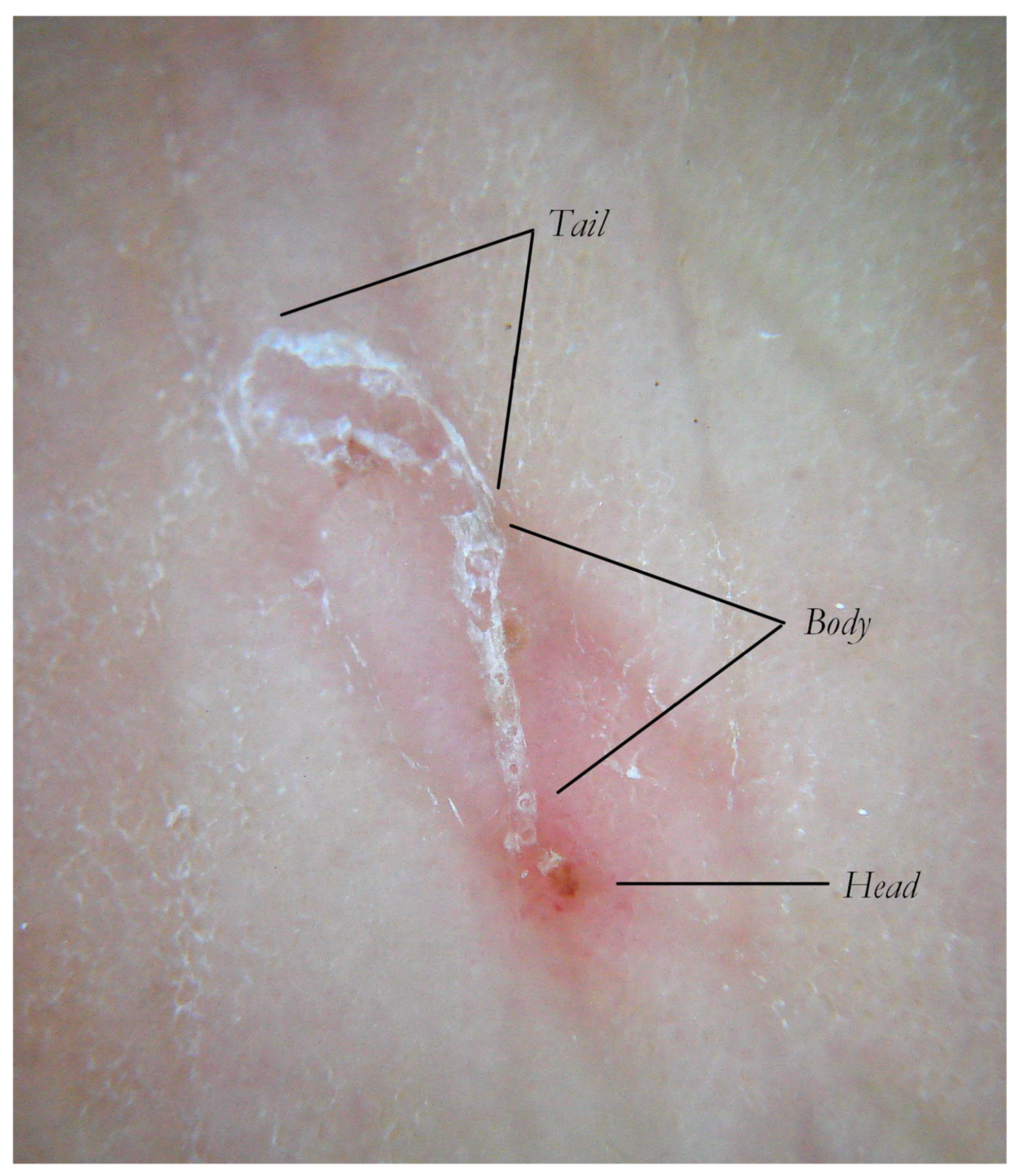
Figure 1.
The Mite-Gallery Unit in non-polarized dry dermoscopy (d-DS). MGU can be divided into three parts. The Head hosts the mite, the Body contains parasite eggs and feces and the Tail, which has not roof but features keratinic collarettes that are visible only in d-DS. An erythema is present in the background around and immediately behind the mite.
Figure 1.
The Mite-Gallery Unit in non-polarized dry dermoscopy (d-DS). MGU can be divided into three parts. The Head hosts the mite, the Body contains parasite eggs and feces and the Tail, which has not roof but features keratinic collarettes that are visible only in d-DS. An erythema is present in the background around and immediately behind the mite.
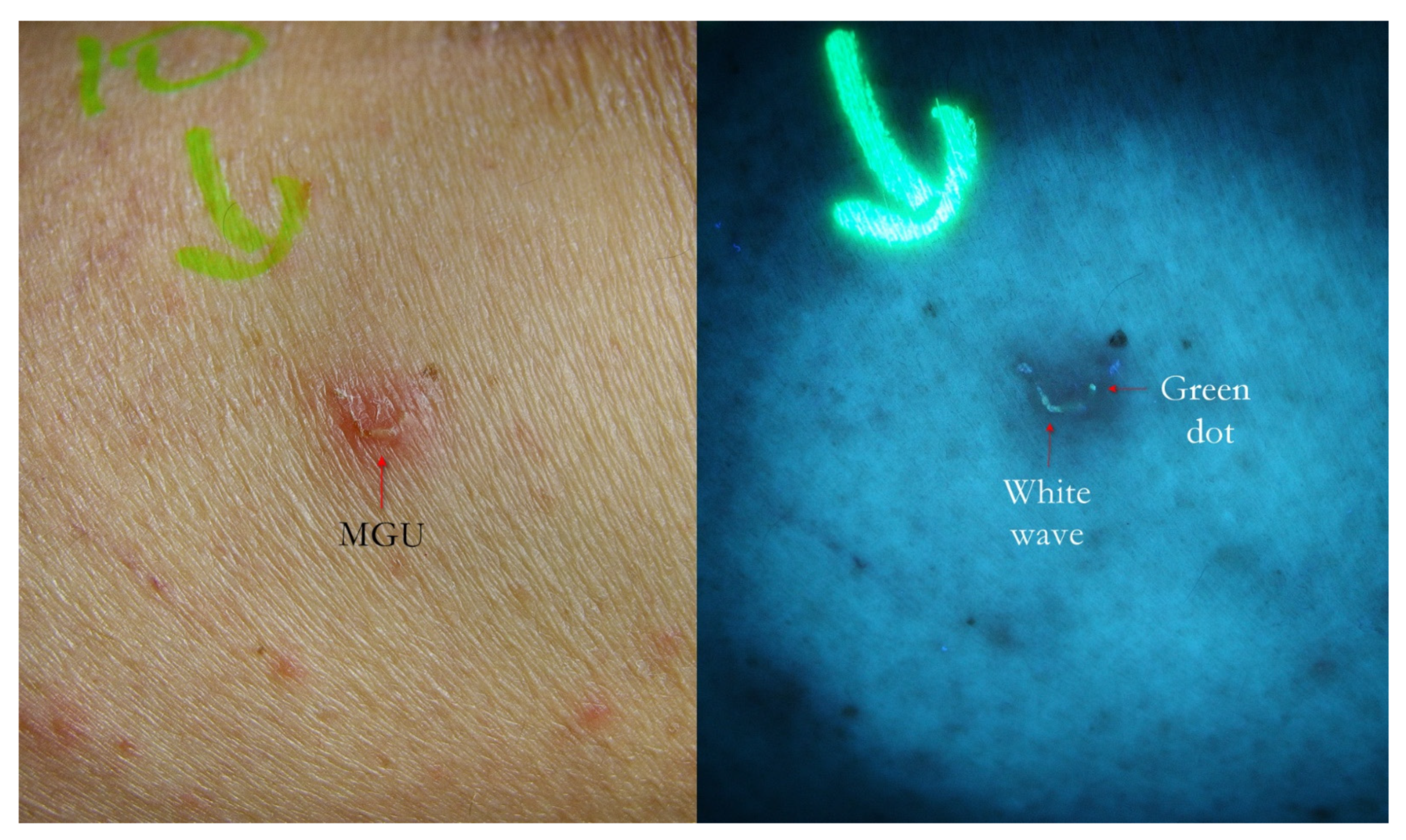
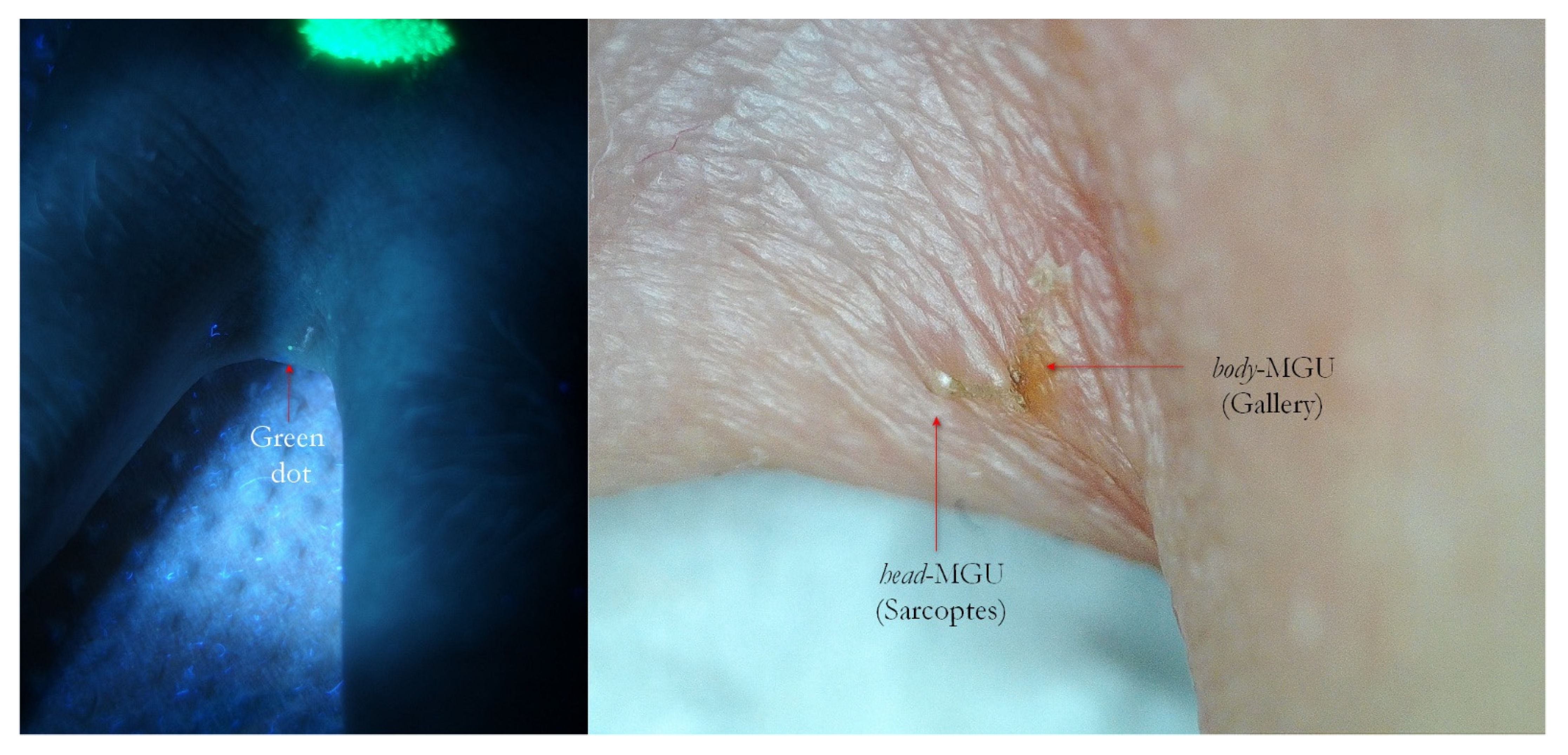
