
An Overview of Physical Exercise Program Protocols and Effects on the Physical Function in Multiple Sclerosis: An Umbrella Review

 , ,
, ,  , , and
, , and 
Abstract
:
1. Introduction
2. Materials and Methods
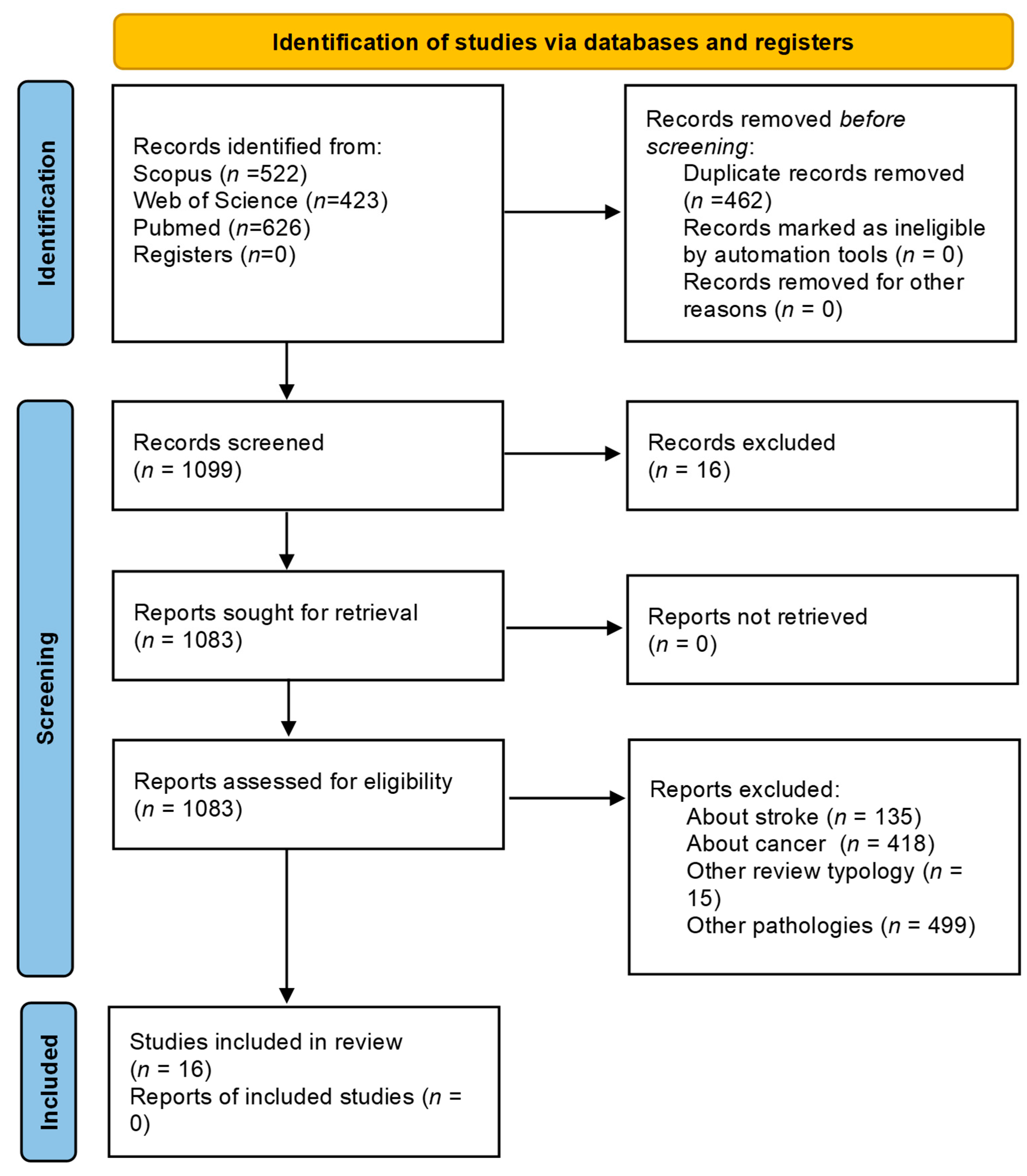
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Sources, Study Sections, and Data Extraction
2.4. Quality Assessment
3. Results
3.1. Characteristics of the Included Studies
3.2. Characteristics of the Interventions
3.3. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Doshi, A.; Chataway, J. Multiple sclerosis, a treatable disease. Clin. Med. 2016, 16 (Suppl. S6), s53–s59. [Google Scholar] [CrossRef]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; Van Der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Correale, J.; Gaitán, M.I.; Ysrraelit, M.C.; Fiol, M.P. Progressive multiple sclerosis: From pathogenic mechanisms to treatment. Brain 2017, 140, 527–546. [Google Scholar] [CrossRef]
- Kuhlmann, T.; Moccia, M.; Coetzee, T.; Cohen, J.A.; Correale, J.; Graves, J.; Marrie, R.A.; Montalban, X.; Yong, V.W.; Thompson, A.J.; et al. Multiple sclerosis progression: Time for a new mechanism-driven framework. Lancet Neurol. 2023, 22, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Cree, B.A.C. Treatment of multiple sclerosis: A review. Am. J. Med. 2020, 133, 1380–1390.e2. [Google Scholar] [CrossRef]
- Zhang, Y.; Taylor, B.V.; Simpson, S.; Blizzard, L.; Campbell, J.A.; Palmer, A.J.; van der Mei, I. Feelings of depression, pain and walking difficulties have the largest impact on the quality of life of people with multiple sclerosis, irrespective of clinical phenotype. Mult. Scler. J. 2021, 27, 1262–1275. [Google Scholar] [CrossRef]
- Rooney, S.; Wood, L.; Moffat, F.; Paul, L. Prevalence of fatigue and its association with clinical features in progressive and non-progressive forms of Multiple Sclerosis. Mult. Scler. Relat. Disord. 2019, 28, 276–282. [Google Scholar] [CrossRef]
- Bakshi, R. Fatigue associated with multiple sclerosis: Diagnosis, impact and management. Mult. Scler. J. 2003, 9, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Green, R.; Cutter, G.; Friendly, M.; Kister, I. Which symptoms contribute the most to patients’ perception of health in multiple sclerosis? Mult. Scler. J. Exp. Transl. Clin. 2017, 3, 2055217317728301. [Google Scholar] [CrossRef]
- 13. Weld-Blundell, I.V.; Grech, L.; Learmonth, Y.C.; Marck, C.H. Lifestyle and complementary therapies in multiple sclerosis guidelines: Systematic review. Acta Neurol. Scand. 2022, 145, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Bowser, B.; O’Rourke, S.; Brown, C.N.; White, L.; Simpson, K.J. Sit-to-stand biomechanics of individuals with multiple sclerosis. Clin. Biomech. 2015, 30, 788–794. [Google Scholar] [CrossRef]
- Thoumie, P.; Lamotte, D.; Cantalloube, S.; Faucher, M.; Amarenco, G. Motor determinants of gait in 100 ambulatory patients with multiple sclerosis. Mult. Scler. J. 2005, 11, 485–491. [Google Scholar] [CrossRef]
