
Detection of the Anaerobic Threshold in Endurance Sports: Validation of a New Method Using Correlation Properties of Heart Rate Variability




Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Exercise Protocol
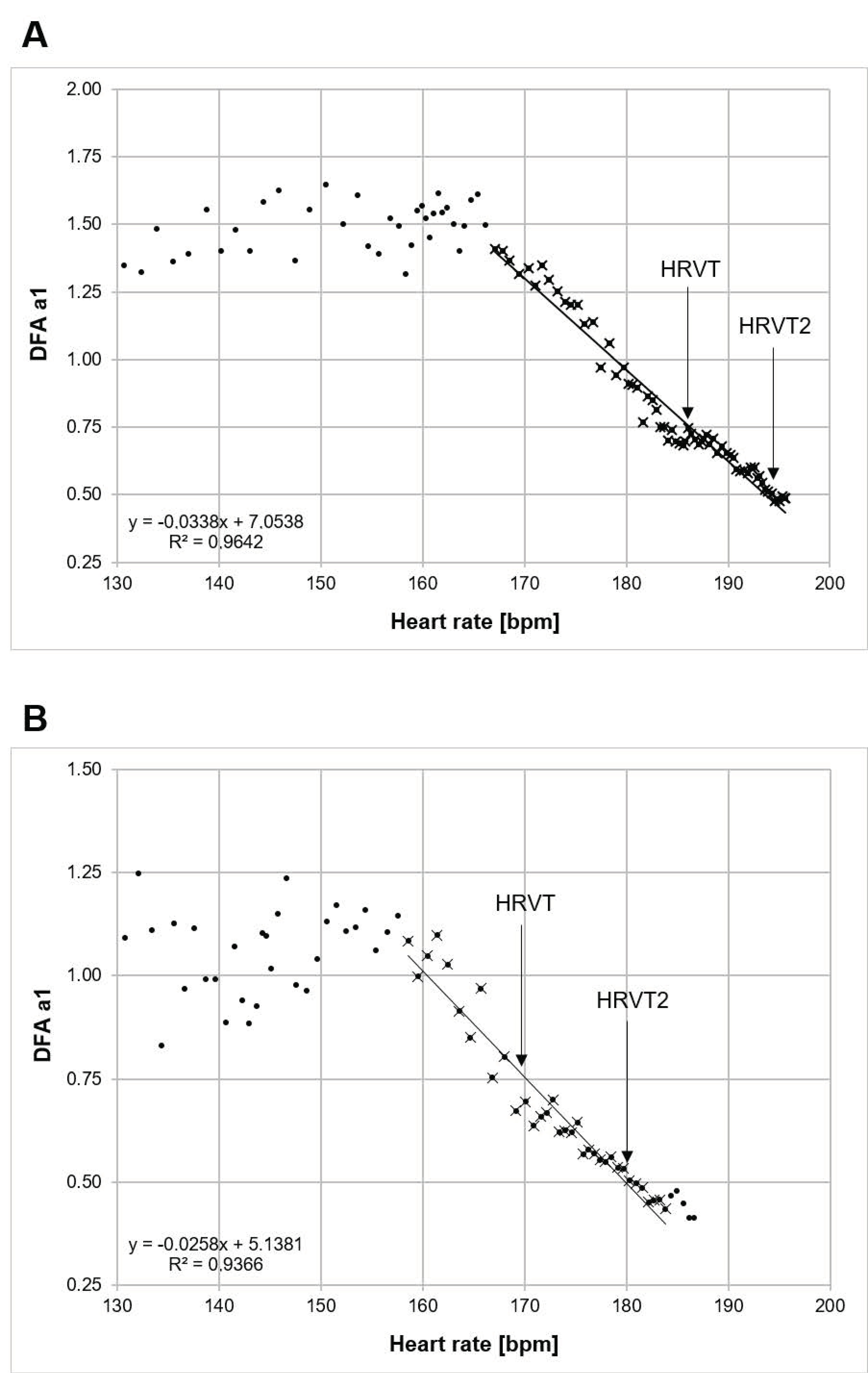
2.3. RR Measurements and Calculation of DFA a1 Derived Threshold
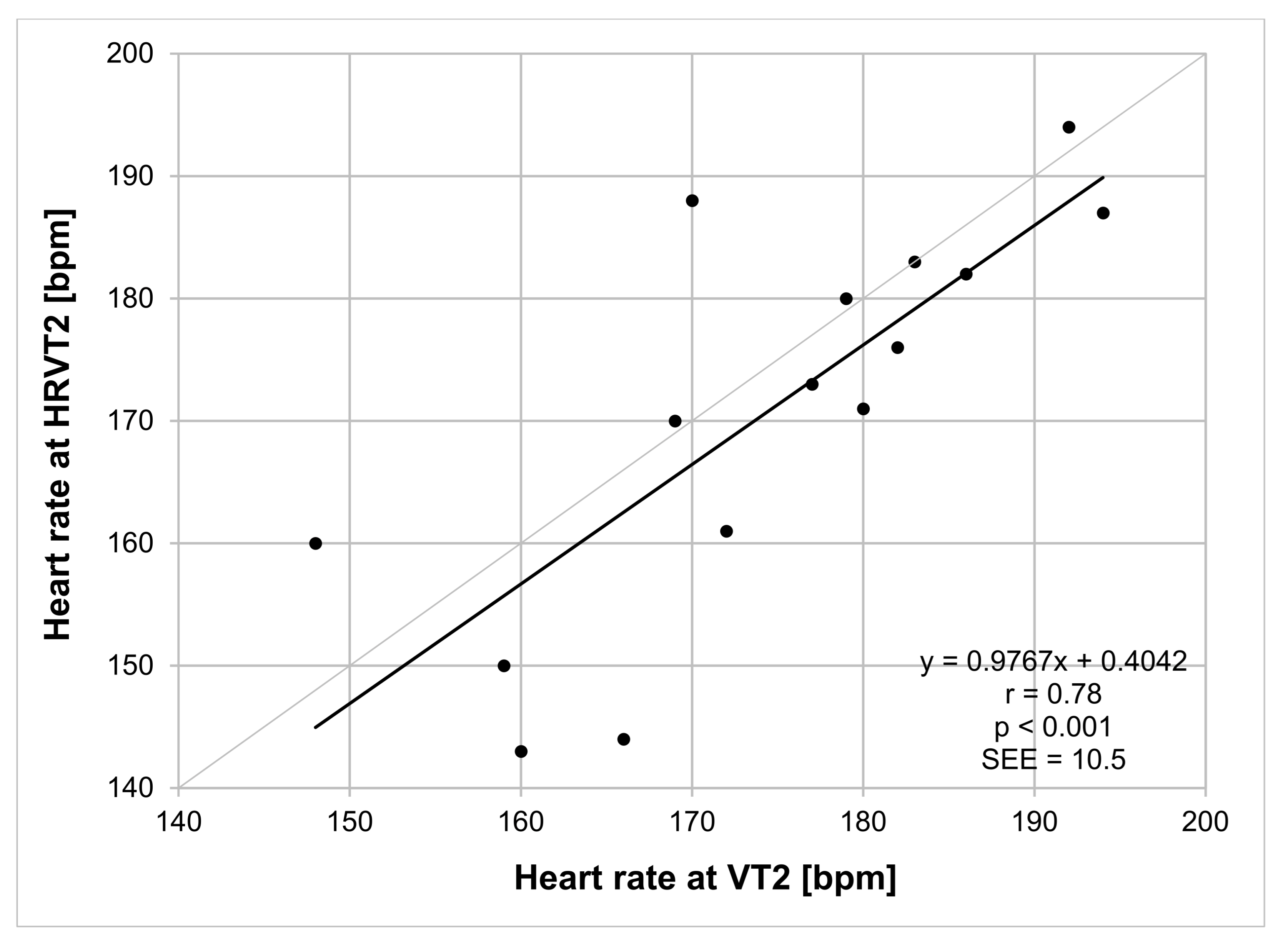
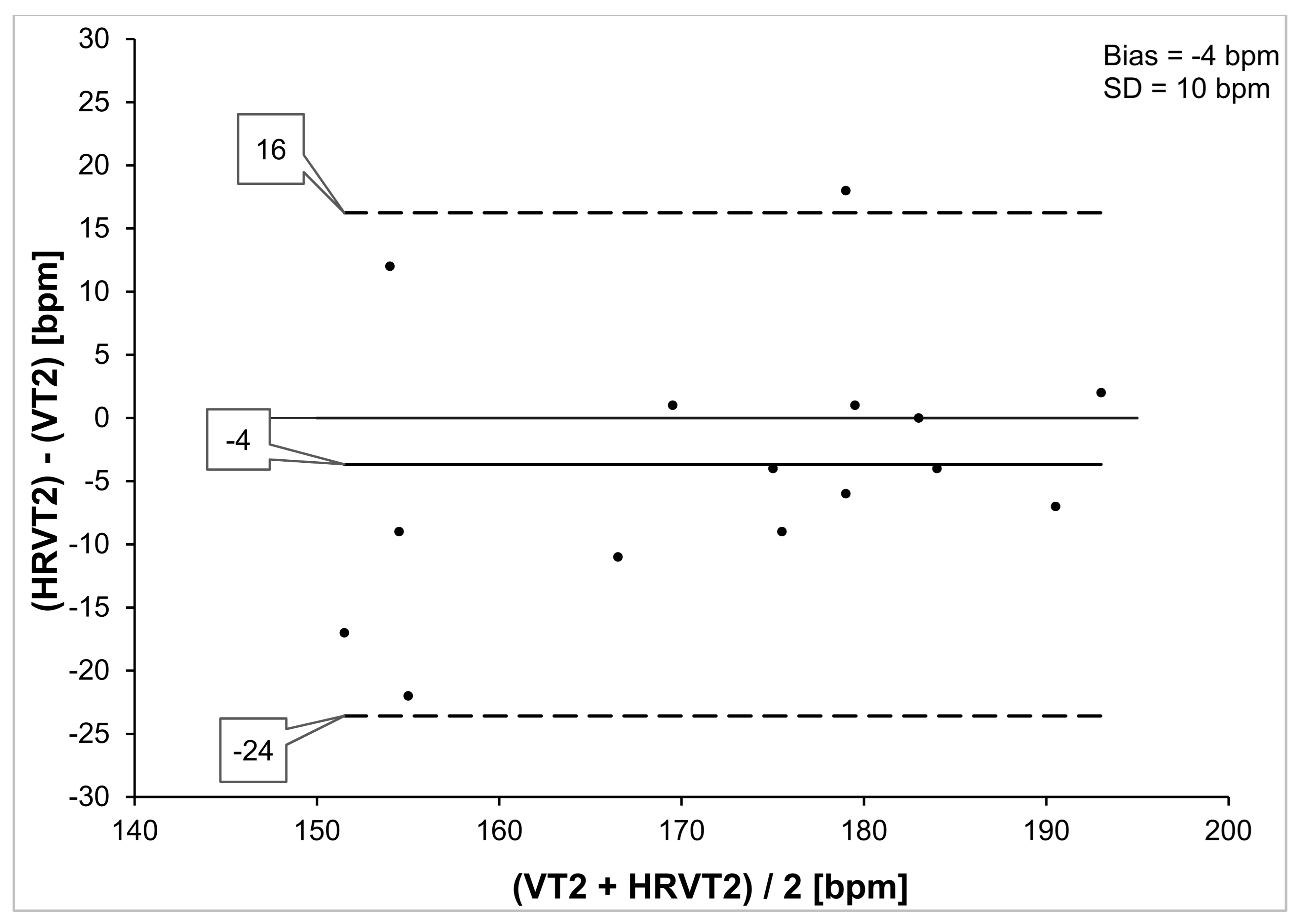
3. Statistics
4. Results
5. Discussion
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stöggl, T.L.; Sperlich, B. Editorial: Training Intensity, Volume and Recovery Distribution Among Elite and Recreational Endurance Athletes. Front. Physiol. 2019, 10, 592. [Google Scholar] [CrossRef]
- Jamnick, N.A.; Pettitt, R.W.; Granata, C.; Pyne, D.B.; Bishop, D.J. An Examination and Critique of Current Methods to Determine Exercise Intensity. Sports Med. 2020, 50, 1729–1756. [Google Scholar] [CrossRef] [PubMed]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H.; Schmid, J.-P. Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Meyer, T.; Lucía, A.; Earnest, C.P.; Kindermann, W. A Conceptual Framework for Performance Diagnosis and Training Prescription from Submaximal Gas Exchange Parameters—Theory and Application. Int. J. Sports Med. 2004, 26, S38–S48. [Google Scholar] [CrossRef] [PubMed]
- Keir, D.A.; Fontana, F.Y.; Robertson, T.C.; Murias, J.M.; Paterson, D.H.; Kowalchuk, J.M.; Pogliaghi, S. Exercise Intensity Thresholds: Identifying the Boundaries of Sustainable Performance. Med. Sci. Sports Exerc. 2015, 47, 1932–1940. [Google Scholar] [CrossRef] [PubMed]
