
Cardiomyopathy and Death Following Chikungunya Infection: An Increasingly Common Outcome



Abstract
:1. Introduction
2. Materials and Methods
3. Results
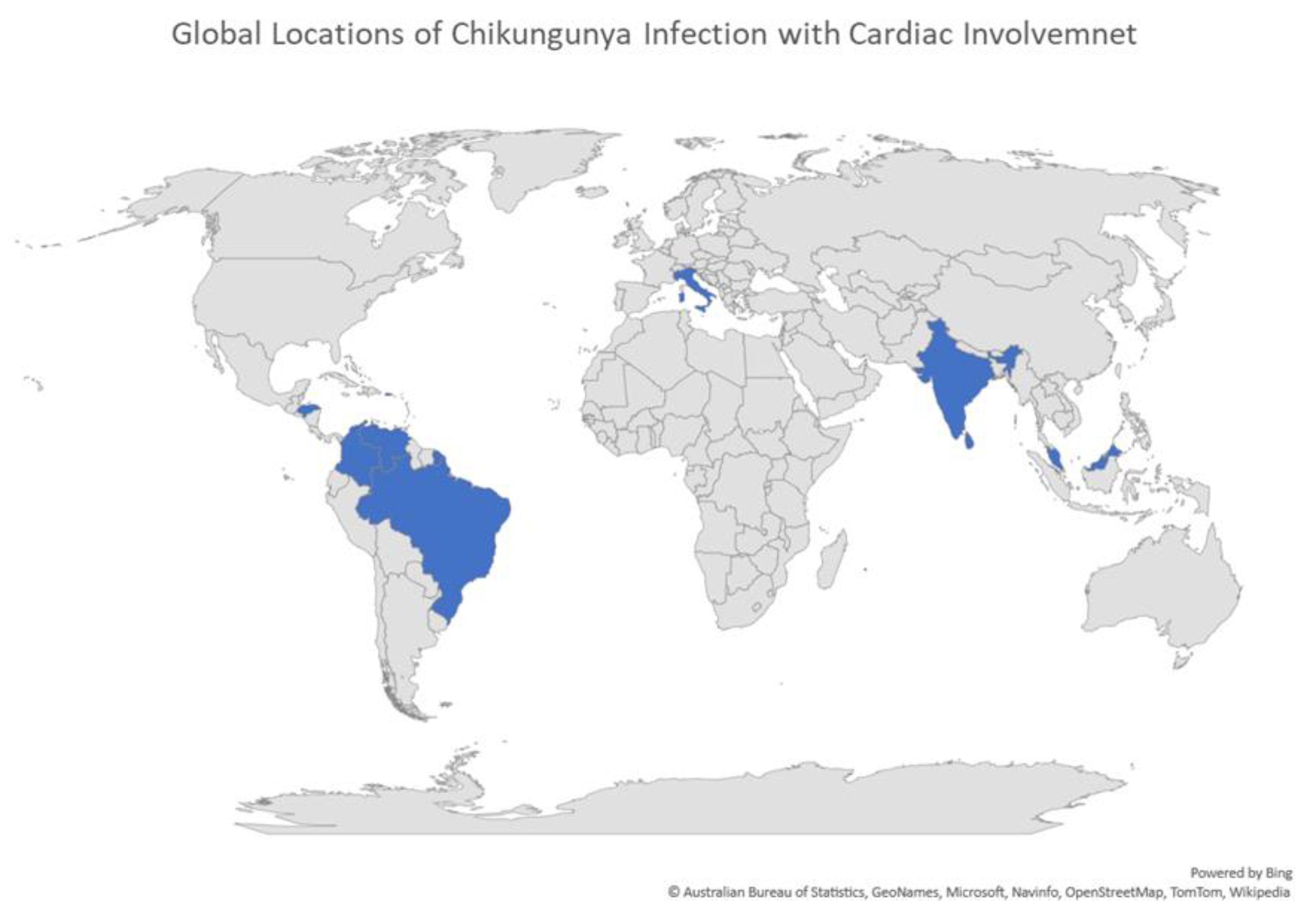
3.1. Locations of CHIKV Infections with Cardiac Symptoms
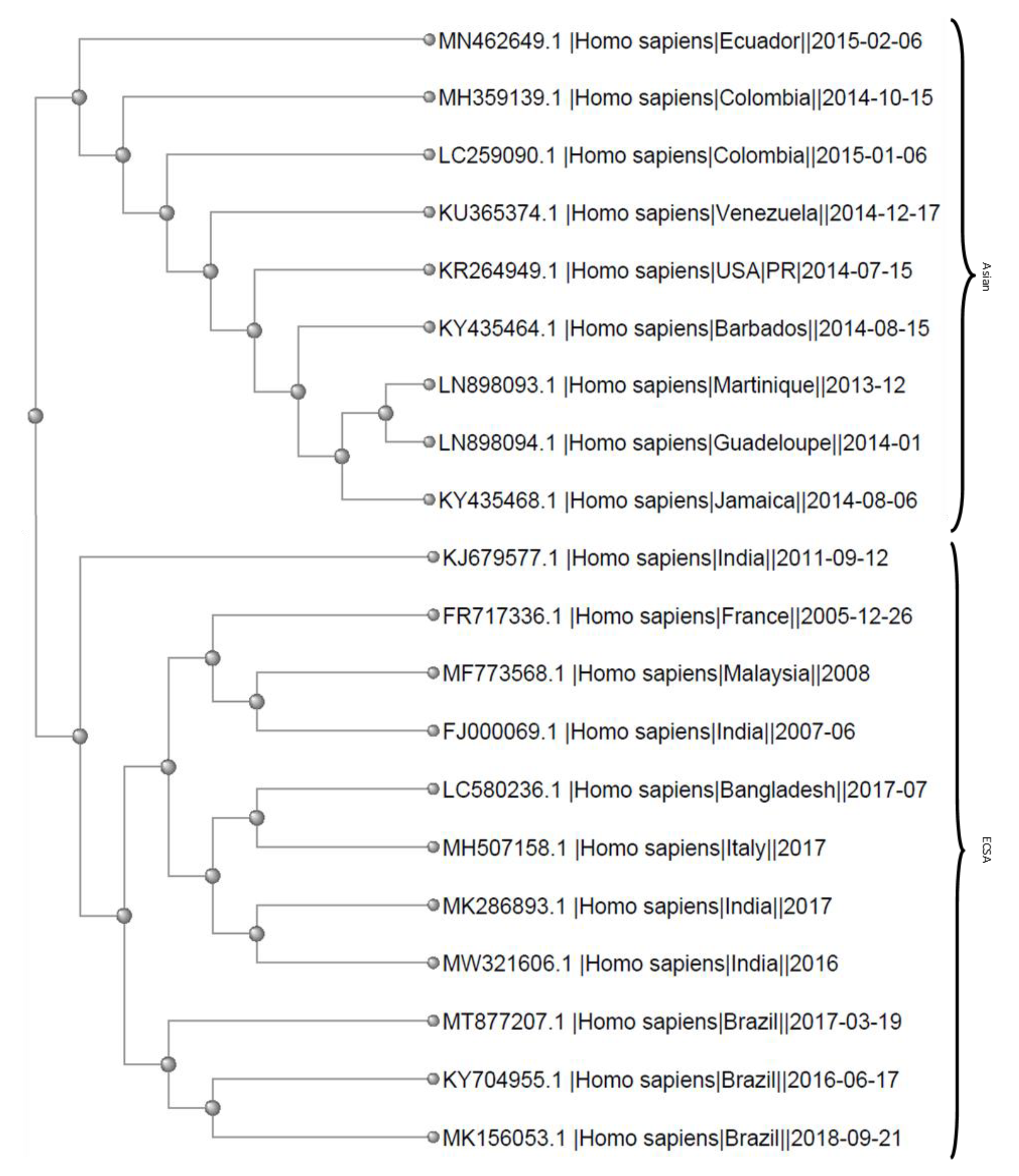
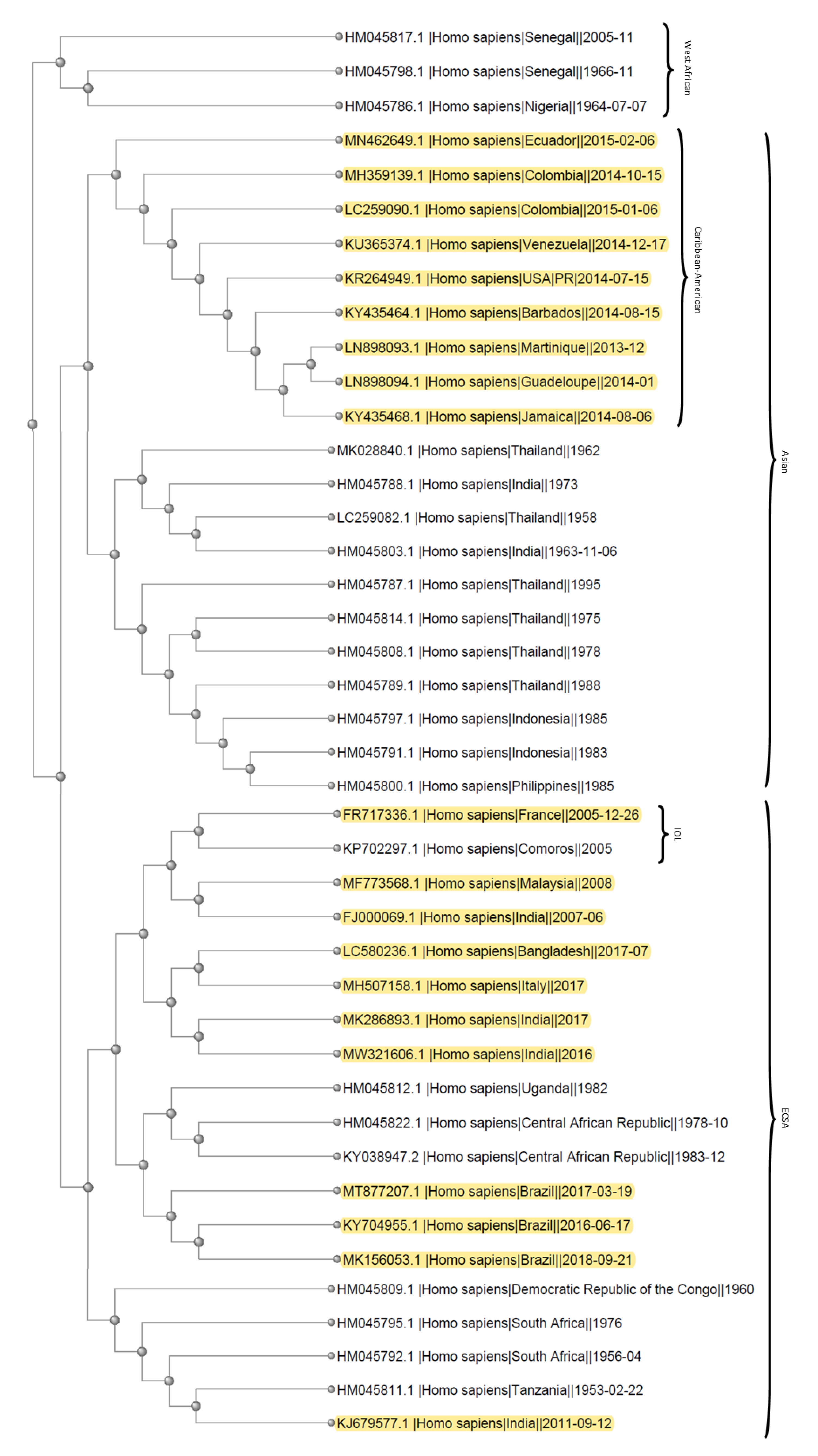
3.2. Phylogenetics
3.3. CHIKV Causes Cardiac Symptoms and Death
3.4. Clinical Features of Single Patient Case Reports
3.5. Clinical Features of Patients from Clinical Studies with Multiple Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zeller, H.; Van Bortel, W.; Sudre, B. Chikungunya: Its History in Africa and Asia and Its Spread to New Regions in 2013–2014|The Journal of Infectious Diseases|Oxford Academic. Available online: https://academic.oup.com/jid/article/214/suppl_5/S436/2632642 (accessed on 30 January 2021).
- Barr, K.L.; Vaidhyanathan, V. Chikungunya in Infants and Children: Is Pathogenesis Increasing? Viruses 2019, 11, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lum, F.-M.; Ng, L.F.P. Cellular and Molecular Mechanisms of Chikungunya Pathogenesis. Antiviral Res. 2015, 120, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Sourisseau, M.; Schilte, C.; Casartelli, N.; Trouillet, C.; Guivel-Benhassine, F.; Rudnicka, D.; Sol-Foulon, N.; Roux, K.L.; Prevost, M.-C.; Fsihi, H.; et al. Characterization of Reemerging Chikungunya Virus. PLoS Pathog. 2007, 3, e89. [Google Scholar] [CrossRef]
- Ozden, S.; Huerre, M.; Riviere, J.-P.; Coffey, L.L.; Afonso, P.V.; Mouly, V.; de Monredon, J.; Roger, J.-C.; El Amrani, M.; Yvin, J.-L.; et al. Human Muscle Satellite Cells as Targets of Chikungunya Virus Infection. PLoS ONE 2007, 2, e527. [Google Scholar] [CrossRef] [PubMed]
- Yactaya, S.; Staples, J.E.; Millot, V.; Cibrelus, L.; Ramon-Pardo, P. Epidemiology of Chikungunya in the Americas. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5137246/ (accessed on 31 January 2021).