Figure 2.
Flash light vs. UVA. A MGU was already recognizable to naked eye (left) as an apparent single structure. However, UVA light was able to distinguish body-MGU (white wave) from head-MGU (green-dot) where Sarcoptes body was physically located (right). The red phlogosis halo around burrow returned a darker light than the rest of background. A yellow highlighter was used.
Figure 2.
Flash light vs. UVA. A MGU was already recognizable to naked eye (left) as an apparent single structure. However, UVA light was able to distinguish body-MGU (white wave) from head-MGU (green-dot) where Sarcoptes body was physically located (right). The red phlogosis halo around burrow returned a darker light than the rest of background. A yellow highlighter was used.
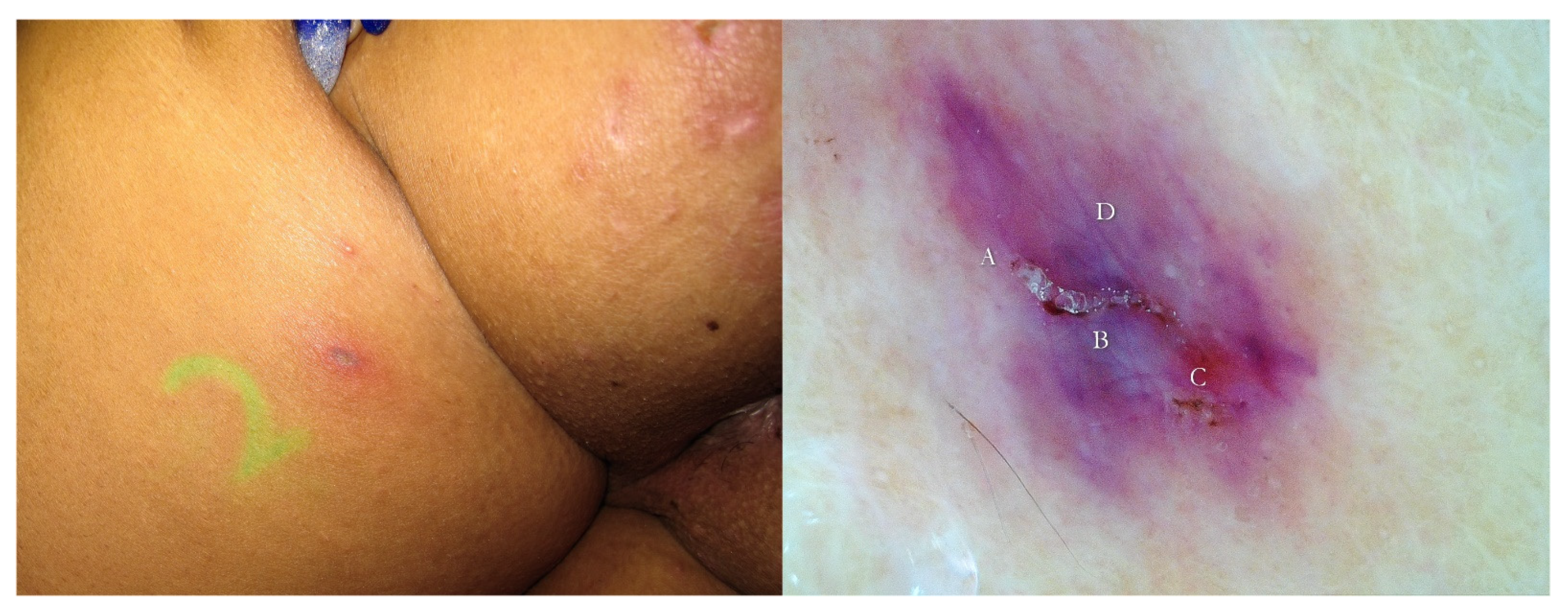
Figure 3.
