
Effect of Oral Antidiabetic Drugs on Tuberculosis Risk and Treatment Outcomes: Systematic Review and Meta-Analysis


 ,
,
Abstract
:1. Introduction
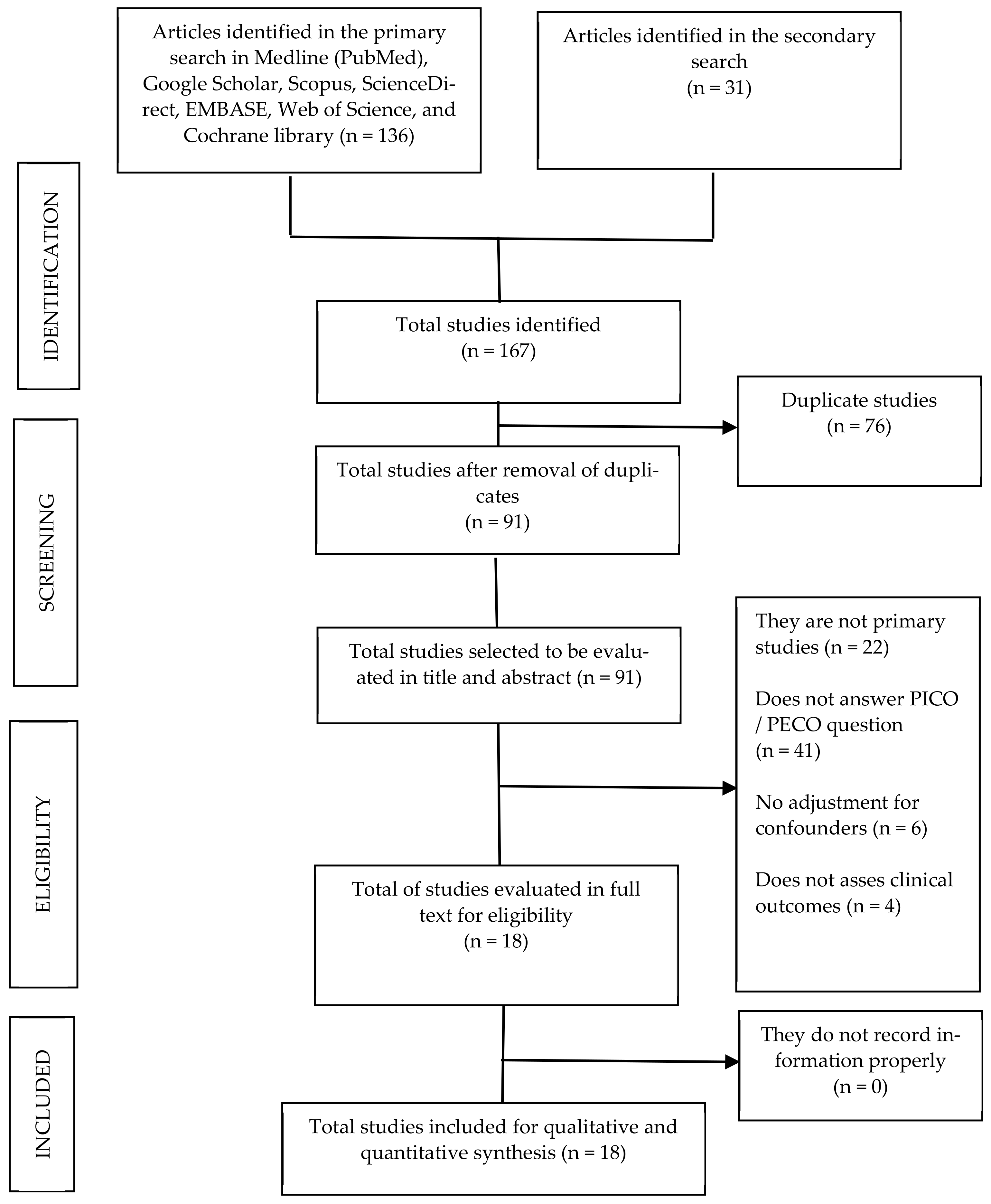
2. Materials and Methods
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants/Cases | Exposition | Outcome | Adjustment of Confounders | OR/RR/HR (95% IC) |
|---|---|---|---|---|---|
| Padmapriydarsini C. [7]. 2022. India. RCT. | Non-DM patients ≥ 18 y. Newly diagnosed, culture-positive PTB patients. Standard ATT (control arm) or standard ATT + 1 g daily MET (METRIF arm). Randomized 322. Completed ATT: 155 in METRIF arm and 151 in control arm. Follow-up: 8 weeks. | MET | Time to sputum culture conversion during 8 weeks of ATT. | Age, BMI, gender, smoking, OH, and smear grading. | HR 0.8 (0.624–1.019); p = 0.082, for median time to sputum culture conversion after 8 weeks of treatment. |
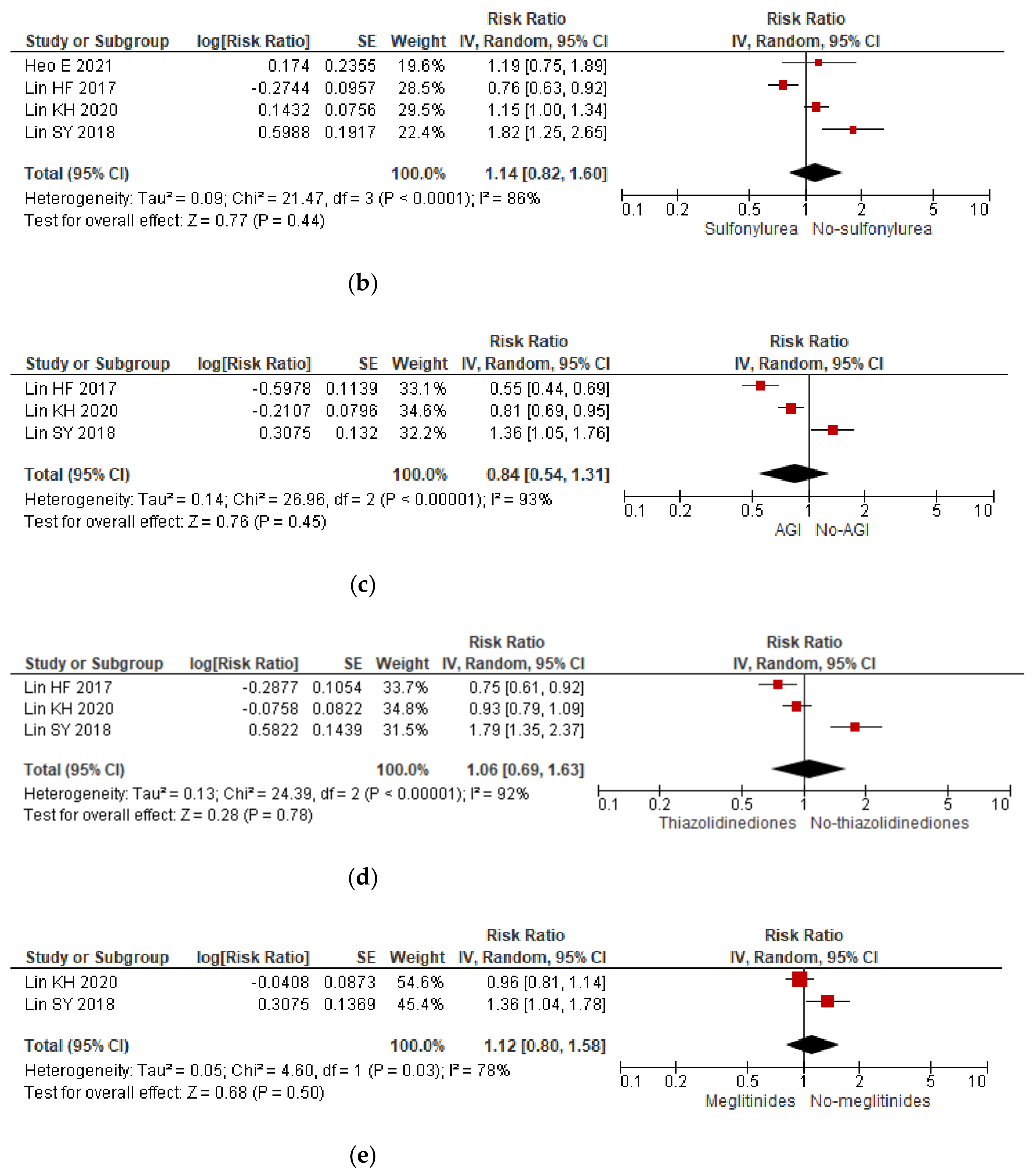
| Heo E. [8]. 2021. South Korea. RCS. | N = 76,973 newly diagnosed patients with T2DM, 13,396 MET users, 52,736 MET non-users, and 10,841 excluded patients. TB cases among MET users 46, and among MET non-users 206. Follow-up: 2 y. | MET | Development of TB within 2 y of the index date. | Age, sex, comorbidities, immunosuppressives, CMI, anti-DM treatment, healthcare utilization, hospitalization days, and outpatient visit days. | HR 1.17 (0.75–1.83); p = 0.482 for MET and prevention of TB development. HR 1.10 (0.67–1.86) for Q1 of CD of MET. HR 1.69 (1.05–2.71) for Q2 of CD of MET. HR 0.49 (0.20–1.21) for Q3 of CD of MET. HR 0.10 (0.01–0.70) for Q4 of CD of MET. HR 1.19 (0.75–1.87); p = 0.46 for SU. |
| Lee Y.J. [15]. 2018. South Korea. RCS. | N = 499 patients with culture-positive PTB. DM at diagnosis 105, among them 62 were treated with MET. Follow-up: 2 months. | MET | Sputum culture conversion after 2 months of treatment. Recurrence of TB (isolation of MTB, clinical, or radiological evidence). | Sex, statin use, insulin, cancer, AFB smear grade, and drug resistance. | Analysis including only the patients with PTB and DM: OR 2.69 (0.92–7.95); p = 0.07 for sputum culture conversion at 2 m. with the use of MET. OR 1.92 (0.42–8.76); p = 0.39 for recurrence rate with the use of MET. |