- Yahia, A.; Ghroubi, S.; Mhiri, C.; Elleuch, M. Relationship between muscular strength, gait and postural parameters in multiple sclerosis. Ann. Phys. Rehabil. Med. 2011, 54, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Gholamzad, M.; Ebtekar, M.; Ardestani, M.S.; Azimi, M.; Mahmodi, Z.; Mousavi, M.J.; Aslani, S. A comprehensive review on the treatment approaches of multiple sclerosis: Currently and in the future. Inflamm. Res. 2019, 68, 25–38. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M.; Kwakkel, G.; Dalgas, U.; Feinstein, A.; Heesen, C.; Feys, P.; Thompson, A.J. Exercise in patients with multiple sclerosis. Lancet Neurol. 2017, 16, 848–856. [Google Scholar] [CrossRef]
- Heine, M.; Van De Port, I.; Rietberg, M.B.; van Wegen, E.E.H.; Kwakkel, G. Exercise therapy for fatigue in multiple sclerosis. Cochrane Database Syst. Rev. 2015, 9, CD009956. [Google Scholar] [CrossRef]
- Pilutti, L.A.; Greenlee, T.A.; Motl, R.W.; Nickrent, M.S.; Petruzzello, S.J. Effects of exercise training on fatigue in multiple sclerosis: A meta-analysis. Psychosom. Med. 2013, 75, 575–580. [Google Scholar] [CrossRef]
- Alphonsus, K.B.; Su, Y.; D’arcy, C. The effect of exercise, yoga and physiotherapy on the quality of life of people with multiple sclerosis: Systematic review and meta-analysis. Complement. Ther. Med. 2019, 43, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Amato, A.; Ragonese, P.; Ingoglia, S.; Schiera, G.; Schirò, G.; Di Liegro, C.M.; Salemi, G.; Di Liegro, I.; Proia, P. Lactate Threshold Training Program on Patients with Multiple Sclerosis: A Multidisciplinary Approach. Nutrients 2021, 13, 4284. [Google Scholar] [CrossRef]
- Ahmadi, A.; Nikbakh, M.; Arastoo, A.; Habibi, A.-H. The effects of a yoga intervention on balance, speed and endurance of walking, fatigue and quality of life in people with multiple sclerosis. J. Hum. Kinet. 2010, 23, 71–78. [Google Scholar] [CrossRef]
- Shohani, M.; Badfar, G.; Nasirkandy, M.P.; Kaikhavani, S.; Rahmati, S.; Modmeli, Y.; Soleymani, A.; Azami, M. The effect of yoga on stress, anxiety, and depression in women. Int. J. Prev. Med. 2018, 9, 21. [Google Scholar]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef]
- Latimer-Cheung, A.E.; Pilutti, L.A.; Hicks, A.L.; Martin-Ginis, K.A.; Fenuta, A.M.; MacKibbon, K.A.; Motl, R.W. Effects of Exercise Training on Fitness, Mobility, Fatigue, and Health-Related Quality of Life Among Adults with Multiple Sclerosis: A Systematic Review to Inform Guideline Development. Arch. Phys. Med. Rehabil. 2013, 94, 1800–1828.e3. [Google Scholar] [CrossRef]
- Kalb, R.; Brown, T.R.; Coote, S.; Costello, K.; Dalgas, U.; Garmon, E.; Giesser, B.; Halper, J.; Karpatkin, H.; Keller, J.; et al. Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course. Mult. Scler. J. 2020, 26, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; McAuley, E.; Snook, E.M. Physical activity and multiple sclerosis: A meta-analysis. Mult. Scler. J. 2005, 11, 459–463. [Google Scholar] [CrossRef]
- Petrigna, L.; Pajaujiene, S.; Delextrat, A.; Gómez-López, M.; Paoli, A.; Palma, A.; Bianco, A. The importance of standard operating procedures in physical fitness assessment: A brief review. Sport Sci. Health 2022, 18, 21–26. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 3, e123–e130. [Google Scholar]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef]
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.; Kristjansson, E.; Grimshaw, J.; Henry, D.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 2009, 62, 1013–1020. [Google Scholar] [CrossRef]