Post-therapy non-specific lesion under buttock after two 5% Permethrin applications 7 days apart (left). Under wet dermoscopy, inside erosion, there was an unexpected MGU with the delta sign of Sarcoptes (A) and a gallery with fecal pellets (B) that faded in a fuzzy tail (C). All around, there was a purplish area (D) corresponding to superficial hematoma caused by patient scratching (right). A yellow highlighter was used.
Figure 3.
Post-therapy non-specific lesion under buttock after two 5% Permethrin applications 7 days apart (left). Under wet dermoscopy, inside erosion, there was an unexpected MGU with the delta sign of Sarcoptes (A) and a gallery with fecal pellets (B) that faded in a fuzzy tail (C). All around, there was a purplish area (D) corresponding to superficial hematoma caused by patient scratching (right). A yellow highlighter was used.
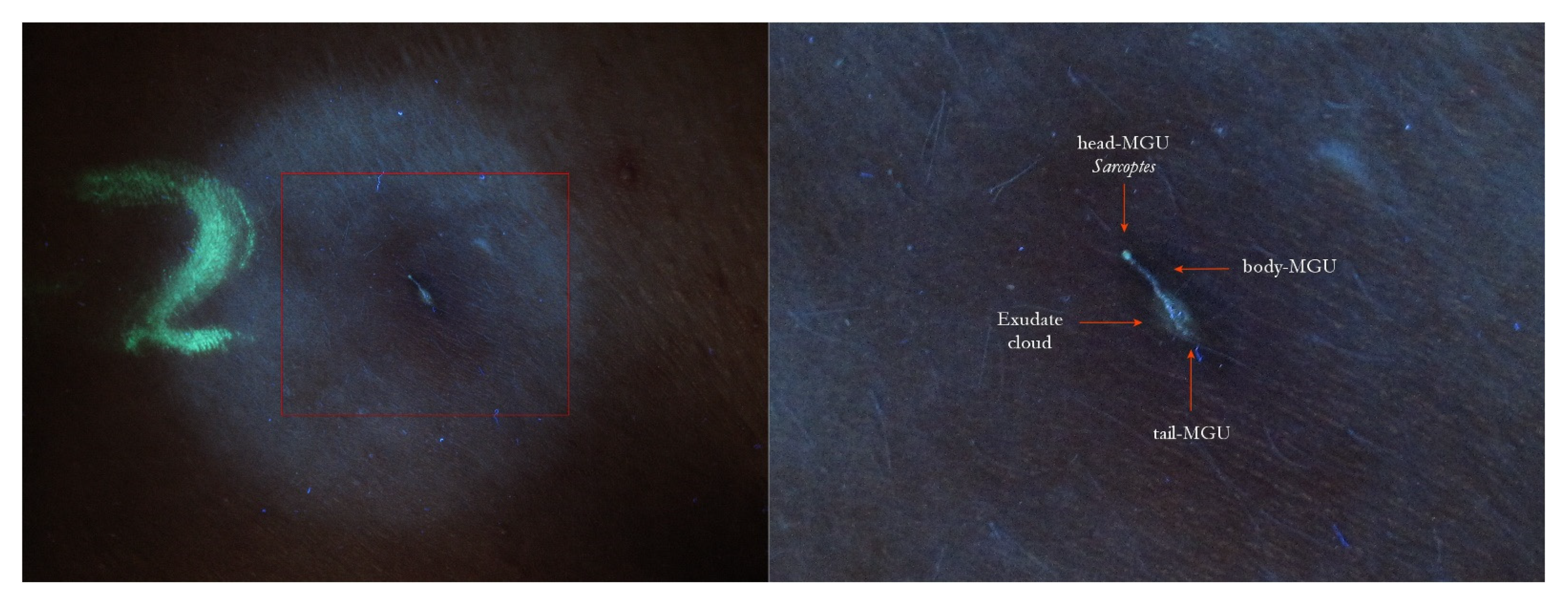
Figure 4.
The same lesion under UVA light showed a linear white luminescence (left, red box). In full-frame vision (right), it was possible to distinguish a Mite-Gallery Unit whose head part was occupied by Sarcoptes, which featured a green hue (green dot). Between body and tail MGU, there was a luminescent cloud caused by exudate and phlogosis around burrow (rocket sign). A yellow highlighter was used.
Figure 4.
The same lesion under UVA light showed a linear white luminescence (left, red box). In full-frame vision (right), it was possible to distinguish a Mite-Gallery Unit whose head part was occupied by Sarcoptes, which featured a green hue (green dot). Between body and tail MGU, there was a luminescent cloud caused by exudate and phlogosis around burrow (rocket sign). A yellow highlighter was used.
Figure 5.
Flash light vs. UVA. Two MGUs appeared as pink fuzzy streaks (left, red arrows). Under UVA they became clear linear structures (white waves), as in the pathognomonic sign of scabies. At one extremity, a little white dot was recognizable (A). A yellow highlighter was used.
Figure 5.
Flash light vs. UVA. Two MGUs appeared as pink fuzzy streaks (left, red arrows). Under UVA they became clear linear structures (white waves), as in the pathognomonic sign of scabies. At one extremity, a little white dot was recognizable (A). A yellow highlighter was used.
Figure 6.
Flash light vs. UVA. The burrow was a clue (left, red arrow) that under UVA light, a very clear linear structure (white wave) formed, suggesting a typical Mite-Gallery Unit (right). A yellow highlighter was used.
Figure 6.
Flash light vs. UVA. The burrow was a clue (left, red arrow) that under UVA light, a very clear linear structure (white wave) formed, suggesting a typical Mite-Gallery Unit (right). A yellow highlighter was used.
