
Assessment of the Relationship between Periodontitis and Cardiac Parameters in Patients with Early Chronic Heart Failure: A Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Periodontal Examination
2.4. Questionnaires
2.5. Blood Sampling
2.6. Echocardiography
2.7. Incremental Test
2.8. Statistics
3. Results
3.1. Summary of Findings
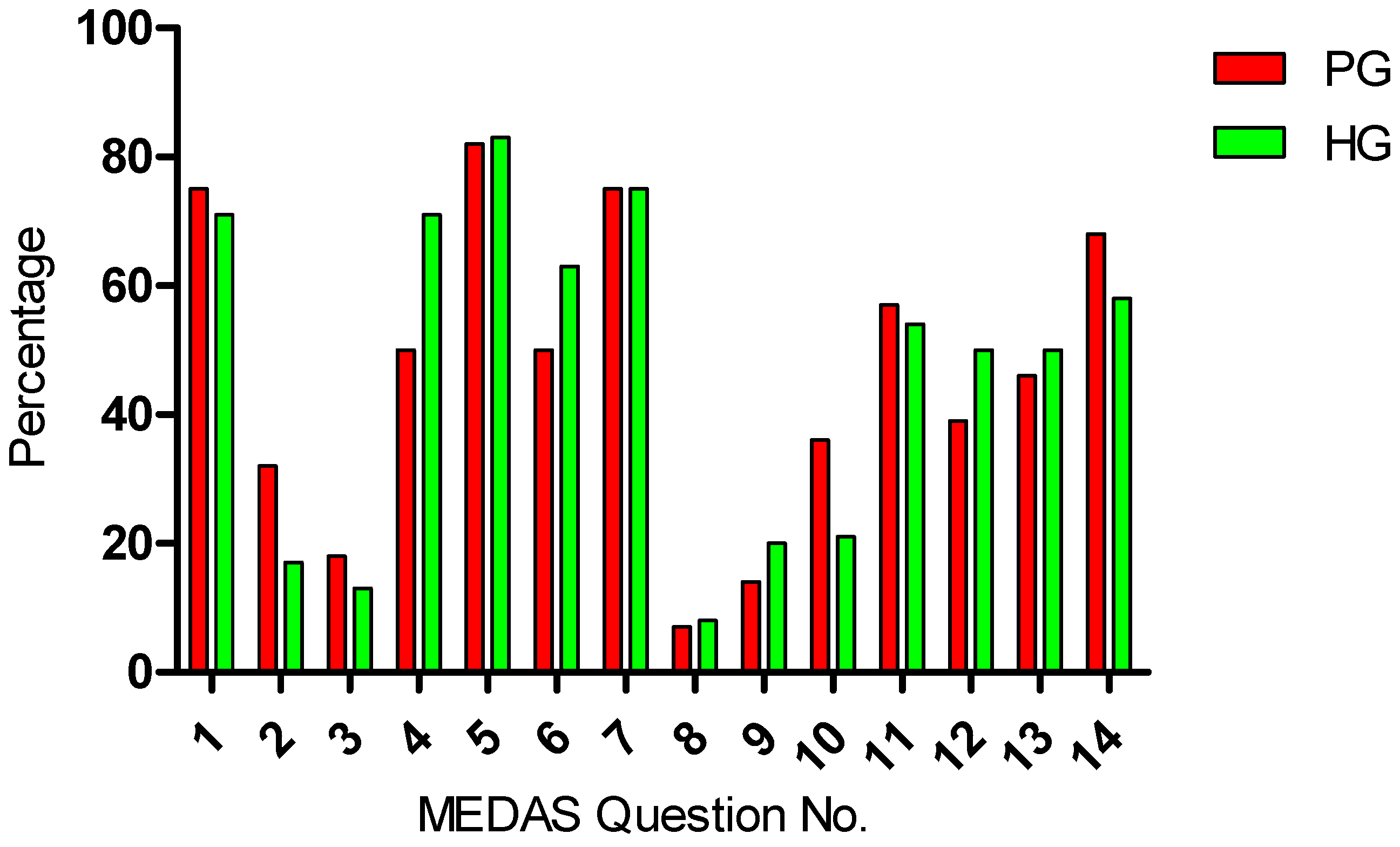
3.2. MEDAS
3.3. OHIP-14 and PHQ
3.4. Correlation Analysis
4. Discussion
4.1. Inflammatory Parameters
4.2. PSR and BMI
4.3. MEDAS
4.4. OHIP-14 and Modified PHQ-9
4.5. Cardiocirculatory Parameters
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mann, D.L. Inflammatory mediators and the failing heart: Past, present, and the foreseeable future. Circ. Res. 2002, 91, 988–998. [Google Scholar] [CrossRef]
- Fröhlich, H.; Herrmann, K.; Franke, J.; Karimi, A.; Täger, T.; Cebola, R.; Katus, H.A.; Zugck, C.; Frankenstein, L.; Fröhlich, H.; et al. Periodontitis in chronic heart failure. Tex. Heart Inst. J. 2016, 43, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Diabetes, heart failure, and renal dysfunction: The vicious circles. Prog. Cardiovasc. Dis. 2019, 62, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Schütt, K.; Aberle, J.; Bauersachs, J.; Birkenfeld, A.; Frantz, S.; Ganz, M.; Jacob, S.; Kellerer, M.; Leschke, M.; Liebetrau, C.; et al. Positionspapier Herzinsuffizienz und Diabetes. Diabetol. Stoffwechs. 2022, 17, 277–288. [Google Scholar]
- Kim, M.; Kim, H.L.; Lim, W.H.; Seo, J.B.; Kim, S.H.; Kim, M.A.; Zo, J.H. Association between arterial stiffness and left ventricular diastolic function: A large population-based cross-sectional study. Front. Cardiovasc. Med. 2022, 9, 1001248. [Google Scholar] [CrossRef]
- Roman, M.J.; Ganau, A.; Saba, P.S.; Pini, R.; Pickering, T.G.; Devereux, R.B. Impact of arterial stiffening on left ventricular structure. Hypertension 2000, 36, 489–494. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Athilingam, P.; D’Aust, R.; Zambroski, C.; McMillan, S.C.; Sahebzemani, F. Predictive validity of NYHA and ACC/AHA Classifications. Int. J. Nurs. Sci. 2013, 3, 22–32. [Google Scholar]
- Jankowska, E.A.; Jakubaszko, J.; Cwynar, A.; Majda, J.; Ponikowska, B.; Kustrzycka-Kratochwil, D.; Reczuch, K.; Borodulin-Nadzieja, L.; Banasiak, W.; Poole-Wilson, P.A.; et al. Bone mineral status and bone loss over time in men with chronic systolic heart failure and their clinical and hormonal determinants. Eur. J. Heart Fail. 2009, 11, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Kato, T.S.; Pronschinske, K.; Qiu, S.; Naka, Y.; Takayama, H.; Schulze-Späte, U.; Cremers, S.; Shane, E.; Mancini, D.; et al. Dynamics of bone turnover markers in patients with heart failure and following haemodynamic improvement through ventricular assist device implantation. Eur. J. Heart Fail. 2012, 14, 1356–1365. [Google Scholar] [CrossRef]