- Suárez-Iglesias, D.; Bidaurrazaga-Letona, I.; Sanchez-Lastra, M.A.; Gil, S.M.; Ayán, C. Effectiveness of equine-assisted therapies for improving health outcomes in people with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2021, 55, 103161. [Google Scholar] [CrossRef]
- Arik, M.I.; Kiloatar, H.; Saracoglu, I. Do Pilates exercises improve balance in patients with multiple sclerosis? A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2022, 57, 103410. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Lastra, M.A.; Martínez-Aldao, D.; Molina, A.J.; Ayán, C. Pilates for people with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2019, 28, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Gharakhanlou, R.; Wesselmann, L.; Rademacher, A.; Lampit, A.; Negaresh, R.; Kaviani, M.; Oberste, M.; Motl, R.W.; Sandroff, B.M.; Bansi, J.; et al. Exercise training and cognitive performance in persons with multiple sclerosis: A systematic review and multilevel meta-analysis of clinical trials. Mult. Scler. J. 2021, 27, 1977–1993. [Google Scholar] [CrossRef]
- Afkar, A.; Ashouri, A.; Rahmani, M.; Sigaroudi, A.E. Effect of exercise therapy on quality of life of patients with multiple sclerosis in Iran: A systematic review and meta-analysis. Neurol. Sci. 2017, 38, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Lauche, R.; Azizi, H.; Dobos, G.; Langhorst, J. Yoga for multiple sclerosis: A systematic review and meta-analysis. PLoS ONE 2014, 9, e112414. [Google Scholar] [CrossRef]
- Dalgas, U.; Stenager, E.; Sloth, M. The effect of exercise on depressive symptoms in multiple sclerosis based on a meta-analysis and critical review of the literature. Eur. J. Neurol. 2015, 22, 443-e34. [Google Scholar] [CrossRef]
- Dennett, R.; Madsen, L.T.; Connolly, L.; Hosking, J.; Dalgas, U.; Freeman, J. Adherence and drop-out in randomized controlled trials of exercise interventions in people with multiple sclerosis: A systematic review and meta-analyses. Mult. Scler. Relat. Disord. 2020, 43, 102169. [Google Scholar] [CrossRef]
- Hao, Z.; Zhang, X.; Chen, P. Effects of Different Exercise Therapies on Balance Function and Functional Walking Ability in Multiple Sclerosis Disease Patients—A Network Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 7175. [Google Scholar] [CrossRef]
- Jørgensen, M.; Dalgas, U.; Wens, I.; Hvid, L. Muscle strength and power in persons with multiple sclerosis—A systematic review and meta-analysis. J. Neurol. Sci. 2017, 376, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Langeskov-Christensen, M.; Heine, M.; Kwakkel, G.; Dalgas, U. Aerobic capacity in persons with multiple sclerosis: A systematic review and meta-analysis. Sports Med. 2015, 45, 905–923. [Google Scholar] [CrossRef] [PubMed]
- Pearson, M.; Dieberg, G.; Smart, N. Exercise as a therapy for improvement of walking ability in adults with multiple sclerosis: A meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 1339–1348.e7. [Google Scholar] [CrossRef] [PubMed]
- Shariat, A.; Najafabadi, M.G.; Fard, Z.S.; Nakhostin-Ansari, A.; Shaw, B.S. A systematic review with meta-analysis on balance, fatigue, and motor function following aquatic therapy in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 68, 104107. [Google Scholar] [CrossRef]
