
Neonatal Sepsis, Antibiotic Susceptibility Pattern, and Treatment Outcomes among Neonates Treated in Two Tertiary Care Hospitals of Yangon, Myanmar from 2017 to 2019

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. Health Care Setting
2.2.3. Health Care Facility and Neonatal Care in Myanmar
2.2.4. Specific Setting
Yangon Children Hospital
Central Women Hospital
2.2.5. Laboratory Services
2.2.6. Neonatal Sepsis Treatment
2.3. Operational Definitions
2.4. Study Population and Period
2.5. Laboratory Procedures
2.6. Data Variables and Collection
2.7. Analysis and Statistics
2.8. Ethics Approval
3. Results
3.1. Characteristics of Study Participants
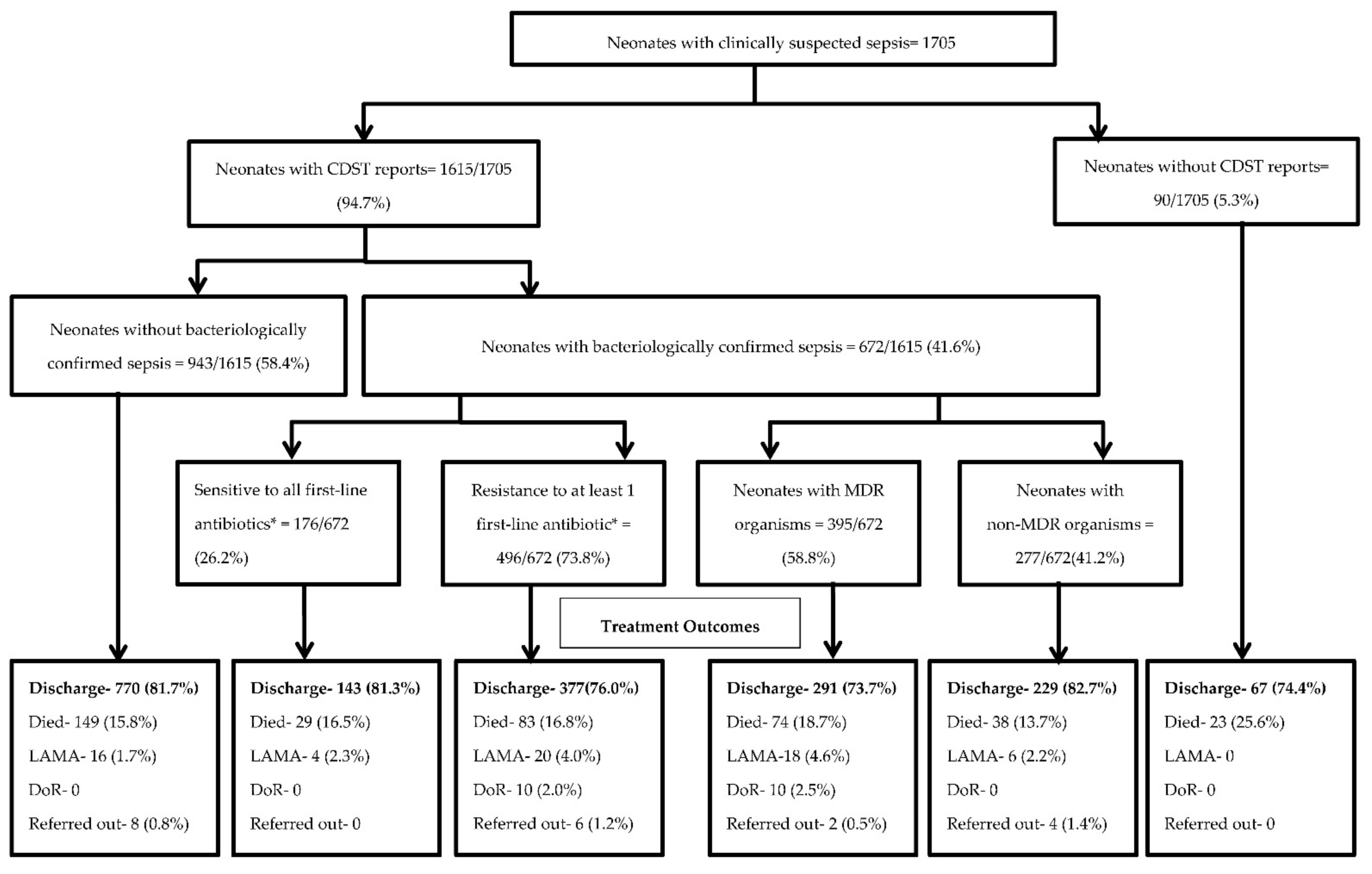
3.2. Culture and Drug Susceptibility Testing (CDST) Uptake, Bacteriological Confirmation, Resistance to First-Line Antibiotics, and Outcomes among Neonates with Clinically Suspected Sepsis
3.3. Associated Risk Factors Related to Neonatal Septicaemia with Positive Culture
3.4. Turn-Around Time of CDST among Neonates with Clinically Suspected Sepsis
3.5. Magnitude and Bacterial Profiles and Antibiotic Susceptibility Pattern among Neonatal Septicaemia
3.6. Associated Risk Factors Related to Neonates with Resistance to First Line Antibiotics
3.7. Multidrug-Resistance Pattern of Bacterial Isolates from Neonatal Septicemia
3.8. Associated Risk Factors Related to Neonates with Unfavourable Treatment Outcomes among Neonates with Bacteriologically Confirmed Sepsis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Open Access Statement
References
- Wang, H.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Abraha, H.N.; Abu-Raddad, L.J.; Abu-Rmeileh, N.M.E.; et al. Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1084–1150. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann-Struzek, C.; Goldfarb, D.M.; Schlattmann, P.; Schlapbach, L.J.; Reinhart, K.; Kissoon, N. The global burden of paediatric and neonatal sepsis: A systematic review. Lancet Respir. Med. 2018, 6, 223–230. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2000, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Pek, J.H.; Gan, M.Y.; Yap, B.J.; Seethor, S.T.T.; Greenberg, R.G.; Hornik, C.P.V.; Tan, B.; Lee, J.H.; Chong, S.L. Contemporary trends in global mortality of sepsis among young infants less than 90 days old: Protocol for a systematic review and meta-analysis. BMJ Open 2020, 10, 1–5. [Google Scholar] [CrossRef]
- Ministry of Health and Sports (MoHS) and ICF. Demographic and Health Survey 2015–16. Myanmar Demographic Household Survey 2015–16; Ministry of Health and Sports (MoHS) and ICF: Nay Pyi Taw, Myanmar, 2017; pp. 167–172. Available online: https://dhsprogram.com/pubs/pdf/FR324/FR324.pdf (accessed on 18 June 2019).