- Roth, G.A.; Forouzanfar, M.H.; Moran, A.E.; Barber, R.; Nguyen, G.; Feigin, V.L.; Naghavi, M.; Mensah, G.A.; Murray, C.J. Demographic and epidemiologic drivers of global cardiovascular mortality. N. Engl. J. Med. 2015, 372, 1333–1341. [Google Scholar] [CrossRef] [PubMed]
- Benigeri, M.; Brodeur, J.M.; Payette, M.; Charbonneau, A.; Ismail, A.I. Community periodontal index of treatment needs and prevalence of periodontal conditions. J. Clin. Periodontol. 2000, 27, 308–312. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Sanz, M.; Marco del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Page, R.C.; Krall, E.A.; Martin, J.; Mancl, L.; Garcia, R.I. Validity and accuracy of a risk calculator in predicting periodontal disease. J. Am. Dent. Assoc. 2002, 133, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef] [PubMed]
- Boyapati, R.; Vudathaneni, V.; Nadella, S.B.; Ramachandran, R.; Dhulipalla, R.; Adurty, C. Mapping the link between cardiac biomarkers and chronic periodontitis: A clinico-biochemical study. J. Indian Soc. Periodontol. 2020, 24, 309–315. [Google Scholar] [CrossRef]
- Williams, R.C.; Offenbacher, S. Periodontal medicine: The emergence of a new branch of periodontology. Periodontology 2000 2000, 23, 9–12. [Google Scholar] [CrossRef]
- Genco, R.; Offenbacher, S.; Beck, J. Periodontal disease and cardiovascular disease: Epidemiology and possible mechanisms. J. Am. Dent. Assoc. 2002, 133, 14S–22S. [Google Scholar] [CrossRef]
- Reynolds, M.A. Modifiable risk factors in periodontitis: At the intersection of aging and disease. Periodontology 2000 2014, 64, 7–19. [Google Scholar] [CrossRef]
- Wood, N.; Johnson, R.B. The relationship between tomato intake and congestive heart failure risk in periodontitis subjects. J. Clin. Periodontol. 2004, 31, 574–580. [Google Scholar] [CrossRef]
- Schulze-Späte, U.; Mizani, I.; Salaverry, K.R.; Chang, J.; Wu, C.; Jones, M.; Kennel, P.J.; Brunjes, D.L.; Choo, T.-H.; Kato, T.S.; et al. Periodontitis and bone metabolism in patients with advanced heart failure and after heart transplantation. ESC Heart Fail. 2017, 4, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Woo, H.G.; Park, J.; Lee, J.S.; Song, T.J. Improved oral hygiene care is associated with decreased risk of occurrence for atrial fibrillation and heart failure: A nationwide population-based cohort study. Eur. J. Prev. Cardiol. 2020, 27, 1835–1845. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Van Dyke, T.E.; Working Group 1 of the Joint EFP/AAP Workshop. Periodontitis and atherosclerotic cardiovascular disease: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Schenkein, H.A.; Loos, B.G. Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J. Periodontol. 2013, 84, 51–69. [Google Scholar] [CrossRef] [PubMed]