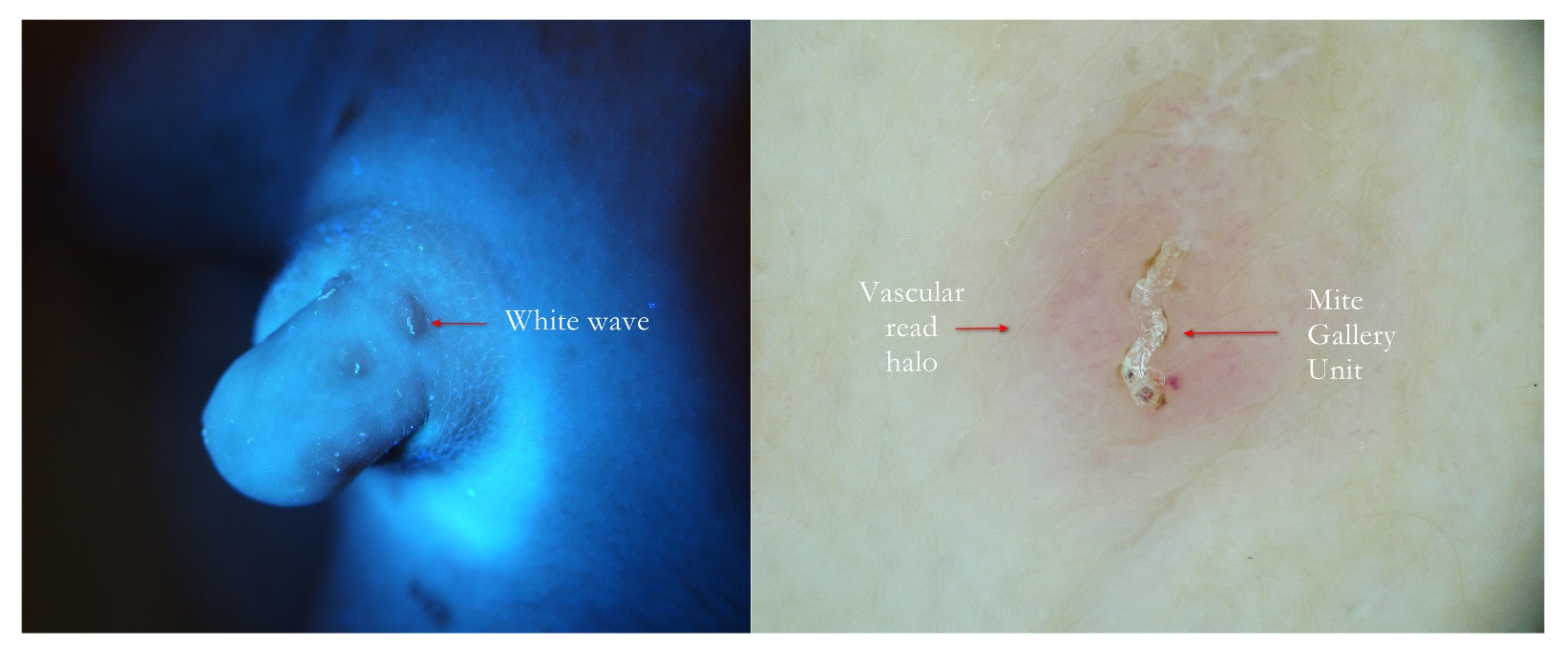
Figure 7.
Scabies penile papules. The at-a-glance bright linear UVA track (left, red arrow) was confirmed to be a typical Mite-Gallery Unit surrounded by a pink vascular infiltrate under wet dermoscopy (right).
Figure 7.
Scabies penile papules. The at-a-glance bright linear UVA track (left, red arrow) was confirmed to be a typical Mite-Gallery Unit surrounded by a pink vascular infiltrate under wet dermoscopy (right).
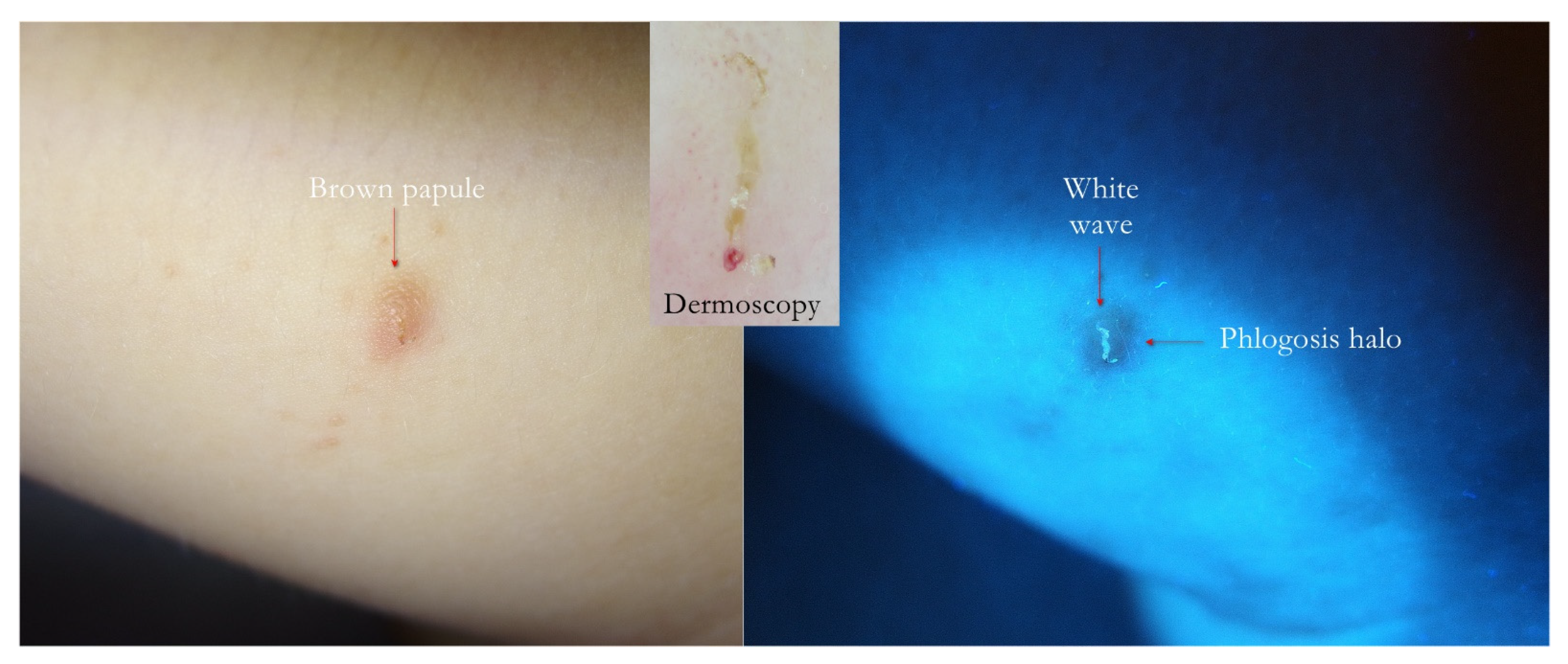
Figure 8.
Flash light vs. UVA. Papular scabies. A generic brown infiltrative lesion on inner side of thigh (left) produced a wavy linear luminescence under UVA (right). In the upward inset, dermatoscopy showed that the white wave was a MGU housed in the papule darker than the background.
Figure 8.
Flash light vs. UVA. Papular scabies. A generic brown infiltrative lesion on inner side of thigh (left) produced a wavy linear luminescence under UVA (right). In the upward inset, dermatoscopy showed that the white wave was a MGU housed in the papule darker than the background.