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Zea-Vera, A.; Ochoa, T.J. Challenges in the diagnosis and management of neonatal sepsis. J. Trop. Pediatrics 2015, 61, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jatsho, J.; Nishizawa, Y.; Pelzom, D.; Sharma, R. Clinical and Bacteriological Profile of Neonatal Sepsis: A Prospective Hospital-Based Study. Int. J. Pediatrics 2020, 2020, 1835945. [Google Scholar] [CrossRef]
- Klingenberg, C.; Kornelisse, R.F.; Buonocore, G.; Maier, R.F. Culture-Negative Early-Onset Neonatal Sepsis—At the Crossroad between Efficient Sepsis Care and Antimicrobial Stewardship. Front. Pediatrics 2018, 6, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaidi, A.K.M.; Huskins, W.C.; Thaver, D.; Bhutta, Z.A.; Abbas, Z.; Goldmann, D.A. Hospital-acquired neonatal infections in developing countries. Lancet 2005, 365, 1175–1188. [Google Scholar] [CrossRef]
- Swarnkar, K.; Swarnkar, M. A Study of Early Onset Neonatal Sepsis with Special Care Centre of Rural India. Internet J. Infect. Dis. 2012, 10, 1–8. [Google Scholar]
- Sankar, M.J. Neonatal sepsis in South Asia: Huge burden and spiralling antimicrobial resistance. BMJ 2019, 1. [Google Scholar] [CrossRef] [Green Version]
- Than, K.M. A Study of Common Causal Organisms in Neonatal Sepsis and Their Drug Sensitivity in Special Care Baby Unit of Mandalay Children’s Hospital and Central Women Hospital. Master’s Thesis, University of Medicine, Mandalay, Myanmar, 2003. [Google Scholar]
- Than, M.M. A Study of Neonatal Sepsis in Special Care Baby Unit of Magway Regional Hospital. Master’s Thesis, University of Medicine, Magway, Myanmar, 2013. [Google Scholar]
- Thazin, M.; Kay, T.H.; Kyaw, O.O.; Aung, W.W.; Zaw, K.K. Predictors for Diagnosis of Neonatal Sepsis in Yangon Children Hospital. In Proceedings of the 42nd Myanmar Health Research Congress, Yangon, Myanmar, 6–10 January 2013; p. 62. [Google Scholar]
- Kyaw, A.T. Prediction Scoring for Early Diagnosis of late Onset Neonatal Sepsis in Yangon Central Women Hospital. Ph.D. Thesis, University of Medicine 1, Yangon, Myanmar, 2020. [Google Scholar]
- Thi, K.S.; Moe, Z.W.; Thein, K.N. Early Onset Sepsis in Extramural Hospital of Myanmar (Burma). Arch. Dis. Child 2019, 104, A129. [Google Scholar]
- Latt, N.N.; Cho, S.M.; Mie, N.; Htun, M.; Saw, Y.M.; Htin, M.N.; Myint, A.; Aoki, F.; Reyer, J.A.; Yamamoto, E.; et al. Healthcare in Myanmar. Nagoya J. Med. Sci. 2016, 78, 123–134. [Google Scholar] [PubMed]
- Department of Public Health Ministry of Health and Sports. The Republic of the Union of Myanmar Hospital Statistics Report; Ministry of Health and Sports: Nay Pyi Taw, Myanmar, 2016; pp. 114–118. [Google Scholar]
- Improving Maternal, Neonatal and Child Health in Myanmar—Optimising the Role of the AMW Cadre Lessons to Support a National Scale Up. 2014. Available online: https://themimu.info/sites/themimu.info/files/assessment_file_attachments/improving_maternal_neonatal_and_child_health_in_myanmar_2013.pdf (accessed on 17 June 2019).