- Shohani, M.; Kazemi, F.; Rahmati, S.; Azami, M. The effect of yoga on the quality of life and fatigue in patients with multiple sclerosis: A systematic review and meta-analysis of randomized clinical trials. Complement. Ther. Clin. Pract. 2020, 39, 101087. [Google Scholar] [CrossRef]
- Taul-Madsen, L.; Connolly, L.; Dennett, R.; Freeman, J.; Dalgas, U.; Hvid, L.G. Is Aerobic or Resistance Training the Most Effective Exercise Modality for Improving Lower Extremity Physical Function and Perceived Fatigue in People With Multiple Sclerosis? A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2021, 102, 2032–2048. [Google Scholar] [CrossRef]
- Torres-Costoso, A.; Martínez-Vizcaíno, V.; Reina-Gutiérrez, S.; Álvarez-Bueno, C.; Guzmán-Pavón, M.J.; Pozuelo-Carrascosa, D.P.; Fernández-Rodríguez, R.; Sanchez-López, M.; Cavero-Redondo, I. Effect of Exercise on Fatigue in Multiple Sclerosis: A Network Meta-analysis Comparing Different Types of Exercise. Arch. Phys. Med. Rehabil. 2022, 103, 970–987.e18. [Google Scholar] [CrossRef]
- Rooney, S.; Wood, L.; Moffat, F.; Paul, L. Is Fatigue Associated with Aerobic Capacity and Muscle Strength in People With Multiple Sclerosis: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 2193–2204. [Google Scholar] [CrossRef]
- Safari, R.; van der Linden, M.L.; Mercer, T.H. Effect of exercise interventions on perceived fatigue in people with multiple sclerosis: Synthesis of meta-analytic reviews. Neurodegener. Dis. Manag. 2017, 7, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Edwards, T.; Michelsen, A.S.; Fakolade, A.O.; Dalgas, U.; Pilutti, L.A. Exercise training improves participation in persons with multiple sclerosis: A systematic review and meta-analysis. J. Sport Health Sci. 2022, 11, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Amatya, B.; Khan, F.; Ng, L.; Galea, M. Rehabilitation for people with multiple sclerosis: An overview of Cochrane systematic reviews. Cochrane Database Syst. Rev. 2019, 1, Cd012732. [Google Scholar] [CrossRef] [PubMed]
- Shobeiri, P.; Karimi, A.; Momtazmanesh, S.; Teixeira, A.L.; Teunissen, C.E.; van Wegen, E.E.H.; Hirsch, M.A.; Yekaninejad, M.S.; Rezaei, N. Exercise-induced increase in blood-based brain-derived neurotrophic factor (BDNF) in people with multiple sclerosis: A systematic review and meta-analysis of exercise intervention trials. PLoS ONE 2022, 17, e0264557. [Google Scholar] [CrossRef]
- Torres-Pareja, M.; Sánchez-Lastra, M.A.; Iglesias, L.; Suárez-Iglesias, D.; Mendoza, N.; Ayán, C. Exercise Interventions for Improving Flexibility in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Medicina 2019, 55, 726. [Google Scholar] [CrossRef]
- Cameron, M.H.; Lord, S. Postural control in multiple sclerosis: Implications for fall prevention. Curr. Neurol. Neurosci. Rep. 2010, 10, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Bulguroglu, I.; Guclu-Gunduz, A.; Yazici, G.; Ozkul, C.; Irkec, C.; Nazliel, B.; Batur-Caglayan, H. The effects of Mat Pilates and Reformer Pilates in patients with Multiple Sclerosis: A randomized controlled study. NeuroRehabilitation 2017, 41, 413–422. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, S.; Shen, J.; Yang, H.; Xu, W.; Shao, M.; Pan, F. Effect of Exercise on Fatigue in Multiple Sclerosis Patients: A Network Meta-analysis. Int. J. Sports Med. 2021, 42, 1250–1259. [Google Scholar] [CrossRef]