- Matusali, G.; Colavita, F.; Bordi, L.; Lalle, E.; Ippolito, G.; Capobianchi, M.R.; Castilletti, C. Tropism of the Chikungunya Virus. Viruses 2019, 11, 175. [Google Scholar] [CrossRef] [Green Version]
- Cunha, M.S.; Costa, P.A.G.; Correa, I.A.; de Souza, M.R.M.; Calil, P.T.; da Silva, G.P.D.; Costa, S.M.; Fonseca, V.W.P.; da Costa, L.J. Chikungunya Virus: An Emergent Arbovirus to the South American Continent and a Continuous Threat to the World. Front. Microbiol. 2020, 11. [Google Scholar] [CrossRef]
- McSweegan, E.; Weaver, S.C.; Lecuit, M.; Frieman, M.; Morrison, T.E.; Hrynkow, S. The Global Virus Network: Challenging Chikungunya. Antivir. Res. 2015, 120, 147–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahendradas, P.; Avadhani, K.; Shetty, R. Chikungunya and the Eye: A Review. J. Ophthalmic Inflamm. Infect. 2013, 3, 35. [Google Scholar] [CrossRef] [Green Version]
- Villero-Wolf, Y.; Mattar, S.; Puerta-González, A.; Arrieta, G.; Muskus, C.; Hoyos, R.; Pinzon, H.; Peláez-Carvajal, D. Genomic Epidemiology of Chikungunya Virus in Colombia Reveals Genetic Variability of Strains and Multiple Geographic Introductions in Outbreak, 2014. Sci. Rep. 2019, 9, 9970. [Google Scholar] [CrossRef]
- Xavier, J.; Giovanetti, M.; Fonseca, V.; Thézé, J.; Gräf, T.; Fabri, A.; Goes de Jesus, J.; Lima de Mendonça, M.C.; Damasceno dos Santos Rodrigues, C.; Mares-Guia, M.A.; et al. Circulation of Chikungunya Virus East/Central/South African Lineage in Rio de Janeiro, Brazil. PLoS ONE 2019, 14, e0217871. [Google Scholar] [CrossRef]
- Rezza, G.; Weaver, S.C. PLOS Neglected Tropical Diseases: Chikungunya as a Paradigm for Emerging Viral Diseases: Evaluating Disease Impact and Hurdles to Vaccine Development. Available online: https://journals.plos.org/plosntds/article/figure?id=10.1371/journal.pntd.0006919.g001 (accessed on 6 February 2021).
