossRef]
- Mayurasakorn, S.; Suttipun, N. The Impact of a Program for Strengthening Dengue Hemorrhagic Fever Case Management on the Clinical Outcome of Dengue Hemorrhagic Fever Patients. Southeast Asian J. Trop. Med. Public Health 2010, 41, 858–863. [Google Scholar]
- Whelan, P.I.; Kurucz, N.; Pettit, W.J.; Krause, V. Elimination of Aedes Aegypti in Northern Australia, 2004–2006. J. Vector Ecol. 2020, 45, 118–126. [Google Scholar] [CrossRef]
- Trewin, B.J.; Darbro, J.M.; Jansen, C.C.; Schellhorn, N.A.; Zalucki, M.P.; Hurst, T.P.; Devine, G.J. The Elimination of the Dengue Vector, Aedes Aegypti, from Brisbane, Australia: The Role of Surveillance, Larval Habitat Removal and Policy. PLoS Negl. Trop. Dis. 2017, 11, e0005848. [Google Scholar] [CrossRef]
- Ammar, S.E.; Mclntyre, M.; Swan, T.; Kasper, J.; Derraik, J.G.B.; Baker, M.G.; Hales, S. Intercepted Mosquitoes at New Zealand’s Ports of Entry, 2001 to 2018: Current Status and Future Concerns. Trop. Med. Infect. Dis. 2019, 4, 101. [Google Scholar] [CrossRef]
- Li, Y.; Kamara, F.; Zhou, G.; Puthiyakunnon, S.; Li, C.; Liu, Y.; Zhou, Y.; Yao, L.; Yan, G.; Chen, X.-G. Urbanization Increases Aedes Albopictus Larval Habitats and Accelerates Mosquito Development and Survivorship. PLoS Negl. Trop. Dis. 2014, 8, e3301. [Google Scholar] [CrossRef]
- Scott, T.W.; Clark, G.G.; Lorenz, L.H.; Amerasinghe, P.H.; Reiter, P.; Edman, J.D. Detection of Multiple Blood Feeding in Aedes Aegypti (Diptera: Culicidae) during a Single Gonotrophic Cycle Using a Histologic Technique. J. Med. Entomol. 1993, 30, 94–99. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Ooi, E.-E.; Horstick, O.; Wills, B. Dengue. Lancet 2019, 393, 350–363. [Google Scholar] [CrossRef]
- Hermida, M.J.; Perez Santangelo, A.; Calero, C.I.; Goizueta, C.; Espinosa, M.; Sigman, M. Learning-by-Teaching Approach Improves Dengue Knowledge in Children and Parents. Am. J. Trop. Med. Hyg. 2021, 105, 1536–1543. [Google Scholar] [CrossRef]
- Alim, M.; Ye, G.-H.; Guan, P.; Huang, D.-S.; Zhou, B.-S.; Wu, W. Comparison of ARIMA Model and XGBoost Model for Prediction of Human Brucellosis in Mainland China: A Time-Series Study. BMJ Open 2020, 10, e039676. [Google Scholar] [CrossRef]
- Liang, G.; Gao, X.; Gould, E.A. Factors Responsible for the Emergence of Arboviruses; Strategies, Challenges and Limitations for Their Control. Emerg. Microbes Infect. 2015, 4, e18. [Google Scholar] [CrossRef]
- Amelia-Yap, Z.H.; Chen, C.D.; Sofian-Azirun, M.; Low, V.L. Pyrethroid Resistance in the Dengue Vector Aedes Aegypti in Southeast Asia: Present Situation and Prospects for Management. Parasites Vectors 2018, 11, 332. [Google Scholar] [CrossRef]
- Dalpadado, R.; Gunathilaka, N.; Amarasinghe, D.; Udayanaga, L. A Challenge for a Unique Dengue Vector Control Programme: Assessment of the Spatial Variation of Insecticide Resistance Status amongst Aedes Aegypti and Aedes Albopictus Populations in Gampaha District, Sri Lanka. Biomed. Res. Int. 2021, 2021, 6619175. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | 1990 | 2019 | ||
|---|---|---|---|---|
| Incident Cases | ASR Per 100,000 | Incident Cases | ASR Per 100,000 | |
| No. X 105 (95%UI) | No. (95%UI) | No. X 105 (95%UI) | No. (95%UI) | |
| Overall | 306.7 (132.2–670.7) | 557.15 (243.32–1212.53) | 568.8 (370.8–1013.5) | 740.4 (478.2–1323.1) |
| Sex | ||||
| Male | 147.3 (63.6–319.3) | 532.1 (233.1–1151.8) | 274.8 (181.2–482.7) | 712.2 (466.5–1256.9) |
| Femal | 159.4 (66.6–347.8) | 584.3 (247.8–1273.1) | 294 (181.3–529.7) | 769.9 (469–1392.9) |
