
The Use of Proton Pump Inhibitors and COVID-19: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction and Assessment of Study Quality
2.4. Statistical Analysis
3. Results
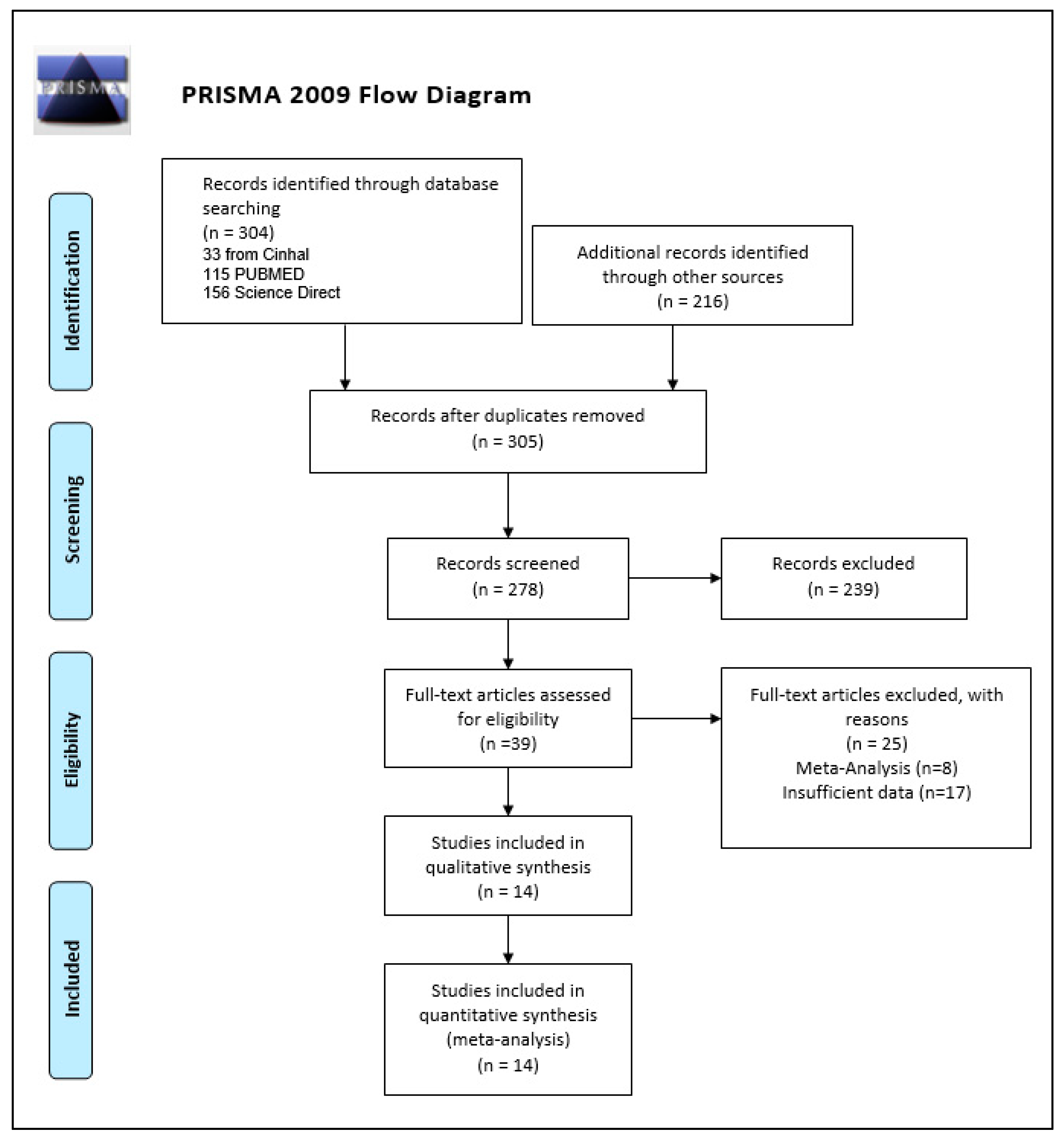
3.1. Search Result
3.2. Study Characteristics and Quality Assessment
3.3. Outcomes
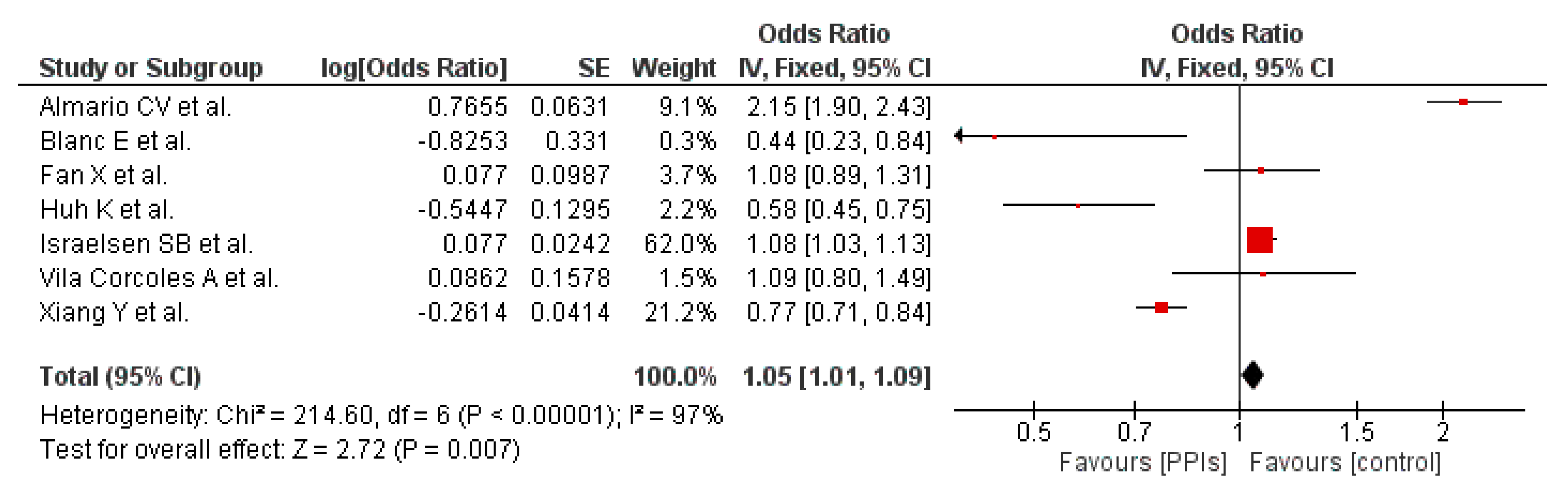
3.3.1. PPI Usage and Susceptibility to COVID-19
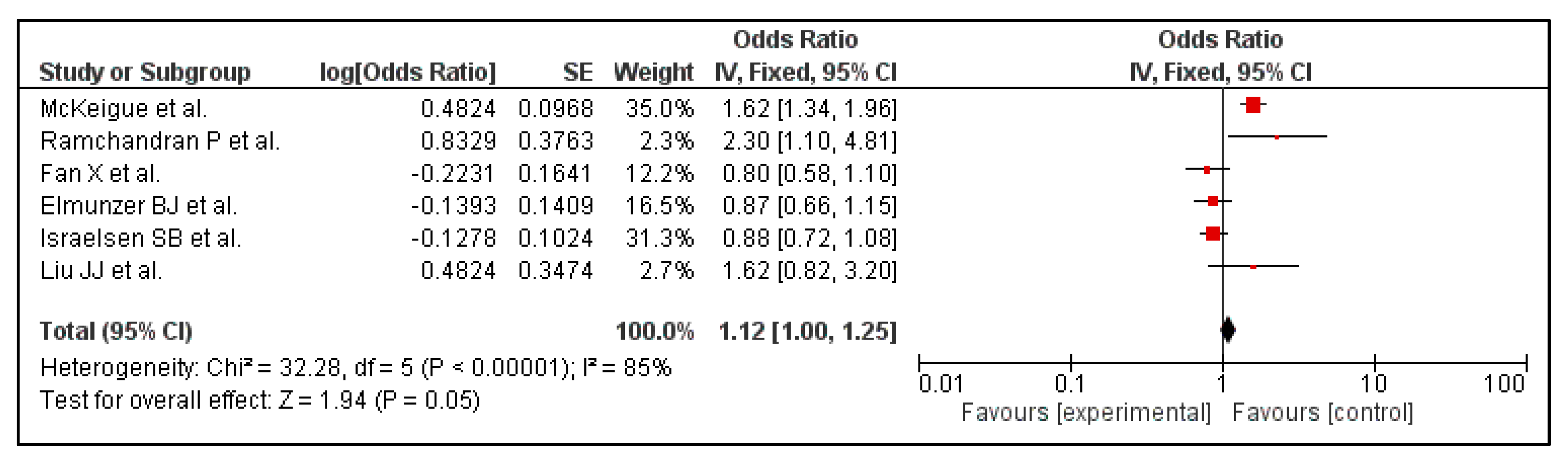
3.3.2. PPI Usage and Composite Poor Outcome
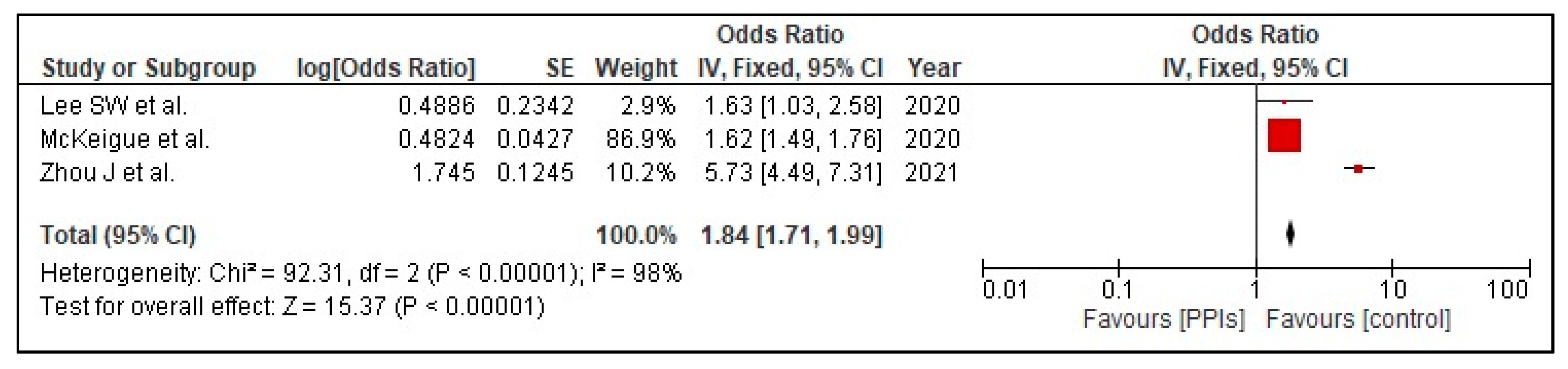
3.3.3. PPI Usage and Mortality
3.4. Publication Bias
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- COVID Live-Coronavirus Statistics-Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 20 February 2022).
- Morán Blanco, J.I.; Alvarenga Bonilla, J.A.; Homma, S.; Suzuki, K.; Fremont-Smith, P.; Villar Gómez de Las Heras, K. Antihistamines and azithromycin as a treatment for COVID-19 on primary health care-A retrospective observational study in elderly patients. Pulm. Pharmacol. Ther. 2021, 67, 101989. [Google Scholar] [CrossRef] [PubMed]
- Usman, M.S.; Siddiqi, T.J.; Khan, M.S.; Ahmed, A.; Ali, S.S.; Michos, E.D.; Hall, M.E.; Krasuski, R.A.; Greene, S.J.; Butler, J.; et al. A Meta-analysis of the Relationship Between Renin-Angiotensin-Aldosterone System Inhibitors and COVID-19. Am. J. Cardiol. 2020, 130, 159–161. [Google Scholar] [CrossRef]