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, 31st ed.; CLSI supplements M100; Clinical and Laboratory Standards Institute: Pittsburgh, PA, USA, 2021; ISBN 9781684401048. [Google Scholar]
- Tette, E.M.A.; Nartey, E.T.; Nuertey, B.D.; Azusong, E.A.; Akaateba, D.; Yirifere, J.; Alandu, A.; Seneadza, N.A.H.; Gandau, N.B.; Renner, L.A. The pattern of neonatal admissions and mortality at a regional and district hospital in the Upper West Region of Ghana; a cross sectional study. PLoS ONE 2020, 15, 1–17. [Google Scholar] [CrossRef]
- Masanja, P.P.; Kibusi, S.M.; Mkhoi, M.L. Predictors of Early Onset Neonatal Sepsis among Neonates in Dodoma, Tanzania: A Case Control Study. Journal of tropical pediatrics 2020, 66, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Mitra, D.K.; Mullany, L.C.; Harrison, M.; Mannan, I.; Shah, R.; Begum, N. Incidence and risk factors of neonatal infections in a rural Bangladeshi population: A community-based prospective study. J. Health Popul. Nutr. 2018, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, N.S.; Sharma, S.; Chaudhary, D.K.; Panthi, P.; Pokhrel, P.; Shrestha, A.; Mandal, P.K. Bacteriological profile of neonatal sepsis and antibiotic susceptibility pattern of isolates admitted at Kanti Children’s Hospital, Kathmandu, Nepal. BMC Res. Notes 2018, 11, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Chaurasia, S.; Jeeva Sankar, M.; Yadav, C.P.; Arya, S.; Kapil, A.; Gaind, R.; Vishnubhatla, S.; Chellani, H.; Ramji, S.; et al. Characterisation and antimicrobial resistance of sepsis pathogens in neonates born in tertiary care centres in Delhi, India: A cohort study. Lancet Glob. Health 2016, 4, e752–e760. [Google Scholar] [CrossRef] [Green Version]
- Yusef, D.; Shalakhti, T.; Awad, S.; Algharaibeh, H.; Khasawneh, W. Clinical characteristics and epidemiology of sepsis in the neonatal intensive care unit in the era of multi-drug resistant organisms: A retrospective review. Pediatrics Neonatol. 2018, 59, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Amare, D.; Mela, M.; Dessie, G. Unfinished agenda of the neonates in developing countries: Magnitude of neonatal sepsis: Systematic review and meta-analysis. Heliyon 2019, 5, e02519. [Google Scholar] [CrossRef] [Green Version]
- Al-shamahy, H.A.; Sabrah, A.A.; Al-robasi, A.B.; Naser, S.M. Types of Bacteria associated with Neonatal Sepsis in Al-Thawra University Hospital, Sana’a, Yemen, and their Antimicrobial Profile. Sultan Qaboos Univ. Med. J. 2012, 12, 48–54. [Google Scholar] [CrossRef]
- El-din, E.M.R.S.; El-sokkary, M.M.A.; Bassiouny, M.R.; Hassan, R. Epidemiology of Neonatal Sepsis and Implicated Pathogens: A Study from Egypt. BioMed Res. Int. 2015, 2015, 509484. [Google Scholar]