| Degner N.R. [16]. 2018. Taiwan. RCS. | N = 2416 (DM 699, without DM 1717). DM patients ≥ 13 y with culture-confirmed PTB undergoing treatment 634 (MET 216, non-MET 418). Follow-up: 6 months. | MET within 30 days of starting ATT. | Mortality among DM patients undergoing ATT. | Age, sex, CKD, cancer, cavitary diseases, ATT adherence. | Analysis including only diabetic patients: HR 0.56 (0.39–0.82; p = 0.002) for MET and mortality. |
| Lin H.F. [17]. 2017. Taiwan. RCS. | N = 22,256 adults (≥20 y) newly diagnosed with T2DM and 89,024 persons without DM. TB 3410. (See Footnote **). Follow-up: ≥ 2 y. | MET, SU, TZD, AGI | Risk of TB. | Sex, age, OH, COPD, cirrhosis, OH, hepatitis C, CKD, cancer. | Analysis including only the diabetic cases: HR 0.52 (0.43–0.62) for MET; HR 0.76 (0.63–0.92) for SU; HR 0.75 (0.61–0.93) for TZD; HR 0.55 (0.44–0.67) for AGI. |
| Lin S.Y. [18]. 2018. Taiwan. RCS | N = 49,028 T2DM patients, MET users (N = 44,002) or MET non-users (N = 5026). Follow-up: 12 y (until death or the end of 2010). | MET | Risk of TB. | DM duration, comorbidities (COPD/CKD), OADs and insulin therapy. | RR 0.24 (0.18–0.32); p ≤0.0001 for active TB and MET. RR 1.82 (1.25–2.64); p = 0.0016 for active TB and SU. RR 1.36 (1.04–1.79); p = 0.0238 for active TB and MEG. RR 1.79 (1.35–2.37); p ≤ 0.0001 for active TB and TZD. RR 1.36 (1.05–1.77); p = 0.0202 for active TB and AGI. |
| Lin K.H. [19]. 2020. Taiwan. CCS. | DM patients ≥ 20 years old. 6224 controls and 1556 TB cases. Mean follow-up: 11 y. | Different OADs. | Risk of TB. | Sex, age, urbanization level, length of hospital stay, income, comorbidities. | RR 1.032 (0.887–1.200) for TB in low dose MET users. RR 0.904 (0.732–1.117) for TB in high dose MET users. RR 1.154 (0.995–1.338) for TB in SU users. RR 0.960 (0.809–1.138) for TB in MEG users. RR 0.810 (0.693–0.948) for TB in AGI. RR 0.927 (0.789–1.087) for TB in TZD users. |
| Lee M.C. [20]. 2018. Taiwan. RCS | Newly diagnosed DM patients. Newly diagnosed DM. A total of 88,866 MET users and 88,866 propensity score-matched MET nonusers. During follow-up, 707 MET users and 807 MET nonusers developed active TB. Total TB cases 1514. Follow-up: ≥ 8 y. | MET | Risk of TB. | Sex, T1DM, age, income, COPD, cirrhosis, cancer, bronchiectasis, etc. | HR 0.84 (0.74–0.96); p = 0.013 for active TB among all subjects. HR 0.83 (0.72–0.97) for high-dose MET. |
