Innovative and Assistive eHealth Technologies for Smart Therapeutic and Rehabilitation Outdoor Spaces for the Elderly Demographic




Abstract
:1. Introduction
- Personalized homecare services, telemedicine and mobile health (mHealth): this include smart watches for daily activities monitoring, remote wearable patient monitoring devices, teleconsultations and eReferrals.
- Integrated health information systems: such as ePrescription, electronic health records (EHR) and eDispensing.
- Non-clinical systems: such as online support groups, online health information services and patient flow management systems.
- Clinical systems: these are mainly used by health professionals within or outside health care institutions such as computer-assisted diagnostics, medication management systems and pharmacy information systems.
- Assistive technologies: these are tools, equipment and devices used to help an individual in overall management of daily life and to compensate sensory, cognitive and physical impairments. Advanced equipment now includes environmental management devices, sensors, embedded systems and videophone network.
- Safety and social technologies: safety technologies are various security units networked with other assistance and surveillance services such as smart floors, bed occupancy sensors, safety bracelets and other integrated sensors interconnected to a remote center for processing. A typical example of a social technology is the health TV which provides speech and visual links through a broadband connection. Big data handling, false alarms and privacy issues are concerns in adopting safety and social technologies.
- Health technologies: these are self-monitoring and self-care systems such as blood pressure monitors, eHealth portals and other internet-based services with remote connection with health professionals.
- Self-activation and personal development technologies: these can be referred to as sport technologies designed to support, analyze and monitor individuals’ development and performance. Examples are pedometers, accelerometers, smart sport watches and activity bracelets. Another recent development under this application is gamification, where motivation is provided for repetitive rehabilitation or exercise.
