
The Relationship between Posture and Muscle Tensive Dysphonia in Teachers: A Systematic Scoping Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Collection and Extraction
2.3. Quality Assessment
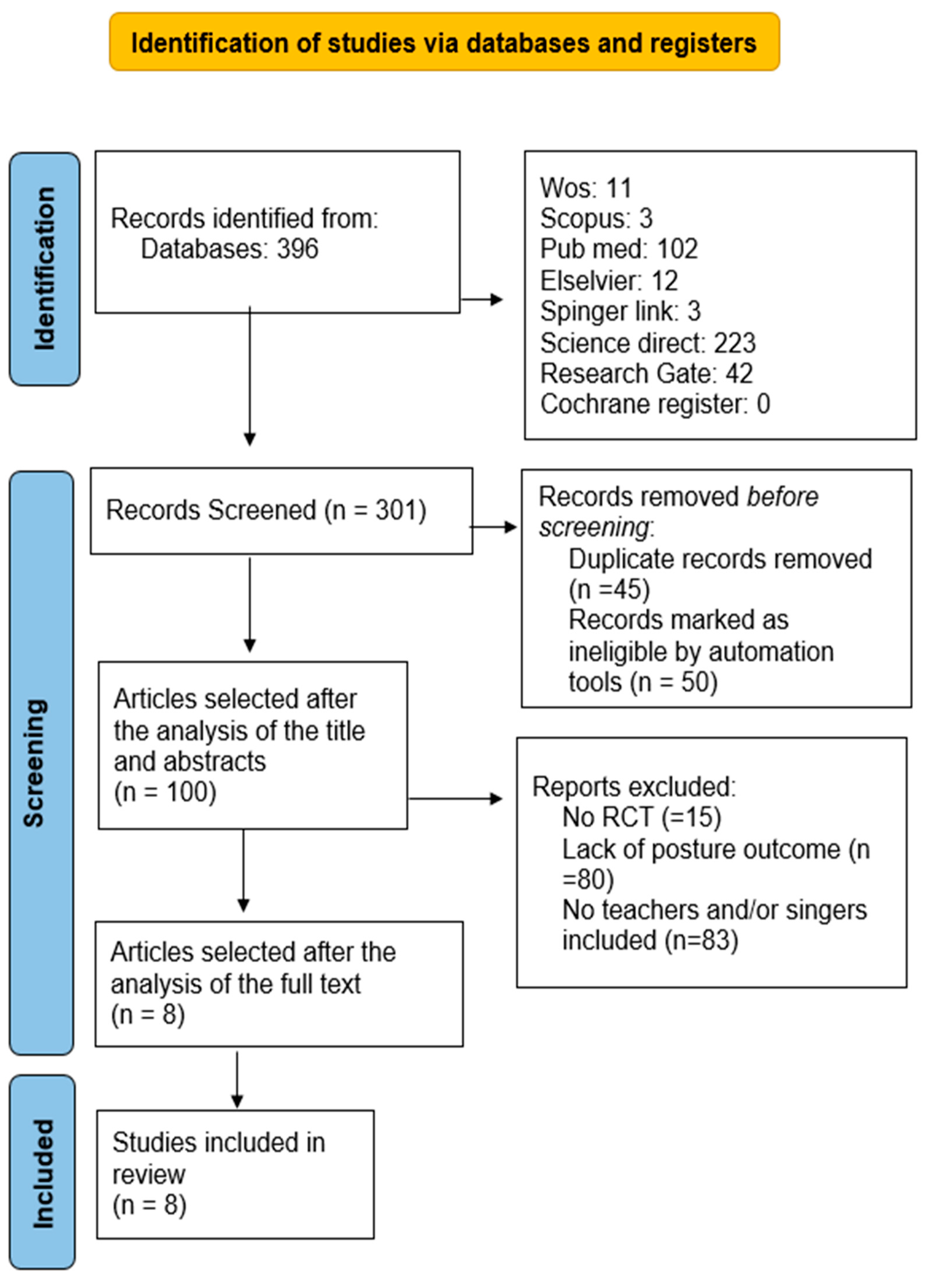
3. Results
3.1. Description of Studies
3.2. Articles Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gobl, C.; Chasaide, A.N. The role of voice quality in communicating emotion, mood and attitude. Speech Commun. 2003, 40, 189–212. [Google Scholar] [CrossRef]
- Patel, R.R.; Awan, S.N.; Barkmeier-Kraemer, J.; Courey, M.; Deliyski, D.; Eadie, T.; Paul, D.; Švec, J.G.; Hillman, R. Recommended protocols for instrumental assessment of voice: American Speech-Language-Hearing Association expert panel to develop a protocol for instrumental assessment of vocal function. Am. J. Speech-Lang. Pathol. 2018, 27, 887–905. [Google Scholar] [CrossRef] [PubMed]
- Scherer, K.R. Expression of emotion in voice and music. J. Voice 1995, 9, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kumar, N.; Tsiartas, A.; Li, M.; Narayanan, S.S. Automatic intelligibility classification of sentence-level pathological speech. Comput. Speech Lang. 2015, 29, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Hruza, V. The Influence of Bernoulli’s Effect on the Function of the Vocal Cords. Eng. Mech. 2008, 15, 175–180. [Google Scholar]
- Zhang, Z. Mechanics of human voice production and control. J. Acoust. Soc. Am. 2016, 140, 2614–2635. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, P. Vocal tract anatomy and the neural bases of talking. J. Phon. 2012, 40, 608–622. [Google Scholar] [CrossRef]
- Zhang, Z. On the Importance of Overall Regulation of Singing to Vocal Music Performance. In Proceedings of the 2017 International Seminar on Social Science and Humanities Research (SSHR 2017); Atlantis Press: Amsterdam, The Netherlands, 2018; pp. 376–380. [Google Scholar]