| Lee M.C. [21]. 2019. Taiwan. RCS. | N = 5846 diabetic TB close contacts. TB cases among MET users 77, among MET non-users 116, among healthy participants 49. Follow-up: 2 y. | MET | Risk of TB. | Age, male, DM complications, TB history, contact area, local TB incidence, income, etc. | HR 0.73 (0.54–0.98); p = 0.035 for risk of incident TB among MET users compared to MET non-users. HR 0.66 (0.49–0.88); p = 0.006 for low dose MET. HR 0.59 (014–2.48); p = 0.473 for high dose. |
| Pan S.W. [22]. 2018. Taiwan. RCS | N = 40,179 patients with T2DM, 263 acquired TB over a mean follow-up of 6.1 y. Patients aged <20 y or with a TB diagnosis were excluded (N = 9475). Follow-up: 6.1 y. | MET | Risk of TB. | Age, sex, adapted DCSI, index year, income. | HR 0.337 (0.169–0.673); p = 0.002 for MET users compared to SU users. MET < 60 cDDD: reference group. MET 60–219 cDDD: HR 0.860 (0.637–1.161). MET 220–479 cDDD: HR 0.706 (0.485–1.028). MET 480 cDDD: HR 0.319 (0.118–0.863). |
| Tseng C.H. [23]. 2018. Taiwan. RCS | N = 423,949 newly diagnosed DM patients. Cases (TB) 2336: 360 never-MET users and 1976 MET users. Follow-up: ≥72 months. | MET | Risk of TB. | Age, DM duration, sex, occupation, living region, HT, dyslipidemia, obesity, DM-related complications, OADs, etc. | HR 0.552 (0.493–0.617) for TB and MET users compared with MET never users. HR 1.037 (0.918–1.173) for 1st tercile of CD of MET. HR 0.533 (0.469–0.606) for 2nd tercile of cumulative dose of MET. HR 0.249 (0.215–0.288) for 3rd tercile of CD of MET. |
| Al-Shaer M.H. [24]. 2018. Qatar. RCS | N = 103 patients with poorly controlled DM and PTB, 72 patients receiving MET. Follow-up: 4 months. | MET | Time to negative smears and the impact of adding MET. | Age, weight, gender, treatment group, ATT dose, AFB load, HbA1c, and total MET daily dose. | OR 0.12 (0.03–0.45) for to sputum smear conversion. |
| Park S [25]. 2019. South Korea. RCS | T2DM patients aged ≥60 y. N = 12,582 patients among each group (MET vs. SU). TB cases among MET group 79, in SU group 103. Follow-up: 11 y. | MET compared to SU. | Risk of TB. | Age, sex, CCI, comorbidities, medications. | HR 0.74 (0.58–0.95) for TB and MET users compared to SU users. HR 0.63 (0.44–0.91) for males compared to females. MET cDDD <50: HR 0.78 (0.51–1.22). MET cDDD 50–200: HR 0.69 (0.36–1.31). MET cDDD 200–400: HR 0.68 (0.33–1.40). MET cDDD >400: HR 0.20 (0.06–0.61) |