- Jockel-Schneider, Y.; Harks, I.; Haubitz, I.; Fickl, S.; Eigenthaler, M.; Schlagenhauf, U.; Baulmann, J. Arterial stiffness and pulse wave reflection are increased in patients suffering from severe periodontitis. PLoS ONE 2014, 9, e103449. [Google Scholar] [CrossRef] [PubMed]
- Masugata, H.; Senda, S.; Hoshikawa, J.; Murao, K.; Hosomi, N.; Okuyama, H.; Inukai, M.; Himoto, T.; Nakatsuka, Y.; Imai, M.; et al. Elevated brachial-ankle pulse wave velocity is associated with left ventricular hypertrophy in hypertensive patients after stroke. Tohoku J. Exp. Med. 2010, 220, 177–182. [Google Scholar] [CrossRef]
- Rabkin, S.W.; Chan, S.H. Correlation of pulse wave velocity with left ventricular mass in patients with hypertension once blood pressure has been normalized. Heart Int. 2012, 7, e5. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Mikhailidis, D.P.; Rizzo, M.; von Haehling, S.; Rysz, J.; Banach, M. The influence of atorvastatin on parameters of inflammation left ventricular function, hospitalizations and mortality in patients with dilated cardiomyopathy—5-year follow-up. Lipids Health Dis. 2013, 12, 47. [Google Scholar] [CrossRef]
- Angeli, F.; Verdecchia, P.; Pellegrino, C.; Pellegrino, R.G.; Pellegrino, G.; Prosciutti, L.; Giannoni, C.; Cianetti, S.; Bentivoglio, M. Association between periodontal disease and left ventricle mass in essential hypertension. Hypertension 2003, 41, 488–492. [Google Scholar] [CrossRef]
- Franek, E.; Klamczynska, E.; Ganowicz, E.; Blach, A.; Budlewski, T.; Gorska, R. Association of chronic periodontitis with left ventricular mass and central blood pressure in treated patients with essential hypertension. Am. J. Hypertens. 2009, 22, 203–207. [Google Scholar] [CrossRef]
- Franek, E.; Napora, M.; Blach, A.; Budlewski, T.; Gozdowski, D.; Jedynasty, K.; Krajewski, J.; Gorska, R. Blood pressure and left ventricular mass in subjects with type 2 diabetes and gingivitis or chronic periodontitis. J. Clin. Periodontol. 2010, 37, 875–880. [Google Scholar] [CrossRef]
- Aoyama, N.; Kure, K.; Minabe, M.; Izumi, Y. increased heart failure prevalence in patients with a high antibody level against periodontal pathogen. Int. Heart J. 2019, 60, 1142–1146. [Google Scholar] [CrossRef]
- Elin, R.J.; Winter, W.E. Laboratory and clinical aspects of B-type natriuretic peptides. Arch. Pathol. Lab. Med. 2004, 128, 697–699. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association Classes of Heart Failure. 2017. Available online: https://www.heart.org/en/health-topics/heart-failure/what-is-heart-failure/classes-of-heart-failure (accessed on 7 November 2022).