- Design-for-all and ambient assisted living (AAL) technologies: the design-for-all concept provides equal opportunities for everyone irrespective of age, gender, ability to function and cultural orientation. A typical example is the sliding door which shows all the design-for-all criteria such as sustainability and affordability. However, this type of eHealth technology application might not always be suitable for all and cost-effective; for example, prosthesis usage requires customization. AAL technologies provides elder care to promote well-being and independence. Examples include robots, medication optimization equipment and wearable technologies.
- Gerontechnology: This is a general term and includes technology from all the previously mentioned categories. Its overall aim is to develop age-friendly technologies in order to promote independence, well-being and prevent age-related health problems.
- Hospital technology and EHR systems: these are patient systems used to integrate data from wearables, smart home-type technologies, electronic patients and health records for monitoring health progress of patients. They provide useful health information such as physical assessment, referral and daily charting used in health and social care.
2. Materials and Methods
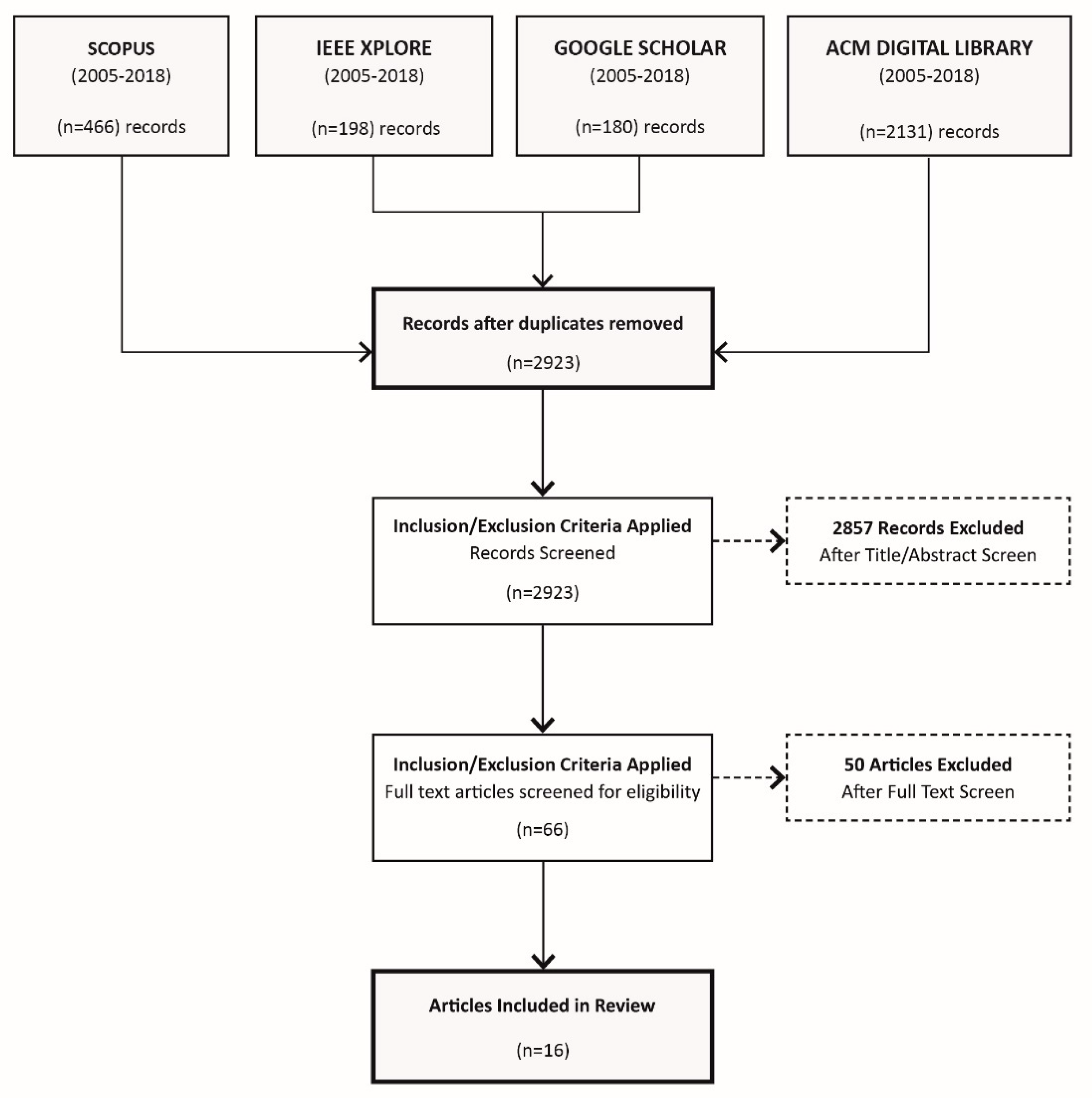
2.1. Data Sources, Search Strategy and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
3. Results
3.1. Assistive eHealth Technologies and Interfaces for Outdoor Interactive Spaces
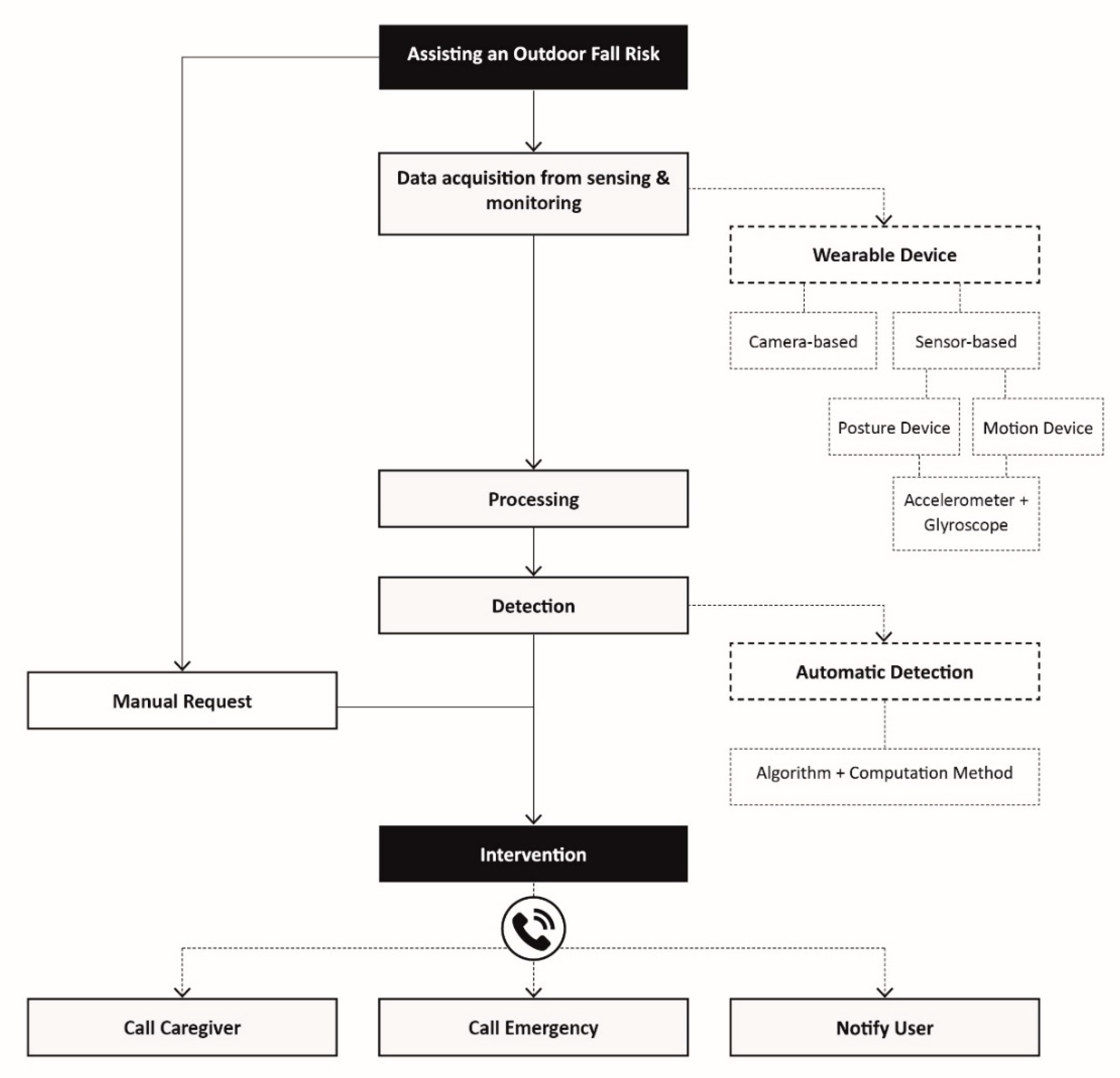
- The use of onsite or remote monitoring tools for rapid detection of environmental changes, changing needs and events. Examples of tools are mobile and static sensors, and software tools for collection, fusion and analysis of data.
- Risk detection and alerts to trigger activation of assistive devices for an emergency response.
- Localization of affected older persons with easy to use communication interfaces.
- eWatch for activity recognition and integrating activity data with location information.