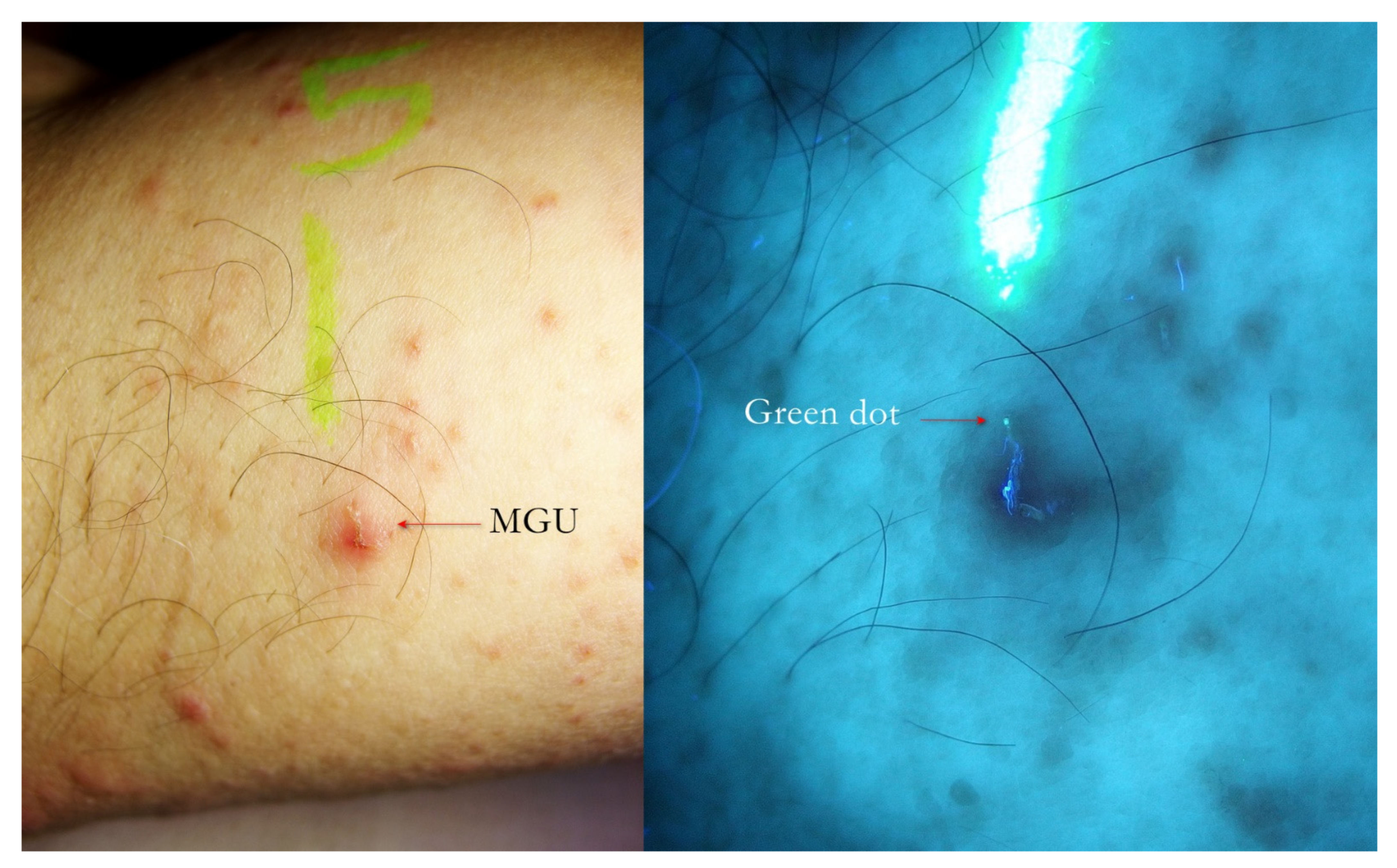
Figure 9.
Flash light vs. UVA. A little erythematous area on which a fuzzy linear lesion appeared to the naked eye (left). UVA light highlighted the undulated line that corresponded to a MGU whose one extremity ended with a green dot where Sarcoptes was located. A yellow highlighter was used.
Figure 9.
Flash light vs. UVA. A little erythematous area on which a fuzzy linear lesion appeared to the naked eye (left). UVA light highlighted the undulated line that corresponded to a MGU whose one extremity ended with a green dot where Sarcoptes was located. A yellow highlighter was used.
Figure 10.
Flash light vs. UVA. A MGU was distinguishable to naked eye (left). UVA light drew attention to the green dot where Sarcoptes body was located. The gallery behind had a bluish hue partially caused by a fabric thread glued on MGU. A yellow highlighter was used.
Figure 10.
Flash light vs. UVA. A MGU was distinguishable to naked eye (left). UVA light drew attention to the green dot where Sarcoptes body was located. The gallery behind had a bluish hue partially caused by a fabric thread glued on MGU. A yellow highlighter was used.
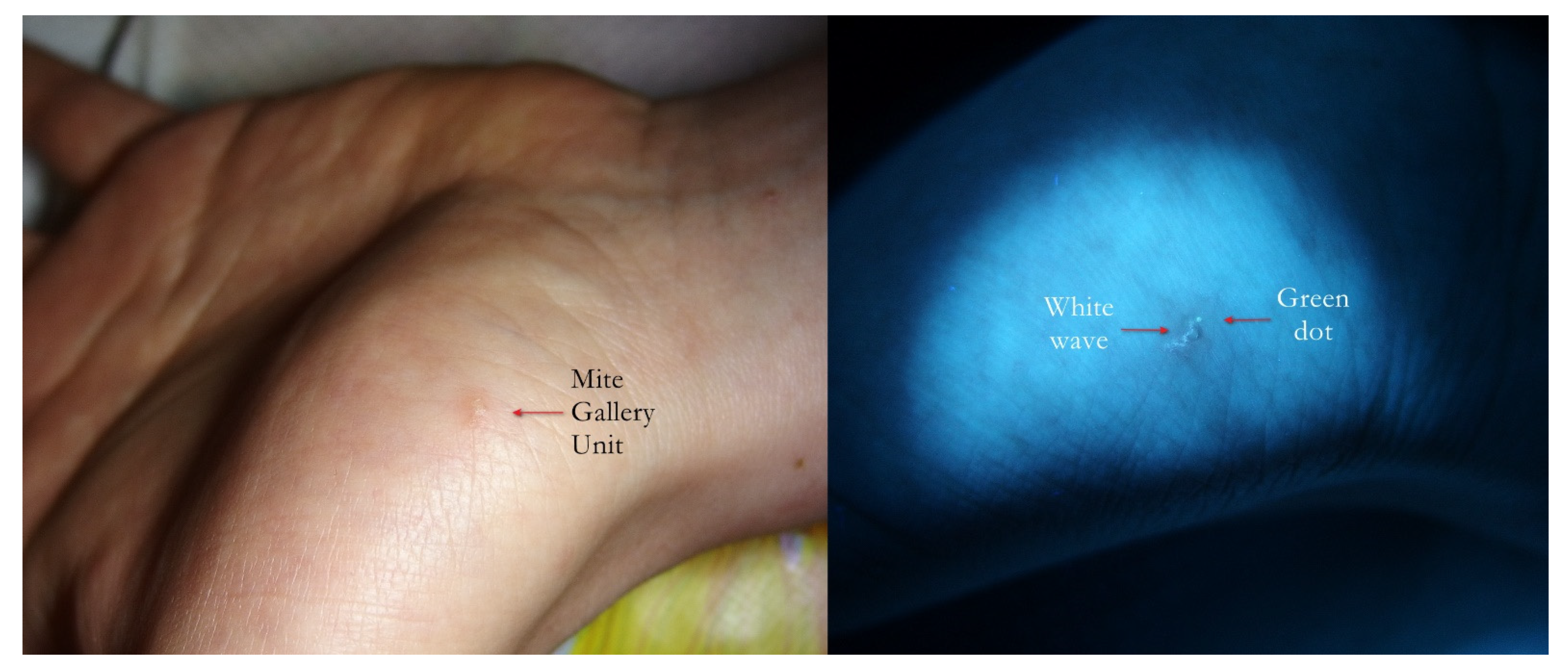
Figure 11.
Flash light vs. UVA. On thenar eminence, a very suggestive linear lesion (left) that under UVA (right) clearly became a wavy gallery (white wave) ending with a green dot where the mite was physically located.
Figure 11.
Flash light vs. UVA. On thenar eminence, a very suggestive linear lesion (left) that under UVA (right) clearly became a wavy gallery (white wave) ending with a green dot where the mite was physically located.