- Bonifay, T.; Prince, C.; Neyra, C.; Demar, M.; Rousset, D.; Kallel, H.; Nacher, M.; Djossou, F.; Epelboin, L. Atypical and Severe Manifestations of Chikungunya Virus Infection in French Guiana: A Hospital-Based Study. PLoS ONE 2018, 13, e0207406. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, M.F.; Bolívar-Mejía, A.; Rodriguez-Morales, A.J.; Ramirez-Vallejo, E. Cardiovascular Involvement and Manifestations of Systemic Chikungunya Virus Infection: A Systematic Review. F1000Research 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Godaert, L.; Nicolon, C.; Najioullah, F.; Kanagaratnam, L.; Césaire, R.; Dramé, M. Is Chikungunya Virus Infection an Independent Risk Factor for 2-Year Mortality in Older Afro-Caribbean Subjects? Infect. Drug Resist. 2020, 13, 2223–2228. [Google Scholar] [CrossRef] [PubMed]
- Vairo, F.; Haider, N.; Kock, R.; Ntoumi, F.; Ippolito, G.; Zumla, A. Chikungunya: Epidemiology, Pathogenesis, Clinical Features, Management, and Prevention. Infect. Dis. Clin. N. Am. 2019, 33, 1003–1025. [Google Scholar] [CrossRef]
- Kearney, M.; Cotton, J.; Richardson, P.; Shah, A. Viral Myocarditis and Dilated Cardiomyopathy: Mechanisms, Manifestations, and Management. Postgrad. Med. J. 2001, 77, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Schultz, J.C.; Hilliard, A.A.; Cooper, L.T.; Rihal, C.S. Diagnosis and Treatment of Viral Myocarditis. Mayo Clin. Proc. 2009, 84, 1001–1009. [Google Scholar] [CrossRef] [Green Version]
- Lima Neto, A.S.; Sousa, G.S.; Nascimento, O.J.; Castro, M.C. Chikungunya-Attributable Deaths: A Neglected Outcome of a Neglected Disease. PLoS Negl. Trop. Dis. 2019, 13, e0007575. [Google Scholar] [CrossRef] [Green Version]
- Frutuoso, L.C.V.; Freitas, A.R.R.; Cavalcanti, L.P.d.G.; Duarte, E.C. Estimated Mortality Rate and Leading Causes of Death among Individuals with Chikungunya in 2016 and 2017 in Brazil. Available online: https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0037-86822020000100316 (accessed on 31 January 2021).
- Guaraldo, L.; Wakimoto, M.D.; Ferreira, H.; Bressan, C.; Calvet, G.A.; Pinheiro, G.C.; Siqueira, A.M.; Brasil, P. Treatment of Chikungunya Musculoskeletal Disorders: A Systematic Review. Expert Rev. Anti Infect. Ther. 2018, 16, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Hatcher, E.L.; Zhdanov, S.A.; Bao, Y.; Blinkova, O.; Nawrocki, E.P.; Ostapchuck, Y.; Schäffer, A.A.; Brister, J.R. Virus Variation Resource-Improved Response to Emergent Viral Outbreaks. Nucleic Acids Res. 2017, 45, D482–D490. [Google Scholar] [CrossRef] [PubMed]
- Obeyesekere, I.; Hermon, Y. Myocarditis and Cardiomyopathy after Arbovirus Infections (Dengue and Chikungunya Fever). Br. Heart J. 1972, 34, 821–827. [Google Scholar] [CrossRef] [Green Version]
- Obeyesekere, I.; Hermon, Y. Arbovirus Heart Disease: Myocarditis and Cardiomyopathy Following Dengue and Chikungunya Fever--a Follow-up Study. Am. Heart J. 1973, 85, 186–194. [Google Scholar] [CrossRef]
- Maiti, C.R.; Mukherjee, A.K.; Bose, B.; Saha, G.L. Myopericarditis Following Chikungunya Virus Infection. J. Indian Med. Assoc. 1978, 70, 256–258. [Google Scholar]
- Nasci, R.S. Movement of Chikungunya Virus into the Western Hemisphere. Emerg. Infect. Dis. 2014, 20, 1394–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, A.M.; Logue, C.H. Changing Patterns of Chikungunya Virus: Re-Emergence of a Zoonotic Arbovirus. J. Gen. Virol. 2007, 88, 2363–2377. [Google Scholar] [CrossRef] [PubMed]
- Gauzere, B.; Bohrer, M.; Drouet, D.; Gasque, P.; Jaffar-Bandjee, M.C.; Filleul, L.; Vandroux, D. Infection à virus Chikungunya à La Réunion en 2005–2006: Formes graves émergentes de l’adulte en réanimation. Médecine Intensive Réanimation 2011, 20, 211–222. [Google Scholar]
- Lemant, J.; Boisson, V.; Winer, A.; Thibault, L.; André, H.; Tixier, F.; Lemercier, M.; Antok, E.; Cresta, M.P.; Grivard, P.; et al. Serious Acute Chikungunya Virus Infection Requiring Intensive Care during the Reunion Island Outbreak in 2005–2006. Crit. Care Med. 2008, 36, 2536–2541. [Google Scholar] [CrossRef] [PubMed]
- Economopoulou, A.; Dominguez, M.; Helynck, B.; Sissoko, D.; Wichmann, O.; Quenel, P.; Germonneau, P.; Quatresous, I. Atypical Chikungunya Virus Infections: Clinical Manifestations, Mortality and Risk Factors for Severe Disease during the 2005-2006 Outbreak on Réunion. Epidemiol. Infect. 2009, 137, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Ramful, D.; Carbonnier, M.; Pasquet, M.; Bouhmani, B.; Ghazouani, J.; Noormahomed, T.; Beullier, G.; Attali, T.; Samperiz, S.; Fourmaintraux, A.; et al. Mother-to-Child Transmission of Chikungunya Virus Infection. Pediatr. Infect. Dis. J. 2007, 26, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Ernould, S.; Walters, H.; Alessandri, J.-L.; Llanas, B.; Jaffar, M.-C.; Robin, S.; Attali, T.; Ramful, D.; Combes, J.-C. [Chikungunya in paediatrics: Epidemic of 2005–2006 in Saint-Denis, Reunion Island]. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2008, 15, 253–262. [Google Scholar] [CrossRef]
- Pellot, A.S.; Alessandri, J.L.; Robin, S.; Sampériz, S.; Attali, T.; Brayer, C.; Pasquet, M.; Jaffar-Bandjee, M.C.; Benhamou, L.S.; Tiran-Rajaofera, I.; et al. Severe forms of chikungunya virus infection in a pediatric intensive care unit on Reunion Island. Med. Trop. Rev. Corps Sante Colon. 2012, 72, 88–93. [Google Scholar]