- Adatara, P.; Afaya, A.; Salia, S.M.; Afaya, R.A.; Konlan, K.D.; Agyabeng-Fandoh, E.; Agbinku, E.; Ayandayo, E.A.; Boahene, I.G. Risk Factors Associated with Neonatal Sepsis: A Case Study at a Specialist Hospital in Ghana. Sci. World J. 2019, 2019, 9369051. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.M.; Saleem, A.F.; Shaikh, A.S.; Munir, O.; Qadir, M. Neonatal sepsis following prolonged rupture of membranes in a tertiary care hospital in Karachi, Pakistan. J. Infect. Dev. Ctries. 2014, 8, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Kabwe, M.; Tembo, J.; Chilukutu, L.; Chilufya, M.; Ngulube, F.; Lukwesa, C.; Kapasa, M.; Enne, V.; Wexner, H.; Mwananyanda, L.; et al. Etiology, antibiotic resistance and risk factors for neonatal sepsis in a large referral center in Zambia. Pediatric Infect. Dis. J. 2016, 35, e191–e198. [Google Scholar] [CrossRef] [Green Version]
- Dalal, P.; Gathwala, G.; Gupta, M.; Singh, J. Bacteriological profile and antimicrobial sensitivity pattern in neonatal sepsis: A study from North India. Int. J. Res. Med Sci. 2017, 5, 1541. [Google Scholar] [CrossRef]
- Leblebicioglu, H.; Koksal, I.; Rosenthal, V.D.; Akan, Ö.A.; Özgültekin, A.; Kendirli, T.; Erben, N.; Alp, E.; Yıldızda, D.; Esen, S.; et al. Impact of the International Nosocomial Infection Control Consortium (INICC) Multidimensional Hand Hygiene Approach, over 8 years, in 11 cities of Turkey. Infect. Control Hosp. Epidemiol. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tumuhamye, J.; Sommerfelt, H.; Bwanga, F.; Ndeezi, G.; Mukunya, D.; Napyo, A.; Nankabirwa, V.; Tumwine, J.K. Neonatal sepsis at Mulago national referral hospital in Uganda: Etiology, antimicrobial resistance, associated factors and case fatality risk. PLoS ONE 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.H.; Chu, S.M.; Hsu, J.F.; Lien, R.; Huang, H.R.; Chiang, M.C.; Fu, R.H.; Lee, C.W.; Huang, Y.C. Risk factors and outcomes for multidrug-resistant Gram-negative bacteremia in the NICU. Pediatrics 2014, 133. [Google Scholar] [CrossRef] [Green Version]
- Islam, Q.R.; Shahidullah, M.; Islam, M.Z.; Mridha, M.A.A.; Akter, S. Bacterial Profile of Neonatal Septicemia and Antibiotic Susceptibility Pattern of the Isolates in Tertiary Care Hospital, Dhaka, Bangladesh. Bangladesh J. Child Health 2019, 43, 35–40. [Google Scholar] [CrossRef]
- Datta, S.; Roy, S.; Chatterjee, S.; Saha, A.; Sen, B.; Pal, T. A Five-Year Experience of Carbapenem Resistance in Enterobacteriaceae Causing Neonatal Septicaemia: Predominance of NDM-1. PLoS ONE 2014. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Neonatal Sepsis | Neonatal Sepsis Refers to Systemic and Generalized Bacterial Infection of the Newborn, Documented by a Positive Blood Culture in the First Four Weeks of Life. |
|---|---|
| Clinically suspected neonatal sepsis | Neonates with clinically suspected sepsis have a constellation of signs and symptoms that can include: fever, poor feeding, respiratory distress, cyanosis, tachycardia, seizures, hyperreflexia, jaundice, and temperature or blood pressure instability. All neonates in whom sepsis was suspected at CWH and YCH during the study period were included in the study. |