- GPS positioning system to locate the individual in outdoor scenario.
- RFID-based location-finding and tracking with guidance system.
- GSM for patient’s alert message and communication.
3.2. Mobile Health (mHealth)
- Ubiquity: a technology is referred to as ubiquitous when it is omnipresent within the zone of its deployment.
- Mobility: this refers to the capability of a device to modify its physical connection point to the telecommunication network without losing its logical connectivity.
- Security: this includes service authorization, confidentiality provision, and station and infrastructure authentication.
- Connection capability: this can be circuit or packet mode of operation. An example of a circuit mode is the conventional telephony with a continuous electrical connection between end points with orderly arrangement of data at the point of exit. The packet mode is currently in use with discrete packets via different routes and can arrive out of order.
- Connection topology: this could be point to point (unicast), point to multipoint (multicast) or point to all points (broadcast).
- Content type: examples include data, video, audio and image.
- Quality of Service (QoS): this refers to the ability of a device to maintain an established connection.
3.3. Reference Architecture for eHealth
4. Discussion
- Wearable: in this approach, the individual to be monitored or tracked wears or carries the sensors [21,22,23,24,25,26,27,28,29,34,36,37,38,39,40,41]. A common example of this approach is the smart watch that has multimodal sensors and is therefore capable of sensing multiple physiological parameters through the wrist.
- Environmental: in this approach, the sensors are deployed in the outdoor space environment or on furniture that will be used by the elderly demographic [32].
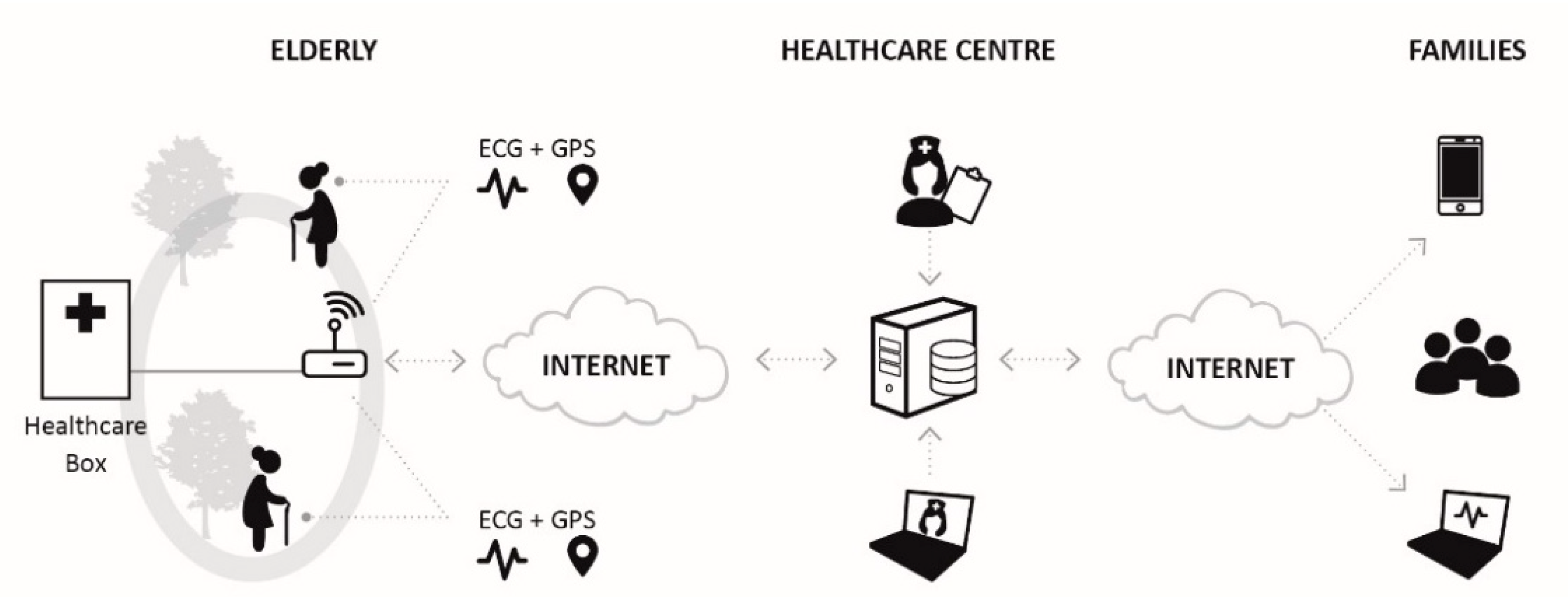
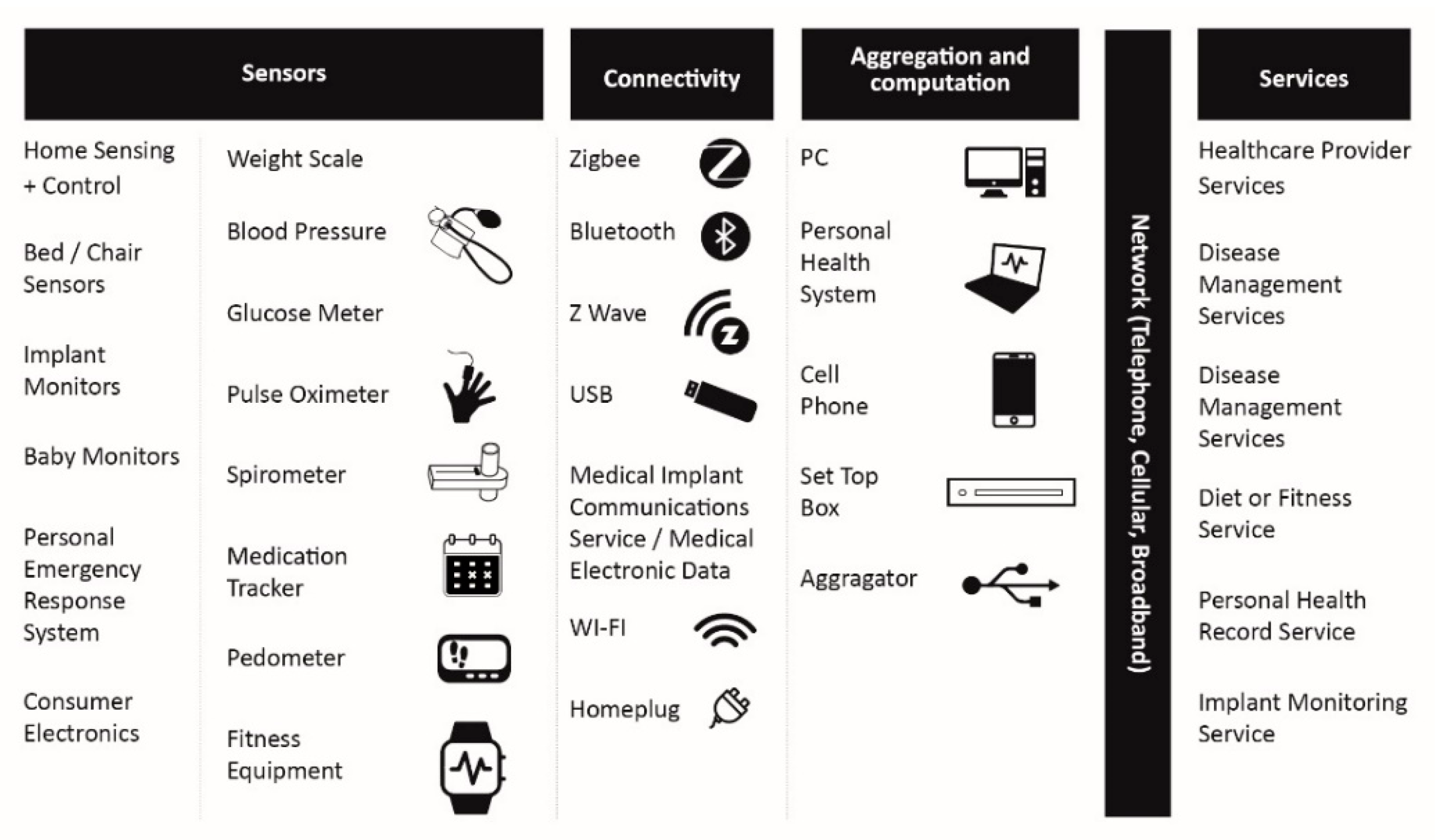
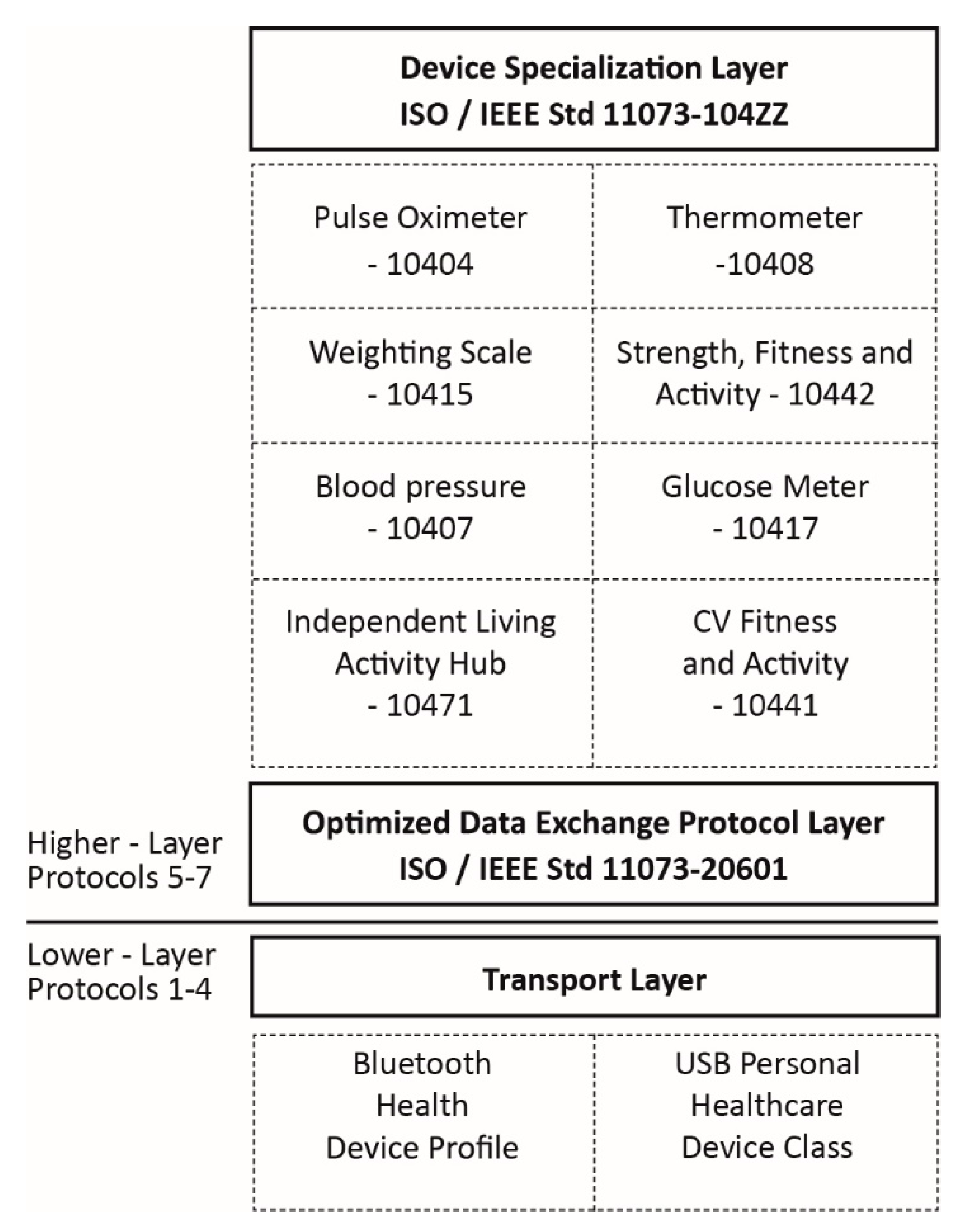
- Sensor access: this refers to short-range technologies such as ZigBee, IEEE 802.15.4 and Bluetooth, which are used by the sensor to send its data to a gateway. This is referred to as the PAN and LAN interfaces in the Continua end-to-end reference architecture (Figure 9).