- Bessaud, M.; Peyrefitte, C.N.; Pastorino, B.A.M.; Tock, F.; Merle, O.; Colpart, J.-J.; Dehecq, J.-S.; Girod, R.; Jaffar-Bandjee, M.-C.; Glass, P.J.; et al. Chikungunya Virus Strains, Reunion Island Outbreak. Emerg. Infect. Dis. 2006, 12, 1604–1605. [Google Scholar] [CrossRef]
- Dilip, C.; Saraswathi, R.; Krishnan, P.; Azeem, A.; Raseena, A.; Ramya, J. Comparitive Evaluation of Different Systems of Medicines and the Present Scenario of Chikungunya in Kerala. Asian Pac. J. Trop. Med. 2010, 3, 443–447. [Google Scholar] [CrossRef] [Green Version]
- Sam, I.C.; Kamarulzaman, A.; Ong, G.S.Y.; Veriah, R.S.; Ponnampalavanar, S.; Chan, Y.F.; AbuBakar, S. Chikungunya Virus-Associated Death in Malaysia. Trop. Biomed. 2010, 27, 343–347. [Google Scholar] [PubMed]
- Menon, P.R.; Krishnan, C.; Sankar, J.; Gopinathan, K.M.; Mohan, G. A Child with Serious Chikungunya Virus (CHIKV) Infection Requiring Intensive Care, after an Outbreak. Indian J. Pediatr. 2010, 77, 1326–1328. [Google Scholar] [CrossRef]
- Wimalasiri-Yapa, B.M.C.R.; Stassen, L.; Huang, X.; Hafner, L.M.; Hu, W.; Devine, G.J.; Yakob, L.; Jansen, C.C.; Faddy, H.M.; Viennet, E.; et al. Chikungunya Virus in Asia-Pacific: A Systematic Review. Emerg. Microbes Infect. 2019, 8, 70–79. [Google Scholar] [CrossRef]
- Kumar, N.P.; Sabesan, S.; Krishnamoorthy, K.; Jambulingam, P. Detection of Chikungunya Virus in Wild Populations of Aedes Albopictus in Kerala State, India. Vector-Borne Zoonotic Dis. 2012, 12, 907–911. [Google Scholar] [CrossRef]
- Chua, H.H.; Abdul Rashid, K.; Law, W.C.; Hamizah, A.; Chem, Y.K.; Khairul, A.H.; Chua, K.B. A Fatal Case of Chikungunya Virus Infection with Liver Involvement. Med. J. Malaysia 2010, 65, 83–84. [Google Scholar]
- Nigam, A.; Sharma, S.; Jain, A.; Gupta, A.; Prakash, A. Vertical Transmission of Chikungunya Manifesting as Foetal Pericardial Effusion. J. Assoc. Phys. India 2016, 64, 76–79. [Google Scholar] [PubMed]
- Crosby, L.; Perreau, C.; Madeux, B.; Cossic, J.; Armand, C.; Herrmann-Storke, C.; Najioullah, F.; Valentino, R.; Thiéry, G. Severe Manifestations of Chikungunya Virus in Critically Ill Patients during the 2013-2014 Caribbean Outbreak. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2016, 48, 78–80. [Google Scholar] [CrossRef] [Green Version]
- Thiery, G.; Crosby, L.; Perreau, C.; Madeux, B.; Cossic, J.; Armand, C.; Herrmann-Storcke, C.; Najioullah, F.; Valentino, R. Critically Ill Patients with Chikungunya Virus Infection during the Carribean Outbreak 2013–2014. Intensive Care Med. Exp. 2015, 3. [Google Scholar] [CrossRef] [Green Version]
- Evans-Gilbert, T. Chikungunya and Neonatal Immunity: Fatal Vertically Transmitted Chikungunya Infection. Am. J. Trop. Med. Hyg. 2017, 96, 913–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendoza, I.; Morr, I.; Mendoza, I.; Morr, C.; Morr, C.; Meza, Y.; Marques, J.; Villalobos, I. Chikungunya myocarditis: An emerging threat to america|Journal of the American College of Cardiology. Available online: https://www.jacc.org/doi/full/10.1016/s0735-1097%2815%2960946-9 (accessed on 31 January 2021).
- Morr-García, I.; Mendoza, I.; Octavio, J.A.; Villalobos, I.; Meza, Y.; Mendoza-Britto, I.; González, K.; Morr-Verenzuela, C.; Morr-Verenzuela, C.; Marques, J. PP. 02.25: Chikungunya induces persistent arterial hypotension in hypertensive patients. J. Hypertens. 2015, 33, e146. [Google Scholar] [CrossRef]
- Gonzalez Carta Karina, A.; Mendoza_Britto Ivan, J.; Finizola, V.; Morr, I.; Torres, J.; Meza, Y.; Marquez, J.; Villalobos, I.; Vasquez, R.; Chazzim, G. Abstract 13292: Bradycardia as a Manifestation of Chikungunya Myocarditis. A New Threat to America. Circulation 2016, 134, A13292. [Google Scholar] [CrossRef]
- Torres, J.R.; Leopoldo, C.G.; Castro, J.S.; Rodríguez, L.; Saravia, V.; Arvelaez, J.; Ríos-Fabra, A.; Longhi, M.A.; Marcano, M. Chikungunya Fever: Atypical and Lethal Cases in the Western Hemisphere: A Venezuelan Experience. IDCases 2015, 2, 6–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Best, C.; Benskin, G. Epidemiology, Clinical and Laboratory Features and Course of Chikungunya among a Cohort of Children during the First Caribbean Epidemic. J. Trop. Pediatr. 2017, 63, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Gavotto, A.; Muanza, B.; Delion, F.; Dusacre, J.-A.; Amedro, P. Chikungunya Disease among Infants in French West Indies during the 2014 Outbreak. Arch. Pédiatrie 2019, 26, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Koeltz, A.; Lastere, S.; Jean-Baptiste, S. Intensive Care Admissions for Severe Chikungunya Virus Infection, French Polynesia. Emerg. Infect. Dis. 2018, 24, 794–796. [Google Scholar] [CrossRef]
- Sharp, T.M.; Keating, M.K.; Shieh, W.-J.; Bhatnager, J. Clinical Characteristics, Histopathology, and Tissue Immunolocalization of Chikungunya Virus Antigen in Fatal Cases|Clinical Infectious Diseases|Oxford Academic. Available online: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa837/5866622 (accessed on 31 January 2021).
- Arocho, J.; Sarasua, A.; Irizarry, J.; Puig-Ramos, A.; Puig, G. 664: Strategic management of critically ill pediatric patien: Critical Care Medicine. Available online: https://journals.lww.com/ccmjournal/Citation/2019/01001/664__STRATEGIC_MANAGEMENT_OF_CRITICALLY_ILL.627.aspx (accessed on 31 January 2021).