| Fu C.P. [26]. 2021. Taiwan. RCS. | N = 9750 patients with T2DM. TB cases 47. Follow-up among MET and non-MET users was 2.8–1.8 and 2.6–1.8 y, respectively. | MET | Risk of TB. | Age, sex, FBS, HbA1c, HDL-C, LDL-C, TC, UACR. | HR 0.54 (0.3–0.99); p = 0.0475 for TB among MET users compared with non-MET users. |
| Chen H.H. [27]. 2020. Taiwan. RCS. | Diabetic patients >20 years old. N = 6399 DPP4i users and 6399 DDP4i non-users. Events (TB cases) among DPP4i users 32, among no DPP4i users 24. Mean follow-up 5 y. | DPP4i (not specified which one). | Risk of TB. | Gender, age, DCSI, comorbidities, anti-HT agents, insulin, etc. | HR 1.04 (0.57–1.92); p = 0.89 for TB in DPP4i users relative to DDP4i non-users. |
| FDA [28]. 2010. USA. RCT. | N = 4959 patients taking DPP4i, and 2868 controls. TB among those taking DPP4i 6 and among controls 0. Duration of treatment with DPP4i until the report of TB ranged from 144–929 days. | DPP4i (saxagliptin). | Risk of TB. | Dose | RR * 1.5790 (1.5526–1.6059; p < 0.0001 for risk of TB. |
| Su W.J. [29]. 2018. Taiwan. RCS. | N = 47,740 T2DM patients and matched controls (1:1). Follow-up: 8 y. Cases not reported. | MET vs. SU | Risk of TB. | Age, sex, income, DCSI | RR 0.328 (0.174–0.625) for TB among MET initiators compared to SU initiators. |
| Bailey CJ [30]. 1212. Phase 3 RCT. | N = 282 T2DM patients. Placebo 68, dapagliflozin (210). TB cases among placebo group 0, TB cases among dapagliflozin group 1. Follow-up: 28 weeks. | Dapagliflozin (1mg, 2.5mg, 5mg) | Risk of TB. | Dose | RR * 1.0313 (0.0425–25.0080); p = 0.9849 for risk of TB. |
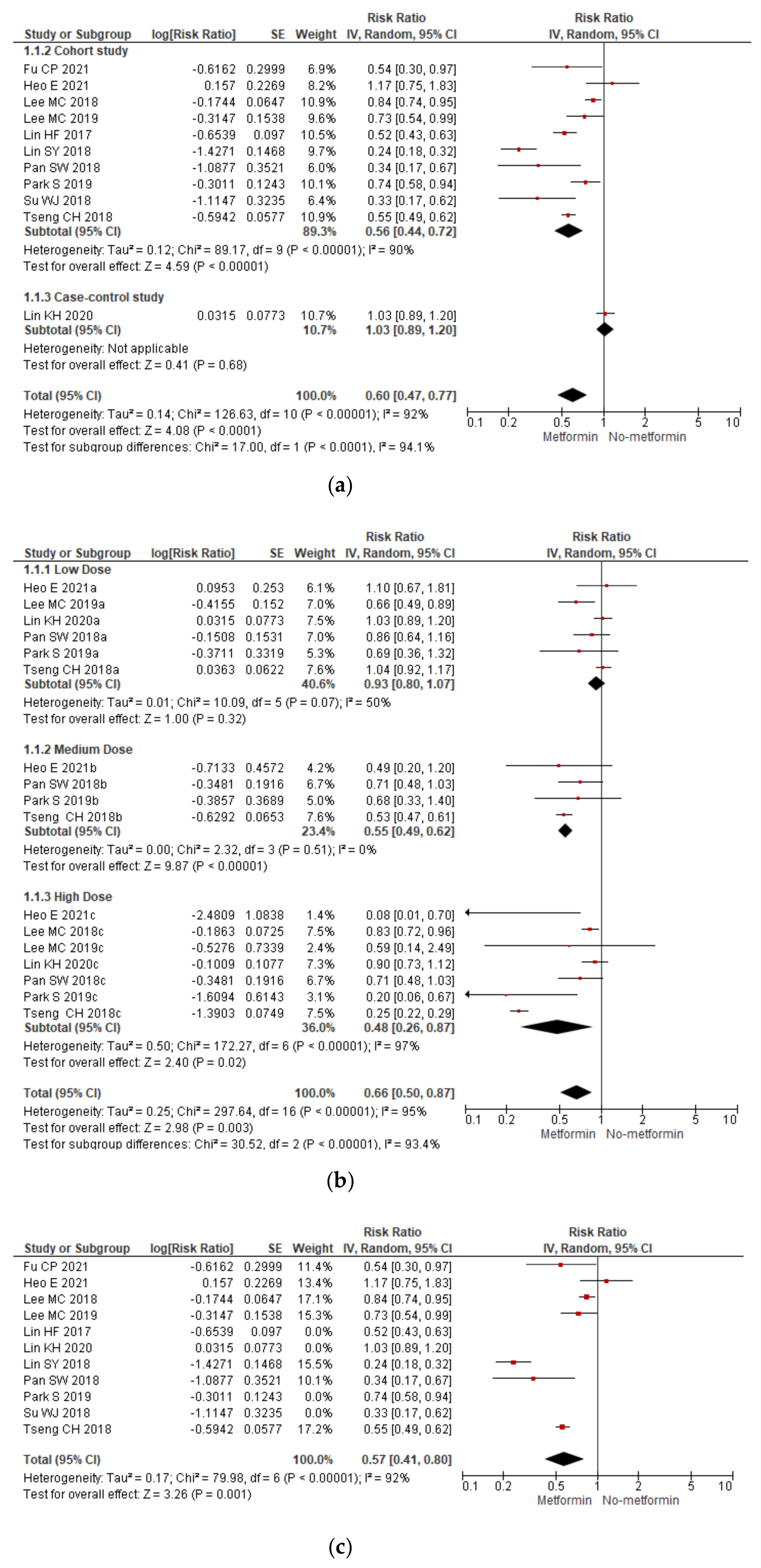
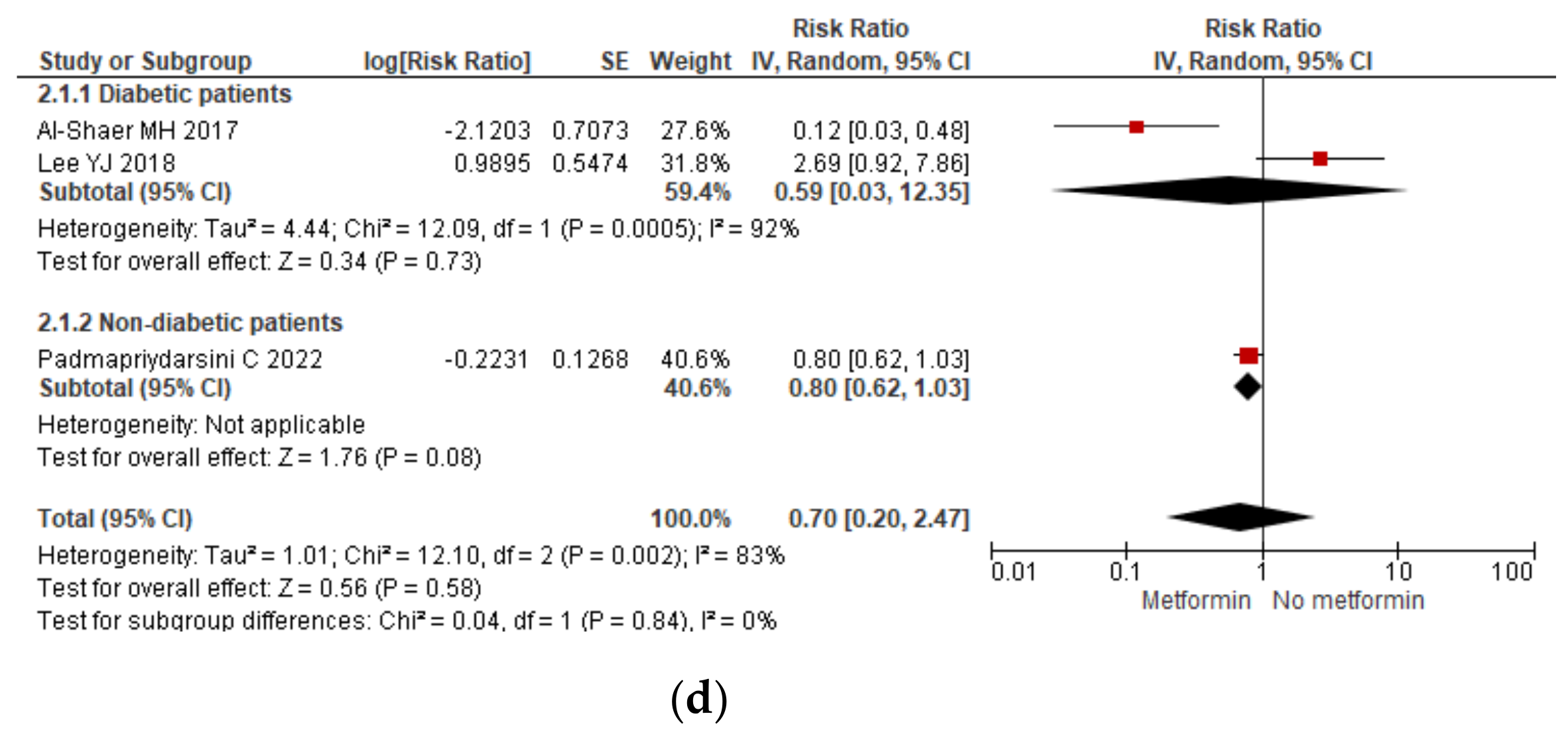
3.1. Metformin
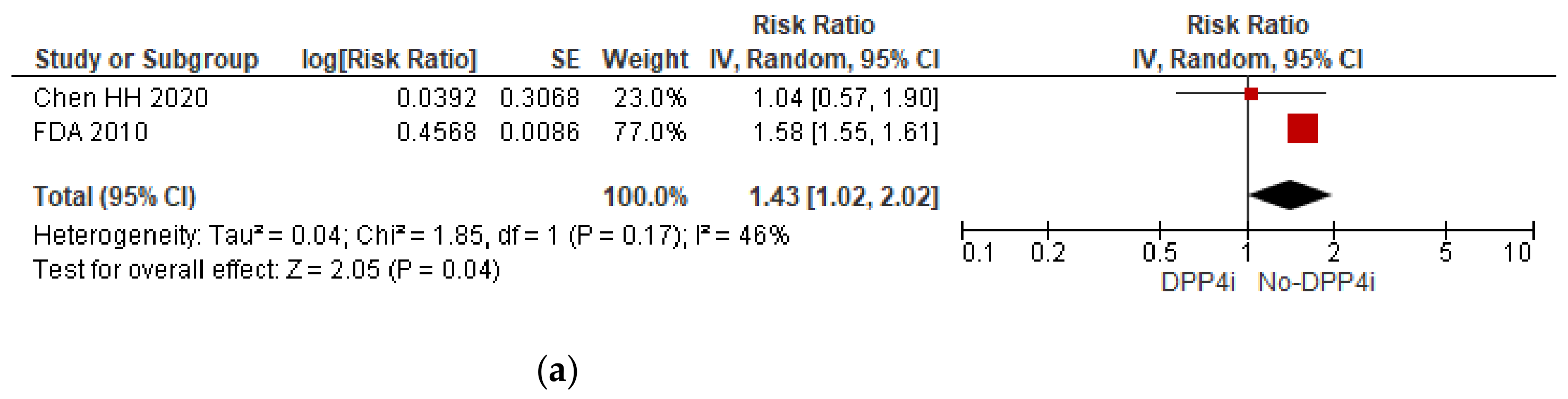
3.2. Other Oral Antidiabetic Drugs (OADs)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Restrepo, B.I. Diabetes and tuberculosis. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Nathella, P.K.; Babu, S. Influence of diabetes mellitus on immunity to human tuberculosis. Immunology 2017, 152, 13–24. [Google Scholar] [CrossRef]