- Abasıyanık, Z.; Ertekin, Ö.; Kahraman, T.; Yigit, P.; Özakbaş, S. The effects of Clinical Pilates training on walking, balance, fall risk, respiratory, and cognitive functions in persons with multiple sclerosis: A randomized controlled trial. Explore 2020, 16, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Tollár, J.; Nagy, F.; Tóth, B.E.; Török, K.; Szita, K.; Csutorás, B.; Moizs, M.; Hortobágyi, T. Exercise Effects on Multiple Sclerosis Quality of Life and Clinical–Motor Symptoms. Med. Sci. Sports Exerc. 2020, 52, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Byrnes, K.L.; Whillier, S. Effects of Nonpharmaceutical Treatments on Symptom Management in Adults with Mild or Moderate Multiple Sclerosis: A Meta-analysis. J. Manip. Physiol. Ther. 2019, 42, 514–531. [Google Scholar] [CrossRef] [PubMed]
- Diechmann, M.D.; Campbell, E.; Coulter, E.; Paul, L.; Dalgas, U.; Hvid, L.G. Effects of Exercise Training on Neurotrophic Factors and Subsequent Neuroprotection in Persons with Multiple Sclerosis—A Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 1499. [Google Scholar] [CrossRef]
- García, J.D.J.; Martínez-Amat, A.; De La Torre-Cruz, M.J.; Fábrega-Cuadros, R.; Díaz, D.C.; Aibar-Almazán, A.; Achalandabaso-Ochoa, A.; Hita-Contreras, F. Suspension training HIIT improves gait speed, strength and quality of life in older adults. Int. J. Sports Med. 2019, 40, 116–124. [Google Scholar] [CrossRef]
- Cannataro, R.; Cione, E.; Bonilla, D.A.; Cerullo, G.; Angelini, F.; D’Antona, G. Strength training in elderly: An useful tool against sarcopenia. Front. Sports Act. Living 2022, 4, 950949. [Google Scholar] [CrossRef]
- Kim, Y.; Mehta, T.; Lai, B.; Motl, R.W. Immediate and Sustained Effects of Interventions for Changing Physical Activity in People with Multiple Sclerosis: Meta-analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2020, 101, 1414–1436. [Google Scholar] [CrossRef]
- Rintala, A.; Hakala, S.; Paltamaa, J.; Heinonen, A.; Karvanen, J.; Sjögren, T. Effectiveness of technology-based distance physical rehabilitation interventions on physical activity and walking in multiple sclerosis: A systematic review and meta-analysis of randomized controlled trials. Disabil. Rehabil. 2018, 40, 373–387. [Google Scholar] [CrossRef]
- Abou, L.; Qin, K.; Alluri, A.; Du, Y.; Rice, L.A. The effectiveness of physical therapy interventions in reducing falls among people with multiple sclerosis: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2022, 29, 74–85. [Google Scholar] [CrossRef]
- Ensari, I.; Motl, R.W.; Pilutti, L.A. Exercise training improves depressive symptoms in people with multiple sclerosis: Results of a meta-analysis. J. Psychosom. Res. 2014, 76, 465–471. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| 1st Author, Year | Guideline | Databases Searched | Main Objective | No. of Study | Risk of Bias | Main Conclusions |
|---|---|---|---|---|---|---|
| Afkar [39] | NI | MEDLINE, Scopus, Google | Study the effect size of exercise therapy on pwMS’ quality of life in physical and mental dimensions | 31 | Quality range from 4 to 8 | High quality of life was determined for 12 vs. 8 weeks of exercise and was found to be lower |
