
Transforming Growth Factor-β Concerning Malarial Infection and Severity: A Systematic Review and Meta-Analysis
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. PICO Questions
2.3. Eligibility Criteria
2.4. Information Sources
2.5. Study Selection
2.6. Definitions
2.7. Data Extraction
2.8. Quality of the Included Studies
2.9. Outcomes
2.10. Data Syntheses
3. Results
3.1. Search Results
3.2. Characteristics and Quality of the Included Studies
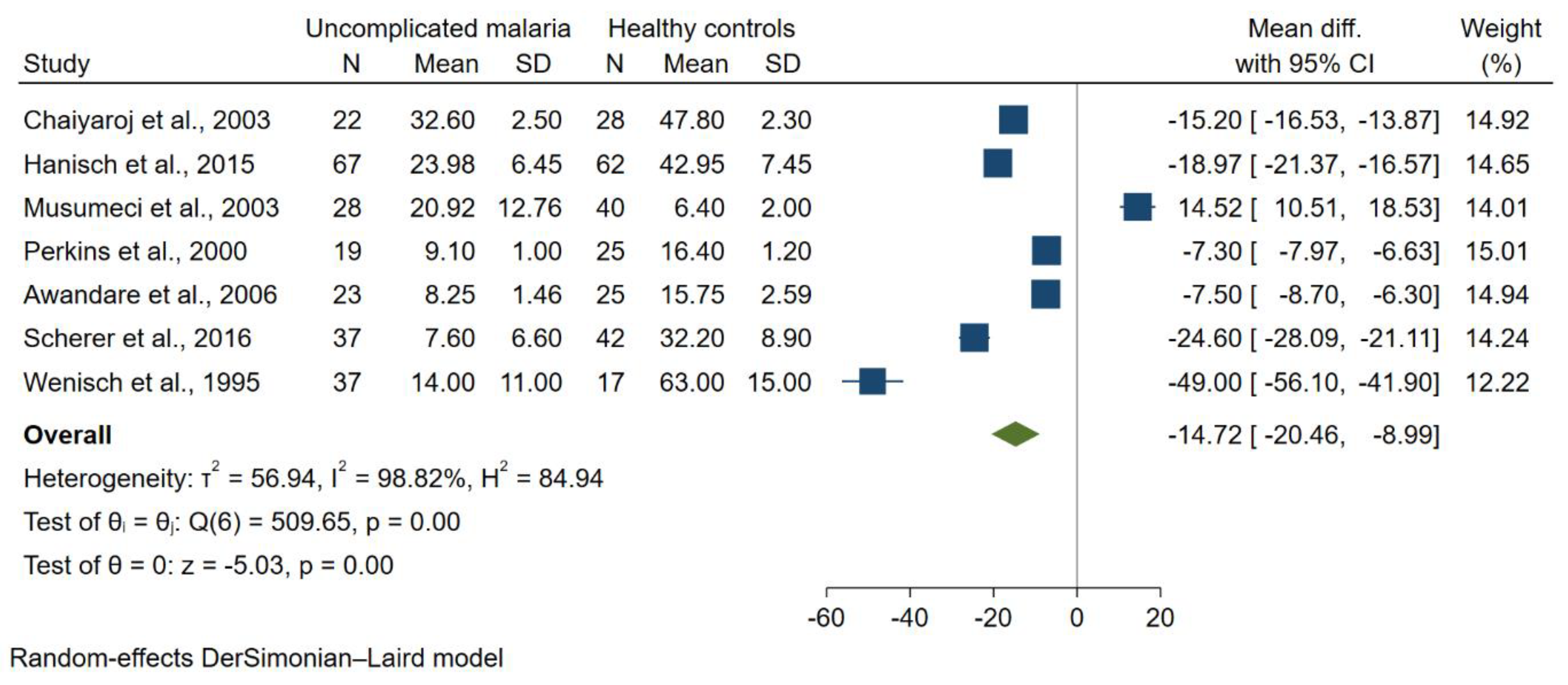
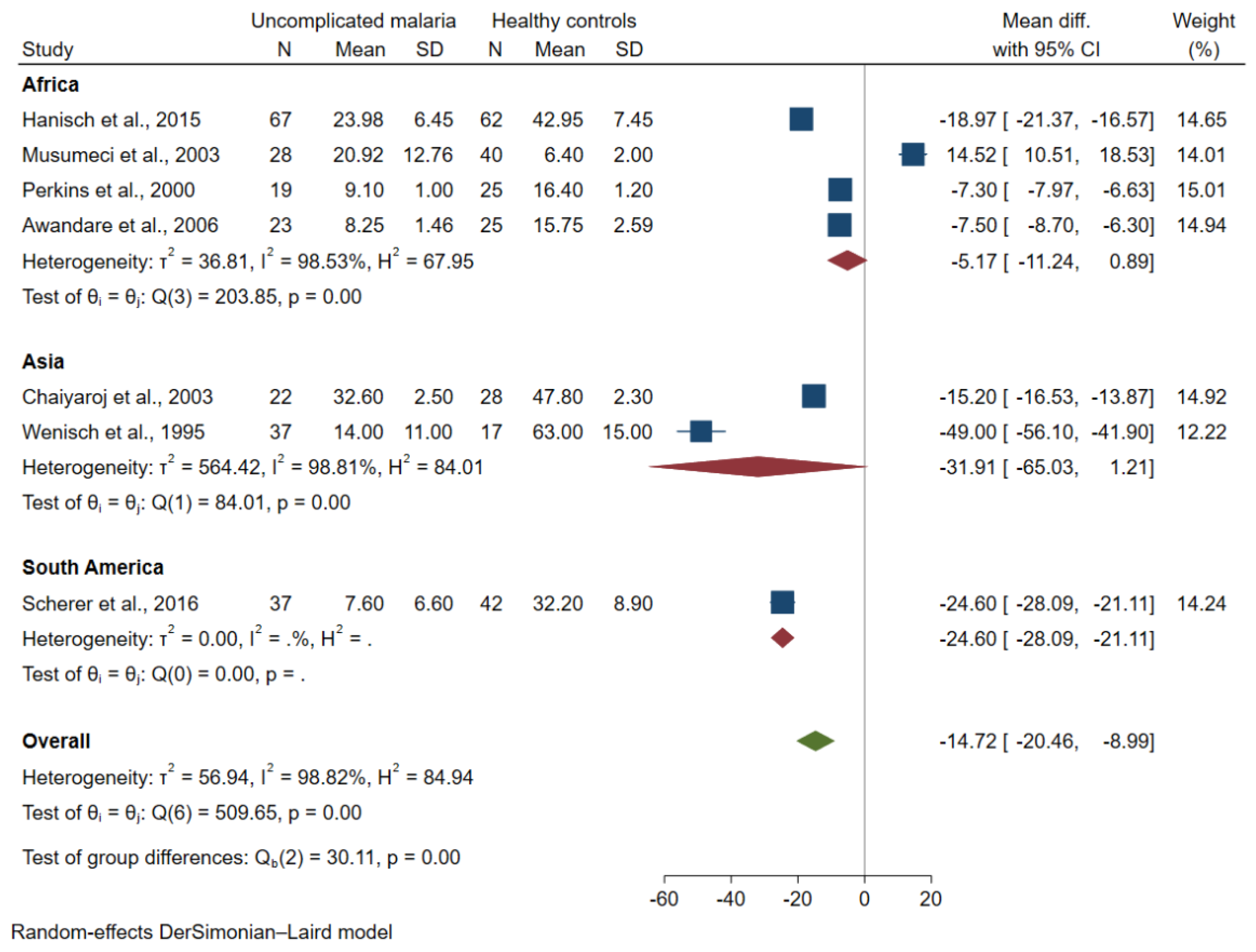
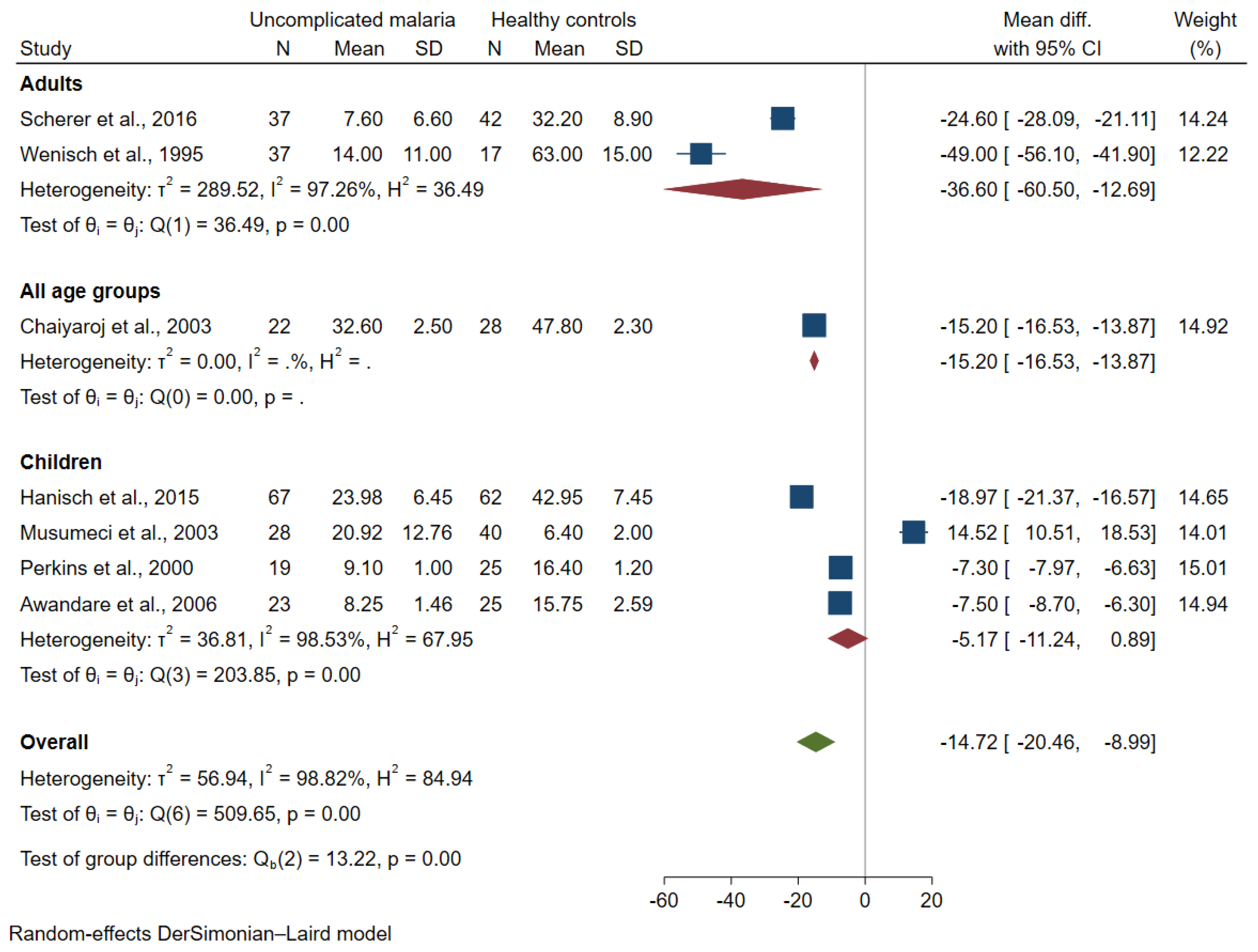
3.3. TGF-β Levels between Uncomplicated Malaria and Healthy Controls
3.4. TGF-β Levels between Severe and Uncomplicated Malaria
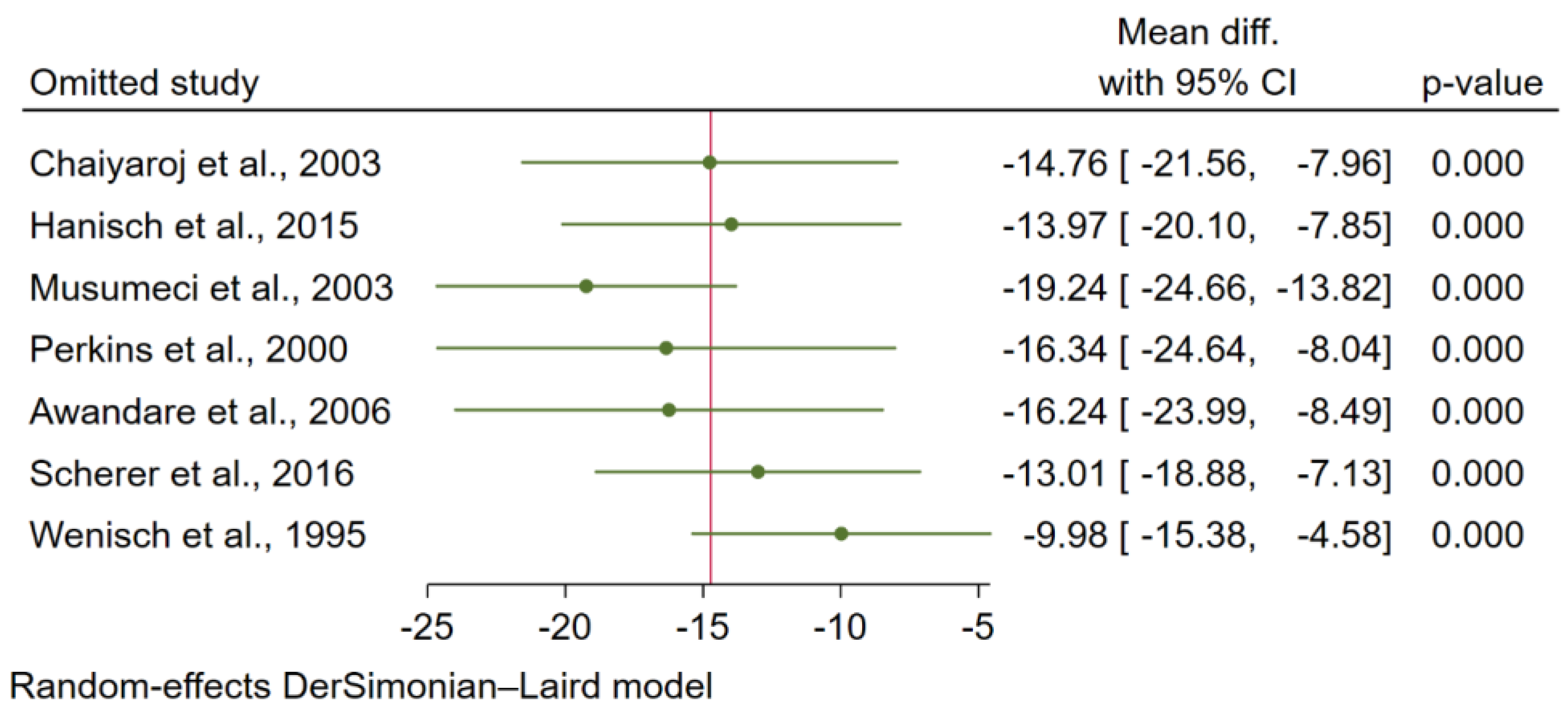
3.5. Sensitivity Analysis
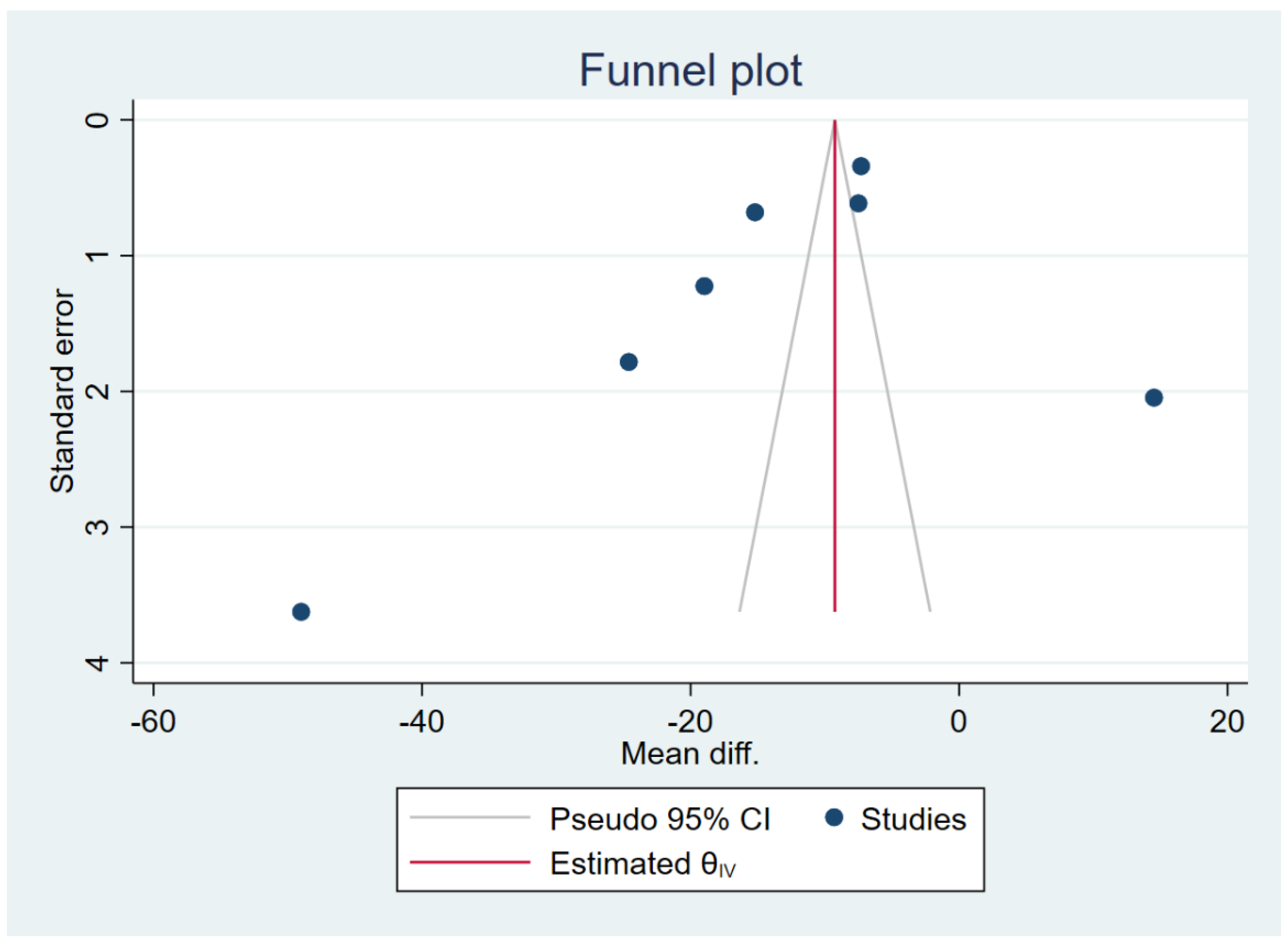
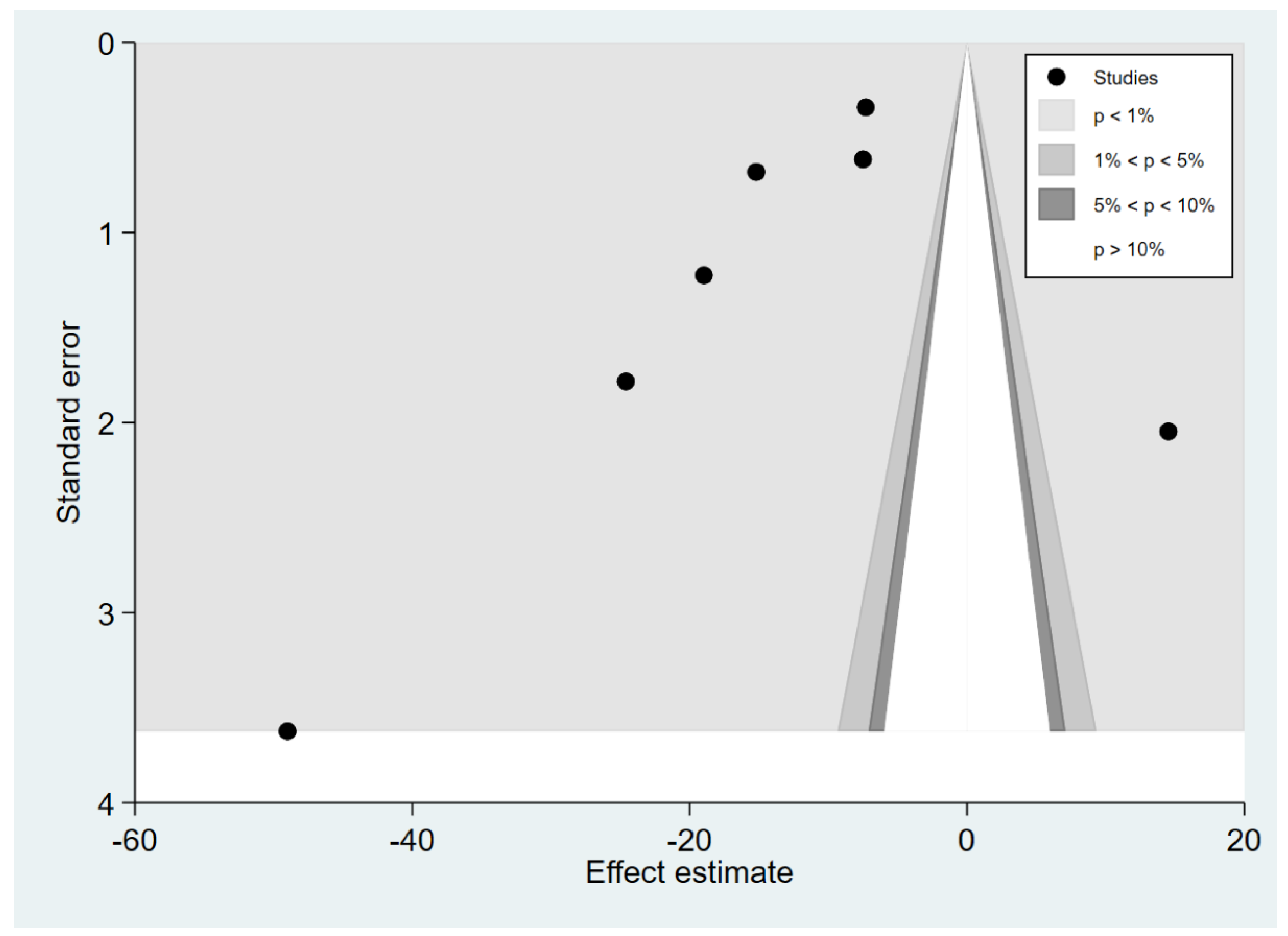
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2021; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.J.; Masangkay, F.R. Prevalence and risk factors related to poor outcome of patients with severe Plasmodium vivax infection: A systematic review, meta-analysis, and analysis of case reports. BMC Infect. Dis. 2020, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Severity and mortality of severe Plasmodium ovale infection: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235014. [Google Scholar] [CrossRef] [PubMed]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Prevalence of severe Plasmodium knowlesi infection and risk factors related to severe complications compared with non-severe P. knowlesi and severe P. falciparum malaria: A systematic review and meta-analysis. Infect. Dis. Poverty 2020, 9, 106. [Google Scholar] [CrossRef] [PubMed]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Global prevalence and mortality of severe Plasmodium malariae infection: A systematic review and meta-analysis. Malar J. 2020, 19, 274. [Google Scholar] [CrossRef]
