
A Cluster of Plasmodium ovale Infections in Belgian Military Personnel after Deployment in Kindu, Democratic Republic of Congo: A Retrospective Study

 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
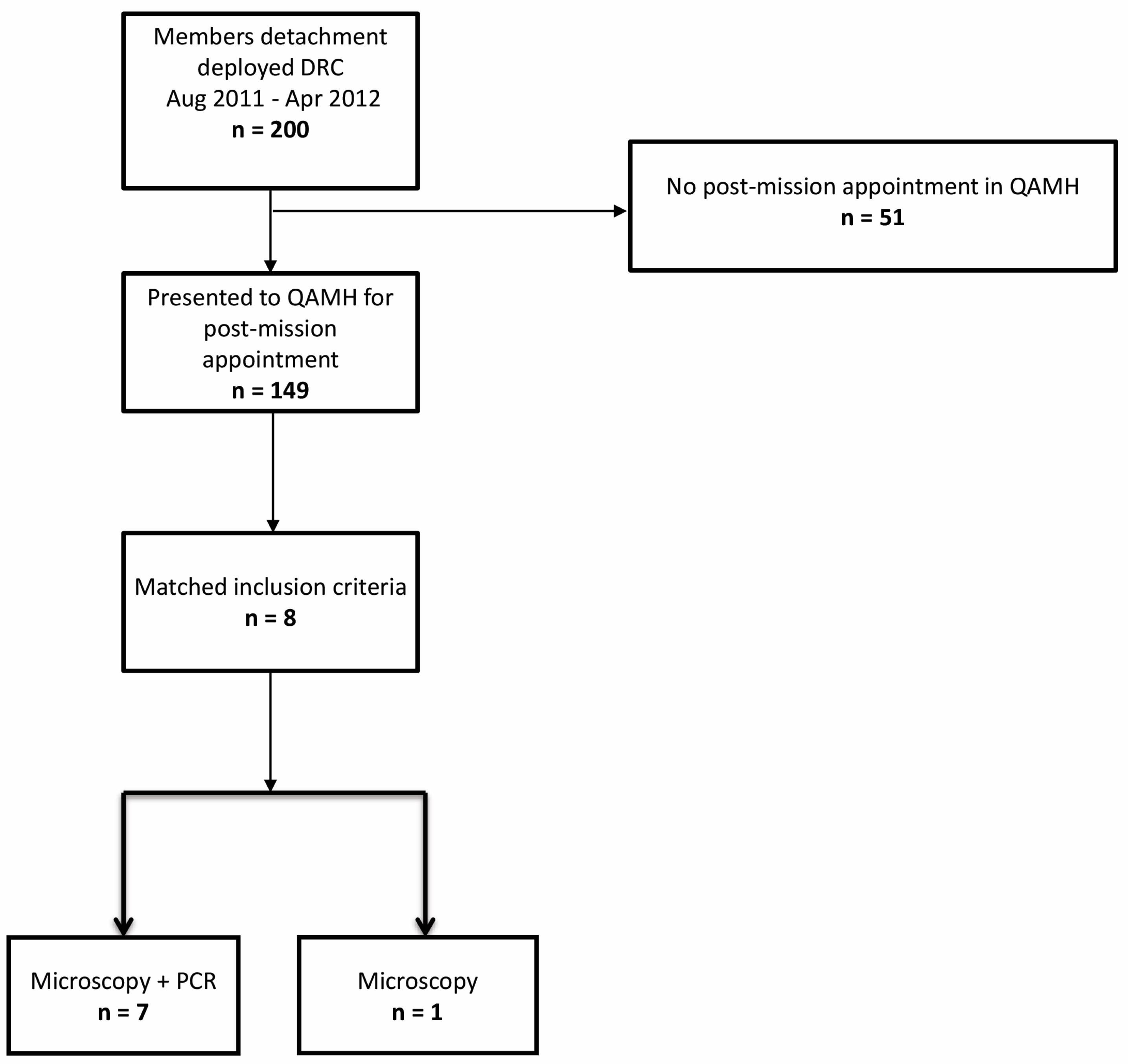
2.1. Study Design and Population
Inclusion Criteria
- a positive thick and thin smear showing P. ovale parasites and/or;
- a positive polymerase chain reaction (PCR) for P. ovale.