Figure 12.
Scabies of interdigital fold of hand. Interdigital MGU under UVA exhibited a green dot (left, red arrow). A bright blue luminescent fabric thread was nearby. Dry dermoscopy of same MGU confirmed Sarcoptes and its gallery (right, red arrows), but site anatomy made it difficult to obtain all-in-focus image. A yellow highlighter was used.
Figure 12.
Scabies of interdigital fold of hand. Interdigital MGU under UVA exhibited a green dot (left, red arrow). A bright blue luminescent fabric thread was nearby. Dry dermoscopy of same MGU confirmed Sarcoptes and its gallery (right, red arrows), but site anatomy made it difficult to obtain all-in-focus image. A yellow highlighter was used.
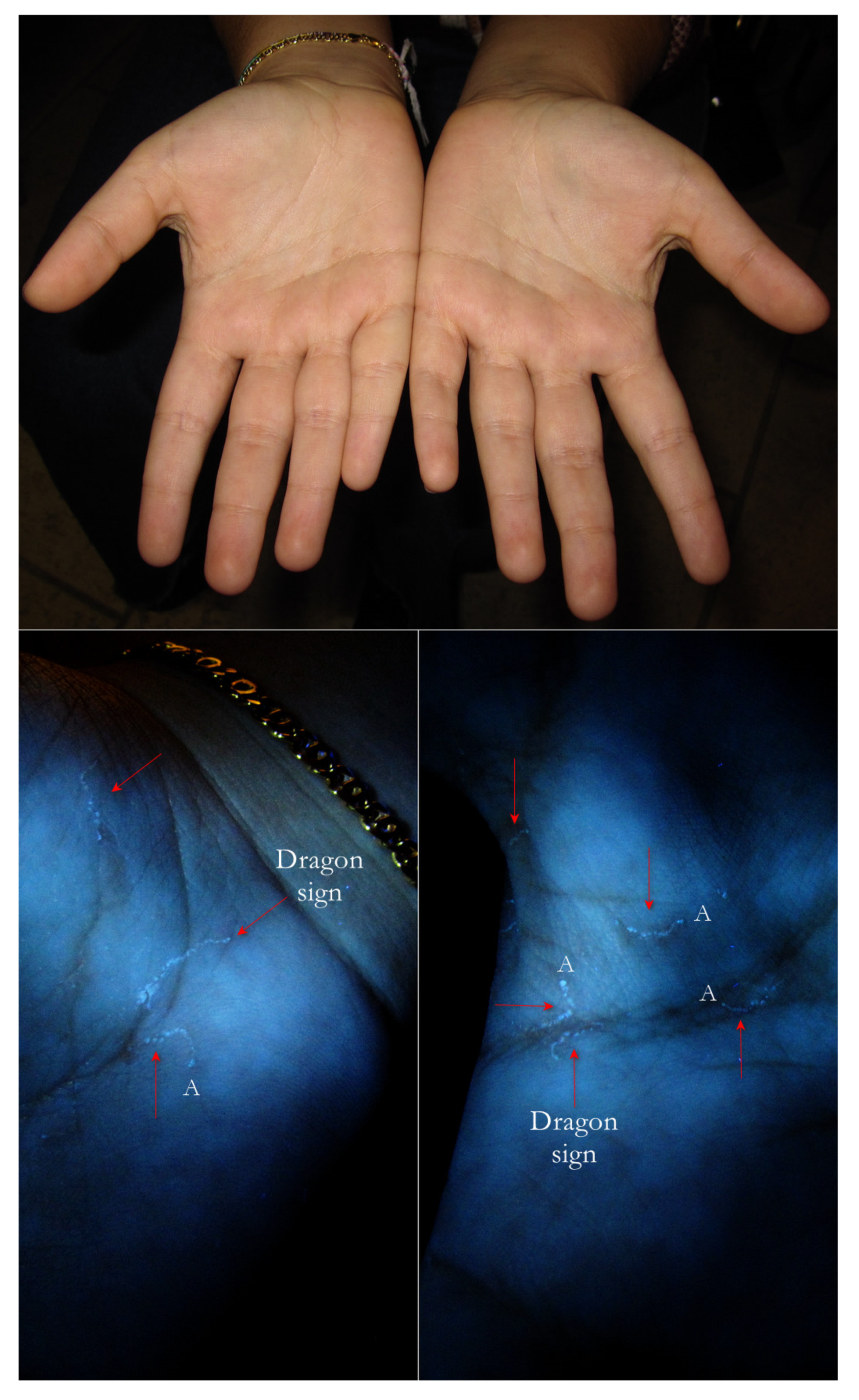
Figure 13.
Flash light vs. UVA. Two palms under flash light did not show any problems. However, under UVA, some Mite-Gallery Units (red arrows) were immediately visible as segmented lines (dragon sign). At one extreme, some of them exhibited a little white dot (A) where the Sarcoptes body was located. The lines drawn were finely segmented because the gallery roof was drilled.
Figure 13.
Flash light vs. UVA. Two palms under flash light did not show any problems. However, under UVA, some Mite-Gallery Units (red arrows) were immediately visible as segmented lines (dragon sign). At one extreme, some of them exhibited a little white dot (A) where the Sarcoptes body was located. The lines drawn were finely segmented because the gallery roof was drilled.
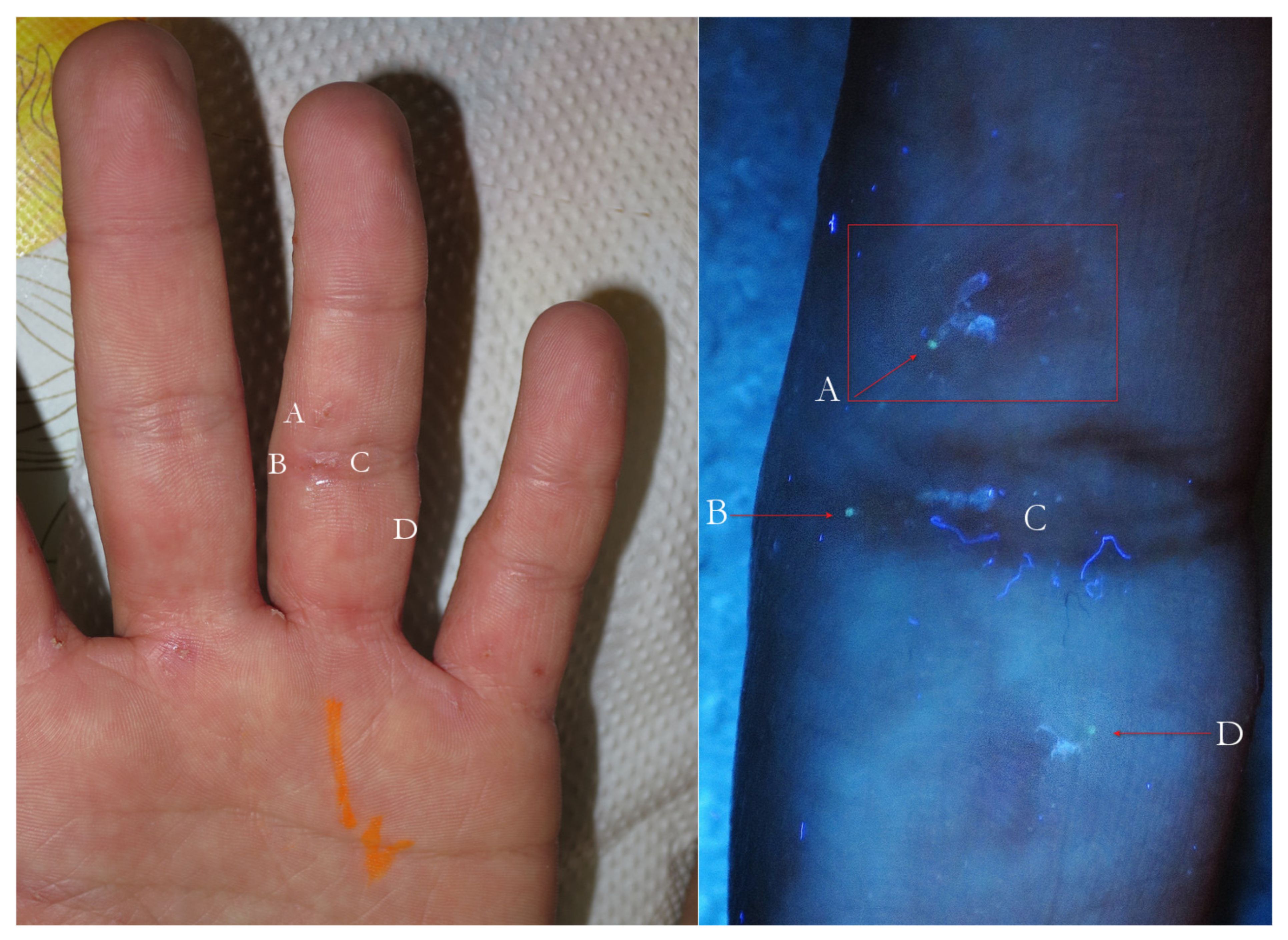
Figure 14.