- McCall, M.B.; Sauerwein, R.W. Interferon-gamma-central mediator of protective immune responses against the pre-erythrocytic and blood stage of malaria. J. Leukoc. Biol. 2010, 88, 1131–1143. [Google Scholar] [CrossRef] [Green Version]
- Torre, D.; Speranza, F.; Martegani, R. Role of proinflammatory and anti-inflammatory cytokines in the immune response to Plasmodium falciparum malaria. Lancet Infect. Dis. 2002, 2, 719–720. [Google Scholar] [CrossRef]
- Sporn, M.B. TGF-beta: 20 years and counting. Microbes Infect. 1999, 1, 1251–1253. [Google Scholar] [CrossRef]
- Drewry, L.L.; Harty, J.T. Balancing in a black box: Potential immunomodulatory roles for TGF-β signaling during blood-stage malaria. Virulence 2020, 11, 159–169. [Google Scholar] [CrossRef] [Green Version]
- de Larco, J.E.; Todaro, G.J. Growth factors from murine sarcoma virus-transformed cells. Proc. Natl. Acad. Sci. USA 1978, 75, 4001–4005. [Google Scholar] [CrossRef] [Green Version]
- Prud’homme, G.J. Pathobiology of transforming growth factor beta in cancer, fibrosis and immunologic disease, and therapeutic considerations. Lab. Investig. J. Tech. Methods Pathol. 2007, 87, 1077–1091. [Google Scholar] [CrossRef]
- Moustakas, A.; Heldin, C.H. Non-Smad TGF-beta signals. J. Cell Sci. 2005, 118, 3573–3584. [Google Scholar] [CrossRef] [PubMed]