2.2. Definitions and Microbiology
2.3. Statistics
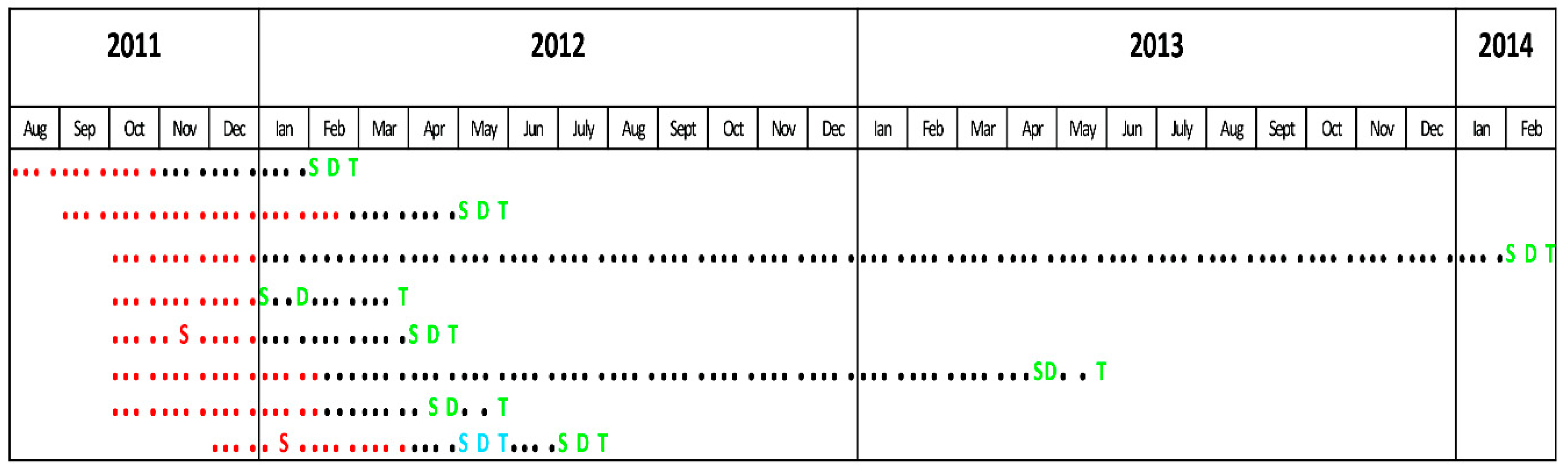
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, M.E.; Weld, L.; Boggild, A.; Keystone, J.S.; Kain, K.; Von Sonnenburg, F.; Schwartz, E.; Network, G.S. Fever in returned travelers: Results from the geosentinel surveillance network. Clin. Infect. Dis. 2007, 44, 1560–1568. [Google Scholar] [CrossRef] [Green Version]
- Bottieau, E.; Clerinx, J.; Enden, E.V.D.; Van Esbroeck, M.; Colebunders, R.; Van Gompel, A.; Ende, J.V.D. Fever After a Stay in the Tropics. Medicine 2007, 86, 18–25. [Google Scholar] [CrossRef]
- Ciminera, P.; Brundage, J. Malaria in U.S. military forces: A description of deployment exposures from 2003 through 2005. Am. J. Trop. Med. Hyg. 2007, 76, 275–279. [Google Scholar] [CrossRef]
- Beiter, K.J.; Wentlent, Z.J.; Hamouda, A.R.; Thomas, B.N. Nonconventional opponents: A review of malaria and leishmaniasis among United States Armed Forces. PeerJ 2019, 7, e6313. [Google Scholar] [CrossRef]
- Groger, M.; Fischer, H.S.; Veletzky, L.; Lalremruata, A.; Ramharter, M. A systematic review of the clinical presentation, treatment and relapse characteristics of human Plasmodium ovale malaria. Malar. J. 2017, 16, 112. [Google Scholar] [CrossRef] [Green Version]
- de Laval, F.; Simon, F.; Bogreau, H.; Rapp, C.; Wurtz, N.; Oliver, M.; Demaison, X.; Dia, A.; De Pina, J.J.; Merens, A.; et al. Emergence of Plasmodium ovale Malaria Among the French Armed Forces in the Republic of Ivory Coast: 20 Years of Clinical and Biological Experience. Clin. Infect. Dis. 2014, 58, e122–e128. [Google Scholar] [CrossRef] [Green Version]
- Armed Forces Health Surveillance Branch. Update: Malaria, U.S. Armed Forces, 2016. MSMR 2017, 24, 2–7. [Google Scholar]
- Guerra, R.I.; Ore, M.; Valdivia, H.O.; Bishop, D.K.; Ramos, M.; Mores, C.N.; Campbell, W.R. A cluster of the first reported Plasmodium ovale spp. infections in Peru occuring among returning UN peace-keepers, a review of epidemiology, prevention and diagnostic challenges in nonendemic regions. Malar. J. 2019, 18, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LiWang, F.; Ratih, D.M.; Lardo, S. Plasmodium ovale infection after one year mefloquine prophylaxis in a young indonesian soldier: A case report. Acta Med. Indones. 2019, 51, 59–62. [Google Scholar]
- Leder, K.; Black, J.; O’Brien, D.; Greenwood, Z.; Kain, K.; Schwartz, E.; Brown, G.; Torresi, J. Malaria in travelers: A review of the geosentinel surveillance network. Clin. Infect. Dis. 2004, 39, 1104–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, S.I.; Okiro, E.A.; Gething, P.W.; Patil, A.P.; Tatem, A.J.; Guerra, C.A.; Snow, R.W. Estimating the global clinical burden of plasmodium falciparum malaria in 2007. PLoS Med. 2010, 7, e1000290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.M.; Messina, J.P.; Hand, C.C.; Juliano, J.J.; Muwonga, J.; Tshefu, A.K.; Atua, B.; Emch, M.; Meshnick, S.R. Molecular malaria epidemiology: Mapping and burden estimates for the democratic republic of the congo, 2007. PLoS ONE 2011, 6, e16420. [Google Scholar] [CrossRef] [Green Version]