- Backhaul access: this refers to long-range technologies such as cellular technology or the fixed IP network, which is used by the gateway to send aggregated sensor data to a server. This is referred to as the WAN interface in the Continua end-to-end reference architecture (Figure 9).
- Technology application considering the dynamic and often harsh outdoor environmental conditions, which could hamper availability and accessibility of wireless network services. Research is required to investigate the performance of various eHealth technologies in outdoor spaces for telehealth monitoring. Metrics that can be used to characterize performance include reliability, throughput, latency and security.
- Deployment of interoperable medical devices to ensure devices from various manufactures can be integrated seamlessly in outdoor environments. This means research efforts need to be geared towards developing standards and protocols for heterogeneous devices to communicate in a plug-and-play fashion. Also, there is a need to ensure backward compatibility with existing legacy devices to operate easily with new medical devices.
- Design, development and deployment of technology to manage user mobility and ensure a more accurate localization of older persons in case of emergency. Research related to the human body (e.g., design of wireless PAN) needs to consider a realistic abstraction of the inter-body channel variations which happens as a result of human mobility behaviours [74]. Also, research is currently required to design and manufacture power or battery sources with higher efficiency and enhanced battery life for assistive technologies used in a landscape-built environment.
- Data security and confidentiality research is required to avoid unauthorized access to private health information system. The integration of Cloud computing and IoT-based health architectures opens a new research area especially in data security.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization [WHO]. Ageing and Health. Available online: http://www.who.int/mediacentre/factsheets/fs404/en/ (accessed on 20 November 2019).
- World Health Organization [WHO]. National Institute on Aging: Global Health and Aging. Available online: http://www.who.int/ageing/publications/global_health.pdf (accessed on 10 February 2020).
- Lohr, K.N.; Field, M.J. Guidelines for Clinical Practice: From Development to Use; National Academies Press: Washington, DC, USA, 1992; pp. 45–64. [Google Scholar]
- Nee, O.; Hein, A.; Gorath, T.; Lsmann, N.H.; Laleci, G.B.; Yuksel, M.; Ludwig, R. SAPHIRE: Intelligent healthcare monitoring based on semantic interoperability platform: Pilot applications. IET Commun. 2008, 2, 192–201. [Google Scholar] [CrossRef]
- Ministry of Health. New Zealand Health Strategy: Future Direction. Available online: https://www.health.govt.nz/system/files/documents/publications/new-zealand-health-strategy-futuredirection-2016-apr16.pdf (accessed on 3 December 2019).
- Merilampi, S.; Sirkka, A. Introduction to Smart eHealth and eCare Technologies; CRC Press: London, UK, 2016; pp. 3–84. [Google Scholar]
- Scholz, N. European Parliamentary Research Service: eHealth-Technology for Health. Available online: http://www.europarl.europa.eu/thinktank/en/document.html?reference=EPRS_BRI(2015)551324 (accessed on 29 November 2019).
- Iakovidis, I.; Le Dour, O.; Karp, P. Biomedical Engineering and eHealth min Europe-Outcomes and Challenges of Past and Current EU Research Programs. IEEE Eng. Med. Biol. Mag. 2007, 26, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Cranney, L.; Phongsavan, P.; Kariuki, M.; Stride, V.; Scott, A.; Hua, M.; Bauman, A. Impact of an outdoor gym on park users’ physical activity: A natural experiment. Health Place 2016, 37, 26–34. [Google Scholar] [CrossRef]
- Doukas, C.; Metsis, V.; Becker, E.; Le, Z.; Makedon, F.; Maglogiannis, I. Digital cities of the future: Extending @home assistive technologies for the elderly and the disabled. Telemat. Inform. 2011, 28, 176–190. [Google Scholar] [CrossRef]
- Kershaw, C.; Lim, J.; McIntosh, J.; Cornwall, J.; Marques, B. Developing Resilience, Independence and Well-being in Older Adults through Interactive Outdoor Spaces. In Proceedings of the Passive Low Energy Architecture (PLEA) Conference, Edinburgh, UK, 2–5 July 2017; Luisa, B., Susan, R., Fergus, N., Eds.; NCEUB: Edinburgh, UK, 2017; pp. 4676–4685. [Google Scholar]
- McCormack, G.R.; Rock, M.; Swanson, K.; Burton, L.; Massolo, A. Physical activity patterns in urban neighbourhood parks: Insights from a multiple case study. BMC Public Health 2014, 14, 962. [Google Scholar] [CrossRef] [Green Version]
- Kershaw, C.; Cornwall, J.; McIntosh, J.; Marques, B. Therapeutic landscape design for older persons health and well-being. In Proceedings of the Third International Conference of Changing Cities, Spatial Design, Landscape and Socio-Economic Dimensions, Syros, Greece, 26–30 June 2017; Aspa, G., Ed.; Grafima Publications: Thessaly, Greece, 2017; pp. 1163–1170. [Google Scholar]
- Kershaw, C.; McIntosh, J.; Marques, B.; Cornwall, J.; Stoner, L.; Wood, P. A potential role for outdoor, interactive spaces as a healthcare intervention for older persons. Perspect. Public Health 2017, 137, 212–213. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Kaklauskas, A.; Abraham, A.; Dzemyda, G.; Raslanas, S.; Seniut, M.; Ubarte, I.; Kurasova, O.; Binkyte-Veliene, A.; Cerkauskas, J. Emotional, affective and biometrical states analytics of a built environment. Eng. Appl. Artif. Intell. 2020, 91, 103621. [Google Scholar] [CrossRef]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, e20. [Google Scholar] [CrossRef]
- Beauvais, B.S.; Rialle, V.; Sablier, J. Myvigi: An android application to detect fall and wandering. In Proceedings of the Sixth International Conference on Mobile Ubiquitous Computing, Systems, Services and Technologies, Barcelona, Spain, 23–28 September 2012; UBICOMM: Barcelona, Spain, 2012; pp. 156–160. [Google Scholar]
- Sposaro, F.; Danielson, J.; Tyson, G. iWander: An Android application for dementia patients. In Proceedings of the Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 3875–3878. [Google Scholar]