- Segarini, P.R.; Rosen, D.M.; Seyedin, S.M. Binding of transforming growth factor-β to cell surface proteins varies with cell type. Mol. Endocrinol. 1989, 3, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gougos, A.; Letarte, M. Primary structure of endoglin, an RGD-containing glycoprotein of human endothelial cells. J. Biol. Chem. 1990, 265, 8361–8364. [Google Scholar] [CrossRef]
- Tian, M.; Neil, J.R.; Schiemann, W.P. Transforming growth factor-β and the hallmarks of cancer. Cell. Signal. 2011, 23, 951–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.A.; Li, M.O. TGF-β: Guardian of T cell function. J. Immunol. 2013, 191, 3973–3979. [Google Scholar] [CrossRef] [Green Version]
- Li, M.O.; Wan, Y.Y.; Sanjabi, S.; Robertson, A.K.; Flavell, R.A. Transforming growth factor-beta regulation of immune responses. Annu. Rev. Immunol. 2006, 24, 99–146. [Google Scholar] [CrossRef] [PubMed]
- Thomson, A.W.; Lotze, M.T. The Cytokine Handbook, Two-Volume Set; Elsevier: Amsterdam, The Netherlands, 2003. [Google Scholar]
- Sanjabi, S.; Oh, S.A.; Li, M.O. Regulation of the immune response by tgf-beta: From conception to autoimmunity and infection. Cold Spring Harb. Perspect. Biol. 2017, 9, a022236. [Google Scholar] [CrossRef] [Green Version]
- Barral, A.; Barral-Netto, M.; Yong, E.C.; Brownell, C.E.; Twardzik, D.R.; Reed, S.G. Transforming growth factor beta as a virulence mechanism for Leishmania braziliensis. Proc. Natl. Acad. Sci. USA 1993, 90, 3442–3446. [Google Scholar] [CrossRef] [Green Version]
- Grainger, J.R.; Smith, K.A.; Hewitson, J.P.; McSorley, H.J.; Harcus, Y.; Filbey, K.J.; Finney, C.A.; Greenwood, E.J.; Knox, D.P.; Wilson, M.S.; et al. Helminth secretions induce de novo T cell Foxp3 expression and regulatory function through the TGF-β pathway. J. Exp. Med. 2010, 207, 2331–2341. [Google Scholar] [CrossRef]