- Cnops, L.; Jacobs, J.; Van Esbroeck, M. Validation of a four-primer real-time PCR as a diagnostic tool for single and mixed Plasmodium infections. Clin. Microbiol. Infect. 2011, 17, 1101–1107. [Google Scholar] [CrossRef] [Green Version]
- Demedts, P.; Wery, M. Indirect immunofluorescence using differentiating antigens in detection of imported malaria. Ann. Soc. Belg. Med. Trop. 1985, 65 (Suppl. 2), 89–96. [Google Scholar]
- Croft, A.M. A lesson learnt: The rise and fall of Lariam and Halfan. J. R Soc. Med. 2007, 100, 170–174. [Google Scholar] [CrossRef] [Green Version]
- Tickell-Painter, M.; Maayan, N.; Saunders, R.; Pace, C.; Sinclair, D. Mefloquine for preventing malaria during travel to endemic areas. Cochrane Database Syst. Rev. 2017, 10, CD006491, PMCID:PMC5686653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, V.; Daily, J.P. Tafenoquine. Curr. Opin. Infect. Dis. 2019, 32, 407–412. [Google Scholar] [CrossRef]
- Marty, P.; Chapdelaine, B.; Le Fichoux, Y.; Chabert, J.M. Paludisme anémiant à Plasmodium ovale après 45 mois d’incubation (Anemic Plasmodium ovale malaria after 45 months’ incubation). Presse Med. 1987, 16, 357. [Google Scholar]
- Rojo-Marcos, G.; Cuadros-González, J.; Gete-García, L.; Gómez-Herruz, P.; Lopez-Rubio, M.; Esteban-Gutiérrez, G. Infección por Plasmodium ovale: Descripción de 16 casos y revisión del tema. Enferm. Infecc. Y Microbiol. Clínica 2011, 29, 204–208. [Google Scholar] [CrossRef]
- Mellon, G.; Ficko, C.; Thellier, M.; Kendjo, M.E.; Aoun, O.; Adriamanantena, D.; Rapp, C. The French national reference center for imported malaria study group two cases of late plasmodium ovale presentation in military personnel. J. Travel Med. 2014, 21, 52–54. [Google Scholar] [CrossRef] [Green Version]
- Milne, L.M.; Kyi, M.S.; Chiodini, P.L.; Warhurst, D.C. Accuracy of routine laboratory diagnosis of malaria in the United Kingdom. J. Clin. Pathol. 1994, 47, 740–742. [Google Scholar] [CrossRef] [Green Version]
- Grobusch, M.P.; Hanscheid, T.; Zoller, T.; Jelinek, T.; Burchard, G.D. Rapid immunochromatographic malarial antigen detection unreliable for detecting plasmodium malariae and plasmodium ovale. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 818–820. [Google Scholar] [CrossRef] [PubMed]