- Master, S.; Guzman, M.; Azócar, M.J.; Muñoz, D.; Bortnem, C. How do laryngeal and respiratory functions contribute to differentiate actors/actresses and untrained voices? J. Voice 2015, 29, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Pettersen, V.; Eggebø, T.M. The movement of the diaphragm monitored by ultrasound imaging: Preliminary findings of diaphragm movements in classical singing. Logop. Phoniatr. Vocology 2010, 35, 105–112. [Google Scholar] [CrossRef]
- Myers, B.R.; Finnegan, E.M. The effects of articulation on the perceived loudness of the projected voice. J. Voice 2015, 29, 390.e9–390.e15. [Google Scholar] [CrossRef]
- Montaño Aparicio, R. Prosodic and Voice Quality Cross-Language Analysis of Storytelling Expressive Categories Oriented to Text-To-Speech Synthesis. Ph.D. Thesis, Universitat Ramon Llull, Barcelona, Spain, 2016. [Google Scholar]
- Khatua, I.; Bose, A.; Kindu, I.; Jana, D. A comparative study of surgical treatment versus conservative treatment of vocal cord nodules in tertiary care hospital. Int. J. Sci. Res. 2020, 9, 39–41. [Google Scholar]
- Vasconcelos, D.d.; Gomes, A.d.O.C.; Araújo, C.M.T.d. Vocal fold polyps: Literature review. Int. Arch. Otorhinolaryngol. 2019, 23, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Aaltonen, L.-M.; Rautiainen, N.; Sellman, J.; Saarilahti, K.; Mäkitie, A.; Rihkanen, H.; Laranne, J.; Kleemola, L.; Wigren, T.; Sala, E. Voice quality after treatment of early vocal cord cancer: A randomized trial comparing laser surgery with radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Price, A.; Lawson, S.; Flannigan, C. Vocal cord granulomas diagnosed on reviewing videolaryngoscopy images. Arch. Dis. Child. 2019, 105, 381. [Google Scholar] [CrossRef] [PubMed]
- Goswami, S.; Patra, T.K. A Clinico-pathological study of Reinke’s oedema. Indian J. Otolaryngol. Head Neck Surg. 2003, 55, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, C.T. Polipi, Noduli e Granulomi delle Corde Vocali—Disturbi di Orecchio, Naso e Gola. Manuali MSD Edizione Professionisti. Manuali MSD. 2022. Available online: https://www.msdmanuals.com/it/casa/problemi-di-orecchie,-naso-e-gola/disturbi-della-laringe/polipi-noduli-e-granulomi-delle-corde-vocali (accessed on 22 January 2024).