Flash light vs. UVA. On the left, some very suggestive signs of MGUs that in full-frame view on the right corresponded to two green dots beside galleries (A–D), one isolated green dot (B) and a white line alone (C). B and C probably belonged to the same Mite-Gallery Unit. Sharp blue tortuous lines are fabric threads on background. A red highlighter was used.
Figure 14.
Flash light vs. UVA. On the left, some very suggestive signs of MGUs that in full-frame view on the right corresponded to two green dots beside galleries (A–D), one isolated green dot (B) and a white line alone (C). B and C probably belonged to the same Mite-Gallery Unit. Sharp blue tortuous lines are fabric threads on background. A red highlighter was used.
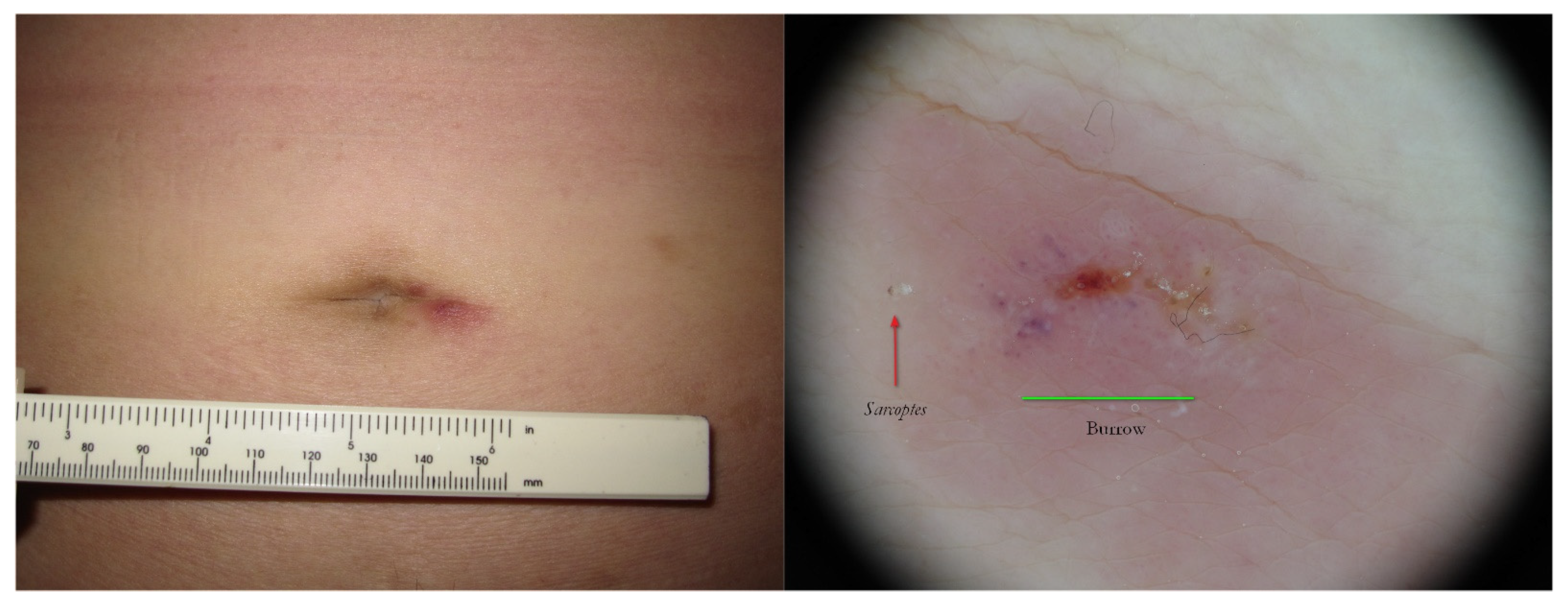
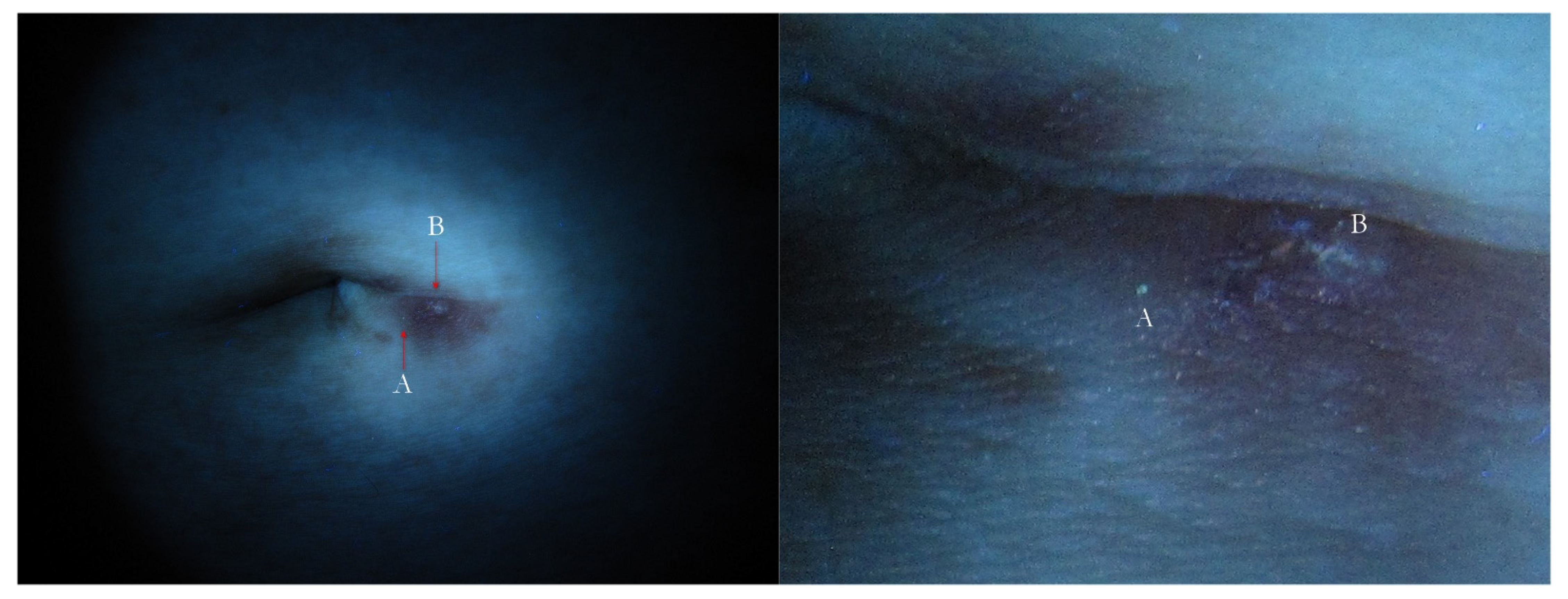
Figure 15.