| Confirmed neonatal sepsis | Confirmed neonatal sepsis was identified as the presence of a clinically significant pathogen isolated from blood cultures with associated signs and symptoms. |
| Onset of sepsis | Neonatal sepsis can be categorized as early onset sepsis (EOS), with symptoms developing during the first 72 hours of life, or late onset sepsis (LOS) with symptoms starting after 72 hours of age. |
| Multidrug-resistant (MDR) organisms | Non-susceptibility to at least one agent in three or more antimicrobial categories was defined as multidrug-resistance (MDR) to groups such as penicillins, aminoglycosides, cephalosporins, fluoroquinolones, and carbapenems. |
| Characteristics | YCH | CWH | Total | p Value $ | |||
|---|---|---|---|---|---|---|---|
| n | (%) * | n | (%) * | n | (%) * | ||
| Total | 1023 | (100) | 682 | (100) | 1705 | (100) | |
| Admission age in days | |||||||
| ≤3 | 580 | (56.7) | 655 | (96.0) | 1235 | (72.4) | <0.001 |
| 4–7 | 164 | (16.0) | 19 | (2.8) | 183 | (10.7) | |
| 8–28 | 279 | (27.3) | 8 | (1.2) | 287 | (16.8) | |
| Gender | |||||||
| Male | 616 | (60.2) | 392 | (57.5) | 1008 | (59.1) | 0.260 |
| Female | 407 | (39.8) | 290 | (42.5) | 697 | (40.9) | |
| Year of admission | |||||||
| 2017 | 434 | (42.4) | 298 | (43.7) | 732 | (42.9) | 0.020 |
| 2018 | 303 | (29.6) | 232 | (34.0) | 535 | (31.4) | |
| 2019 | 286 | (28.0) | 152 | (22.3) | 438 | (25.7) | |
| Gestational age | |||||||
| Preterm (<37 wk ) | 353 | (34.5) | 470 | (68.9) | 823 | (48.3) | <0.001 |
| Term (37 up to 42 wk ) | 642 | (62.8) | 210 | (30.8) | 852 | (50.0) | |
| Post term (>42 wk ) | 9 | (0.9) | 2 | (0.3) | 11 | (0.6) | |
| Missing | 19 | (1.9) | 0 | (0.0) | 19 | (1.1) | |
| PROM (>18 h) | |||||||
| Yes | 273 | (26.7) | 168 | (24.6) | 441 | (25.9) | 0.343 |
| No | 750 | (73.3) | 514 | (75.4) | 1264 | (74.1) | |
| Place of Delivery | |||||||
| Institutional | 802 | (78.4) | 682 | (100.0) | 1484 | (87.0) | <0.001 |
| Home | 221 | (21.6) | 0 | (0.0) | 221 | (13.0) | |
| Mode of delivery | |||||||
| Normal | 576 | (56.3) | 285 | (41.8) | 861 | (50.5) | <0.001 |
| Forceps/Vacuum | 15 | (1.5) | 22 | (3.2) | 37 | (2.2) | |
| Elective Caesarean section | 54 | (5.3) | 19 | (2.8) | 73 | (4.3) | |
| Emergency Caesarean section | 378 | (37.0) | 356 | (52.2) | 734 | (43.0) | |
| Delivery conducted by | |||||||
| Doctor | 755 | (73.8) | 678 | (99.4) | 1433 | (84.0) | <0.001 |
| Others # | 268 | (26.2) | 4 | (0.6) | 272 | (16.0) | |
| Meconium staining liquor | |||||||
| Yes | 75 | (7.3) | 150 | (22.0) | 225 | (13.2) | <0.001 |
| No | 948 | (92.7) | 532 | (78.0) | 1480 | (86.8) | |
| Foul smelling liquor | |||||||
| Yes | 70 | (6.8) | 24 | (3.5) | 94 | (5.5) | 0.003 |
| No | 953 | (93.2) | 658 | (96.5) | 1611 | (94.5) | |