- Adir, Y.; Humbert, M.; Saliba, W. COVID-19 risk and outcomes in adult asthmatic patients treated with biologics or systemic corticosteroids: Nationwide real-world evidence. J. Allergy Clin. Immunol. 2021, 148, 361–367.e13. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk factors for severe disease and death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sattar, N.; Valabhji, J. Obesity as a Risk Factor for Severe COVID-19: Summary of the Best Evidence and Implications for Health Care. Curr. Obes. Rep. 2021, 10, 282–289. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, H.; Du, H.; Ma, R.; Nan, Y.; Zhang, T. Risk Factors for COVID-19 in Patients with Hypertension. Can. J. Infect. Dis. Med. Microbiol. J. Can. Mal. Infect. Microbiol. Med. 2021, 2021, 5515941. [Google Scholar] [CrossRef]
- Ksiądzyna, D.; Szeląg, A.; Paradowski, L. Overuse of proton pump inhibitors. Pol. Arch. Med. Wewn. 2015, 125, 289–298. [Google Scholar] [CrossRef]
- Charpiat, B.; Bleyzac, N.; Tod, M. Proton Pump Inhibitors are Risk Factors for Viral Infections: Even for COVID-19? Clin. Drug Investig. 2020, 40, 897–899. [Google Scholar] [CrossRef]
- Li, T.; Xie, Y.; Al-Aly, Z. The association of proton pump inhibitors and chronic kidney disease: Cause or confounding? Curr. Opin. Nephrol. Hypertens. 2018, 27, 182–187. [Google Scholar] [CrossRef]