- Sevilla, T.; Cuesta, A.; Chumillas, M.J.; Mayordomo, F.; Pedrola, L.; Palau, F.; Vílchez, J.J. Clinical, electrophysiological and morphological findings of Charcot–Marie–Tooth neuropathy with vocal cord palsy and mutations in the GDAP1 gene. Brain 2003, 126, 2023–2033. [Google Scholar] [CrossRef] [PubMed]
- Behlau, M.; Madazio, G.; Oliveira, G. Functional dysphonia: Strategies to improve patient outcomes. Patient Relat. Outcome Meas. 2015, 6, 243–253. [Google Scholar] [CrossRef]
- Behlau, M.; Madazio, G.; Pacheco, C.; Vaiano, T.; Badaró, F.; Barbara, M. Coaching strategies for behavioral voice therapy and training. J. Voice 2023, 37, 295.e1–295.e10. [Google Scholar] [CrossRef]
- Roy, N. Differential diagnosis of muscle tension dysphonia and spasmodic dysphonia. Curr. Opin. Otolaryngol. Head Neck Surg. 2010, 18, 165–170. [Google Scholar] [CrossRef]
- Feng, S.; Weng, C.; Cai, S.; Yang, Z.; Wu, M.; Kang, N. The prevalence and risk factors for perceived voice disorders in public school teachers. Laryngoscope Investig. Otolaryngol. 2022, 7, 790–798. [Google Scholar] [CrossRef]
- Bermúdez de Alvear, R.M.; Barón, F.J.; Martínez-Arquero, A.G. School teachers’ vocal use, risk factors, and voice disorder prevalence: Guidelines to detect teachers with current voice problems. Folia Phoniatr. Logop. 2011, 63, 209–215. [Google Scholar] [CrossRef]
- Assunção, A.; Bassi, I.; de Medeiros, A.; de Souza Rodrigues, C.; Gama, A. Occupational and individual risk factors for dysphonia in teachers. Occup. Med. 2012, 62, 553–559. [Google Scholar] [CrossRef]
- Hu, Q.; Zhu, S.-Y.; Luo, F.; Gao, Y.; Yang, X.-Y. High-frequency sonographic measurements of true and false vocal cords. J. Ultrasound Med. 2010, 29, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.B. Sounds of education: Teacher role and use of voice in interactions with young children. Int. J. Early Child. 2017, 49, 57–72. [Google Scholar] [CrossRef]
- Laukkanen, A.-M.; Ilomäki, I.; Leppänen, K.; Vilkman, E. Acoustic measures and self-reports of vocal fatigue by female teachers. J. Voice 2008, 22, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Caçador, M.; Paço, J. The Influence of Posture and Balance on Voice: A Review: A Influência da Postura e do Equilíbrio na Voz: Revisão. Gaz. Méd. 2018, 5. Available online: http://www.gazetamedica.com/index.php/gazeta/article/view/159 (accessed on 22 January 2024). [CrossRef]
- Priel, V.Z. A numerical definition of posture. Hum. Factors 1974, 16, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.; Skinner, M. The demands of professional opera singing on cranio-cervical posture. Eur. Spine J. 2009, 18, 562–569. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 3, e123–e130. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y. GRADE guidelines: 4. Rating the quality of evidence—Study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Schiavenato, M.; Chu, F. PICO: What it is and what it is not. Nurse Educ. Pract. 2021, 56, 103194. [Google Scholar] [CrossRef]
- Andriollo, D.B.; Frigo, L.F.; Cielo, C.A. Effect of pompage on pain, disability and craniocervical position of female teachers-Randomized clinical trial. Fisioter. Em Mov. 2022, 35, e35118. [Google Scholar] [CrossRef]