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [PubMed]
- Russell, S.D.; Saval, M.A.; Robbins, J.L.; Ellestad, M.H.; Gottlieb, S.S.; Handberg, E.M.; Zhou, Y.; Chandler, B.; HF-ACTION Investigators. New York Heart Association functional class predicts exercise parameters in the current era. Am. Heart J. 2009, 158, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Bruno, E.; Manoukian, S.; Venturelli, E.; Oliverio, A.; Rovera, F.; Iula, G.; Morelli, D.; Peissel, B.; Azzolini, J.; Roveda, E.; et al. Adherence to Mediterranean Diet and Metabolic Syndrome in BRCA Mutation Carriers. Integr. Cancer Ther. 2018, 17, 153–160. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- John, M.T.; Patrick, D.L.; Slade, G.D. The German version of the Oral Health Impact Profile—Translation and psychometric properties. Eur. J. Oral Sci. 2002, 110, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D. Derivation and validation of a short-form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Chand, S.; Joseph, K.; Sankaranarayanan, A.; Issac, A.; Babu, G.; Wilson, B.; Joseph, J. Evaluation of C-Reactive Protein and Fibrinogen in Patients with Chronic and Aggressive Periodontitis: A Clinico-Biochemical Study. J. Clin. Diagn. Res. 2017, 11, ZC41–ZC45. [Google Scholar] [CrossRef]
- Al-Zahrani, M.S.; Bissada, N.F.; Borawskit, E.A. Obesity and periodontal disease in young, middle-aged, and older adults. J. Periodontol. 2003, 74, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Filho, I.S.; Fritas Coelho, J.M.; da Cruz, S.S.; Passos, J.S.; Teixeira de Freitas, C.O.; Aragão Farias, N.S.; Amorim da Silva, R.; Silva Pereira, M.N.; Lima, T.L.; Barreto, M.L. Chronic periodontitis and C-reactive protein levels. J. Periodontol. 2011, 82, 969–978. [Google Scholar] [CrossRef]
- Gani, D.K.; Lakshmi, D.; Krishnan, R.; Emmadi, P. Evaluation of C-reactive protein and interleukin-6 in the peripheral blood of patients with chronic periodontitis. J. Indian Soc. Periodontol. 2009, 13, 69–74. [Google Scholar] [CrossRef]
- Rai, B.; Kaur, J.; Anand, S.C. Possible relationship between periodontitis and dementia in a North Indian old age population: A pilot study. Gerodontology 2012, 29, e200–e205. [Google Scholar] [CrossRef]
- Pussinen, P.J.; Tuomisto, K.; Jousilahti, P.; Havulinna, A.S.; Sundvall, J.; Salomaa, V. Endo-toxemia, immune response to periodontal pathogens, and systemic inflammation associate with incident cardiovascular disease events. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1433–1439. [Google Scholar] [CrossRef]
- Molinsky, R.L.; Yuzefpolskaya, M.; Norby, F.L.; Yu, B.; Shah, A.M.; Pankow, J.S.; Ndumele, C.E.; Lutsey, P.L.; Papapanou, P.N.; Beck, J.D.; et al. Periodontal Status, C-Reactive Protein, NT-proBNP, and Incident Heart Failure: The ARIC Study. JACC Heart Fail. 2022, 10, 731–741. [Google Scholar] [CrossRef]
- Wu, C.-K.; Lee, J.-K.; Chiang, F.-T.M.; Yang, C.-H.; Huang, S.-W.B.; Hwang, J.-J.; Lin, J.-L.; Tseng, C.-D.; Chen, J.-J.; Tsai, C.-T. Plasma levels of tumor necrosis factor-alpha and interleukin-6 are associated with diastolic heart failure through downregulation of sarcoplasmic reticulum Ca2+ ATPase. Crit. Care Med. 2011, 39, 984–992. [Google Scholar] [CrossRef]
- Savvatis, K.; Müller, I.; Fröhlich, M.; Pappritz, K.; Zietsch, C.; Hamdani, N.; Grote, K.; Schieffer, B.; Klingel, K.; Van Linthout, S.; et al. Interleukin-6 receptor inhibition modulates the immune reaction and restores titin phosphorylation in experimental myocarditis. Basic Res. Cardiol. 2014, 109, 449. [Google Scholar] [CrossRef] [PubMed]