- Halsey, E.S.; Baldeviano, G.C.; Edgel, K.A.; Vilcarromero, S.; Sihuincha, M.; Lescano, A.G. Symptoms and Immune Markers in Plasmodium/Dengue Virus Co-infection Compared with Mono-infection with Either in Peru. PLoS Negl. Trop. Dis. 2016, 10, e0004646. [Google Scholar] [CrossRef]
- Nyirenda, T.S.; Molyneux, M.E.; Kenefeck, R.; Walker, L.S.; MacLennan, C.A.; Heyderman, R.S.; Mandala, W.L. T-Regulatory cells and inflammatory and inhibitory cytokines in malawian children residing in an area of high and an area of low malaria transmission during acute uncomplicated malaria and in convalescence. J. Pediatric Infect. Dis. Soc. 2015, 4, 232–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, V.S.; Imade, G.E.; Molta, N.B.; Tawde, P.; Pam, S.D.; Obadofin, M.O.; Sagay, S.A.; Egah, D.Z.; Iya, D.; Afolabi, B.B.; et al. Cytokine-associated neutrophil extracellular traps and antinuclear antibodies in Plasmodium falciparum infected children under six years of age. Malar J. 2008, 7, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esamai, F.; Ernerudh, J.; Janols, H.; Welin, S.; Ekerfelt, C.; Mining, S.; Forsberg, P. Cerebral malaria in children: Serum and cerebrospinal fluid TNF-α and TGF-β levels and their relationship to clinical outcome. J. Trop. Pediatrics 2003, 49, 216–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanisch, B.R.; Bangirana, P.; Opoka, R.O.; Park, G.S.; John, C.C. Thrombocytopenia may mediate disease severity in Plasmodium falciparum malaria through reduced transforming growth factor beta-1 regulation of proinflammatory and anti-inflammatory cytokines. Pediatric Infect. Dis. J. 2015, 34, 783–788. [Google Scholar] [CrossRef] [Green Version]