| Cramer, 2014 [40] | PRISMA | MEDLINE, Scopus, Cochrane | Examine accessible information on yoga’s efficiency and safety | 9 | Cochrane tool: overall medium | There were short-term effects of yoga on fatigue and mood but not on health-related quality of life or mobility. No evidence was found for the effects of yoga compared to exercise. |
| Dalgas [41] | PRISMA | MEDLINE, Embase, Cochrane, PEDro, SPORTDiscus | Study the effects of exercise on depressive symptoms in pwMS | 12 | PEDro score: 5.6–1.3 points | There was temporary improvement after 5 and 10 weeks of intervention but not after 15 weeks |
| Dennett 2020 [42] | PRISMA | MEDLINE, Scopus, Embase, PEDro, SPORTDiscus, WoS | Summarize interventions and identify moderators related to adherence and dropout | 93 | TESTEX rating scale: 7.5/15 | Half of the existing exercises reported data on adherence and dropout. |
| Gharakhanlou, 2021 [38] | PRISMA | MEDLINE, Embase, Cochrane, SPORTDiscus | Investigate how exercise affects pwMS’ overall cognitive performance | 13 | TESTEX: non-sufficient | Exercise training did not have significant effects on global cognitive performance, attention, executive function, or learning/memory. |
| Hao [43] | NI | MEDLINE, Embase, Cochrane, WoS, CNKI | Study the effects of 7 different exercise therapies on the balance function and functional walking ability of pwMS | 31 | 13% high risk of bias | Exercise interventions improved dynamic and static balance and the functional walking ability of pwMS. |
| Isintas Arik, 2022 [36] | PRISMA | MEDLINE, Scopus, PEDro, Science Direct | Evaluate the effects of Pilates workouts on balance in pwMS | 8 | PEDro results ≥ 4 | Pilates improved static and dynamic balance. |
| Jørgensen, 2017 [44] | PRISMA | MEDLINE, Embase, Cochrane, SPORTDiscus, PEDro | Association of how progressive resistance training affects muscle function | 10 | PEDro score ≥ 5 | Progressive resistance training increased muscle strength, muscle power, and explosive muscle strength. |
| Langeskov-Christensen [45] | PRISMA | MEDLINE, Embase, Cochrane, PEDro, CINAHL, SPORTDiscus | Evaluate the effects of longitudinal studies evaluating training-induced effects on VO2max in PwMS | 17 | PEDro score: 5.5 ± 1.5 (range 3–8) | Aerobic training improved aerobic capacity to a level close to the reduction of secondary health risks. |
| Pearson 2015 [46] | PRISMA | MEDLINE, Embase, Cochrane, CINAHL, SPORTDiscus | Provide information on exercise for improving walking ability in pwMS | 13 | PEDro scale ≥ 6 | Improvement in walking ability was seen. |
| Sánchez-Lastra, 2019 [37] | PRISMA | MEDLINE, Scopus, PEDro, SPORTDiscus | Study the effects of Pilates on pwMS | 14 | NI | There were significant effects on quality of life, pain, walking ability, and physical function but not on functional mobility, cardiorespiratory fitness, or depression. |
| Shariat, 2022 [47] | PRISMA | MEDLINE, Cochrane, WoS, Ovid | Evaluate the effects of long-term aquatic training on balance, fatigue, and motor function in pwMS | 16 | Joanna Briggs checklists: above 8 | Aquatic therapy improved physical fatigue to a greater extent than the control group; it significantly improved fatigue and balance. |