Surrepticius scabies. A non-specific lesion on navel in an asymptomatic patient (left). Wet dermoscopy of the same lesion (right) showed a Sarcoptes as a brownish triangle (red arrow) and a burrow was no longer distinguishable because it was modified by host phlogosis-exuding reaction (green segment).
Figure 15.
Surrepticius scabies. A non-specific lesion on navel in an asymptomatic patient (left). Wet dermoscopy of the same lesion (right) showed a Sarcoptes as a brownish triangle (red arrow) and a burrow was no longer distinguishable because it was modified by host phlogosis-exuding reaction (green segment).
Figure 16.
Surreptitious scabies. The same patient under UVA. The navel lesion shows too little signs (left) that in full-frame view can be identified as a green dot (A) and a fuzzy white line (B), corresponding to Sarcoptes body and gallery remnants, respectively (right).
Figure 16.
Surreptitious scabies. The same patient under UVA. The navel lesion shows too little signs (left) that in full-frame view can be identified as a green dot (A) and a fuzzy white line (B), corresponding to Sarcoptes body and gallery remnants, respectively (right).
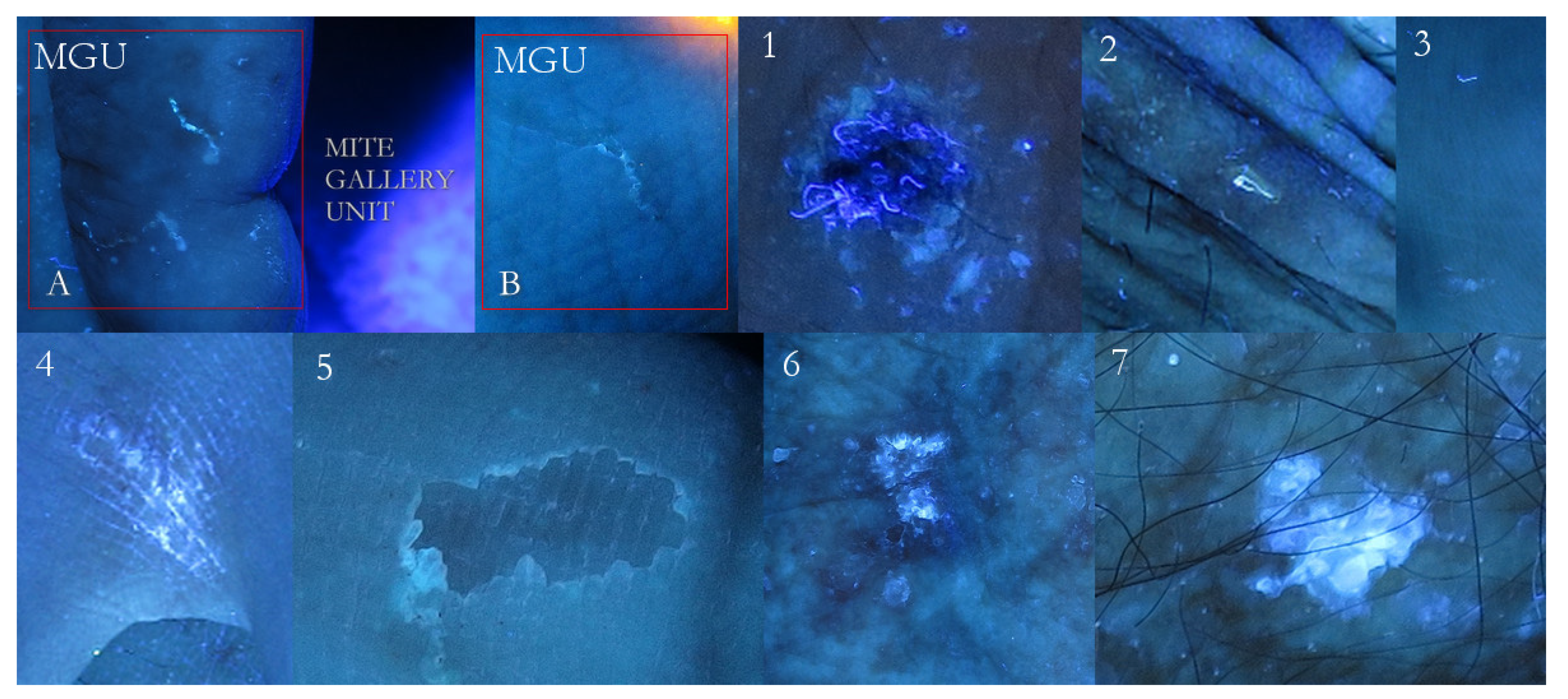
Figure 17.
False-positive examples. A mosaic table of possible positive signs compared to Mite-Gallery Units (A + B). Fabric threads captured by an erosion (1). Single thread shinier then any MGU (2). A thread above, a remnant of burrow down (3). Bright luminescent exogenous substance contaminating interdigital hand folds (4). Very superficial erosion as a faint luminescent scalloped collarette (5). An evident white luminescence of an epidermal keratosis (6). A very bright white lamellar luminescence of an actinic keratosis (7). These signs can be found separately or close to specific scabies lesions.
Figure 17.
False-positive examples. A mosaic table of possible positive signs compared to Mite-Gallery Units (A + B). Fabric threads captured by an erosion (1). Single thread shinier then any MGU (2). A thread above, a remnant of burrow down (3). Bright luminescent exogenous substance contaminating interdigital hand folds (4). Very superficial erosion as a faint luminescent scalloped collarette (5). An evident white luminescence of an epidermal keratosis (6). A very bright white lamellar luminescence of an actinic keratosis (7). These signs can be found separately or close to specific scabies lesions.
Table 1.
Diagnostic criteria established in 2020 by IACS (International Alliance for the Control of Scabies).
Table 1.
Diagnostic criteria established in 2020 by IACS (International Alliance for the Control of Scabies).
| A. Confirmed Scabies |
| At least one of: |
| A1. Mites, eggs, faeces on light microscopy of skin samples |
| A2. Mites, eggs, faeces visualized on an individual using a high-powered imaging device |
| A3. Mites visualized on individual using dermoscopy |
| |
| B. Clinical Scabies |
| At least one of: |
| B1. Scabies burrows |
| B2. Typical lesion affecting male genitalia |
| B3. Typical lesions in a typical distribution and two history features |
| |
| C. Suspected Scabies |
| One of: |
| C1. Typical lesions in a typical distribution and one history feature |
| C2. Atypical lesions or atypical distribution and two history features |
| |
| History Features |
| H1. Itch |
| H2. Positive contact history |




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}