| Birth Asphyxia | |||||||
| Yes | 186 | (18.2) | 233 | (34.2) | 419 | (24.6) | <0.001 |
| No | 763 | (74.6) | 449 | (65.8) | 1212 | (71.1) | |
| Missing | 74 | (7.2) | 0 | (0.0) | 74 | (4.3) | |
| Birth weight | |||||||
| Very low (<1500 g) | 127 | (12.4) | 272 | (39.9) | 399 | (23.4) | <0.001 |
| Low (1500 g to 2500 g) | 294 | (28.7) | 235 | (34.5) | 529 | (31.0) | |
| Normal (>2500 g) | 602 | (58.8) | 175 | (25.7) | 777 | (45.6) | |
| Hyperbilirubinemia (>20 mg per dL) | |||||||
| Yes | 459 | (44.9) | 463 | (67.9) | 922 | (54.1) | <0.001 |
| No | 564 | (55.1) | 219 | (32.1) | 783 | (45.9) | |
| Hypothermia (Temperature < 35.5 °C) | |||||||
| Yes | 260 | (25.4) | 10 | (1.5) | 270 | (15.8) | <0.001 |
| No | 763 | (74.6) | 672 | (98.5) | 1435 | (84.2) | |
| Onset | |||||||
| Early | 503 | (49.2) | 333 | (48.8) | 836 | (49.0) | 0.889 |
| Late | 520 | (50.8) | 349 | (51.2) | 869 | (51.0) | |
| Time Variable | Count |
|---|---|
| Turn-Around Time (n = 1533) | Median Days (IQR) |
| Admission and CDST test | 2 (2–4) |
| CDST test and receipt of results | 6 (6–6) |
| Admission to CDST results | 7 (6–9) |
| Time to Reporting CDST Results (Days) | n (%) |
| ≤ 6 | 474 (29.3) |
| 7–14 | 968 (60.0) |
| ≥15 | 91 (5.6) |
| Missing | 82 (5.1) |
| Drugs | S. aureus | S. epidermidis | CoNS (Others) | Enterococcus spp. | Others * | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | |
| Total | 73 | 34 | 115 | 13 | 16 | 251 | ||||||
| Ampicillin | 37/43 | (86.0) | 21/23 | (91.3) | 43/49 | (87.8) | 4/10 | (40.0) | 4/14 | (28.6) | 109/139 | (78.4) |
| Cloxacillin | 12/20 | (60.0) | 18/22 | (81.8) | 35/47 | (74.5) | 0/1 | (0.0) | 1/1 | (100.0) | 66/101 | (65.3) |
| Amoxi-Clav | 11/27 | (40.7) | 24/29 | (82.8) | 47/62 | (75.8) | 4/6 | (66.7) | NT | NT | 86/134 | (64.2) |
| Gentamicin | 21/67 | (31.3) | 12/28 | (42.9) | 28/111 | (25.2) | 3/6 | (50.0) | 3/7 | (17.6) | 67/229 | (29.3) |
| Amikacin | 2/30 | (6.7) | 2/5 | (40.0) | 0/28 | (0.0) | 3/6 | (50.0) | 1/1 | (100.0) | 8/70 | (11.4) |
| Cefotaxime | 15/44 | (34.0) | 7/21 | (33.3) | 40/81 | (49.4) | 4/5 | (80.0) | 0/3 | NT | 66/154 | (42.9) |
| Ceftazidime | 3/12 | (25.0) | 19/24 | (79.2) | 14/21 | (66.7) | 2/2 | (100.0) | NT | NT | 38/59 | (64.4) |
| Cefoperazone# | 3/7 | (42.9) | 14/20 | (70.0) | 9/25 | (60.0) | 2/2 | (100.0) | 0/1 | (0.0) | 28/45 | (62.2) |
| Vancomycin | 4/27 | (14.8) | 2/23 | (8.7) | 13/64 | (20.3) | 0/7 | (0.0) | 0/11 | (0.0) | 19/132 | (14.4) |
| PT | 10/34 | (29.4) | 21/27 | (77.8) | 17/38 | 44.7) | 2/5 | (40.0) | NT | NT | 50/104 | (48.1) |
| Imipenem | 7/34 | (20.6) | 19/25 | (76.0) | 18/38 | (47.4) | 0/2 | (0.0) | 1/4 | (25.0) | 45/103 | (43.7) |
| Meropenem | 3/15 | (20.0) | 17/21 | (81.0) | 13/21 | (61.9) | 1/2 | (50.0) | 0/2 | (0.0) | 34/61 | (55.7) |
| Linezolid | 3/43 | (7.0) | 0/23 | (0.0) | 5/75 | (6.7) | 0/6 | (0.0) | 1/8 | (12.5) | 9/155 | (5.8) |