- Chaiyaroj, S.C.; Rutta, A.S.; Muenthaisong, K.; Watkins, P.; Na Ubol, M.; Looareesuwan, S. Reduced levels of transforming growth factor-beta1, interleukin-12 and increased migration inhibitory factor are associated with severe malaria. Acta Trop. 2004, 89, 319–327. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines for Malaria; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials. 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awandare, G.A.; Hittner, J.B.; Kremsner, P.G.; Ochiel, D.O.; Keller, C.C.; Weinberg, J.B.; Clark, I.A.; Perkins, D.J. Decreased circulating macrophage migration inhibitory factor (MIF) protein and blood mononuclear cell MIF transcripts in children with Plasmodium falciparum malaria. Clin. Immunol. 2006, 119, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Budiningsih, I.; Dachlan, Y.P.; Hadi, U.; Middeldorp, J.M. Quantitative cytokine level of TNF-α, IFN-γ, IL-10, TGF-β and circulating Epstein-Barr virus DNA load in individuals with acute Malaria due to P. falciparum or P. vivax or double infection in a Malaria endemic region in Indonesia. PLoS ONE 2021, 16, e0261923. [Google Scholar] [CrossRef] [PubMed]
- Bwanika, R.; Kato, C.D.; Welishe, J.; Mwandah, D.C. Cytokine profiles among patients co-infected with Plasmodium falciparum malaria and soil borne helminths attending Kampala International University Teaching Hospital, in Uganda. Allergy Asthma Clin. Immunol. 2018, 14, 10. [Google Scholar] [CrossRef]
- Hojo-Souza, N.S.; Pereira, D.B.; de Souza, F.S.; de Oliveira Mendes, T.A.; Cardoso, M.S.; Tada, M.S.; Zanini, G.M.; Bartholomeu, D.C.; Fujiwara, R.T.; Bueno, L.L. On the cytokine/chemokine network during Plasmodium vivax malaria: New insights to understand the disease. Malar J. 2017, 16, 42. [Google Scholar] [CrossRef] [Green Version]