- Freitas, A.R.R.; Donalisio, M.R.; Alarcón-Elbal, P.M. Excess Mortality and Causes Associated with Chikungunya, Puerto Rico, 2014–2015. Emerg. Infect. Dis. 2018, 24, 2352–2355. [Google Scholar] [CrossRef]
- López, P.; De Jesús, O.; García-Justiniano, J.; Rivera-Amill, V. Novel Molecular Signatures of Chikungunya Virus in Puerto Rico. P. R. Health Sci. J. 2019, 38, 27–32. [Google Scholar]
- Torres, J.R.; Falleiros-Arlant, L.H.; Dueñas, L.; Pleitez-Navarrete, J.; Salgado, D.M.; Castillo, J.B.-D. Congenital and Perinatal Complications of Chikungunya Fever: A Latin American Experience. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2016, 51, 85–88. [Google Scholar] [CrossRef] [Green Version]
- van Enter, B.J.D.; Huibers, M.H.W.; van Rooij, L.; Steingrover, R.; van Hensbroek, M.B.; Voigt, R.R.; Hol, J. Perinatal Outcomes in Vertically Infected Neonates During a Chikungunya Outbreak on the Island of Curaçao. Am. J. Trop. Med. Hyg. 2018, 99, 1415–1418. [Google Scholar] [CrossRef]
- van Ewijk, R.; Huibers, M.H.W.; Manshande, M.E.; Ecury-Goossen, G.M.; Duits, A.J.; Calis, J.C.; van Wassenaer-Leemhuis, A.G. Neurologic Sequelae of Severe Chikungunya Infection in the First 6 Months of Life: A Prospective Cohort Study 24-Months Post-Infection. BMC Infect. Dis. 2021, 21, 179. [Google Scholar] [CrossRef]
- Villamil-Gómez, W.; Alba-Silvera, L.; Menco-Ramos, A.; Gonzalez-Vergara, A.; Molinares-Palacios, T.; Barrios-Corrales, M.; Rodríguez-Morales, A.J. Congenital Chikungunya Virus Infection in Sincelejo, Colombia: A Case Series. J. Trop. Pediatr. 2015, 61, 386–392. [Google Scholar] [CrossRef] [Green Version]
- Betancur, J.-F.; Navarro, E.P.; Bravo Bonilla, J.H.; Cortés, A.D.; Vélez, J.D.; Echeverry, A.; Suso, J.-P.; Cañas, C.A.; Tobón, G.J. Catastrophic Antiphospholipid Syndrome Triggered by Fulminant Chikungunya Infection in a Patient With Systemic Lupus Erythematosus. Arthritis Rheumatol. 2016, 68, 1044. [Google Scholar] [CrossRef] [Green Version]
- Farrell, D.F.; Lupone, C.D.; Kenneson, A.; Cueva, C.; Heydari, N.; Barzallo Aguilera, J.H.; Polhemus, M.; Endy, T.P.; Stewart-Ibarra, A.M. Case Report: An Acute Chikungunya Infection and a Recent Secondary Dengue Infection in a Peripartum Case in Ecuador. Am. J. Trop. Med. Hyg. 2018, 98, 838–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Agrawal, G.; Wazir, S.; Kumar, A.; Dubey, S.; Balde, M.; Yadav, B.S. Experience of Perinatal and Neonatal Chikungunya Virus (CHIKV) Infection in a Tertiary Care Neonatal Centre during Outbreak in North India in 2016: A Case Series. J. Trop. Pediatr. 2019, 65, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Jain, J.; Kumar, A.; Narang, M.; Zakaria, M.K.; Marcello, A.; Kumar, D.; Gaind, R.; Sunil, S. Chikungunya Outbreak in Delhi, India, 2016: Report on Coinfection Status and Comorbid Conditions in Patients. New Microbes New Infect. 2017, 20, 39–42. [Google Scholar] [CrossRef]
- Cavalcante, J.W. Aspectos clínicos, laboratoriais e histopatológicos dos óbitos por Chikungunya, necropsiados no Ceará, 2016–2017. 2019. Available online: http://www.repositorio.ufc.br/handle/riufc/43496 (accessed on 21 June 2021).
- Sá, P.K.d.O.; Nunes, M.d.M.; Leite, I.R.; Campelo, M.d.G.L.d.C.; Leão, C.F.R.; Souza, J.R.d.; Castellano, L.R.; Fernandes, A.I.V. Chikungunya Virus Infection with Severe Neurologic Manifestations: Report of Four Fatal Cases. Rev. Soc. Bras. Med. Trop. 2017, 50, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Farias, L.A.B.G.; Beserra, F.L.C.N.; Fernandes, L.; Teixeira, A.A.R.; Ferragut, J.M.; Girão, E.S.; Pires Neto, R.d.J. Myocarditis Following Recent Chikungunya and Dengue Virus Coinfection: A Case Report. Arq. Bras. Cardiol. 2019, 113, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo, J.; Alencar, G.; Nóbrega, M.; Mazzarollo, C.; Diniz, J.; Albuquerque, E.; Sena, A.; Silveira, C.; Osella, O. Echocardiographic Evaluation of Late Cardiac Issues Caused by the Chikungunya Fever. Arq. Bras. Cardiol. IMAGEM Cardiovasc. 2018, 31. [Google Scholar] [CrossRef]
- Oliveira, R.d.M.A.B.; Barreto, F.K.d.A.; Maia, A.M.P.C.; Gomes, I.P.; Simião, A.R.; Barbosa, R.B.; Rodrigues, A.S.R.; Lopes, K.W.; Araújo, F.M.d.C.; do Vale, R.L.S.; et al. Maternal and Infant Death after Probable Vertical Transmission of Chikungunya Virus in Brazil–Case Report. BMC Infect. Dis. 2018, 18. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.M.; Been Sayed, S.J.; Moniruzzaman, M.; Kabir, A.K.M.H.; Mallik, M.U.; Hasan, M.R.; Siddique, A.B.; Hossain, M.A.; Uddin, N.; Hassan, M.M.; et al. Clinical and Laboratory Characteristics of an Acute Chikungunya Outbreak in Bangladesh in 2017. Am. J. Trop. Med. Hyg. 2019, 100, 405–410. [Google Scholar] [CrossRef]
- Colavita, F.; Vita, S.; Lalle, E.; Carletti, F.; Bordi, L.; Vincenti, D.; Pozzetto, I.; Aiuti, M.; Vairo, F.; Capobianchi, M.R.; et al. Overproduction of IL-6 and Type-I IFN in a Lethal Case of Chikungunya Virus Infection in an Elderly Man During the 2017 Italian Outbreak. Open Forum Infect. Dis. 2018, 5. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.K.; Kumar, M.; Bhandari, N.; Kushwaha, A. Severe Sepsis and Septic Shock Associated with Chikungunya Fever in an Adolescent. J. Trop. Pediatr. 2018, 64, 557–559. [Google Scholar] [CrossRef]
- Agarwal, A.; Gupta, S.; Yadav, A.K.; Nema, R.K.; Ansari, K.; Biswas, D. Molecular and Phylogenetic Analysis of Chikungunya Virus in Central India during 2016 and 2017 Outbreaks Reveal High Similarity with Recent New Delhi and Bangladesh Strains. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2019, 75, 103940. [Google Scholar] [CrossRef] [PubMed]
- Cardona-Ospina, J.A.; Jiménez-Canizales, C.E.; Vásquez-Serna, H.; Garzón-Ramírez, J.A.; Alarcón-Robayo, J.F.; Cerón-Pineda, J.A.; Rodríguez-Morales, A.J. Fatal Dengue, Chikungunya and Leptospirosis: The Importance of Assessing Co-Infections in Febrile Patients in Tropical Areas. Trop. Med. Infect. Dis. 2018, 3, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Athayde, C.C.d.; Nishijuka, F.A.; Queiroz, M.C.d.C.; Luna, M.M.; Figueiredo, J.L.; Albuquerque, N.M.d.; Castilho, S.C.R.d.; Castro, R.R.T. Acute Decompensated Heart Failure Due to Chikungunya Fever. Arq. Bras. Cardiol. 2020, 114, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo, J.M.; Albuquerque, E.S.; Mazzarollo, C.; Oliveira, K.B.; Araujo, D.C.L.; Sena, A.D.M.; Alencar, M.P.C.; Brindeiro-Filho, D.F.; Silveira, C.A.M. P804 Heart Complication of Chikungunya Fever: Ecocardiographic Evaluation of Late Effects. Eur. Heart J. Cardiovasc. Imaging 2020, 21. [Google Scholar] [CrossRef]
- Lee, V.J.; Chow, A.; Zheng, X.; Carrasco, L.R.; Cook, A.R.; Lye, D.C.; Ng, L.-C.; Leo, Y.-S. Simple Clinical and Laboratory Predictors of Chikungunya versus Dengue Infections in Adults. PLoS Negl. Trop. Dis. 2012, 6, e1786. [Google Scholar] [CrossRef]
- Chandorkar, N.; Raj, D.; Kumar, R.; Warsi, S. Fever, Marked Tachycardia and Vesiculobullous Rash in an Infant with Chikungunya Fever. BMJ Case Rep. 2017, 2017. [Google Scholar] [CrossRef]
- Lenglet, Y.; Barau, G.; Robillard, P.-Y.; Randrianaivo, H.; Michault, A.; Bouveret, A.; Gérardin, P.; Boumahni, B.; Touret, Y.; Kauffmann, E.; et al. Infection à Chikungunya chez la femme enceinte et risque de transmission materno-fœtale: Étude dans un contexte d’épidémie en 2005-2006 à l’île de la Réunion. J. Gynécologie Obstétrique Biol. Reprod. 2006, 35, 578–583. [Google Scholar] [CrossRef]
- da Silva Junior, G.B.; Pinto, J.R.; Mota, R.M.S.; Pires Neto, R.d.J.; Daher, E.D.F. Risk Factors for Death among Patients with Chikungunya Virus Infection during the Outbreak in Northeast Brazil, 2016-2017. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 221–226. [Google Scholar] [CrossRef]
- Noronha, L.d.F.M.; Queiroz, R.B.d. Heart Changes in Elderly Chikungunya: Integration Review/Cardiac Changes in Elderly People with Chikungunya: Integrative Review|Noronha|Research Magazine: Care Is Fundamental Online. Available online: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/8634 (accessed on 13 February 2021).