- Foxlin, E. Pedestrian tracking with shoe-mounted inertial sensors. IEEE Comput. Graph. Appl. 2005, 25, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aziz, A.A.; Abdel-Salam, H.; El-Sayad, Z. The role of ICTs in creating the new social public place of the digital era. Alex. Eng. J. 2016, 55, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.C.; Chiu, M.J.; Hsiao, C.C.; Lee, R.G.; Tsai, Y.S. Wireless Health Care Service System for Elderly with Dementia. IEEE Trans. Inform. Technol. Biomed. 2006, 10, 696–704. [Google Scholar] [CrossRef]
- Lin, C.C.; Lin, P.Y.; Lu, P.K.; Hsieh, G.Y.; Lee, W.L.; Lee, R.G. A Healthcare Integration System for Disease Assessment and Safety Monitoring of Dementia Patients. IEEE Trans. Inform. Technol. Biomed. 2008, 12, 579–586. [Google Scholar]
- Rainham, D.; Krewski, D.; McDowell, I.; Sawada, M.; Liekens, B. Development of a wearable global positioning system for place and health research. Int. J. Health Geogr. 2008, 7, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oswald, F.; Wahl, H.-W.; Voss, E.; Schilling, O.; Freytag, T.; Auslander, G.; Shoval, N.; Heinik, J.; Landau, R. The Use of Tracking Technologies for the Analysis of Outdoor Mobility in the Face of Dementia: First Steps into a Project and Some Illustrative Findings from Germany. J. Hous. Elder. 2010, 24, 55–73. [Google Scholar] [CrossRef]
- Zheng, H.; Nugent, C.; McCullagh, P.; Huang, Y.; Zhang, S.; Burns, W.; Davies, R.; Black, N.; Wright, P.; Mawson, S.; et al. Smart self-management: Assistive technology to support people with chronic disease. J. Telemed. Telecare 2010, 16, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.N.K.; Wheeler, S.; Tavares, C.; Jones, R. How smartphones are changing the face of mobile and participatory healthcare: An overview, with example from eCAALYX. Biomed. Eng. Online 2011, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Worringham, C.; Rojek, A.; Stewart, I. Development and Feasibility of a Smartphone, ECG and GPS Based System for Remotely Monitoring Exercise in Cardiac Rehabilitation. PLoS ONE 2011, 6, e14669. [Google Scholar] [CrossRef] [Green Version]
- Shanin, F.; Das, H.A.; Krishnan, G.A.; Neha, L.S.; Thaha, N.; Aneesh, R.P.; Embrandiri, S.; Jayakrishan, S. Portable and centralised e-health record system for patient monitoring using internet of things (IoT). In Proceedings of the International CET Conference on Control, Communication, and Computing (IC4), Thiruvananthapuram, India, 5–7 July 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 165–170. [Google Scholar]
- Blaya, J.A.; Fraser, H.S.; Holt, B. E-health technologies show promise in developing countries. Health Aff. 2010, 29, 244–251. [Google Scholar] [CrossRef]
- Heikkilä, T.; Strömmer, E.; Kivikunnas, S.; Järviluoma, M.; Korkalainen, M.; Kyllönen, V.; Sarjanoja, E.M.; Peltomaa, I. Low intrusive Ehealth monitoring: Human posture and activity level detection with an intelligent furniture network. IEEE Wirel. Commun. 2013, 20, 57–63. [Google Scholar] [CrossRef]
- Schwickert, L.; Becker, C.; Lindemann, U.; Maréchal, C.; Bourke, A.; Chiari, L.; Helbostad, J.L.; Zijlstra, W.; Aminian, K.; Todd, C.; et al. Fall detection with body-worn sensors. Z. Gerontol. Geriatr. 2013, 46, 706–719. [Google Scholar] [CrossRef]
- Yared, R.; Mallat, H.K.; Abdulrazak, B. Ambient technology to support elderly people in outdoor risk situations. In Proceedings of the International Conference on Information and Communication Technologies for Ageing Well and e-Health, Lisbon, Portugal, 20–22 May 2015; Springer: Cham, Switzerland, 2015; pp. 35–56. [Google Scholar]
- Islam, S.R.; Kwak, D.; Kabir, M.H.; Hossain, M.; Kwak, K.S. The internet of things for health care: A comprehensive survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Wang, L.H.; Hsiao, Y.M.; Xie, X.Q.; Lee, S.Y. An outdoor intelligent healthcare monitoring device for the elderly. IEEE Trans. Consum. Electron. 2016, 62, 128–135. [Google Scholar] [CrossRef]
- Hossain, M.S.; Muhammad, G. Cloud-assisted Industrial Internet of Things (IIoT)—Enabled framework for health monitoring. Comput. Netw. 2016, 101, 192–202. [Google Scholar] [CrossRef]
- Almeida, A.; Fiore, A.; Mainetti, L.; Mulero, R.; Patrono, L.; Rametta, P. An IoT-Aware Architecture for Collecting and Managing Data Related to Elderly Behavior. Wirel. Commun. Mob. Comput. 2017, 2017, 5051915. [Google Scholar] [CrossRef]
- Hu, J.-X.; Chen, C.-L.; Fan, C.-L.; Wang, K.-H. An Intelligent and Secure Health Monitoring Scheme Using IoT Sensor Based on Cloud Computing. J. Sens. 2017, 2017, 3734764. [Google Scholar] [CrossRef]
- Garcia, A.C.B.; Vivacqua, A.S.; Sánchez-Pi, N.; Martí, L.; Molina, J.M. Crowd-Based Ambient Assisted Living to Monitor the Elderly’s Health Outdoors. IEEE Softw. 2017, 34, 53–57. [Google Scholar] [CrossRef]
- Chan, M.; Campo, E.; Bourennane, W.; Estève, D. Connectivity for the indoor and outdoor elderly people safety management: An example from our current project. In Proceedings of the European Symposium on Biomedical Engineering (ESBME 2010), Kuala Lumpur, Malaysia, 30 November–2 December 2010; pp. 1–4. [Google Scholar]
- Boulos, M.N.K.; Brewer, A.C.; Karimkhani, C.; Buller, D.B.; Dellavalle, R.P. Mobile medical and health apps: State of the art, concerns, regulatory control and certification. Online J. Public Health Inform. 2014, 5, 229. [Google Scholar]
- Davis, T.L.; DiClemente, R.; Prietula, M. Taking mHealth Forward: Examining the Core Characteristics. JMIR mHealth uHealth 2016, 4, e97. [Google Scholar] [CrossRef]
- Coughlan, J.; Manduchi, R. Functional assessment of a camera phone-based wayfinding system operated by blind and visually impaired users. Int. J. Artif. Intell. Tools 2009, 18, 379–397. [Google Scholar] [CrossRef] [PubMed]
- ETSI. eHEALTH; Architecture; Analysis of User Service Models, Technologies and Applications Supporting eHealth. Available online: https://www.etsi.org/deliver/etsi_tr/102700_102799/102764/01.01.01_60/tr_102764v010101p.pdf (accessed on 29 January 2020).