| Ciprofloxacin | 13/47 | (27.7) | 7/25 | (28.0) | 31/62 | (50.0) | 4/4 | (100.0) | 2/8 | (25.0) | 57/146 | (39.0) |
| Levofloxacin | 6/36 | (16.7) | 8/24 | (33.3) | 30/76 | (39.5) | 5/10 | (50.0) | 5/11 | (45.5) | 54/157 | (34.4) |
| Erythromycin | 15/25 | (60.0) | 12/21 | (57.1) | 30/49 | (61.2) | 4/7 | (57.1) | 2/8 | (25.0) | 63/110 | (57.3) |
| Co-trimoxazole | 7/21 | (33.3) | 7/17 | (41.2) | 16/41 | (39.0) | 4/15 | (80.0) | 0/4 | (0.0) | 34/88 | (38.6) |
| Drugs | K. pneumoniae | S. marcescens | B. cepacia | P. aeruginosa | Acinetobacter spp. | Enterobacter spp. | Others * | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | n/N | (%) | |
| Total | 90 | 66 | 33 | 33 | 40 | 36 | 123 | 421 | ||||||||
| Ampicillin | 59/63 | (93.7) | 30/30 | (100.0) | 20/20 | (100.0) | 5/5 | (100.0) | 19/19 | (100.0) | 24/24 | (100.0) | 60/67 | (89.6) | 217/228 | (95.2) |
| Cloxacillin | 0/1 | (0.0) | 1/2 | (50.0) | 0/1 | (0.0) | 0/5 | (0.0) | 0/1 | (0.0) | 0/1 | (0.0) | 0/2 | (0.0) | 1/2 | (50.0) |
| Amoxi-Clav | 27/45 | (60.0) | 49/50 | (98.0) | 10/12 | (83.3) | 5/15 | (33.0) | 9/12 | (75.0) | 21/24 | (87.5) | 31/61 | (50.8) | 152/219 | (69.4) |
| Gentamicin | 57/74 | (77.0) | 22/31 | (71.0) | 21/25 | (84.0) | 17/18 | (94.0) | 11/37 | (30.0) | 15/25 | (60.0) | 53/104 | (51.0) | 196/314 | (62.4) |
| Amikacin | 10/82 | (12.2) | 29/59 | (49.0) | 22/30 | (73.3) | 14/28 | (50.0) | 6/25 | (24.0) | 8/28 | (28.6) | 28/107 | (26.2) | 117/359 | (32.6) |
| Cefotaxime | 40/73 | (54.8) | 30/55 | (55.0) | 16/23 | (69.6) | 5/21 | (24.0) | 6/23 | (26.0) | 16/27 | (59.2) | 27/81 | (33.3) | 140/303 | (46.2) |
| Ceftazidime | 56/60 | (93.3) | 17/32 | (53.0) | 9/19 | (47.4) | 5/12 | (42.0) | 9/16 | (56.0) | 10/18 | (55.5) | 42/76 | (55.3) | 148/233 | (63.5) |
| Cefoperazone# | 13/60 | (21.7) | 7/11 | (64.0) | 2/15 | (13.3) | 1/2 | (50.0) | 4/8 | (50.0) | 2/6 | (33.3) | 5/13 | (38.5) | 34/115 | (29.6) |
| PT | 11/68 | (16.2) | 21/33 | (64.0) | 12/27 | (44.4) | 1/17 | (5.9) | 7/31 | (23.0) | 11/27 | (40.7) | 24/85 | (28.2) | 87/288 | (30.2) |
| Imipenem | 4/67 | (6.0) | 10/23 | (44.0) | 20/23 | (87.0) | 12/26 | (46.0) | 4/27 | (15.0) | 5/23 | (21.7) | 26/88 | (29.5) | 81/277 | (29.2) |
| Meropenem | 9/73 | (12.3) | 17/53 | (32.0) | 5/25 | (20.0) | 0/8 | (0.0) | 2/22 | (9.1) | 7/24 | (29.2) | 20/72 | (27.8) | 60/277 | (21.7) |
| Ciprofloxacin | 17/62 | (27.4) | 4/43 | (9.3) | 15/27 | (55.6) | 2/27 | (7.4) | 1/27 | (3.7) | 0/23 | (0.0) | 21/87 | (24.2) | 60/296 | (20.3) |
| Levofloxacin | 11/73 | (15.1) | 2/57 | (3.5) | 5/32 | (15.6) | 0/12 | (0.0) | 2/24 | (5.9) | 1/31 | (3.2) | 14/101 | (13.9) | 35/340 | (10.3) |
| Co-trimoxazole | 34/63 | (64.2) | 4/45 | (8.9) | 1/18 | (5.6) | 2/3 | (67.0) | 4/5 | (80.0) | 6/18 | (33.3) | 23/66 | (34.8) | 74/218 | (33.9) |