- Haastrup, P.F.; Thompson, W.; Søndergaard, J.; Jarbøl, D.E. Side Effects of Long-Term Proton Pump Inhibitor Use: A Review. Basic Clin. Pharmacol. Toxicol. 2018, 123, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Caplin, M.; Khan, K.; Savage, K.; Rode, J.; Varro, A.; Michaeli, D.; Grimes, S.; Brett, B.; Pounder, R.; Dhillon, A. Expression and processing of gastrin in hepatocellular carcinoma, fibrolamellar carcinoma and cholangiocarcinoma. J. Hepatol. 1999, 30, 519–526. [Google Scholar] [CrossRef]
- Cavalcoli, F.; Zilli, A.; Conte, D.; Ciafardini, C.; Massironi, S. Gastric neuroendocrine neoplasms and proton pump inhibitors: Fact or coincidence? Scand. J. Gastroenterol. 2015, 50, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Wahlin, K.; Engstrand, L.; Lagergren, J. Maintenance therapy with proton pump inhibitors and risk of gastric cancer: A nationwide population-based cohort study in Sweden. BMJ Open 2017, 7, e017739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Israelsen, S.B.; Ernst, M.T.; Lundh, A.; Lundbo, L.F.; Sandholdt, H.; Hallas, J.; Benfield, T. Proton Pump Inhibitor Use Is Not Strongly Associated With SARS-CoV-2 Related Outcomes: A Nationwide Study and Meta-analysis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2021, 19, 1845–1854.e6. [Google Scholar] [CrossRef] [PubMed]