- Faude, O.; Kindermann, W.; Meyer, T. Lactate threshold concepts: How valid are they? Sports Med. 2009, 39, 469–490. [Google Scholar] [CrossRef]
- Caen, K.; Pogliaghi, S.; Lievens, M.; Vermeire, K.; Bourgois, J.G.; Boone, J. Ramp vs. step tests: Valid alternatives to determine the maximal lactate steady-state intensity? Eur. J. Appl. Physiol. 2021, 1–9. [Google Scholar] [CrossRef]
- Bellotti, C.; Calabria, E.; Capelli, C.; Pogliaghi, S. Determination of maximal lactate steady state in healthy adults: Can NIRS help? Med. Sci. Sports Exerc. 2013, 45, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Fontana, F.Y.; Keir, D.A.; Bellotti, C.; de Roia, G.F.; Murias, J.M.; Pogliaghi, S. Determination of respiratory point compensation in healthy adults: Can non-invasive near-infrared spectroscopy help? J. Sci. Med. Sport 2015, 18, 590–595. [Google Scholar] [CrossRef]
- Allen, H.; Coggan, A. Training and Racing with a Power Meter; Velo Press: Boulder, CO, USA, 2010. [Google Scholar]
- Lillo-Beviá, J.R.; Courel-Ibáñez, J.; Cerezuela-Espejo, V.; Morán-Navarro, R.; Martínez-Cava, A.; Pallarés, J.G. Is the Functional Threshold Power a Valid Metric to Estimate the Maximal Lactate Steady State in Cyclists? J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Klitzke Borszcz, F.; Ferreira Tramontin, A.; Pereira Costa, V. Is the Functional Threshold Power Interchangeable with the Maximal Lactate Steady State in Trained Cyclists? Int. J. Sports Physiol. Perform. 2019, 14, 1029–1035. [Google Scholar] [CrossRef]