- Martinez, N.; Kornfeld, H. Diabetes and immunity to tuberculosis. Eur. J. Immunol. 2014, 44, 617–626. [Google Scholar] [CrossRef] [Green Version]
- Huangfu, P.; Ugarte-Gil, C.; Golub, J.; Pearson, F.; Critchley, J. The effects of diabetes on tuberculosis treatment outcomes: An updated systematic review and meta-analysis. Int. J. Tuberc. Lung Dis. 2019, 23, 783–796. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Li, L.; Xia, L.; Feng, X.; Chen, F.; Cao, S.; Wei, X. Impact of metformin on the risk and treatment outcomes of tuberculosis in diabetics: A systematic review. BMC Infect. Dis. 2019, 19, 859. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; He, J.Q. Impacts of metformin on tuberculosis incidence and clinical outcomes in patients with diabetes: A systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 2020, 76, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Padmapriydarsini, C.; Mamulwar, M.; Mohan, A.; Shanmugam, P.; Gomathy, N.S.; Mane, A.; Singh, U.B.; Pavankumar, N.; Kadam, A.; Kumar, H.; et al. Randomized Trial of Metformin with Anti-Tuberculosis Drugs for Early Sputum Conversion in Adults with Pulmonary Tuberculosis. Clin. Infect. Dis. 2022, 75, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Heo, E.; Kim, E.; Jang, E.J.; Lee, C.H. The cumulative dose-dependent effects of metformin on the development of tuberculosis in patients newly diagnosed with type 2 diabetes mellitus. BMC Pulm. Med. 2021, 21, 303. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://handbook-5-1.cochrane.org/ (accessed on 7 September 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- McKenzie, D.P.; Thomas, C. Relative risks and odds ratios: Simple rules on when and how to use them. Eur. J. Clin. Investig. 2020, 50, e13249. [Google Scholar] [CrossRef] [PubMed]
- Thorlund, K.; Walter, S.D.; Johnston, B.C.; Furukawa, T.A.; Guyatt, G.H. Pooling health-related quality of life outcomes in meta-analysis-a tutorial and review of methods for enhancing interpretability. Res. Synth. Methods 2011, 2, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Anzures-Cabrera, J.; Sarpatwari, A.; Higgins, J.P. Expressing findings from meta-analyses of continuous outcomes in terms of risks. Stat Med. 2011, 30, 2967–2985. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Han, S.K.; Park, J.H.; Lee, J.K.; Kim, D.K.; Chung, H.S.; Heo, E.Y. The effect of metformin on culture conversion in tuberculosis patients with diabetes mellitus. Korean J. Intern. Med. 2018, 33, 933–940. [Google Scholar] [CrossRef]