- Cainzos-Achirica, M.; Enjuanes, C.; Greenland, P.; McEvoy, J.W.; Cushman, M.; Dardari, Z.; Nasir, K.; Budoff, M.J.; Al-Mallah, M.H.; Yeboah, J.; et al. The prognostic value of interleukin 6 in multiple chronic diseases and all-cause death: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2018, 278, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Duprez, D.A.; Gross, M.D.; Kizer, J.R.; Ix, J.H.; Hundley, W.G.; Jacobs, D.R., Jr. Predictive Value of Collagen Biomarkers for Heart Failure With and Without Preserved Ejection Fraction: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Heart Assoc. 2018, 7, 5. [Google Scholar] [CrossRef]
- Vasan, R.S.; Sullivan, L.M.; Roubenoff, R.; Dinarello, C.A.; Harris, T.; Benjamin, E.J.; Sawyer, D.B.; Levy, D.; Wilson, P.W.; D’Agostino, R.B. Inflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: The Framingham Heart Study. Circulation 2003, 107, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Jug, B.; Salobir, B.G.; Vene, N.; Sebestjen, M.; Sabovic, M.; Keber, I. Interleukin-6 is a stronger prognostic predictor than high-sensitive C-reactive protein in patients with chronic stable heart failure. Heart Vessel. 2009, 24, 271–276. [Google Scholar] [CrossRef]
- Geenen, L.W.; Baggen, V.J.; van den Bosch, A.E.; Eindhoven, J.A.; Kauling, R.M.; Cuypers, J.A.; Roos-Hesselink, J.W.; Boersma, E. Prognostic value of C-reactive protein in adults with congenital heart disease. Heart 2020, 107, 474–481. [Google Scholar] [CrossRef]
- Yan, A.T.; Yan, R.T.; Cushman, M.; Redheuil, A.; Tracy, R.P.; Arnett, D.K.; Rosen, B.D.; McClelland, R.L.; Bluemke, D.A.; Lima, J.A. Relationship of interleukin-6 with regional and global left-ventricular function in asymptomatic individuals without clinical cardiovascular disease: Insights from the Multi-Ethnic Study of Atherosclerosis. Eur. Heart J. 2010, 7, 875–882. [Google Scholar] [CrossRef]
- Markousis-Mavrogenis, G.; Tromp, J.; Ouwerkerk, W.; Devalaraja, M.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; Filippatos, G.S.; van der Harst, P.; Lang, C.C.; et al. The clinical significance of interleukin-6 in heart failure: Results from the BIOSTAT-CHF study. Eur. J. Heart Fail. 2019, 8, 965–973. [Google Scholar] [CrossRef]
- Johns, I.; Moschonas, K.E.; Medina, J.; Ossei-Gerning, N.; Kassianos, G.; Halcox, J.P. Risk classification in primary prevention of CVD according to QRISK2 and JBS3 ‘heart age’, and prevalence of elevated high-sensitivity C reactive protein in the UK cohort of the EURIKA study. Open Heart 2018, 5, e000849. [Google Scholar] [CrossRef]
- Lee, Y.; McKechnie, T.; Doumouras, A.G.; Handler, C.; Eskicioglu, C.; Gmora, S.; Anvari, M.; Hong, D. Diagnostic Value of C-Reactive Protein Levels in Postoperative Infectious Complications After Bariatric Surgery: A Systematic Review and Meta-Analysis. Obes. Surg. 2019, 29, 2022–2029. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.M.; Lee, S.; Hwang, W.; Son, E.; Kim, T.W.; Kim, K.; Kim, Y.H. Obesity and periodontitis: A systematic review and updated meta-analysis. Front Endocrinol. 2022, 13, 999455. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Li, J.; Cochran, D.L. Inflammation and uncoupling as mechanisms of periodontal bone loss. J. Dent. Res. 2011, 90, 143–153. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation, Geneva, 8–11 December 2008. Available online: https://apps.who.int/iris/handle/10665/44583 (accessed on 3 July 2019).
- Arboleda, S.; Vargas, M.; Losada, S.; Pinto, A. Review of obesity and periodontitis: An epidemiological view. Br. Dent. J. 2019, 227, 235–239. [Google Scholar] [CrossRef]
- Khader, Y.S.; Bawadi, H.A.; Haroun, T.F.; Alomari, M.; Tayyem, R.F. The association between periodontal disease and obesity among adults in Jordan. J. Clin. Periodontol. 2009, 36, 18–24. [Google Scholar] [CrossRef]
- Saito, T.; Shimazaki, Y.; Sakamoto, M. Obesity and periodontitis. N. Engl. J. Med. 1998, 339, 482–483. [Google Scholar] [CrossRef]