- Almario, C.V.; Chey, W.D.; Spiegel, B.M.R. Increased Risk of COVID-19 Among Users of Proton Pump Inhibitors. Am. J. Gastroenterol. 2020, 115, 1707–1715. [Google Scholar] [CrossRef]
- Xiang, Y.; Wong, K.C.-Y.; So, H.-C. Exploring Drugs and Vaccines Associated with Altered Risks and Severity of COVID-19: A UK Biobank Cohort Study of All ATC Level-4 Drug Categories Reveals Repositioning Opportunities. Pharmaceutics 2021, 13, 1514. [Google Scholar] [CrossRef]
- Ramachandran, P.; Perisetti, A.; Gajendran, M.; Jean-Louis, F.; Bansal, P.; Dwivedi, A.K.; Goyal, H. Pre-hospitalization proton pump inhibitor use and clinical outcomes in COVID-19. Eur. J. Gastroenterol. Hepatol. 2020, 34, 137–141. [Google Scholar] [CrossRef]
- Fan, X.; Liu, Z.; Miyata, T.; Dasarathy, S.; Rotroff, D.M.; Wu, X.; Poulsen, K.L.; Nagy, L.E. Effect of Acid Suppressants on the Risk of COVID-19: A Propensity Score-Matched Study Using UK Biobank. Gastroenterology 2021, 160, 455–458.e5. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 62, e1–e34. [Google Scholar]
- Strategy, S. Supplementary Table 1. Search Strategy Used in Each Database Searched. 2019. Available online: https://www.ijhpm.com/jufile?ar_sfile=44803 (accessed on 4 November 2021).