- Nsubuga, J.; Kato, C.D.; Nanteza, A.; Matovu, E.; Alibu, V.P. Plasma cytokine profiles associated with rhodesiense sleeping sickness and falciparum malaria co-infection in North Eastern Uganda. Allergy Asthma Clin. Immunol. 2019, 15, 63. [Google Scholar] [CrossRef] [PubMed]
- Scherer, E.F.; Cantarini, D.G.; Siqueira, R.; Ribeiro, E.B.; Braga, É.M.; Honório-França, A.C.; França, E.L. Cytokine modulation of human blood viscosity from vivax malaria patients. Acta Trop. 2016, 158, 139–147. [Google Scholar] [CrossRef]
- Wenisch, C.; Parschalk, B.; Burgmann, H.; Looareesuwan, S.; Graninger, W. Decreased serum levels of TGF-β in patients with acute Plasmodium falciparum malaria. J. Clin. Immunol. 1995, 15, 69–73. [Google Scholar] [CrossRef]
- Musumeci, M.; Malaguarnera, L.; Simporè, J.; Messina, A.; Musumeci, S. Modulation of immune response in Plasmodium falciparum malaria: Role of IL-12, IL-18 and TGF-β. Cytokine 2003, 21, 172–178. [Google Scholar] [CrossRef]
- Olupot-Olupot, P.; Urban, B.C.; Jemutai, J.; Nteziyaremye, J.; Fanjo, H.M.; Karanja, H.; Karisa, J.; Ongodia, P.; Bwonyo, P.; Gitau, E.N.; et al. Endotoxaemia is common in children with Plasmodium falciparum malaria. BMC Infect. Dis. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, D.J.; Weinberg, J.B.; Kremsner, P.G. Reduced interleukin-12 and transforming growth factor-beta1 in severe childhood malaria: Relationship of cytokine balance with disease severity. J. Infect. Dis. 2000, 182, 988–992. [Google Scholar] [CrossRef]