- Inglis, E.C.; Iannetta, D.; Passfield, L.; Murias, J.M. Maximal Lactate Steady State Versus the 20-Minute Functional Threshold Power Test in Well-Trained Individuals: “Watts” the Big Deal? Int. J. Sports Physiol. Perform. 2020, 15, 541–547. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, P.L.; Morales, J.S.; Foster, C.; Lucía, A.; de La Villa, P. Is the Functional Threshold Power a Valid Surrogate of the Lactate Threshold? Int. J. Sports Physiol. Perform. 2018, 13, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Burnley, M.; Black, M.I.; Poole, D.C.; Vanhatalo, A. The maximal metabolic steady state: Redefining the ‘gold standard’. Physiol. Rep. 2019, 7, e14098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karsten, B.; Petrigna, L.; Klose, A.; Bianco, A.; Townsend, N.; Triska, C. Relationship between the Critical Power Test and a 20-min Functional Threshold Power Test in Cycling. Front. Physiol. 2021, 11, 613151. [Google Scholar] [CrossRef] [PubMed]
- Gronwald, T.; Rogers, B.; Hoos, O. Fractal Correlation Properties of Heart Rate Variability: A New Biomarker for Intensity Distribution in Endurance Exercise and Training Prescription? Front. Physiol. 2020, 11, 550572. [Google Scholar] [CrossRef]
- White, D.W.; Raven, P.B. Autonomic neural control of heart rate during dynamic exercise: Revisited. J. Physiol. 2014, 592, 2491–2500. [Google Scholar] [CrossRef] [PubMed]