- Elmunzer, B.J.; Wolf, B.J.; Scheiman, J.M.; Tierney, W.M.; Taylor, J.R. Association Between Preadmission Acid Suppressive Medication Exposure and Severity of Illness in Patients Hospitalized With COVID-19. Gastroenterology 2021, 160, 1417–1422.e14. [Google Scholar] [CrossRef]
- Lee, S.W.; Ha, E.K.; Yeniova, A.Ö.; Moon, S.Y.; Kim, S.Y.; Koh, H.Y.; Yang, J.M.; Jeong, S.J.; Moon, S.J.; Cho, J.Y.; et al. Severe clinical outcomes of COVID-19 associated with proton pump inhibitors: A nationwide cohort study with propensity score matching. Gut 2021, 70, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.; Sloan, M.E.; Owings, A.H.; Figgins, E.; Gauthier, J.; Gharaibeh, R.; Robinson, T.; Williams, H.; Sindel, C.B.; Backus, F.; et al. Increased ACE2 Levels and Mortality Risk of Patients With COVID-19 on Proton Pump Inhibitor Therapy. Am. J. Gastroenterol. 2021, 116, 1638–1645. [Google Scholar] [CrossRef]
- Lee, S.W.; Yang, J.M.; Yoo, I.K.; Moon, S.Y.; Ha, E.K.; Yeniova, A.Ö.; Cho, J.Y.; Kim, M.S.; Shin, J.I.; Yon, D.K. Proton pump inhibitors and the risk of severe COVID-19: A post-hoc analysis from the Korean nationwide cohort. Gut 2021, 70, 2013–2015. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wang, X.; Lee, S.; Wu, W.K.K.; Cheung, B.M.Y.; Zhang, Q.; Tse, G. Proton pump inhibitor or famotidine use and severe COVID-19 disease: A propensity score-matched territory-wide study. Gut 2021, 70, 2012–2013. [Google Scholar] [CrossRef] [PubMed]
- McKeigue, P.M.; Kennedy, S.; Weir, A.; Bishop, J.; McGurnaghan, S.J.; McAllister, D.; Robertson, C.; Wood, R.; Lone, N.; Murray, J.; et al. Relation of severe COVID-19 to polypharmacy and prescribing of psychotropic drugs: The REACT-SCOT case-control study. BMC Med. 2021, 19, 51. [Google Scholar] [CrossRef] [PubMed]
- Blanc, F.; Waechter, C.; Vogel, T.; Schorr, B.; Demuynck, C.; Martin-Hunyadi, C.; Meyer, M.; Mutelica, D.; Bougaa, N.; Fafi-Kremer, S.; et al. Interest of Proton Pump Inhibitors in Reducing the Occurrence of COVID-19: A Case-Control Study. Preprints 2020, 2020050016. [Google Scholar] [CrossRef]
- Huh, K.; Ji, W.; Kang, M.; Hong, J.; Bae, G.H.; Lee, R.; Na, Y.; Choi, H.; Gong, S.Y.; Jung, J. Association of previous medications with the risk of COVID-19: A nationwide claims-based study from South Korea. MedRxiv 2020, 1–24. [Google Scholar] [CrossRef]
- Vila-Corcoles, A.; Satue-Gracia, E.; Ochoa-Gondar, O.; Torrente-Fraga, C.; Gomez-Bertomeu, F.; Vila-Rovira, A.; Hospital-Guardiola, I.; de Diego-Cabanes, C.; Bejarano-Romero, F.; Rovira-Veciana, D.; et al. Use of distinct anti-hypertensive drugs and risk for COVID-19 among hypertensive people: A population-based cohort study in Southern Catalonia, Spain. J. Clin. Hypertens. 2020, 22, 1379–1388. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, version 6.2 (updated February 2021); Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 7 November 2021).