- Cardoso, R.; Meneses, R.F.; Lumini-Oliveira, J.; Pestana, P. Myofascial release effects in teachers’ posture, muscle tension and voice quality: A randomized controlled trial. J. Voice 2023, 37, 635.e15–635.e27. [Google Scholar] [CrossRef]
- Marszałek, S.; Niebudek-Bogusz, E.; Woźnicka, E.; Malińska, J.; Golusiński, W.; Śliwińska-Kowalska, M. Assessment of the influence of osteopathic myofascial techniques on normalization of the vocal tract functions in patients with occupational dysphonia. Int. J. Occup. Med. Environ. Health 2012, 25, 225–235. [Google Scholar] [CrossRef]
- Cardoso, R.; Meneses, R.F.; Lumini-Oliveira, J.; Pestana, P.; Guimaraes, B. Associations between teachers’ posture, muscle tension and voice complaints. J. Voice 2021, 35, 933.e23–933.e31. [Google Scholar] [CrossRef] [PubMed]
- Colla, C.N.; Andriollo, D.B.; Cielo, C.A. Self-assessment of teachers with normal larynges and vocal and osteomuscular complaints. J. Voice 2022. [Google Scholar] [CrossRef]
- Faralli, M.; Lapenna, R.; Pagliari, J.; Longari, F.; D’Ascanio, L.; Ricci, G. The effect of speech rehabilitation therapy for muscle tension dysphonia on global postural strategy. Hear. Balance Commun. 2017, 15, 271–281. [Google Scholar] [CrossRef]
- Kooijman, P.; De Jong, F.; Oudes, M.; Huinck, W.; Van Acht, H.; Graamans, K. Muscular tension and body posture in relation to voice handicap and voice quality in teachers with persistent voice complaints. Folia Phoniatr. Logop. 2005, 57, 134–147. [Google Scholar] [CrossRef]
- Rantala, L.; Sala, E.; Kankare, E. Teachers’ working postures and their effects on the voice. Folia Phoniatr. Logop. 2018, 70, 24–36. [Google Scholar] [CrossRef]
- Lowell, S.Y.; Kelley, R.T.; Colton, R.H.; Smith, P.B.; Portnoy, J.E. Position of the hyoid and larynx in people with muscle tension dysphonia. Laryngoscope 2012, 122, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Almeida, V.; Guimarães, F.; Moço, V.; Menezes, S.; Mafort, T.; Lopes, A. Correlation between pulmonary function, posture, and body composition in patients with asthma. Rev. Port. Pneumol. 2013, 19, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Menoncin, L.C.M.; Jurkiewicz, A.L.; Silvério, K.C.A.; Camargo, P.M.; Wolff, N.M.M. Alterações musculares e esqueléticas cervicais em mulheres disfônicas. Arq. Int. Otorrinolaringol. 2010, 14, 461–466. [Google Scholar] [CrossRef]
- Caçador, M.; Papoila, A.; Brás-Geraldes, C.; Garcia, C.S.; Constantino, T.; Almeida, M.; Stapleton-Garcia, P.; Paço, J. Evaluation of vocal changes after vestibular rehabilitation in patients with balance disorders. J. Vestib. Res. 2020, 30, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, M.; Bonilha, H.S. The Impact of Respiratory Exercises on Voice Outcomes: A Systematic Review of the Literature. J. Voice 2020, 34, 648.e1–648.e39. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Year | Patient (Number), (f), [m]; Age; Years of Employment | Aims | Outcomes | Treatment | Results |
|---|---|---|---|---|---|
| Randomized Controlled Trials | |||||
| Andriollo (2021) [36] | (56) 28 controls 21–60 years 5–18 years, aver. 9.1 | Study the changes after pompage in teachers with vocal complaints | PPT, audiometry, laryngoscopy, NDI, visual postural analysis, craniocervical frames | No | Improvement in NDI, craniocervical posture, and laryngoscopy. |