- Degner, N.R.; Wang, J.Y.; Golub, J.E.; Karakousis, P.C. Metformin Use Reverses the Increased Mortality Associated with Diabetes Mellitus During Tuberculosis Treatment. Clin. Infect. Dis. 2018, 66, 198–205. [Google Scholar] [CrossRef]
- Lin, H.F.; Liao, K.F.; Chang, C.M.; Lai, S.W.; Tsai, P.Y.; Sung, F.C. Anti-Diabetic Medication Reduces Risk of Pulmonary Tuberculosis in Diabetic Patients: A Population-based Cohort Study in Taiwan. Kuwait Med. J. 2017, 49, 22–28. [Google Scholar]
- Lin, S.Y.; Tu, H.P.; Lu, P.L.; Chen, T.C.; Wang, W.H.; Chong, I.W.; Chen, Y.H. Metformin is associated with a lower risk of active tuberculosis in patients with type 2 diabetes: Metformin reduces TB risk in diabetics. Respirology 2018, 23, 1063–1073. [Google Scholar] [CrossRef] [Green Version]
- Lin, K.H.; Luo, C.W.; Chen, S.P.; Tu, D.G.; Lin, M.S.; Kuan, Y.H. α-Glucosidase Inhibitor Can Effectively Inhibit the Risk of Tuberculosis in Patients with Diabetes: A Nested Case-Control Study. BioMed Res. Int. 2020, 2020, 8085106. [Google Scholar] [CrossRef]
- Lee, M.C.; Chiang, C.Y.; Lee, C.H.; Ho, C.M.; Chang, C.H.; Wang, J.Y.; Chen, S.M. Metformin use is associated with a low risk of tuberculosis among newly diagnosed diabetes mellitus patients with normal renal function: A nationwide cohort study with validated diagnostic criteria. PLoS ONE 2018, 13, e0205807. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.C.; Lee, C.H.; Lee, M.R.; Wang, J.Y.; Chen, S.M. Impact of metformin use among tuberculosis close contacts with diabetes mellitus in a nationwide cohort study. BMC Infect. Dis. 2019, 19, 936. [Google Scholar] [CrossRef] [Green Version]