- Hlatky, M.A.; Chung, S.C.; Escobedo, J.; Hillegass, W.B.; Melsop, K.; Rogers, W.; Brooks, M.M.; BARI 2D Study Group. The effect of obesity on quality of life in patients with diabetes and coronary artery disease. Am. Heart J. 2010, 159, 292–300. [Google Scholar] [CrossRef]
- Zorena, K.; Jachimowicz-Duda, O.; Ślęzak, D.; Robakowska, M.; Mrugacz, M. Adipokines and Obesity. Potential Link to Metabolic Disorders and Chronic Complications. Int. J. Mol. Sci. 2020, 21, 3570. [Google Scholar] [CrossRef]
- Graziani, F.; Gennai, S.; Solini, A.; Petrini, M. A systematic review and meta-analysis of epidemiologic observational evidence on the effect of periodontitis on diabetes An update of the EFP-AAP review. J. Clin. Periodont. 2018, 45, 167–187. [Google Scholar] [CrossRef]
- Huertas, J.R.; Battino, M.; Lenaz, G.; Mataix, F.J. Changes in mitochondrial and microsomal rat liver coenzyme Q9 and Q10 content induced by dietary fat and endogenous lipid peroxidation. FEBS Lett. 1991, 287, 89–92. [Google Scholar] [CrossRef]
- Ochoa-Herrera, J.J.; Huertas, J.R.; Quiles, J.L.; Mataix, J. Dietary oils high in oleic acid, but with different non-glyceride contents, have different effects on lipid profiles and peroxidation in rabbit hepatic mitochondria. J. Nutr. Biochem. 2001, 12, 357–364. [Google Scholar] [CrossRef]
- Lobb, K.; Chow, C.K. Fatty acid classification and nomenclature. In Fatty Acids in Foods and Their Health Implications; Chow, C.K., Ed.; CRC Press: Boca Raton, FL, USA, 2008; pp. 1–15. [Google Scholar]
- Calder, P.C. n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am. J. Clin. Nutr. 2006, 83, 1505S–1519S. [Google Scholar] [CrossRef]
- Bullon, P.; Morillo, J.M.; Ramirez-Tortosa, M.C.; Quiles, J.L.; Newman, H.N.; Battino, M. Metabolic syndrome and periodontitis: Is oxidative stress a common link? J. Dent. Res. 2009, 88, 503–518. [Google Scholar] [CrossRef] [PubMed]
- Varela-López, A.; Giampieri, F.; Bullón, P.; Battino, M.; Quiles, J.L. Role of Lipids in the Onset, Progression and Treatment of Periodontal Disease. A Systematic Review of Studies in Humans. Int. J. Mol. Sci. 2016, 17, 1202. [Google Scholar] [CrossRef] [PubMed]
- El-Sharkawy, H.; Aboelsaad, N.; Eliwa, M.; Darweesh, M.; Alshahat, M.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Adjunctive treatment of chronic periodontitis with daily dietary supplementation with omega-3 Fatty acids and low-dose aspirin. J. Periodontol. 2010, 81, 1635–1643. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P.; Lingström, P. Nutrition, dental caries and periodontal disease: A narrative review. J. Clin. Periodontol. 2017, 44, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Ferrazzano, G.F.; Amato, I.; Ingenito, A.; Zarrelli, A.; Pinto, G.; Pollio, A. Plant polyphenols and their anti-cariogenic properties: A review. Molecules 2011, 16, 1486–1507. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Murata, R.M.; Duarte, S. Antimicrobial traits of tea- and cranberry-derived polyphenols against Streptococcus mutans. Caries Res. 2011, 45, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Milward, M.; Chapple, I. The role of diet in periodontal disease. Clin. Dent. Health 2013, 52, 18–21. [Google Scholar]
- Dodington, D.W.; Fritz, P.C.; Sullivan, P.J.; Ward, W.E. Higher Intakes of Fruits and Vegetables, β-Carotene, Vitamin C, α-Tocopherol, EPA, and DHA Are Positively Associated with Periodontal Healing after Nonsurgical Periodontal Therapy in Nonsmokers but Not in Smokers. J. Nutr. 2015, 145, 2512–2519. [Google Scholar] [CrossRef]
- Ritchie, C.S.; Kinane, D.F. Nutrition, inflammation, and periodontal disease. Nutrition 2003, 19, 475–476. [Google Scholar] [CrossRef]