- Nazneen, S.; Saha, M.; Hossain, R.; Ahsan, A.; Fatema, K.; Ahmed, F.; Saha, D.; Sultana, R. Chikungunya Viral Infection Requiring Intensive Care–Experience in a Tertiary Care Hospital in Bangladesh. BIRDEM Med. J. 2017, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Simon, F.; Paule, P.; Oliver, M. Chikungunya Virus-Induced Myopericarditis: Toward an Increase of Dilated Cardiomyopathy in Countries with Epidemics? Am. J. Trop. Med. Hyg. 2008, 78, 212–213. [Google Scholar] [CrossRef] [Green Version]
- Selly, J.-B.; Boumahni, B.; Edmar, A.; Jamal Bey, K.; Randrianaivo, H.; Clerici, G.; Millat, G.; Caillet, D. Cardiac sinus node dysfunction due to a new mutation of the SCN5A gene. Arch. Pediatr. Organe Off. Soc. Francaise Pediatr. 2012, 19, 837–841. [Google Scholar] [CrossRef]
- Villamil-Gómez, W.E.; Ramirez-Vallejo, E.; Cardona-Ospina, J.A.; Silvera, L.A.; Rodríguez-Morales, A.J. Electrocardiographic Alterations in Patients with Chikungunya Fever from Sucre, Colombia: A 42-Case Series. Travel Med. Infect. Dis. 2016, 14, 510–512. [Google Scholar] [CrossRef]
- Perti, T.; Lucero-Obusan, C.A.; Schirmer, P.L.; Winters, M.A.; Holodniy, M. Chikungunya Fever Cases Identified in the Veterans Health Administration System, 2014. PLoS Negl. Trop. Dis. 2016, 10. [Google Scholar] [CrossRef]
- Mavalankar, D.; Shastri, P.; Bandyopadhyay, T.; Parmar, J.; Ramani, K.V. Increased Mortality Rate Associated with Chikungunya Epidemic, Ahmedabad, India. Emerg. Infect. Dis. 2008, 14, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.R.R.; Cavalcanti, L.; Zuben, A.P.V.; Donalisio, M.R. Excess Mortality Related to Chikungunya Epidemics in the Context of Co-Circulation of Other Arboviruses in Brazil. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5731794/ (accessed on 31 January 2021).
- Powers, A.M.; Brault, A.C.; Tesh, R.B.; Weaver, S.C. Re-Emergence of Chikungunya and O’nyong-Nyong Viruses: Evidence for Distinct Geographical Lineages and Distant Evolutionary Relationships. J. Gen. Virol. 2000, 81, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Sam, I.-C.; Loong, S.-K.; Michael, J.C.; Chua, C.-L.; Wan Sulaiman, W.Y.; Vythilingam, I.; Chan, S.-Y.; Chiam, C.-W.; Yeong, Y.-S.; AbuBakar, S.; et al. Genotypic and Phenotypic Characterization of Chikungunya Virus of Different Genotypes from Malaysia. PLoS ONE 2012, 7, e50476. [Google Scholar] [CrossRef] [Green Version]
- Al Amin, M.; Ibrahim, S.; Balkhair, A.; Al Busaidi, I.; Gaifer, Z.; Taher, H.B. Chikungunya Masquerading as Acute Rheumatism in an Omani Traveler. Oman Med. J. 2019, 34, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Rahim, M.A.; Uddin, K.N. Chikungunya: An Emerging Viral Infection with Varied Clinical Presentations in Bangladesh: Reports of Seven Cases. BMC Res. Notes 2017, 10, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, D.E. Fundamentals of Electrocardiography Interpretation. Anesth. Prog. 2006, 53, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Tomoda, H.; Aoki, N. Right Bundle Branch Block in Acute Myocardial Infarction Treated by Primary Coronary Angioplasty and Stenting. Angiology 2005, 56, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Ashley, E.A.; Niebauer, J. Understanding the Echocardiogram. In Cardiology Explained; Remedica: Limassol, Cyprus, 2004. [Google Scholar]
- Couturier, E.; Guillemin, F.; Mura, M.; Léon, L.; Virion, J.-M.; Letort, M.-J.; De Valk, H.; Simon, F.; Vaillant, V. Impaired Quality of Life after Chikungunya Virus Infection: A 2-Year Follow-up Study. Rheumatol. Oxf. Engl. 2012, 51, 1315–1322. [Google Scholar] [CrossRef] [Green Version]
- Cerbino-Neto, J.; Mesquita, E.C.; Amancio, R.T.; Brasil, P.E.A.A.d. Events Preceding Death among Chikungunya Virus Infected Patients: A Systematic Review. Available online: https://www.scielo.br/scielo.php?pid=S0037-86822020000100201&script=sci_arttext (accessed on 31 January 2021).
- Mason, J.W. Myocarditis and Dilated Cardiomyopathy|Cardiovascular Research|Oxford Academic. Available online: https://academic.oup.com/cardiovascres/article/60/1/5/322628 (accessed on 30 January 2021).
- The Human Protein Atlas Tissue Expression of MXRA8-Primary Data-The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000162576-MXRA8/tissue/primary+data (accessed on 9 June 2021).
- Schnierle, B.S. Cellular Attachment and Entry Factors for Chikungunya Virus. Viruses 2019, 11, 1078. [Google Scholar] [CrossRef] [Green Version]
- Human Protein Atlas Tissue Expression of PHB-Primary Data-The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000167085-PHB/tissue/primary+data (accessed on 9 June 2021).