| Neonatal Bloodstream Pathogens | No. of Isolates | MDR Isolates (Number, %) | Non-MDR Isolates (Number, %) | CFR Due to MDR in Culture-Positive Isolates (n/N, %) | CFR Due to Non-MDR in Culture-Positive Isolates (n/N, %) |
|---|---|---|---|---|---|
| Gram-positive organisms | 251 | 123 (49.0) | 128 (51.0) | 19/28 (67.9) | 9/28 (32.1) |
| S. aureus | 73 | 30 (41.1) | 43 (59.0) | 6/10 (60.0) | 4/10 (40.0) |
| S. epidermidis | 34 | 24 (70.6) | 10 (29.4) | 2/2 (100) | 0/0 (0.0) |
| CoNS (others) | 115 | 62 (54.0) | 53 (46.1) | 10/14 (71.4) | 4/14 (28.6) |
| Enterococcus spp. | 13 | 6 (46.2) | 7 (53.8) | ||
| Streptococcus spp. | 8 | 0 | 8 (100) | ||
| Others Gram-positive organisms | 8 | 1 (12.5) | 7 (87.5) | 1/1 (100) | 0/7 (0.0) |
| Gram-negative organisms | 421 | 272 (64.6) | 149 (35.4) | 54/84 (64.3) | 30/84 (35.7) |
| Klebsiella pneumoniae | 90 | 72 (80.0) | 18 (20.0) | 16/20 (80.0) | 4/20 (20.0) |
| Serratia marcescens | 66 | 42 (63.7) | 24 (36.4) | 4/8 (50.0) | 4/8 (50.0) |
| Other Serratia spp. | 16 | 8 (50.0) | 8 (50.0) | 4/5 (80.0) | 1/5 (20.0) |
| Burkholderia cepacia | 33 | 26 (78.8) | 7 (21.2) | ||
| Pseudomonas aeruginosa | 33 | 16 (48.5) | 17 (51.5) | 5/9 (55.5) | 4/9 (44.5) |
| Acinetobacter baumannii | 29 | 13 (44.8) | 16 (55.2) | 5/7 (71.4) | 2/7 (28.6) |
| Enterobacter spp. | 36 | 26 (69.4) | 10 (30.5) | 5/9 (55.5) | 4/9 (44.5) |
| Citrobacter spp. | 16 | 13 (81.2) | 3 (18.8) | 5/5 (100) | 0/5 (0.0) |
| Other Gram-negative bacilli | 44 | 17 (40.9) | 27 (59.1) | 3/9 (33.3) | 6/9 (66.6) |
| E.coli | 29 | 24 (82.8) | 5 (17.2) | 7/8 (87.5) | 1/8 (12.5) |
| Other Acinobacter spp. | 11 | 4 (36.4) | 7 (63.6) | 0/3 (0.0) | 3/3 (100) |
| Other Klebsiella spp. | 18 | 11 (61.1) | 7 (38.9) | 0/1 (0.0) | 1/1 (100) |
| Total | 672 | 395 (58.8) | 277 (41.2) | 73/112 (65.2) | 39/112 (34.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oo, N.A.T.; Edwards, J.K.; Pyakurel, P.; Thekkur, P.; Maung, T.M.; Aye, N.S.S.; Nwe, H.M. Neonatal Sepsis, Antibiotic Susceptibility Pattern, and Treatment Outcomes among Neonates Treated in Two Tertiary Care Hospitals of Yangon, Myanmar from 2017 to 2019. Trop. Med. Infect. Dis. 2021, 6, 62. https://doi.org/10.3390/tropicalmed6020062
Oo NAT, Edwards JK, Pyakurel P, Thekkur P, Maung TM, Aye NSS, Nwe HM. Neonatal Sepsis, Antibiotic Susceptibility Pattern, and Treatment Outcomes among Neonates Treated in Two Tertiary Care Hospitals of Yangon, Myanmar from 2017 to 2019. Tropical Medicine and Infectious Disease. 2021; 6(2):62. https://doi.org/10.3390/tropicalmed6020062
Chicago/Turabian StyleOo, Nan Aye Thida, Jeffrey K. Edwards, Prajjwal Pyakurel, Pruthu Thekkur, Thae Maung Maung, Nant San San Aye, and Hla Myat Nwe. 2021. "Neonatal Sepsis, Antibiotic Susceptibility Pattern, and Treatment Outcomes among Neonates Treated in Two Tertiary Care Hospitals of Yangon, Myanmar from 2017 to 2019" Tropical Medicine and Infectious Disease 6, no. 2: 62. https://doi.org/10.3390/tropicalmed6020062