- Thornton, A.; Lee, P. Publication bias in meta-analysis: Its causes and consequences. J. Clin. Epidemiol. 2000, 53, 207–216. [Google Scholar] [CrossRef]
- Pranata, R.; Huang, I.; Lawrensia, S.; Henrina, J.; Lim, M.A.; Lukito, A.A.; Kuswardhani, R.A.T.; Wibawa, I.D.N. Proton pump inhibitor on susceptibility to COVID-19 and its severity: A systematic review and meta-analysis. Pharmacol. Rep. 2021, 73, 1642–1649. [Google Scholar] [CrossRef] [PubMed]
- Hariyanto, T.I.; Prasetya, I.B.; Kurniawan, A. Proton pump inhibitor use is associated with increased risk of severity and mortality from coronavirus disease 2019 (COVID-19) infection. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver. 2020, 52, 1410–1412. [Google Scholar] [CrossRef]
- Price, E.; Treacher, D.F. Reduced gastric acidity, proton pump inhibitors and increased severity of COVID-19 infections. Crit. Care. 2021, 25, 73. [Google Scholar] [CrossRef] [PubMed]
- Trifan, A.; Stanciu, C.; Girleanu, I.; Stoica, O.C.; Singeap, A.M.; Maxim, R.; Chiriac, S.A.; Ciobica, A.; Boiculese, L. Proton pump inhibitors therapy and risk of Clostridium difficile infection: Systematic review and meta-analysis. World J. Gastroenterol. 2017, 23, 6500–6515. [Google Scholar] [CrossRef]
- Arendse, L.B.; Danser, A.H.J.; Poglitsch, M.; Touyz, R.M.; Burnett, J.C.J.; Llorens-Cortes, C.; Ehlers, M.R.; Sturrock, E.D. Novel Therapeutic Approaches Targeting the Renin-Angiotensin System and Associated Peptides in Hypertension and Heart Failure. Pharmacol. Rev. 2019, 71, 539–570. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Sultan, N.; Nazareno, J.; Gregor, J. Association between proton pump inhibitors and respiratory infections: A systematic review and meta-analysis of clinical trials. Can. J. Gastroenterol. 2008, 22, 761–766. [Google Scholar] [CrossRef]
- Biswas, S.; Benedict, S.H.; Lynch, S.G.; LeVine, S.M. Potential immunological consequences of pharmacological suppression of gastric acid production in patients with multiple sclerosis. BMC Med. 2012, 10, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palencia-Herrejón, E.; Sánchez, B.; Escobar, I.; Gómez-Lus, M.L. Proton pump inhibitors and infection risk. Rev. Esp. Quimioter. Publ. Of. Soc. Esp. Quimioter. 2011, 24, 4–12. [Google Scholar]
- Laheij, R.J.F.; Sturkenboom, M.C.J.M.; Hassing, R.-J.; Dieleman, J.; Stricker, B.H.C.; Jansen, J.B.M.J. Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA 2004, 292, 1955–1960. [Google Scholar] [CrossRef]
- Ghebremariam, Y.T.; Cooke, J.P.; Gerhart, W.; Griego, C.; Brower, J.B.; Doyle-Eisele, M.; Moeller, B.C.; Zhou, Q.; Ho, L.; de Andrade, J.; et al. Pleiotropic effect of the proton pump inhibitor esomeprazole leading to suppression of lung inflammation and fibrosis. J. Transl. Med. 2015, 13, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zedtwitz-Liebenstein, K.; Wenisch, C.; Patruta, S.; Parschalk, B.; Daxböck, F.; Graninger, W. Omeprazole treatment diminishes intra- and extracellular neutrophil reactive oxygen production and bactericidal activity. Crit. Care Med. 2002, 30, 1118–1122. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-H.; Chang, Y.-S.; Lin, T.-M.; Hu, L.-F.; Hou, T.-Y.; Hsu, H.-C.; Shen, Y.-C.; Kuo, P.-I.; Chen, W.-S.; Lin, Y.-C.; et al. Proton Pump Inhibitors Increase the Risk of Autoimmune Diseases: A Nationwide Cohort Study. Front. Immunol. 2021, 12, 736036. [Google Scholar] [CrossRef]
- Imhann, F.; Bonder, M.J.; Vila, A.V.; Fu, J.; Mujagic, Z.; Vork, L.; Tigchelaar, E.F.; Jankipersadsing, S.A.; Cenit, M.C.; Harmsen, H.J.M.; et al. Proton pump inhibitors affect the gut microbiome. Gut 2016, 65, 740–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgibbon, G.; Mills, K.H.G. The microbiota and immune-mediated diseases: Opportunities for therapeutic intervention. Eur. J. Immunol. 2020, 50, 326–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year [Reference] from, Study Location | Study Design and Setting | No. of COVID-19 Tested Positive Patients | Exposure | Primary Outcome(s) |