- Pan, S.W.; Yen, Y.F.; Kou, Y.R.; Chuang, P.H.; Su, V.Y.F.; Feng, J.Y.; Chan, Y.J.; Su, W.J. The Risk of TB in Patients with Type 2 Diabetes Initiating Metformin vs. Sulfonylurea Treatment. Chest 2018, 153, 1347–1357. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin Decreases Risk of Tuberculosis Infection in Type 2 Diabetes Patients. J. Clin. Med. 2018, 7, E264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Shaer, M.H.; Elewa, H.; Alkabab, Y.; Nazer, L.H.; Heysell, S.K. Fixed-dose combination associated with faster time to smear conversion compared to separate tablets of anti-tuberculosis drugs in patients with poorly controlled diabetes and pulmonary tuberculosis in Qatar. BMC Infect. Dis. 2018, 18, 384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Yang, B.R.; Song, H.J.; Jang, S.H.; Kang, D.Y.; Park, B.J. Metformin and tuberculosis risk in elderly patients with diabetes mellitus. Int. J. Tuberc. Lung Dis. 2019, 23, 924–930. [Google Scholar] [CrossRef]
- Fu, C.P.; Lee, C.L.; Li, Y.H.; Lin, S.Y. Metformin as a potential protective therapy against tuberculosis in patients with diabetes mellitus: A retrospective cohort study in a single teaching hospital. J. Diabetes Investig. 2021, 12, 1603–1609. [Google Scholar] [CrossRef]
- Chen, H.H.; Hsieh, M.C.; Ho, C.W.; Chen, C.C.; Hsu, S.P.; Lin, C.L.; Kao, C.H. Effects of dipeptidyl peptidase-4 inhibitor treatment doses on tuberculosis in patients with diabetes: A long-term nationwide population-based cohort study. Ann. Palliat. Med. 2020, 9, 2817–2825. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Highlights of Prescribing Information. Kombiglyze® XR (Saxagliptin and Metformin Hydrochloride Extended-Release). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/200678s024lbl.pdf (accessed on 8 September 2022).
- Su, W.J.; Pan, S.W.; Yen, Y.F.; Su, V.Y.; Chuang, P.H.; Feng, J.Y. The Effect of Metformin Versus Sulfonylurea on the Risk of Tuberculosis Disease in Patients with Type 2 Diabetes Mellitus: A Population-Based Cohort Study. Am. J. Respir. Crit. Care Med. 2018, 197, A4313. [Google Scholar]
- Bailey, C.J.; Iqbal, N.; T’joen, C.; List, J.F. Dapagliflozin monotherapy in drug-naïve patients with diabetes: A randomized-controlled trial of low-dose range. Diabetes Obes. Metab. 2012, 14, 951–959. [Google Scholar] [CrossRef]
- WHO Collaborating Centre for Drug Statistics Methodology. Definition and General Considerations. Available online: https://www.whocc.no/ddd/definition_and_general_considera/ (accessed on 9 September 2022).