- Bigaillon, C.; Fontan, E.; Cavallo, J.-D.; Hernandez, E.; Spiegel, A. Ineffectiveness of the Binax NOW malaria test for diagnosis of plasmodium ovale Malaria. J. Clin. Microbiol. 2005, 43, 1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yerlikaya, S.; Campillo, A.; Gonzalez, I.J. A Systematic Review: Performance of Rapid Diagnostic Tests for the Detection of Plasmodium knowlesi, Plasmodium malariae, and Plasmodium ovale Monoinfections in Human Blood. J. Infect. Dis. 2018, 218, 265–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doderer-Lang, C.; Atchade, P.S.; Meckert, L.; Haar, E.; Perrotey, S.; Filisetti, D.; Aboubacar, A.; Pfaff, A.W.; Brunet, J.; Chabi, N.W.; et al. The ears of the African elephant: Unexpected high seroprevalence of Plasmodium ovale and Plasmodium malariae in healthy populations in Western Africa. Malar. J. 2014, 13, 240. [Google Scholar] [CrossRef]
- CDC Malaria Treatment Guidelines for Clinicians. Available online: https://www.cdc.gov/malaria/diagnosis_treatment/clinicians1.html#treatment (accessed on 1 June 2021).
- Epelboin, L.; Rapp, C.; Faucher, J.; Méchaï, F.; Bottieau, E.; Matheron, S.; Malvy, D.; Caumes, E. Management and treatment of uncomplicated imported malaria in adults. Update of the French malaria clinical guidelines. Médecine Mal. Infect. 2020, 50, 194–212. [Google Scholar] [CrossRef]
- Arnsten, J.H.; Demas, P.A.; Farzadegan, H.; Grant, R.; Gourevitch, M.; Chang, C.; Buono, D.; Eckholdt, H.; Howard, A.A.; Schoenbaum, E.E. Antiretroviral therapy adherence and viral suppression in HIV-Infected drug users: Comparison of self-report and electronic monitoring. Clin. Infect. Dis. 2001, 33, 1417–1423. [Google Scholar] [CrossRef]
- Landry, P.; Iorillo, D.; Darioli, R.; Burnier, M.; Genton, B. Do Travelers Really Take Their Mefloquine Malaria Chemoprophylaxis? Estimation of Adherence by an Electronic Pillbox. J. Travel Med. 2006, 13, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, C.L.; Brazeau, N.F.; Keeler, C.; Mwandagalirwa, M.K.; Tshefu, A.K.; Juliano, J.J.; Meshnick, S.R. Under the radar: Epidemiology of plasmodium ovale in the democratic republic of the congo. J. Infect. Dis. 2020, 223, 1005–1014. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costescu Strachinaru, D.I.; Wauters, A.; Van Esbroeck, M.; Strachinaru, M.; Vanbrabant, P.; Soentjens, P. A Cluster of Plasmodium ovale Infections in Belgian Military Personnel after Deployment in Kindu, Democratic Republic of Congo: A Retrospective Study. Trop. Med. Infect. Dis. 2021, 6, 125. https://doi.org/10.3390/tropicalmed6030125
Costescu Strachinaru DI, Wauters A, Van Esbroeck M, Strachinaru M, Vanbrabant P, Soentjens P. A Cluster of Plasmodium ovale Infections in Belgian Military Personnel after Deployment in Kindu, Democratic Republic of Congo: A Retrospective Study. Tropical Medicine and Infectious Disease. 2021; 6(3):125. https://doi.org/10.3390/tropicalmed6030125
Chicago/Turabian StyleCostescu Strachinaru, Diana Isabela, An Wauters, Marjan Van Esbroeck, Mihai Strachinaru, Peter Vanbrabant, and Patrick Soentjens. 2021. "A Cluster of Plasmodium ovale Infections in Belgian Military Personnel after Deployment in Kindu, Democratic Republic of Congo: A Retrospective Study" Tropical Medicine and Infectious Disease 6, no. 3: 125. https://doi.org/10.3390/tropicalmed6030125