- Piette, J.D.; Lun, K.C.; Moura, L.A., Jr.; Fraser, H.S.; Mechael, P.N.; Powell, J.; Khoja, S.R. Impacts of e-health on the outcomes of care in low-and middle-income countries: Where do we go from here? Bull. World Health Organ. 2012, 90, 365–372. [Google Scholar] [CrossRef]
- Wiljer, D.; Urowitz, S.; Apatu, E.; DeLenardo, C.; Eysenbach, G.; Harth, T.; Pai, H.; Leonard, K.; Canadian Committee for Patient Accessible Health Records (CCPAEHR). Patient accessible electronic health records: Exploring recommendations for successful implementation strategies. J. Med. Internet Res. 2008, 10, e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagliari, C.; Detmer, D.; Singleton, P. Potential of electronic personal health records. BMJ Br. Med. J. 2007, 335, 330. [Google Scholar] [CrossRef] [Green Version]
- Chehri, A.; Mouftah, H.; Jeon, G. A Smart Network Architecture for eHealth Applications. In Intelligent Interactive Multimedia Systems and Services; Tsihrintzis, G.A., Damiani, E., Virvou, M., Howlett, R.J., Jain, L.C., Eds.; Springer: Berlin, Germany, 2010; pp. 157–166. [Google Scholar]
- Wartena, F.; Muskens, J.; Schmitt, L.; Petkovic, M. Continua: The reference architecture of a personal telehealth ecosystem. In Proceedings of the 12th IEEE International Conference on e-Health Networking Applications and Services (Healthcom 2010), Lyon, France, 1–3 July 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 399–404. [Google Scholar]
- Moorman, B. Medical Device Interoperability: Overview of Key Initiatives. Biomed. Instrum. Technol. 2010, 44, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Carroll, R.; Cnossen, R.; Schnell, M.; Simons, D. Continua: An Interoperable Personal Healthcare Ecosystem. IEEE Pervasive Comput. 2007, 6, 90–94. [Google Scholar] [CrossRef]
- Kartsakli, E.; Lalos, A.S.; Antonopoulos, A.; Tennina, S.; Renzo, M.D.; Alonso, L.; Verikoukis, C. A Survey on M2M Systems for mHealth: A Wireless Communications Perspective. Sensors 2014, 14, 18009–18052. [Google Scholar] [CrossRef] [Green Version]
- Wark, T.; Hu, W.; Corke, P.; Hodge, J.; Keto, A.; Mackey, B.; Foley, G.; Sikka, P.; Brunig, M. Springbrook: Challenges in developing a long-term, rainforest wireless sensor network. In Proceedings of the 2008 International Conference on Intelligent Sensors, Sensor Networks and Information Processing, Sydney, Australia, 15–18 December 2008; IEEE: Piscataway, NJ, USA, 2008; pp. 599–604. [Google Scholar]
- Tedesco, S.; Barton, J.; O’Flynn, B. A review of activity trackers for senior citizens: Research perspectives, commercial landscape and the role of the insurance industry. Sensors 2017, 17, 1277. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.C.; Lin, C.C.; Wang, Y.H.; Hsieh, H.J. Development of Health Care System Based on Wearable Devices. In Proceedings of the 2019 Prognostics and System Health Management Conference (PHM-Paris), Paris, France, 2–5 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 249–252. [Google Scholar]
- Yared, R.; Abou Jaoude, C.; Demerjian, J. Smart-phone based system to monitor walking activity: MHealth solution. In Proceedings of the 2018 IEEE Middle East and North Africa Communications Conference (MENACOMM), Jounieh, Lebanon, 18–20 April 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1–5. [Google Scholar]
- Mekki, K.; Bajic, E.; Chaxel, F.; Meyer, F. A comparative study of LPWAN technologies for large-scale IoT deployment. ICT Express 2019, 5, 1–7. [Google Scholar] [CrossRef]
- Gaddam, A.; Wilkin, T.; Angelova, M.; Valera, A.; McIntosh, J.; Marques, B. Design & Development of IoT Based Rehabilitation Outdoor Landscape for Gait Phase Recognition. In Proceedings of the 2019 13th International Conference on Sensing Technology (ICST) 2019, Sydney, Australia, 2–4 December 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1–7. [Google Scholar]
- Mehmood, Y.; Haider, N.; Imran, M.; Timm-Giel, A.; Guizani, M. M2M communications in 5G: State-of-the-art architecture, recent advances, and research challenges. IEEE Commun. Mag. 2017, 55, 194–201. [Google Scholar] [CrossRef]
- European Commission. eHealth Network: Refined eHealth European Interoperability Framework. Available online: https://ec.europa.eu/health//sites/health/files/ehealth/docs/ev_20151123_co03_en.pdf (accessed on 10 December 2019).
- Nijeweme-D’Hollosy, W.O.; Velsen, L.V.; Huygens, M.; Hermens, H. Requirements for and Barriers towards Interoperable eHealth Technology in Primary Care. IEEE Internet Comput. 2015, 19, 10–19. [Google Scholar] [CrossRef]
- Rezaei, R.; Chiew, T.K.; Lee, S.P.; Shams Aliee, Z. Interoperability evaluation models: A systematic review. Comput. Ind. 2014, 65, 1–23. [Google Scholar] [CrossRef]