| Cardoso (2021) [37] | (18) [6] 12 controls 27–60 years No info | Study the effect of myofascial release on teachers’ posture and MTD | Frames, palpation of muscle tension, algometer, voice aerodynamic, acoustic-auditory perceptual voice | Myofascial release | Improvement in vertical alignment of the head, pelvis, scapula, and vocal parameters. |
| Marszalek (2012) [38] | (38) [2] 38–59 years No info | Assess the use of osteopathic procedures in the diagnosis and treatment of MTD | Laryngostroboscopy MPT calculation, VHI visual postural assessment performed by an osteopath | Osteopathic treatment and speech therapy | Improvement in head and neck position correlated with more improvement in VHI than in MPT. Hypertone at the sternocleidomastoid level of the geniohyoid and cricothyroid. |
| Cross-Sectional | |||||
| Cardoso (2020) [39] | (18) [6] 11 controls 27–60 years No info | Study the differences in posture, muscle tension, and voice | Postural assessment (photograms, palpation), aerodynamic, acoustic, and perceptual assessment of voice | No treatment | Teachers with voice disorders had greater hypertone of laryngeal and hyoid muscles. |
| Colla (2022) [40] | 57 21–60 years No info | Study the results of self-assessment of teachers with and without voice disorders | Videolaryngoscopic evaluation, Hearing screening, VAPP, V-RQOL, VHI, VoiSS, VTDS, HADS, URICA-VOICE, NMQ | Self-assessment results, reference parameters | There are higher values concerning voice impairment, musculoskeletal pain, and emotional disorders than the reference parameters. |
| Prospective Cohort | |||||
| Faralli (2017) [41] | (34) [3] 15–35 years | Examine postural control in MTD after a treatment based on speech rehabilitation | Romberg, laryngoscopy, laryngostroboscopy, VHI, acoustic voice analysis through CSLM and MDVP, postural analysis through SPeV, ECR, and ECO | Rehabilitation speech | Altered proprioceptive signals at the cervical level altered posture and voice, which in turn was altered by them. Speech rehabilitation led to improvement in subjective symptoms. |
| Qualitative | |||||
| Kooijman (2005) [42] | 25 No info | Study the relationship between body posture and voice disorders in teachers | VHI and DSI, Postural assessment, palpation of muscle tension | No treatment | Some postures predispose to voice disorders: posteriorly shifted weight, anterior protraction of the head, hypertonia of the sternocleidomastoid, and cricothyroid. |
| Controlled Clinical Trials | |||||
| Rantala (2018) [43] | (32) [8] 27–57 years Up to 10 years | Evaluate the associations between the voice and working postures of teachers | VEAW, VHI, and evaluation of the voice through recording it during a reading and one-day class | No treatment, posture correction | Teachers with greater vocal disorders tended to tilt their heads, rotate their torsos, and raise their arms when explaining the lesson. |
| Andriollo (2021) [36] | Cardoso (2021) [37] | Marszalek (2012) [38] | Cardoso (2020) [39] | Colla (2022) [40] | Faralli (2017) [41] | Kooijman (2005) [42] | Rantala (2018) [43] | |