- Narasimhan, P.; Wood, J.; MacIntyre, C.R.; Mathai, D. Risk Factors for Tuberculosis. Pulm. Med. 2013, 2013, 828939. [Google Scholar] [CrossRef]
- Meregildo-Rodriguez, E.D.; Chunga-Chévez, E.V.; Robles-Arce, L.G.; Vásquez-Tirado, G.A. Further insights into to the role of statins against active tuberculosis: Systematic review and meta-analysis. Infez. Med. 2022, 30, 194–203. [Google Scholar]
- Duan, H.; Liu, T.; Zhang, X.; Yu, A.; Cao, Y. Statin use and risk of tuberculosis: A systemic review of observational studies. Int. J. Infect. Dis. 2020, 93, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Sheng, L.; Lou, L. Statin Use May Be Associated with Reduced Active Tuberculosis Infection: A Meta-Analysis of Observational Studies. Front. Med. 2020, 7, 121. [Google Scholar] [CrossRef] [PubMed]
- Scifres, C.M.; Iams, J.D.; Klebanoff, M.; Macones, G.A. Meta-Analysis versus Large Clinical Trials: Which Should Guide Our Management? Am. J. Obstet. Gynecol. 2009, 200, e1–e484. [Google Scholar] [CrossRef]
- Paul, M.; Leeflang, M.M. Reporting of systematic reviews and meta-analysis of observational studies. Clin. Microbiol. Infect. 2021, 27, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Nie, X.; Wu, Z.; Zhang, Y.; Feng, G.; Cai, S.; Lv, Y.; Peng, X. Can statistic adjustment of OR minimize the potential confounding bias for meta-analysis of case-control study? A secondary data analysis. BMC Med. Res. Methodol. 2017, 17, 179. [Google Scholar] [CrossRef]
- Saxagliptin and tuberculosis. Prescrire Int. 2013, 22, 17.
- Saxagliptin. No more effective than other gliptins, but a high potential for drug interactions. Prescrire Int. 2011, 20, 33–37.






| Author | Study | Tool | Conclusion |
|---|---|---|---|
| Padmapriydarsini C. [7]. 2022. Multicentric (India) study. | Phase 3 RCT. | ROB 2 | Low risk |
| Bailey C.J. [30]. 1212. Multicentric (USA, Canada, Mexico, Russia, India, South Africa and Puerto Rico) study. | RCT | ROB 2 | Low risk |
| Heo E. [8]. 2021. Korea. | RCS | NOS | Low risk |
| Lee Y.J. [15]. 2018. South Korea. | RCS | NOS | Low risk |
| Lin H.F. [17]. 2017. Taiwan. | RCS | NOS | Low risk |
| Degner N.R. [16]. 2018. Taiwan. | RCS | NOS | Low risk |
| Lee M.C. [20]. 2018. Taiwan. | RCS | NOS | Low risk |
| Lin S.Y. [18]. 2018. Taiwan. | RCS | NOS | Low risk |
| Pan S.W. et al. [22]. 2018. Taiwan. | RCS | NOS | Low risk |
| Tseng C.H. [23]. 2018. Taiwan. | RCS | NOS | Low risk |
| Al-Shaer M.H. [24]. 2018. Qatar. | RCS | NOS | Low risk |
| Park S. [25]. 2019. South Korea. | RCS | NOS | Low risk |
| Lee M.C. [21]. 2019. Taiwan. | RCS | NOS | Low risk |
| Fu C.P. [26]. 2021. Taiwan. | RCS | NOS | Low risk |
| Chen H.H. [27]. 2020. Taiwan. | RCS | NOS | Low risk |
| FDA [28]. 2010. USA. RCT | RCS | NOS | Low risk |
| Su W.J. [29]. 2018. Taiwan. | RCS | NOS | Low risk |
| Lin K.H. [19]. 2020. Taiwan. | CCS | NOS | Low risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meregildo-Rodriguez, E.D.; Asmat-Rubio, M.G.; Zavaleta-Alaya, P.; Vásquez-Tirado, G.A. Effect of Oral Antidiabetic Drugs on Tuberculosis Risk and Treatment Outcomes: Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 343. https://doi.org/10.3390/tropicalmed7110343
Meregildo-Rodriguez ED, Asmat-Rubio MG, Zavaleta-Alaya P, Vásquez-Tirado GA. Effect of Oral Antidiabetic Drugs on Tuberculosis Risk and Treatment Outcomes: Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2022; 7(11):343. https://doi.org/10.3390/tropicalmed7110343
Chicago/Turabian StyleMeregildo-Rodriguez, Edinson Dante, Martha Genara Asmat-Rubio, Petterson Zavaleta-Alaya, and Gustavo Adolfo Vásquez-Tirado. 2022. "Effect of Oral Antidiabetic Drugs on Tuberculosis Risk and Treatment Outcomes: Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 7, no. 11: 343. https://doi.org/10.3390/tropicalmed7110343