| Sociodemographic index | ||||
| Low | 34.9 (15.3–96.4) | 674.4 (312.1–1861.22) | 67.6 (28.8–175.5) | 619.51 (283.41–1614.6) |
| Low-middle | 150.3 (41.7–426.1) | 1337.13 (383.83–3760.47) | 231.1 (98.4–571.5) | 1317.83 (554.94–3275.4) |
| Middle | 92.2 (54.7–181.9) | 532.06 (320.61–1036.57) | 186 (145.5–344.7) | 787.68 (616.02–1474.61) |
| High-middle | 24.8 (14–66.7) | 214.76 (120.51–579.03) | 69.7 (34.7–110.4) | 522.75 (261.31–859.96) |
| High | 4.3 (3.5–5.2) | 54.69 (43.12–66.82) | 9 (6–12.9) | 91.79 (61.91–131.49) |
| Regions | ||||
| High-income Asia Pacific | 0.3 (0.2–0.5) | 17.95 (11.69–27.62) | 0.6 (0.5–0.8) | 36.75 (27.11–50.8) |
| Central Asia | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| East Asia | 18.2 (14.7–21.6) | 148.91 (122.43–176.25) | 67.1 (24–126.2) | 494.33 (173.26–942.48) |
| South Asia | 180.7 (46.6–464.3) | 1663.51 (444.97–4250.09) | 312.4 (120.5–765) | 1740.79 (660.93–4287.12) |
| Southeast Asia | 48.9 (27.7–129.4) | 1036.23 (600.63–2682.51) | 77 (70–85.6) | 1153.57 (1049.49–1281.59) |
| Australasia | 0.4 (0.1–1) | 185.77 (25.62–483.21) | 0.6 (0.1–1.4) | 188.65 (34.24–466.29) |
| Caribbean | 2.9 (1.9–4) | 819.65 (560.26–1141.61) | 3.5 (2–5.4) | 747.08 (427.62–1140.19) |
| Central Europe | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Eastern Europe | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Western Europe | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Andean Latin America | 1.7 (1–2.6) | 455.98 (299.54–665.71) | 4 (3.3–4.9) | 632.56 (518.08–754.08) |
| Central Latin America | 11.5 (10.5–12.6) | 713.32 (633.97–797.16) | 19.4 (16.3–22.6) | 771.16 (651.56–892.79) |
| Southern Latin America | 0.7 (0.1–1.9) | 151.83 (26.41–381.95) | 1.1 (0.4–2.5) | 167.41 (51.67–376.2) |
| Tropical Latin America | 10.9 (7.3–14.8) | 710.56 (481.73–959.89) | 22.3 (19.7–24.8) | 990.1 (891.27–1089.11) |
| North Africa and Middle East | 3.4 (0.5–7.4) | 100.95 (20.62–209.55) | 7 (0.9–15) | 115.37 (17.71–242.93) |
| High-income North America | 0.1 (0.1–0.2) | 4.98 (3.56–6.36) | 0.2 (0.2–0.3) | 6.44 (4.61–8.32) |
| Oceania | 0.6 (0.5–0.7) | 1009.45 (793.94–1198.93) | 4.2 (1–8.2) | 3173.48 (762.33–6161.18) |
| Central Sub-Saharan Africa | 3.4 (1.6–5.5) | 617.81 (313.33–989.16) | 6.8 (2–12.7) | 539.27 (197.31–961.59) |
| Eastern Sub-Saharan Africa | 8.2 (3.9–12.8) | 435.67 (221.9–671.89) | 15.7 (4.6–27.8) | 382.19 (121.33–666.8) |
| Southern Sub-Saharan Africa | 0.3 (0.2–0.6) | 59.7 (33.39–106.06) | 0.4 (0.1–0.9) | 48.63 (13.05–111.58) |
| Western Sub-Saharan Africa | 14.5 (8.7–20.3) | 769.29 (484.42–1055.63) | 26.3 (6.3–47.5) | 606.75 (201.38–1033.46) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, N.; Zheng, J.-X.; Guo, Z.-Y.; Li, L.-H.; Xia, S.; Lv, S.; Zhou, X.-N. Dengue Incidence Trends and Its Burden in Major Endemic Regions from 1990 to 2019. Trop. Med. Infect. Dis. 2022, 7, 180. https://doi.org/10.3390/tropicalmed7080180
Tian N, Zheng J-X, Guo Z-Y, Li L-H, Xia S, Lv S, Zhou X-N. Dengue Incidence Trends and Its Burden in Major Endemic Regions from 1990 to 2019. Tropical Medicine and Infectious Disease. 2022; 7(8):180. https://doi.org/10.3390/tropicalmed7080180
Chicago/Turabian StyleTian, Na, Jin-Xin Zheng, Zhao-Yu Guo, Lan-Hua Li, Shang Xia, Shan Lv, and Xiao-Nong Zhou. 2022. "Dengue Incidence Trends and Its Burden in Major Endemic Regions from 1990 to 2019" Tropical Medicine and Infectious Disease 7, no. 8: 180. https://doi.org/10.3390/tropicalmed7080180