- Prakash, D.; Fesel, C.; Jain, R.; Cazenave, P.A.; Mishra, G.C.; Pied, S. Clusters of cytokines determine malaria severity in Plasmodium falciparum-infected patients from endemic areas of central India. J. Infect. Dis. 2006, 194, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, Y.; Gotoh, Y.; Uemura, O.; Tanaka, S.; Ando, T.; Nishida, M. Age-dependent decrease in serum transforming growth factor (TGF)-beta 1 in healthy Japanese individuals; population study of serum TGF-beta 1 level in Japanese. Dis. Markers 2005, 21, 71–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrington, L.; Vance, H.; Rek, J.; Prahl, M.; Jagannathan, P.; Katureebe, A.; Arinaitwe, E.; Kamya, M.R.; Dorsey, G.; Feeney, M.E. Both inflammatory and regulatory cytokine responses to malaria are blunted with increasing age in highly exposed children. Malar J. 2017, 16, 499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omer, F.M.; Kurtzhals, J.A.; Riley, E.M. Maintaining the immunological balance in parasitic infections: A role for TGF-beta? Parasitol. Today 2000, 16, 18–23. [Google Scholar] [CrossRef]
- Mahittikorn, A.; Mala, W.; Srisuphanunt, M.; Masangkay, F.R.; Kotepui, K.U.; Wilairatana, P.; Kotepui, M. Tumour necrosis factor-alpha as a prognostic biomarker of severe malaria: A systematic review and meta-analysis. J. Travel. Med. 2022, 29, taac053. [Google Scholar] [CrossRef]
- Diallo, T.O.; Remoue, F.; Schacht, A.M.; Charrier, N.; Dompnier, J.P.; Pillet, S.; Garraud, O.; N’Diaye, A.A.; Capron, A.; Capron, M.; et al. Schistosomiasis co-infection in humans influences inflammatory markers in uncomplicated Plasmodium falciparum malaria. Parasite Immunol. 2004, 26, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Walther, M.; Tongren, J.E.; Andrews, L.; Korbel, D.; King, E.; Fletcher, H.; Andersen, R.F.; Bejon, P.; Thompson, F.; Dunachie, S.J.; et al. Upregulation of TGF-beta, FOXP3, and CD4+CD25+ regulatory T cells correlates with more rapid parasite growth in human malaria infection. Immunity 2005, 23, 287–296. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | % |
|---|---|---|
| Study designs | ||
| Prospective observational studies | 6 | 46.2 |
| Case–control studies | 3 | 23.1 |
| Cross-sectional studies | 3 | 23.1 |
| Cohort study | 1 | 7.69 |
| Study areas | ||
| Africa | 7 | 53.8 |
| Asia | 4 | 30.8 |
| South America | 2 | 15.4 |
| Plasmodium spp. | ||
| P. falciparum | 10 | 76.9 |
| P. vivax | 2 | 15.4 |
| P. falciparum/P. vivax/mixed infection | 1 | 7.69 |
| Participants | ||
| Children | 6 | 46.2 |
| Adults | 4 | 30.8 |
| All age groups | 3 | 23.1 |
| Methods for malaria detection | ||
| Microscopy | 9 | 69.2 |
| Microscopy/RDT | 2 | 15.4 |
| Microscopy/PCR | 2 | 15.4 |
| Methods for TGF-β quantification | ||
| ELISA | 11 | 84.6 |
| Bead-based assay | 2 | 15.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotepui, K.U.; Kwankaew, P.; Masangkay, F.R.; Mahittikorn, A.; Kotepui, M. Transforming Growth Factor-β Concerning Malarial Infection and Severity: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 299. https://doi.org/10.3390/tropicalmed7100299
Kotepui KU, Kwankaew P, Masangkay FR, Mahittikorn A, Kotepui M. Transforming Growth Factor-β Concerning Malarial Infection and Severity: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2022; 7(10):299. https://doi.org/10.3390/tropicalmed7100299
Chicago/Turabian StyleKotepui, Kwuntida Uthaisar, Pattamaporn Kwankaew, Frederick Ramirez Masangkay, Aongart Mahittikorn, and Manas Kotepui. 2022. "Transforming Growth Factor-β Concerning Malarial Infection and Severity: A Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 7, no. 10: 299. https://doi.org/10.3390/tropicalmed7100299