- Mallilankaraman, K.; Shedlock, D.J.; Bao, H.; Kawalekar, O.U.; Fagone, P.; Ramanathan, A.A.; Ferraro, B.; Stabenow, J.; Vijayachari, P.; Sundaram, S.G.; et al. A DNA Vaccine against Chikungunya Virus Is Protective in Mice and Induces Neutralizing Antibodies in Mice and Nonhuman Primates. PLoS Negl. Trop. Dis. 2011, 5. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.-L.; Dong, H.-L.; Zhang, Y.-N.; Xu, L.-L.; Deng, C.-L.; Li, X.-F.; Li, X.-D.; Ye, H.-Q.; Yuan, Z.-M.; Qin, C.-F.; et al. Visualization of Chikungunya Virus Infection in Vitro and in Vivo. Emerg. Microbes Infect. 2019, 8, 1574–1583. [Google Scholar] [CrossRef] [Green Version]
- Ngwe Tun, M.M.; Muthugala, R.; Kyaw Kyaw, A.; Shimada, S.; Morita, K.; Hayasaka, D. Pathogenetic Potential Relating to Metabolic Activity in a Mouse Model of Infection with the Chikungunya Virus East/Central/South African Genotype. Viruses 2020, 12, 169. [Google Scholar] [CrossRef] [Green Version]
- Cojan-Minzat, B.O.; Zlibut, A.; Agoston-Coldea, L. Non-Ischemic Dilated Cardiomyopathy and Cardiac Fibrosis. Heart Fail. Rev. 2020. [Google Scholar] [CrossRef]
- Schultheiss, H.-P.; Fairweather, D.; Caforio, A.L.P.; Escher, F.; Hershberger, R.E.; Lipshultz, S.E.; Liu, P.P.; Matsumori, A.; Mazzanti, A.; McMurray, J.; et al. Dilated Cardiomyopathy. Nat. Rev. Dis. Primer 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Al-Akchar, M.; Kiel, J. Acute Myocarditis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Wiyatno, A.; Febrianti, E.S.Z.; Dewantari, A.K.; Myint, K.S.; Safari, D.; Idris, N.S. Characterization of Rhinovirus C from a 4-Year-Old Boy with Acute Onset Dilated Cardiomyopathy in Jakarta, Indonesia. JMM Case Rep. 2018, 5, e005139. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez Carta Karina, A.; Mendoza Britto Ivan, J.; Alvirez-Gonzalez Enrique, J.; Morr, I.; Meza, Y.; Finizola, V.; Gomez, C.; Misticchio, F.; Martinez, N.; Allison, T. Abstract 14717: Zika Myocarditis, Risk Factors, Prior Arbovirus Infection Brings Out the Worst. Circulation 2017, 136, A14717. [Google Scholar] [CrossRef]
- Aletti, M.; Lecoules, S.; Kanczuga, V.; Soler, C.; Maquart, M.; Simon, F.; Leparc-Goffart, I. Transient Myocarditis Associated With Acute Zika Virus Infection. Clin. Infect. Dis. 2017, 64, 678–679. [Google Scholar] [CrossRef] [PubMed]
- Blauwet, L.A.; Cooper, L.T. Myocarditis. Prog. Cardiovasc. Dis. 2010, 52, 274–288. [Google Scholar] [CrossRef] [Green Version]
- English, R.F.; Janosky, J.E.; Ettedgui, J.A.; Webber, S.A. Outcomes for Children with Acute Myocarditis. Cardiol. Young 2004, 14, 488–493. [Google Scholar] [CrossRef]
- Roy, C.J.; Adams, A.P.; Wang, E.; Plante, K.; Gorchakov, R.; Seymour, R.L.; Vinet-Oliphant, H.; Weaver, S.C. Chikungunya Vaccine Candidate Is Highly Attenuated and Protects Nonhuman Primates against Telemetrically Monitored Disease Following a Single Dose. J. Infect. Dis. 2014, 209, 1891–1899. [Google Scholar] [CrossRef] [PubMed]
- Hunjul, G.N.E.; Balla, S.A. Knowledge of Chikungunya Disease among Academic Population in Private Universities, Khartoum State, Sudan-2019. Int. J. Trop. Dis. Health 2020, 41, 1–8. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Location | Year | Lineage |
|---|---|---|
| Sri Lanka [24,25] | 1972 | Asian [28] |
| India [26] | 1978 | Asian [28] |
| Reunion Island [29,30,31,32,33,34] | 2005 | IOL [35] |
| Kerala, India [36] | 2007 | IOL [36] |
| Malaysia [37] | 2008 | ECSA [37] |
| Aaryad, Kerala, India [38] | 2009 | IOL [39,40] |
| Malaysia [41] | 2010 | ECSA [41] |
| India [42] | 2011 | ECSA [39] |
| Guadeloupe and Martinique [43] | 2013–2014 | Asian [27] |
| Caribbean [44] | 2013–2014 | Asian [27] |
| Jamaica [45] | 2014 | Asian [27] |
| Venezuela [46,47,48,49] | 2014 | Asian [49] |
| Barbados [50] | 2014 | Asian [50] |
| French West Indies [51] | 2014 | Asian [51] |
| Tahiti, French Polynesia [52] | 2014 | Asian [52] |
| Puerto Rico [53,54,55] | 2014 | Asian [56] |
| San Salvador/El Salvador [57] | 2014 | Asian [57] |
| Willemstad, Curacao [58] | 2014 | Asian [59] |
| French Guiana [14] | 2014–2015 | Asian [11] |
| Sucre, Colombia [60] | 2014–2015 | Asian [11] |
| Columbia [61] | 2015 | Asian [11] |
| Machala, Ecuador [62] | 2015 | Asian [62] |
| North India [63] | 2016 | Asian or ECSA [64] |
| Paraiba, Brazil [65] | 2016 | Asian or ECSA [12] |
| Ceara, Brazil [66] | 2016–2017 | Asian or ECSA [12] |
| Brazil [21,67,68,69] | 2017 | Asian or ECSA [12] |
| Dhaka, Bangladesh [70] | 2017 | IOL [70] |
| Italy [71] | 2017 | IOL [71] |
| India [72] | 2017 | ECSA [73] |
| Columbia [74] | 2018 | Asian [11] |
| Brazil [75] | 2018 | Asian or ECSA [12] |
| Patient | Sex/Age | Pre-Existing Conditions | Symptoms | Lineage |
|---|---|---|---|---|
| 1 | F/44 | Tachycardia, ventricular abnormalities, gallop rhythm, cardiomegaly, abnormal electrocardiogram, later developed congestive cardiomyopathy [24] | Asian | |
| 2 | M/46 | Fever three months prior | Atrial fibrillation and cardiomegaly [24] | Asian |
| 3 | F/21 | Myopericarditis, pericardial effusion, abnormal echocardiogram, abnormal electrocardiogram [83] | IOL | |
| 4 | M/5.5 | Myocarditis, abnormal electrocardiogram, abnormal echocardiogram, congestive cardiac failure [38] | IOL | |
| 5 | M/71 | Hypertension, alcoholic cardiomyopathy | Acute decompensated heart failure [75] | ECSA or Asian |
| 6 | M/28 | Tachycardia, hypotension, abnormal electrocardiogram, abnormal echocardiogram, pericardial effusion, altered LV ejection fraction, LV hypercontractility, myocarditis, DENV coinfection [67] | ECSA or Asian | |
| 7 | M/77 | Hypertension, ischemic heart disease, CABG | Acute cardiac arrest, death, abnormal electrocardiogram, abnormal echocardiogram, dilated left cardiomyopathy [71] | IOL |
| 8 | M/0 | Tachycardia, bradycardia, pulmonary hemorrhage, death [69] | ECSA or Asian | |
| 9 | NR | Fetal heart rhythm abnormalities, fetal distress, intracerebral hemorrhage, death [58] | Asian | |
| 10 | NR | Fetal heart rate abnormalities, fetal distress, skin rash went away [58] | Asian | |
| 11 | M/12 | Hypotensive shock, hemodynamic instability, abnormal echocardiogram, LV hypokinesia, LV dysfunction, hypotension, myocarditis [72] | ECSA | |
| 12 | M/5 | Cardiorespiratory arrest, death [66] | ECSA or Asian | |
| 13 | F/51 | Respiratory difficulties, cardiorespiratory arrest, death [66] | ECSA or Asian | |
| 14 | F/0.25 | Tachycardia, abnormal electrocardiogram [78] | ECSA or Asian | |
| 15 | F/0 | Fetal pericardial effusion, cardiomegaly [42] | ECSA or Asian | |