- Neiva, R.F.; Al-Shammari, K.; Nociti, F.H., Jr.; Soehren, S.; Wang, H.L. Effects of vitamin-B complex supplementation on periodontal wound healing. J. Periodontol. 2005, 76, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Zong, G.; Holtfreter, B.; Scott, A.E.; Völzke, H.; Petersmann, A.; Dietrich, T.; Newson, R.S.; Kocher, T. Serum vitamin B12 is inversely associated with periodontal progression and risk of tooth loss: A prospective cohort study. J. Clin. Periodontol. 2016, 43, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Boyd, L. Nutrition and the periodontium. In Diet and Nutrition in Oral Health, 2nd ed.; Palmer, C.A., Friedman, G.J., Friedman, D.R., Eds.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2007. [Google Scholar]
- Boyd, L.; Palmer, C. Nutrition and oral health. In Complete Review of Dental Hygiene; Brian, J.N., Cooper, M.D., Eds.; Prentice-Hall: Upper Saddle River, NJ, USA, 2001. [Google Scholar]
- Lingström, P.; Moynihan, P. Nutrition, saliva, and oral health. Nutrition 2003, 19, 567–569. [Google Scholar] [CrossRef]
- Marton, I.J.; Balla, G.; Hegedus, C.; Redi, P.; Szilagyi, Z.; Karmazsin, L.; Kiss, C. The role of reactive oxygen intermediates in the pathogenesis of chronic apical periodontitis. Oral Microbiol. Immunol. 1993, 8, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Manz, M.C.; Taylor, G.W.; Yoshihara, A.; Miyazaki, H. Relations of serum ascorbic acid and α-tocopherol to periodontal disease. J. Dent. Res. 2012, 91, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Muniz, F.W.; Nogueira, S.B.; Mendes, F.L.; Rösing, C.K.; Moreira, M.M.; de Andrade, G.M.; Carvalho, R.S. The impact of antioxidant agents complimentary to periodontal therapy on oxidative stress and periodontal outcomes: A systematic review. Arch. Oral Biol. 2015, 60, 1203–1214. [Google Scholar] [CrossRef]
- Ferenchick, E.K.; Ramanuj, P.; Pincus, H.A. Depression in primary care: Part 1—screening and diagnosis. BMJ 2019, 365, l794. [Google Scholar] [CrossRef] [PubMed]
- Alkan, A.; Cakmak, O.; Yilmaz, S.; Cebi, T.; Gurgan, C. Relationship Between Psychological Factors and Oral Health Status and Behaviours. Oral Health Prev. Dent. 2015, 13, 331–339. [Google Scholar]
- Jardim, L.C.; Flores, P.T.; do Carmo Dos Santos Araújo, M.; Chiesa, J.; de Moraes, C.M.B.; Antoniazzi, R.P. Oral health-related quality of life in breast cancer survivors. Support Care Cancer 2020, 28, 65–71. [Google Scholar] [CrossRef]
- Ochs, M.M.; Fritz, T.; André, F.; Riffel, J.; Mereles, D.; Müller-Hennessen, M.; Giannitsis, E.; Katus, H.A.; Friedrich, M.G.; Buss, S.J. A comprehensive analysis of cardiac valve plane displacement in healthy adults: Age-stratified normal values by cardiac magnetic resonance. Int. J. Cardiovasc. Imaging 2017, 33, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Mao, M.; Li, Y.Q.; Chen, Y.J.; Yu, H.D.; Xie, W.Z.; Huang, Q.; Leng, W.D.; Xiong, J. Periodontitis Is Associated With Heart Failure: A Population-Based Study (NHANES III). Front. Physiol. 2022, 13, 854606. [Google Scholar] [CrossRef] [PubMed]
- Walther, C.; Wenzel, J.; Schnabel, R.B.; Heydecke, G.; Seedorf, U.; Beikler, T.; Borof, K.; Nikorowitsch, J.; Schrage, B.; Blankenberg, S.; et al. Association between periodontitis and heart failure in the general population. ESC Heart Fail. 2022, 9, 4189–4197. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Questions | Criteria for 1 Point |
|---|---|
| 1. Do you use olive oil as a main culinary fat? | Yes |
| 2. How much olive oil do you consume in a given day (including oil used for frying, salads, out-of-house meals, etc.)? | ≥4 tablespoons |
| 3. How many vegetable servings do you consume per day? (1 serving = 80 g) | ≥5 or ≥3 portions of raw vegetables or salad |
| 4. How many fruit units (including natural fruit juices) do you consume per day? | ≥3 |
| 5. How many servings of red meat, hamburger, or meat products (ham, sausage, etc.) do you consume per day? (1 serving = 100–150 g) | <1 |
| 6. How many servings of butter, margarine, or cream do you consume per day? (1 serving = 12 g/1 tablespoon) | <1 |