| Shohani, 2020 [48] | PRISMA | MEDLINE, Scopus, Cochrane, WoS, Science Direct | Investigate how yoga impacts pwMS’ quality of life and level of fatigue | 10 | High or uncertain risk of bias | Yoga was not healing for fatigue or health-related quality of life. |
| Suarez-Iglesias, 2021 [35] | PRISMA | MEDLINE, Scopus, PEDro, SPORTDiscus | Assess the information on the potential healing properties of EAT in PwMS | 9 | PEDro results ≥ 6 | There were significant effects on static balance, walking distance, quality of life, spasticity, pain, and incontinence. No significant results were found for depression and constipation or muscular strength. |
| Taul-Madsen, 2021 [49] | PRISMA | MEDLINE, Scopus, Embase, WoS, SPORTDiscus | Study the effects of exercises on lower limb function and perceived fatigue in pwMS | 27 | NI | Resistance and aerobic training improved lower extremity physical function and perceived fatigue. |
| Torres-Costoso [50] | PRISMA | MEDLINE, Embase, Cochrane, WoS. SPORTDiscus | Determine whether and which physical exercise has a positive influence on fatigue | 58 | RoB2: low risk of bias | Physical exercise reduced fatigue. |
| 1st Author, Year | Number of Participants, MS Type | Intervention | Main Results |
|---|---|---|---|
| Afkar [39] | No.: 535, not reported | Mixed |
D: 4–12 weeks; F: 2–3/week; D/s: 20–75 min;
aerobic, yoga, combination, aquatic, and resistance |
| Cramer, 2014 [40] | No.: range of 20–314, mixed | Yoga | D: 8–24 weeks; F: 1–3/week; D/s: 60–90 min; Hatha yoga, Iyengar yoga, yoga postures and meditation or relaxation, and yogic breathing techniques. |
| Dalgas, 2015 [41] | No.: 591, mixed | Mixed | D: 3–26 weeks; endurance training, resistance training, combined training, or other exercise modalities, including sports climbing, yoga, and water activities. Three studies evaluated several exercise interventions. |
| Dennett, 2020 [42] | No.: 4007, mixed | Mixed | D: 3–26 weeks; F: 1–7/week; yoga, cycling, body weight, mobility, strength training, balance training, endurance, and stretching |
| Gharakhanlou, 2021 [38] | No.: 639, mixed | Aerobic training and resistance training | D: 8–26 weeks; F: 2–4/week; D/s: 20–60 min I: from low to vigorous, with different modalities of intervention; aerobic, resistance exercises, or mixed; 1 added balance |
| Hao, 2022 [43] | No.: 904, not reported | Mixed | D: 2–24 weeks; F: 1–6/week; D/s: 10–60 min; aquatic, yoga, Pilates, aquatic, aerobic, resistance, and virtual reality training |
| Isintas Arik, 2022 [36] | No.: 349, mixed | Pilates | D: 8–12 weeks; D/s: 45–60 min; I: low to moderate; F: 1–3/week |
| Jørgensen, 2017 [44] | No.: 236, not reported | Progressive resistance training | D: 3–24 weeks; F: 2–5/week; I: progressively increasing between 50 and 90% of 1RM. Number of exercises from 2 to 5; one study included upper body exercises. |
| Langeskov-Christensen [45] | No.: 330, not reported | Aerobic | D: 3–26 weeks, F: 2–5/week; D/s: 15–45 min; cycling, treadmill walking, rowing, and aquatic aerobics |
| Pearson 2015 [46] | No.: range 12–119, not reported | Mixed | D: 4–26 weeks; aerobic, yoga, mixed, resistance, and balance |
| Sánchez-Lastra, 2019 [37] | No.: 507, mixed | Pilates | D: 8–16 weeks; F: 1–3/week; D/s: 15–90 min; I: controlled using the color of the TheraBand® |