| 16 | M/75 | Tachycardia, multi-organ failure, hemodynamic instability, atrial fibrillation, cardiorespiratory arrest, death [49] | Asian | |
| 17 | M/65 | Hypertension | Tachycardia, hypotensive, cardiac arrest, death [49] | Asian |
| 18 | F/32 | Hypotension, tachycardia, hemodynamic instability, abnormal echocardiogram [49] | Asian | |
| 19 | F/10 | SCN5A mutation, bradycardia | Bradycardia, cardiac sinus node dysfunction, needed pacemaker [84] | IOL |
| 20 | F/66 | Tachycardia, became hypertensive, cardiac decompensation, cardiac arrhythmia, death [41] | ECSA | |
| 21 | F/0 | Bradycardia, hypotensive, possible septic shock, death [45] | Asian | |
| 22 | M/87 | DENV, leptospirosis, chronic heart failure | Cardiac deterioration, death [74] | Asian |
| 23 | F/53 | Hypertension, cardiac failure | Cardiomegaly, abnormal echocardiogram, death [37] | ECSA |
| Total Patients | # Male | # Female | Age Range | Pre-Existing Conditions | Symptoms | Lineage |
|---|---|---|---|---|---|---|
| 42 | 20 | 22 | Median 60, 17 over 65, 16 under 40 | All patients showed palpitations, abnormal electrocardiogram in 71.4%, myocarditis suspected in 100% [85] | Asian | |
| 16 | 14 | 2 | Median 9.5 days, up to 3 months | Cardiovascular involvement including high pulmonary pressures in 4, myocarditis in 1, one death due to multi-organ failure [50] | Asian | |
| 399 confirmed, 291 probables | 395 | 295 | Median 38 years, range 21–96 | 8.9% with hypertension, 1.5% with ischemic heart disease | Hypotension in 5, mortality rate of 0.5% [70] | IOL |
| 21 | 10 | 11 | Median 3 months | At least 1 with myocarditis [54] | Asian | |
| 64 | 37 | 27 | Median 62, range 49–71 | Hypertension in 37, chronic heart failure in 12 | 2 had myocarditis, evidence of exacerbation of preexisting conditions, both myocarditis patients died (they did not have preexisting conditions, 11 and 56/F) [52] | Asian |
| 203 suspected, 69 confirmed | Children less than 15 years | DENV coinfection, myocarditis, and bradycardia in one [50] | Asian | |||
| 287 | 117 | 170 | 59 +/− 8 | 91 had palpitations, 45% had arrythmia (33% bradyarrhythmia), 19 cases of tachyarrhythmia, tachycardia, 3 cases of sudden death. Possible myocarditis [48] | Asian | |
| 180 | 167 | 13 | 68.8 +/− 16.2, 54.8 +/− 16.5 | Hypertension in 118, coronary heart disease in 32, congestive heart failure in 13 | 4 patients experienced exacerbation of congestive heart failure [86] | Asian |
| 257 | 133 | 124 | 63 +/− 9 | Hypertension in 63 | Arterial hypotension in 25, 51% had arrhythmias, 33% had bradyarrhythmia’s [47] | Asian |
| 43 | 18 | 25 | mean 62.5, range 24–88 | 84% had comorbidities | Chronic cardiac failure in 7, cardiac arrest in 4, related to comorbidities, 49% mortality rate, exacerbation of previous conditions [29] | IOL |
| 209 | 65 | 144 | 99 aged 20–40, 77 aged 40–60, 17 aged 60–80, 13 aged 10–20, 3 aged 80+ | Myocarditis in 1 [36] | IOL | |
| 610 | 271 | 339 | median 70, range 15–95 | 546 with comorbidity | 226 with cardiac abnormality, 110 of these had underlying cardiac condition, 137 had hypertension; 84 cases had heart failure, 29 of which had underlying cardiomyopathy, 10 with coronary artery disease, 6 with valvular disease, 4 with history of myocardial infarction, and 1 with arrhythmias; 35 cases of myocarditis, 4 cases of acute myocardial infarction [31] | IOL |
| 33 | adults | 18% had exacerbations of previous conditions | 1 with myocarditis [30] | IOL | ||
| 38 | neonates (average symptoms day 4) | Abnormal echocardiograms in 16, showing hypertrophy in 5, ventricular dysfunction in 2, pericarditis in 2, coronary artery dilation in 6 [32] | IOL | |||
| 86 | 50 | 36 | median 3.5, range 3 weeks–17 years | 7 total with cardiac symptoms, 2 with heart rhythm disturbances [33] | IOL | |
| 9 | children | 5 with cardiac complications including myocarditis and hemodynamic disorders [34] | IOL | |||
| 23 | 19 | 4 | 1 aged 31–40, 1 aged 41–50, 4 aged 51–60, 5 aged 61–70, 9 aged 71–80, 3 aged 81–90 | 3 patients with cardiac involvement, cardiogenic shock causing death in 1 [82] | IOL |
| Feature | N (%) | Correlation Coefficient | p Value |
|---|---|---|---|
| Male | 11 (48%) | 0.1455 | 0.5293 |
| Female | 10 (43%) | −0.1455 | 0.5293 |
| Preexisting Condition | 7 (30%) | 0.1234 | 0.5749 |
| A226V mutation | 4 (17%) | −0.2097 | 0.3370 |
| Asian Lineage | 7 (41%) | 0.5494 | 0.0224 |
| Tachycardia | 9 (39%) | −0.0542 | 0.8057 |
| Arrythmia | 12 (52%) | 0.0454 | 0.8368 |
| Palpitations | 0 | NA | NA |
| Hypertension | 4 (17%) | 0.2496 | 0.2507 |
| Hypotension | 5 (22%) | −0.0825 | 0.7080 |
| Myocarditis | 4 (17%) | −0.4393 | 0.0360 |
| Cardiomegaly | 4 (17%) | −0.2097 | 0.3370 |
| Heart Failure | 11 (48%) | 0.4773 | 0.0213 |
| Abnormal electrocardiogram | 6 (100%) | 0 | 1 |
| Abnormal echocardiogram | 7 (100%) | 0 | 1 |
| Death | 11 (48%) | NA | NA |
| Feature | N (%) | Correlation Coefficient | p Value |
|---|---|---|---|
| Male | 1316 (52%) | 0.3522 | 0.2379 |
| Female | 1212 (48%) | 0.5303 | 0.0623 |
| Preexisting Condition | 935 (32%) | 0.8893 | 0.0001 |
| A226V mutation | 9 (53%) | 0.2932 | 0.2534 |
| Asian | 8 (47%) | −0.2932 | 0.2534 |
| IOL | 9 (53%) | 0.2932 | 0.2534 |
| Tachycardia | 9 (1%) | −0.09995 | 0.7027 |
| Arrythmia | 292 (10%) | 0.07249 | 0.7822 |
| Palpitations | 133 (5%) | −0.1372 | 0.5994 |
| Hypertension | 636 (22%) | 0.8288 | 0.0001 |
| Hypotension | 37 (1%) | −0.1675 | 0.5204 |
| Myocarditis | 98 (3%) | 0.4798 | 0.0513 |
| Cardiomegaly | 0 | NA | NA |
| Heart Failure | 116 (4%) | 0.9417 | 0.0001 |
| Abnormal electrocardiogram | 35 (95%) | −0.6378 | 0.2470 |
| Abnormal echocardiogram | 18 (82%) | −0.2487 | 0.6347 |
| Death | 142 (5%) | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Traverse, E.M.; Hopkins, H.K.; Vaidhyanathan, V.; Barr, K.L. Cardiomyopathy and Death Following Chikungunya Infection: An Increasingly Common Outcome. Trop. Med. Infect. Dis. 2021, 6, 108. https://doi.org/10.3390/tropicalmed6030108
Traverse EM, Hopkins HK, Vaidhyanathan V, Barr KL. Cardiomyopathy and Death Following Chikungunya Infection: An Increasingly Common Outcome. Tropical Medicine and Infectious Disease. 2021; 6(3):108. https://doi.org/10.3390/tropicalmed6030108
Chicago/Turabian StyleTraverse, Elizabeth M., Hannah K. Hopkins, Vedana Vaidhyanathan, and Kelli L. Barr. 2021. "Cardiomyopathy and Death Following Chikungunya Infection: An Increasingly Common Outcome" Tropical Medicine and Infectious Disease 6, no. 3: 108. https://doi.org/10.3390/tropicalmed6030108