- Photovoltaics, D.G.; Storage, E. IEEE Guide for Smart Grid Interoperability of Energy Technology and Information Technology Operation with the Electric Power System (EPS), End-Use Applications, and Loads; IEEE: New York, NY, USA, 2011; pp. 1–126. [Google Scholar] [CrossRef]
- Sheikh, A.; Sood, H.S.; Bates, D.W. Leveraging health information technology to achieve the “triple aim” of healthcare reform. J. Am. Med. Inform. Assoc. 2015, 22, 849–856. [Google Scholar] [CrossRef]
- Zutshi, A.; Grilo, A.; Jardim-Goncalves, R. The business interoperability quotient measurement model. Comput. Ind. 2012, 63, 389–404. [Google Scholar] [CrossRef]
- Naudet, Y.; Latour, T.; Guedria, W.; Chen, D. Towards a systemic formalisation of interoperability. Comput. Ind. 2010, 61, 176–185. [Google Scholar] [CrossRef]
- Munk, S. An analysis of basic interoperability related terms, system of interoperability types. Acad. Appl. Res. Mil. Sci. 2002, 2002, 117–132. [Google Scholar]
- Novakouski, M.; Lewis, G. Interoperability in the e-Government Context (CMU/SEI-2011-TN-014). Available online: http://resources.sei.cmu.edu/library/asset-view.cfm?AssetID=9869 (accessed on 2 February 2020).
- Veer, H.; Wiles, A. Achieving Technical Interoperability-the ETSI Approach, European Telecommunications Standards Institute. Available online: https://www.etsi.org/images/files/ETSIWhitePapers/IOP%20whitepaper%20Edition%203%20final.pdf (accessed on 10 November 2019).
- Guijarro, L. Semantic interoperability in eGovernment initiatives. Comput. Stand. Interfaces 2009, 31, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Charalabidis, Y.; Panetto, H.; Loukis, E.; Mertins, K. Interoperability approaches for enterprises and administrations worldwide. Electron. J. e-Commer. Tools Appl. 2008, 2, 1–10. [Google Scholar]
- Scott, P. Meeting the challenges of healthcare interoperability. Healthc. IT Manag. 2009, 4, 24–25. [Google Scholar]
- Alam, M.; Hamida, E. Surveying Wearable Human Assistive Technology for Life and Safety Critical Applications: Standards, Challenges and Opportunities. Sensors 2014, 14, 9153–9209. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Peer reviewed articles (2005–2018) Empirical research English language literature Outdoor built environment eHealth/assistive technologies in outdoor space Aged 60 years or older with complex needs | Non-peer reviewed articles Smart homes and home-health monitoring Conference proceedings Narrative reviews, lecture notes and studies published in theses Non-health related studies and technology applications |
| Study | Medical Condition and Disability Addressed | Acquisition of Technology | Data Communication Technology | Main Outcomes |
|---|---|---|---|---|
| Foxlin [20] | Patients’ daily activities monitoring and on-foot location tracking | wireless inertial sensor (magnetometer) with Global Positioning System (GPS) | Radio frequency (RF) module | The system used a shoe-mounted miniature magnetometer coupled wirelessly to a personal digital assistant (PDA) to track patients. |
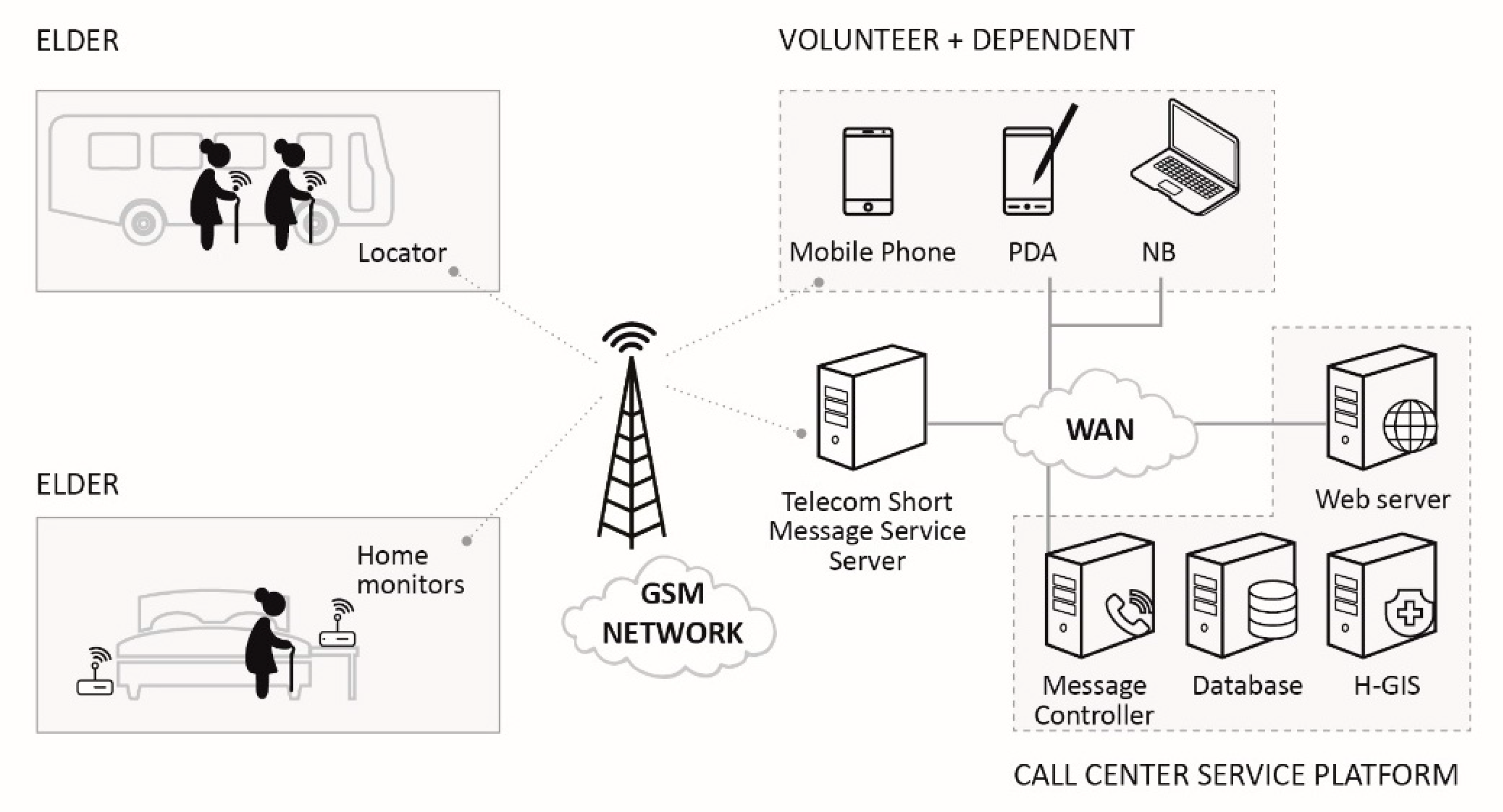
| Lin et al. [23] | Dementia | Motion sensor with GPS | Global System for Mobile Communications (GSM) | Emergency messages and commands from remote server were sent via a GSM link. |
| Lin et al. [24] | Disease assessment and outdoor safety monitoring of dementia patients | RFID tag | RF and Bluetooth modules with Mobile phone | The system used different size tags and tame transformation signatures (TTS) algorithm to ensure privacy. |
| Rainham et al. [25] | Monitoring location | GPS | Satellites | A lightweight, wearable GPS receiver to measure the temporal and spatial features of daily activities was developed. |
| Zheng et al. [27] | Chronic conditions (diabetes mellitus and cardiovascular disease) | Accelerometer and GPS | Cellular technology | A smart phone having an accelerometer and a GPS was used to monitor patients’ outdoor activity and location. |
| Oswald et al. [26] | Analysis of outdoor mobility in the face of dementia | Wrist-watch with body contact sensor and RF capability, and GPS | GSM | The accuracy of data collected varied depending on the local terrain and weather conditions. |
| Boulos et al. [28] | Chronic conditions (diabetes mellitus and cardiovascular disease) | smart garment with wireless health sensors and GPS | Cellular technology and Bluetooth | A smartphone app coupled with the GPS location sensor to initiate a bidirectional communication between the patient’s PAN and a remote server accessible over the internet was developed. |
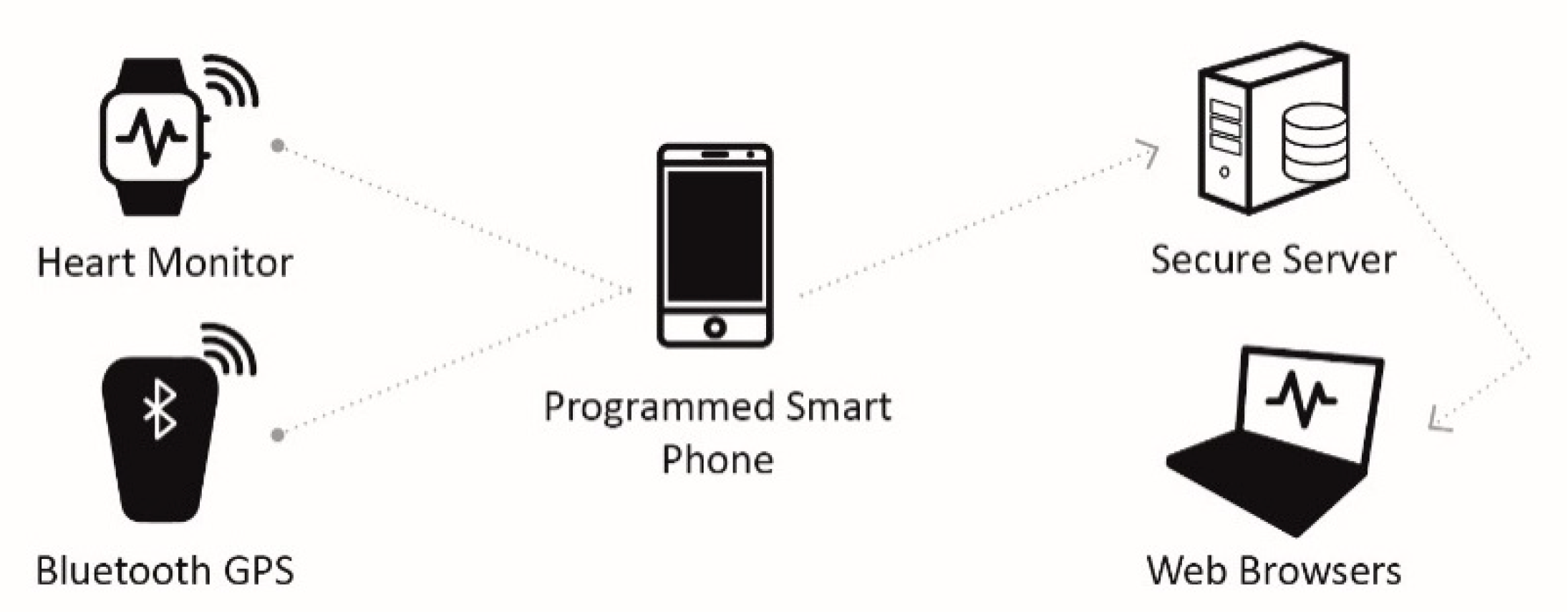
| Worringham et al. [29] | Cardiac rehabilitation | Electrocardiogram (ECG), heart rate and GPS modules | Cellular technology and Bluetooth | The system provided a more flexible way to remotely monitor supervised cardiac rehabilitation via a programmed smartphone to asecure server for real-time monitoring by qualified medical personnel. |