|---|---|---|---|---|
| Elmunzer BJ et al., 2021 [22]; North America | Cohort | 1846 | PPI use within 1 month (after hospital admission) | Lack of association between PPI use and severity; No association between use of PPI and mortality |
| Almario CV et al., 2020 [16]; USA | Cohort | 3386 | PPI use once daily, and PPI use twice daily | Lack of association between PPI use and severity; No association between use of PPI and mortality |
| Lee SW et al., 2020 [23]; Korea | Cohort | 4785 | Current PPI use (within 90 days before the first positive SARS-CoV-2 RNA test and before hospitalization) | Severity (higher dose-PPI use and posthospitalization PPI use was significantly associated with severe COVID-19 symptoms) |
| Israelsen SB et al., 2021 [15]; Denmark | CaseControl | 4473 | Current PPI use (within 90 days before the first positive SARS-CoV-2 RNA test and before hospitalization) | Severity (hospital admission but not severe outcomes); No association found between PPI use and mortality |
| Liu JJ et al., 2021 [24]; MississiPPI | Cohort | 56 | PPI use once daily; PPI use twice daily | Mortality |
| Fan X et al., 2021 [19]; United Kingdom | Cohort | 9469 | PPI use (unspecified) | No significant association found between PPI use and mortality |
| Lee SW et al., 2020 [25]; Korea | Cohort | 4785 | Current PPI use and past PPI use | Composite endpoint 1 (requirement of oxygen therapy, intensive care unit admission, administration of invasive ventilation, or death); Composite endpoint 2 (severed clinical outcomes of COVID-19, intensive care unit admission, administration of invasive ventilation, or death) |
| Zhou J et al., 2021 [26]; China | Cohort | 4445 | Current PPI use and past PPI use | Severity |
| Ramchandran et al., 2020 [18]; USA | Cohort | 295 | PPI use (unspecified) | Severity (risk for developing acute respiratory distress syndrome); Mortality |
| McKeigue PM et al., 2020 [27]; Scotland | Matched Case Control | 4251 | Average daily doses of proton pump inhibitors | Severity and mortality (dose-response relationship was strongest in those PPI users aged less than 75 years) |
| Blanc F et al., 2020 [28], France | Retrospective CaseControl | 89 | Current PPI use and past PPI use | COVID-19 incidence (PPI use lowered the risk of COVID-19 infection) |
| Huh K et al., 2020 [29]; Korea | Case Control | 7341 | Past PPI use | No significant association found between PPI use and COVID-19 infection |
| Xiang Y et al., 2021 [17], China | Cohort | 397,000 | Current PPI use and past PPI use | Risk of COVID-19 Infection, severity, and mortality; Protective association between PPI use and COVID-19 |
| Vila-Corcoles A et al., 2021 [30], Spain | Cohort | 34,936 | Current PPI use | No significant association found between PPI use and COVID-19 infection |
| Study | Total Patients | Age | Males | Hypertension | Diabetes | Cardiovascular Disease | Renal Disease | Respiratory Disease |
|---|---|---|---|---|---|---|---|---|
| Elmunzer BJ et al., 2021 [22]; North America | 1846 | Mean 59.9 SD 16.4 | 1044 (56.6%) | 1146 (62.1%) | 658 (35.6%) | 478 (25.9%) | 175 (9.48%) | 368 (20.0%) |
| Almario CV et al., 2020 [16]; America | 3386 | N/A | 1168 (34.5%) | N/A | 243 (7.2%) | N/A | N/A | N/A |
| Lee SW et al., 2020 [23]; Korea | 4785 | Mean 45.4 SD 18.8 | 1893 (44.7%) | 945 (19.8%) | 524 (11.0%) | 263 (5.5%) | 150 (3.1%) | 523 (11.0%) |
| Israelsen SB et al., 2021 [15]; Denmark | 4473 | Median 60 IQR 48–73 | 1989 (44.5%) | N/A | 564 (12.6%) | 832 (18.6%) | 231 (5.2%) | 560 (12.6%) |
| Liu JJ et al., 2021 [24]; Mississippi | 56 | Mean 58 SD 14 | 20 (35.7%) | 39 (69.6%) | 24 (43.6%) | 3 (5.4%) | 7 (17.9%) | N/A |
| Fan X et al., 2021 [19]; United Kingdom | 9469 | >65 | 4611 (48.7%) | N/A | 1226 (12.9%) | 1741 (18.3%) | 753 (7.9%) | 1738 (18.3%) |