| Shariat, 2022 [47] | No.: 794, mixed | Aquatic therapy | D: 3–20 weeks; D/s: 45–135 min; freestyle swimming and shallow water calisthenics aerobics exercise, Ai-Chi exercise in the swimming pool, ergometer water group, and aquatic plyometric exercises |
| Shohani, 2020 [48] | No.: 693, not reported | Yoga | D: 8–24 weeks; F:1–3/week; D/s: 60–120 min each; Hatha yoga and Iyengar yoga |
| Suarez-Iglesias, 2021 [35] | No.: 225, not reported | Equine-assisted therapy | D: 8–24 weeks; F: 1–2/week; D: 20–50 D/s |
| Taul-Madsen, 2021 [49] | No.: 966, mixed | Aerobic training and resistance training | AT. D: 3–26 weeks; F: 1–5/week, D/s: 27–69 min; I: moderate, high, or unknown RT. D: 8–24 weeks; F: 1–3/week; D/s: 30–60 min; I moderate, high, or unknown |
| Torres-Costoso, 2022 [50] | No.: 2644, not reported | Mixed | D: 4–26 weeks; F: 1–5/week; D/s: 15–120 min; aerobic, stretching, flexion and rotation movements, resistance, combined, yoga, Pilates balance, mobilization, and aquatic exercise + current treatment. |
| 1st Author, Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Afkar [39] | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Cramer, 2014 [40] | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 9 |
| Dalgas, 2015 [41] | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Dennett, 2020 [42] | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 7 |
| Gharakhanlou, 2021 [38] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 10 |
| Hao, 2022 [43] | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Isintas Arik, 2022 [36] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 |
| Jørgensen, 2017 [44] | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 7 |
| Langeskov-Christensen [45] | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 5 |
| Pearson, 2015 [46] | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 5 |
| Sánchez-Lastra, 2019 [37] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 9 |
| Shariat, 2022 [47] | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 9 |
| Shohani, 2020 [48] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Suarez-Iglesias, 2021 [35] | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 9 |
| Taul-Madsen, 2021 [49] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 8 |
| Torres-Costoso, 2022 [50] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sortino, M.; Petrigna, L.; Trovato, B.; Amato, A.; Castorina, A.; D’Agata, V.; Maugeri, G.; Musumeci, G. An Overview of Physical Exercise Program Protocols and Effects on the Physical Function in Multiple Sclerosis: An Umbrella Review. J. Funct. Morphol. Kinesiol. 2023, 8, 154. https://doi.org/10.3390/jfmk8040154
Sortino M, Petrigna L, Trovato B, Amato A, Castorina A, D’Agata V, Maugeri G, Musumeci G. An Overview of Physical Exercise Program Protocols and Effects on the Physical Function in Multiple Sclerosis: An Umbrella Review. Journal of Functional Morphology and Kinesiology. 2023; 8(4):154. https://doi.org/10.3390/jfmk8040154
Chicago/Turabian StyleSortino, Martina, Luca Petrigna, Bruno Trovato, Alessandra Amato, Alessandro Castorina, Velia D’Agata, Grazia Maugeri, and Giuseppe Musumeci. 2023. "An Overview of Physical Exercise Program Protocols and Effects on the Physical Function in Multiple Sclerosis: An Umbrella Review" Journal of Functional Morphology and Kinesiology 8, no. 4: 154. https://doi.org/10.3390/jfmk8040154