|---|---|---|---|---|---|---|---|---|
| OUTCOME: VHI | ||||||||
| Mean value pre-intervention/treatment or baseline evaluation | X | X | Total: undeclared | X | Total: 22.07 ± 17.12 | Total: 42.77 ± 8.71 | Total: 72 | Physical subsection: 13.4 ± 5.72 |
| Mean value post-intervention/treatment | X | X | Total: lower of 19.6 | X | No intervention | Total: 26.72 ± 8.11 | No intervention | Physical subsection: 7.9 ± 5.32 |
| OUTCOME: Postural analysis without palpation | ||||||||
| Mean value pre-intervention/treatment | Evaluation with SAPO [37] HFE: 158.02 AP: 35.31 | Evaluation with SAPO [37] HAH: 2.29 HAASIS: 1.67 HAA: 1.66 HAP: −2.75 HAST3: −1.59 VAB: 1.25 VAHA: 2.54 | X | Evaluation with SAPO [37]. VCG: HAH: 1.78 ± 1.37 HAASIS:1.42 ± 1.13 HAA: 1.55 ± 1.28 HAP: −3.21 ± 5.50 HAST3:−1.34 ± 4.18 VAB: 1.20 ± 1.03 VAHA: 2.68 ± 2.15 | X | Postural analysis through SPeV [41] SEC: 410.73 SECR: 544.69 | X | X |
| Mean value post-intervention/treatment | HFE: 155.33 AP: 35.28 | HAH: 1.56 HAASIS: 1.63 HAA: 1.59 HAP: −2.66 HAST3: −1.60 VAB: 1.22 VAHA: 2.14 | X | WVCG: HAH: 1.17 ± 2.76 HAASIS:0.81 ± 2.30 HAA: 0.87 ± 2.30 HAP: −3.78 ± 4.26 HAST3: −1.83 ± 3.89 VAB: 0.45 ± 2.01 VAHA: 3.23 ± 3.74 | X | SEC: 333.15 SECR: 465.07 | X | X |
| Question | Andriollo, 2021 [36] | Cardoso, 2021 [37] | Faralli, 2017 [41] | Kooijman, 2005 [42] | Marszalek, 2012 [38] | Rantala, 2018 [43] |
|---|---|---|---|---|---|---|
| Are the characteristics of the patients in terms of gender, age, and average weight specified? | YES, not gender | YES, not gender | YES | YES, not gender | YES | YES |
| Is there a control group present? | YES | YES | NN | NN | NO | High |
| Are the operators and measurers blind? | YES | YES | NO | NN | NO | Mod |
| Are the descriptions of the treatments or any protocols done on the patients explained in a clear and illustrative manner? | YES | YES | YES | YES | YES | Mod |
| Are all outcomes listed and explained? | YES | YES | NO | YES | YES | High |
| How reproducible is it considering patient characteristics, outcomes, and interventions? | High | High | Mod | Mod | High | High |
| How high is the risk of bias considering the validity of the selected outcomes, the blindness of the operators, and the explanation of the interventions? | Low | Low | Low | Mod | Mod | Mod |
| Quality | High | High | Mod | Mod | Mod | Mod |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzone, R.; Petrigna, L.; Signorelli, D.; Musumeci, G. The Relationship between Posture and Muscle Tensive Dysphonia in Teachers: A Systematic Scoping Review. J. Funct. Morphol. Kinesiol. 2024, 9, 60. https://doi.org/10.3390/jfmk9020060
Franzone R, Petrigna L, Signorelli D, Musumeci G. The Relationship between Posture and Muscle Tensive Dysphonia in Teachers: A Systematic Scoping Review. Journal of Functional Morphology and Kinesiology. 2024; 9(2):60. https://doi.org/10.3390/jfmk9020060
Chicago/Turabian StyleFranzone, Roberta, Luca Petrigna, Daniele Signorelli, and Giuseppe Musumeci. 2024. "The Relationship between Posture and Muscle Tensive Dysphonia in Teachers: A Systematic Scoping Review" Journal of Functional Morphology and Kinesiology 9, no. 2: 60. https://doi.org/10.3390/jfmk9020060