| 7. How many sweet or carbonated beverages do you drink per day? | <1 |
| 8. How many glasses of wine do you drink per week? | ≥10 glasses (0.25 L = 1 glass) |
| 9. How many servings of legumes do you consume per week? (1 serving = 150 g) | ≥3 |
| 10. How many servings of fish or shellfish do you consume per week? (1 serving = 100–150 g of fish or 200 g of shellfish) | ≥3 |
| 11. How many times per week do you consume commercial sweets or pastries (not homemade), such as cakes, cookies, biscuits, or custard? | <3 |
| 12. How many servings of nuts (including peanuts) do you consume per week? (1 serving = 30 g) | ≥3 |
| 13. Do you preferentially consume chicken, turkey, or rabbit meat instead of veal, pork, hamburger, or sausage? | Yes |
| 14. How many times per week do you consume vegetables, pasta, rice, or other dishes seasoned with sofrito (sauce made with tomato and onion, leek, or garlic and simmered with olive oil)? | ≥2 |
| Parameter | Reference | PG n = 29 | NPG n = 29 | p-Value |
|---|---|---|---|---|
| Age [years] | 70.69 (6.6) | 63.21 (10.4) | <0.004 | |
| Height [cm] | 171.5 (8.3) | 173.4 (10.6) | n.s. | |
| Weight [kg] | 82.2 (15.1) | 78.4 (15.6) | n.s. | |
| BMI [kg/m2] | 27.8 (3.9) | 26.0 (4.3) | n.s. | |
| WC [cm] | 100.1 (14.0) | 92.6 (13.5) | n.s. | |
| Number of teeth | 23.7 (6.3) | 25.1 (4.1) | n.s. | |
| Mean PSR | 3.2 (0.7) | 0.3 (0.3) | <0.0001 | |
| NT-proBNP [pg/mL] | <125 | 642 (807) | 341 (256) | <0.023 |
| hsTropT [pg/mL] | <14 | 11.7 (5.0) | 7.1 (4.7) | <0.001 |
| CRP [mg/L] | Low < 1 Moderate 1–3 High > 3 | 2.1 (2.1) | 2.1 (2.3) | n.s. |
| IL-6 [pg/mL] | <7 | 3.8 (2.4) | 3.5 (2.2) | n.s. |
| HbA1c [%] | <6.5 | 5.9 (1.0) | 5.6 (0.5) | n.s. |
| Leukocytes [104/µL] | 3.5–9.8 | 6.4 (2.1) | 6.1 (1.5) | n.s. |
| Total cholesterol [mmol/L] | <5.2 | 4.66 (1.1) | 4.66 (1.38) | n.s. |
| Triglyceride [mmol/L] | <1.7 | 1.19 (0.44) | 1.28 (0.60) | n.s. |
| LDL [mmol/L] | <4.2 | 2.86 (0.85) | 2.80 (1.12) | n.s. |
| HDL [mmol/L] | >1.03 | 1.19 (0.44) | 1.28 (0.60) | n.s. |
| EFbip [%] | >51 | 48.42 (9.17) | 53.38 (6.39) | <0.022 |
| E/A | >1.1 | 0.88 (0.24) | 1.07 (0.33) | <0.040 |
| E/e’ | <14 | 10.13 (4.49) | 9.04 (3.47) | n.s. |
| TAPSE [cm] | ≥1.6 | 2.00 (0.37) | 2.10 (0.34) | n.s. |
| MAPSElat [cm] | ≥1.4 | 1.17 (0.23) | 1.34 (0.19) | <0.005 |
| SBP [mmHg] | 143.3 (14.5) | 138.7 (15.6) | n.s. | |
| DBP [mmHg] | 84.0 (9.5) | 84.6 (8.1) | n.s. | |
| SBP ET [mmHg] | 202.2 (30.4) | 194.4 (28.3) | n.s. | |
| DBP ET [mmHg] | 92.0 (11.3) | 91.6 (11.2) | n.s. | |
| HR ET [bpm] | 133.8 (18.9) | 141.7 (23.2) | n.s. | |
| % reference HRmax [bpm] | 89.2 (13.4) | 90.1 (14.6) | n.s. | |
| Pmax [Watt] | 111.7 (37.8) | 117.9 (50.9) | n.s. | |
| % reference Pmax [Watt] | 82.0 (27.0) | 85.4 (31.7) | n.s. | |
| RPPmax [mmHg × bpm × 100−1] | 268.85 (61.97) | 274.11 (67.03) | n.s. | |
| RPP/Watt [mmHg × bpm × 100−1 × Pmax-1] | 2.50 (0.72) | 2.52 (0.76) | n.s. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulze, A.; Kwast, S.; Pökel, C.; Busse, M. Assessment of the Relationship between Periodontitis and Cardiac Parameters in Patients with Early Chronic Heart Failure: A Cross-Sectional Study. J. Funct. Morphol. Kinesiol. 2024, 9, 52. https://doi.org/10.3390/jfmk9010052
Schulze A, Kwast S, Pökel C, Busse M. Assessment of the Relationship between Periodontitis and Cardiac Parameters in Patients with Early Chronic Heart Failure: A Cross-Sectional Study. Journal of Functional Morphology and Kinesiology. 2024; 9(1):52. https://doi.org/10.3390/jfmk9010052
Chicago/Turabian StyleSchulze, Antina, Stefan Kwast, Christoph Pökel, and Martin Busse. 2024. "Assessment of the Relationship between Periodontitis and Cardiac Parameters in Patients with Early Chronic Heart Failure: A Cross-Sectional Study" Journal of Functional Morphology and Kinesiology 9, no. 1: 52. https://doi.org/10.3390/jfmk9010052