| Zhou J et al., 2021 [26]; China | 4445 | Median 44.8 | 307(58.6%) | 209 (39.9%) | 136 (26.0%) | 136 (26.0%) | 102 (19.5%) | 516 (98.5%) |
| Lee SW et al., 2020 [25]; Korea | 4785 | ≥18 | N/A | N/A | N/A | N/A | N/A | N/A |
| Ramchandaran P et al., 2020 [18]; USA | 295 | >60 | 162 (54.9%) | 209 (70.8%) | 132 (44.7%) | 45 (15.2%) | N/A | 44 (14.9%) |
| McKeigue PM et al., 2021 [27]; Scotland | 4251 | N/A | N/A | N/A | 949 (22.3%) | 2649 (62.3%) | 96 (2.3%) | 1430 (33.6%) |
| Blanc F et al., 2020 [28]; France | 89 | Mean 84.4 SD 7.9 | 31 (34.8%) | 61 (68.5%) | 36 (40.4%) | 53 (59.6%) | 47 (52.8%) | 15 (16.9%) |
| Huh K et al., 2020 [29]; South Korea | 6507 | N/A | 2815 (43.3%) | 1780 (27.4%) | 1562 (24.0%) | 1095 (16.8%) | 749 (11.5%) | 2893 (44.5%) |
| Xiang Y et al., 2021 [17]; United Kingdom | 397,000 | Mean 68.1 SD 8.1 | 177,441 (44.7%) | 131,180 (33.0%) | 28,287 (7.1%) | 31,258 (7.9%) | N/A | 69,397 (17.4%) |
| Vila-Corcoles A et al., 2021 [30]; Spain | 205 | N/A | 83 (40.5%) | N/A | 69 (33.7%) | 85 (41.5%) | 39 (19.0%) | 42 (20.5%) |
| Current | Prior | ||
|---|---|---|---|
| Elmunzer BJ et al., 2021 [22]; North America | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 417 (Within one month of hospital admission) | N/A | |
| Almario CV et al., 2020 [16]; America | Once daily | 2436 | N/A |
| Twice daily | 198 | N/A | |
| N/A | N/A | N/A | |
| Lee SW et al., 2021 [23]; Korea | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 364 (Within 30 days before first COVID test) | 188 (More than 30 days, up to a year before first COVID test) | |
| Israelsen SB et al., 2021 [15]; Denmark | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 4473 (Within 90 days before positive COVID test, before hospitalization) | 19338 (More than 90 days before positive COVID test, before hospitalization) | |
| Liu JJ et al., 2021 [24]; Mississippi | Once daily | 26 | N/A |
| Twice daily | 5 | N/A | |
| N/A | N/A | N/A | |
| Fan X et al., 2021 [19]; United Kingdom | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 250 | N/A | |
| Zhou J et al., 2021 [26]; China | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 524 | N/A | |
| Lee SW et al., 2021 [25]; Korea | Once daily | 489 | N/A |
| Twice daily (or more) | 312 | N/A | |
| N/A | 801 | N/A | |
| Ramchandaran P et al., 2020 [18]; USA | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 46 | N/A | |
| McKeigue PM et al., 2020 [27]; Scotland | Once daily | 1743 | N/A |
| Twice daily | 239 | N/A | |
| N/A | N/A | N/A | |
| Blanc F et al., 2020 [28]; France | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 23 | N/A | |
| Huh K et al., 2020 [29]; South Korea | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 851 | N/A | |
| Xiang Y et al., 2021 [17]; United Kingdom | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 8086 | N/A | |
| Vila-Corcoles A et al., 2020 [30]; Spain | Once daily | N/A | N/A |
| Twice daily | N/A | N/A | |
| N/A | 99 | N/A | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fatima, K.; Almas, T.; Lakhani, S.; Jahangir, A.; Ahmed, A.; Siddiqui, A.; Rahim, A.; Qureshi, S.A.; Arshad, Z.; Golani, S.; et al. The Use of Proton Pump Inhibitors and COVID-19: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 37. https://doi.org/10.3390/tropicalmed7030037
Fatima K, Almas T, Lakhani S, Jahangir A, Ahmed A, Siddiqui A, Rahim A, Qureshi SA, Arshad Z, Golani S, et al. The Use of Proton Pump Inhibitors and COVID-19: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2022; 7(3):37. https://doi.org/10.3390/tropicalmed7030037
Chicago/Turabian StyleFatima, Kaneez, Talal Almas, Shan Lakhani, Arshia Jahangir, Abdullah Ahmed, Ayra Siddiqui, Aiman Rahim, Saleha Ahmed Qureshi, Zukhruf Arshad, Shilpa Golani, and et al. 2022. "The Use of Proton Pump Inhibitors and COVID-19: A Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 7, no. 3: 37. https://doi.org/10.3390/tropicalmed7030037