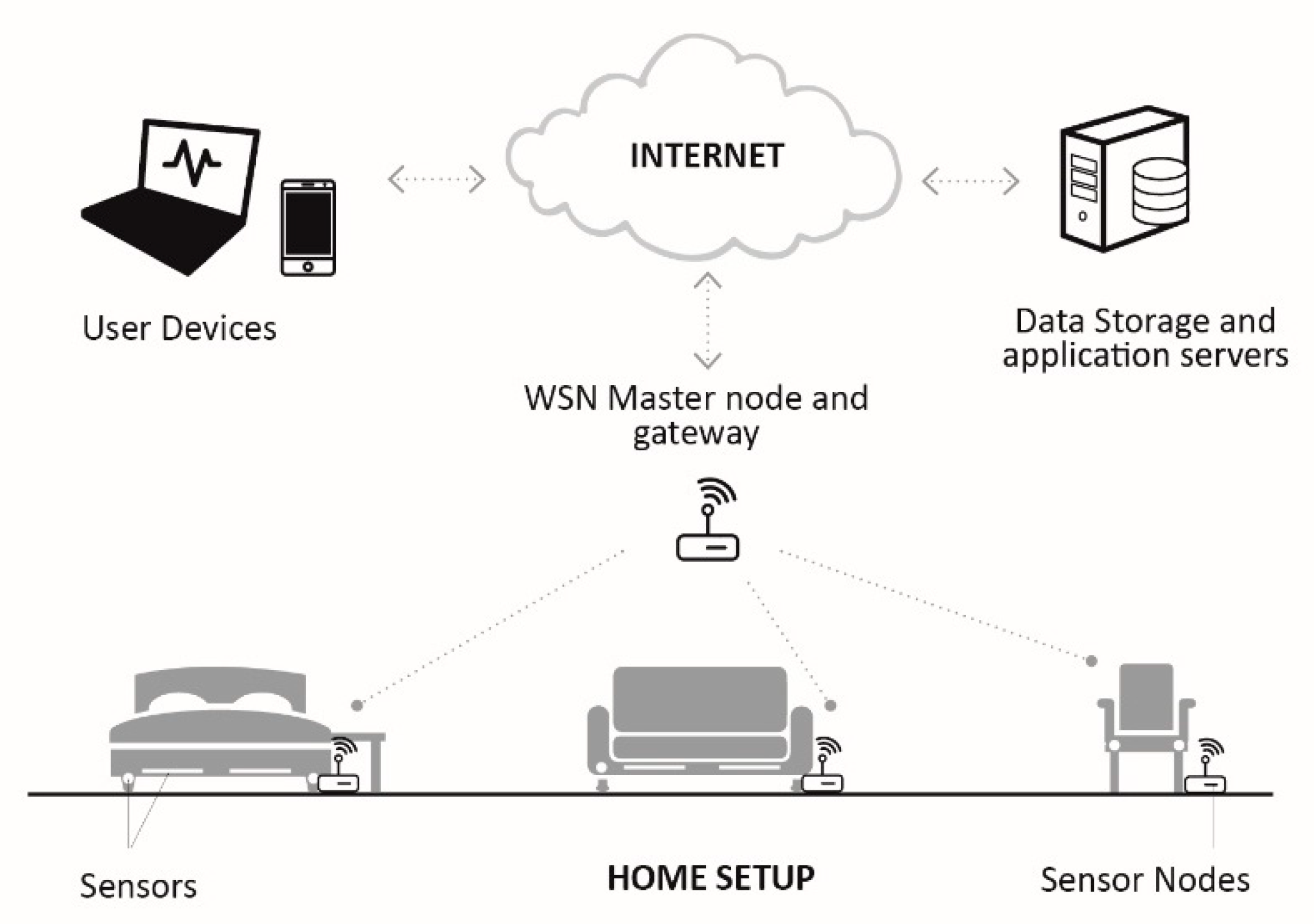
| Heikkilä et al. [32] | Posture and activity monitoring | Capacitive sensors in a wireless sensor network (WSN) | Fixed or wireless Internet Protocol (IP) network and Institute of Electrical and Electronics Engineers (IEEE) 802.15.4 | Intelligent furniture was developed to detect variations in activities and postures using a proprietary WSN and internet. |
| Yared et al. [34] | Monitoring and detecting falls, wandering and other related risks | Accelerometer, gyroscope, Radio-frequency identification (RFID) tags and GPS | Cellular technology | The use of eHealth technologies capable of delivering ubiquitous assistance services and integrated platforms that support safety, independence and overall well-being of older persons in outdoor spaces was proposed. |
| Wang et al. [36] | ECG monitoring, patient outdoor position and location | ECG module and GPS | ZigBee | The proposed intelligent system consists of multi-function healthcare box placed outdoors which monitors the GPS and ECG data of the patient. Accuracy of detection depends on movement, location variation and interference. |
| Hossain and Muhammad [37] | ECG monitoring | ECG module | Internet and Smartphone with Bluetooth/Wi-Fi | A Cloud integrated Internet of Things (IoT) enabled ECG signal monitoring with watermarked data has been proposed. |
| Garcia et al. [40] | Temperature, wandering and fall detection | GPS, Accelerometer, Light and Temperature sensors | Internet | Elderly data obtained from sensors integrated with a mobile phone were sent via the internet to the eHealth monitor. Trusted, private and neighborhood-based social network such as “Nextdoor” and “GoNeighbour” were adopted for data privacy and security. |
| Almeida et al. [38] | Behavioral analysis and risk detection | Personal data capturing systems consisting of different types of sensors to capture mobility, outdoor localization and ambient parameters. | Cellular technology | The proposed smart city-oriented system captures and processes heterogeneous data in an assistive environment at multiple levels. The data model allows participating cities to choose the level of abstraction that can be used for system integration. |
| Chan et al. [41] | Mobility, posture assessment and fall detection | eWatch, GPS and RFID tag | RF, ZigBee and GSM | A flexible smart system capable of operating both indoor and outdoor with multisensory unit to monitor the trajectory of an older person was implemented. |
| Hu et al. [39] | Chronic conditions | IoT medical sensor | Cellular technology | An IoT sensor-based Cloud computing architecture was proposed to safely and securely monitor the health of older persons for chronic conditions anywhere. |
| Global System for Mobile Communications (GSM) | General Packet Radio Services (GPRS) | Terrestrial Trunked Radio (TETRA) | Third Generation (3G) | Wireless Fidelity (WiFi) (IEEE 802.11a/b/g/n) | Worldwide Interoperability for Microwave Access (WiMAX) | |
|---|---|---|---|---|---|---|
| Description | Cellular network used for mobile phones. | General Packet Radio Service | Private mobile radio for ambulance and a host of other services | Third-generation mobile phone network technology | A suite of wireless Ethernet standards | Worldwide Interoperability for Microwave Access operating in the licensed spectrum zone |
| Mobility | Yes | Yes | Yes | Yes | Limited | Yes |
| Security | Privacy enhanced | Privacy enhanced | Yes | Privacy enhanced | No | No |
| Connection capability | Packet, Circuit | Packet | Packet, Circuit | Packet, Circuit | Packet | Packet |
| Connection topology | Unicast | Unicast | Unicast, Multicast, Broadcast | Unicast, Multicast, Broadcast | Unicast, Multicast, Broadcast | Unicast, Multicast, Broadcast |
| Content | Audio | Data | Audio, Data | Audio, Data, Video | Data | Data, Video |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, B.; McIntosh, J.; Valera, A.; Gaddam, A. Innovative and Assistive eHealth Technologies for Smart Therapeutic and Rehabilitation Outdoor Spaces for the Elderly Demographic. Multimodal Technol. Interact. 2020, 4, 76. https://doi.org/10.3390/mti4040076
Marques B, McIntosh J, Valera A, Gaddam A. Innovative and Assistive eHealth Technologies for Smart Therapeutic and Rehabilitation Outdoor Spaces for the Elderly Demographic. Multimodal Technologies and Interaction. 2020; 4(4):76. https://doi.org/10.3390/mti4040076
Chicago/Turabian StyleMarques, Bruno, Jacqueline McIntosh, Alvin Valera, and Anuroop Gaddam. 2020. "Innovative and Assistive eHealth Technologies for Smart Therapeutic and Rehabilitation Outdoor Spaces for the Elderly Demographic" Multimodal Technologies and Interaction 4, no. 4: 76. https://doi.org/10.3390/mti4040076