- Tulppo, M.P.; Makikallio, T.H.; Takala, T.E.; Seppanen, T.; Huikuri, H.V. Quantitative beat-to-beat analysis of heart rate dynamics during exercise. Am. J. Physiol. Circ. Physiol. 1996, 271, H244–H252. [Google Scholar] [CrossRef]
- Cottin, F.; Médigue, C.; Lopes, P.; Lepretre, P.-M.; Heubert, R.; Billat, V. Ventilatory Thresholds Assessment from Heart Rate Variability during an Incremental Exhaustive Running Test. Int. J. Sports Med. 2006, 28, 287–294. [Google Scholar] [CrossRef]
- Karapetian, G.K.; Engels, H.J.; Gretebeck, R.J. Use of heart rate variability to estimate LT and VT. Int. J. Sports Med. 2008, 29, 652–657. [Google Scholar] [CrossRef]
- Gronwald, T.; Hoos, O.; Ludyga, S.; Hottenrott, K. Non-linear dynamics of heart rate variability during incremental cycling exercise. Res. Sports Med. 2019, 27, 88–98. [Google Scholar] [CrossRef]
- Gronwald, T.; Hoos, O. Correlation properties of heart rate variability during endurance exercise: A systematic review. Ann. Noninvasive Electrocardiol. 2020, 25, e12697. [Google Scholar] [CrossRef] [Green Version]
- Ivanov, P.C.; Amaral, L.A.N.; Goldberger, A.L.; Havlin, S.; Rosenblum, M.G.; Stanley, H.E.; Struzik, Z.R. From 1/f noise to multifractal cascades in heartbeat dynamics. Chaos Interdiscip. J. Nonlinear Sci. 2001, 11, 641–652. [Google Scholar] [CrossRef] [Green Version]
- Eke, A.; Herman, P.; Kocsis, L.; Kozak, L.R. Fractal characterization of complexity in temporal physiological signals. Physiol. Meas. 2002, 23, R1–R38. [Google Scholar] [CrossRef] [Green Version]
- Balagué, N.; Hristovski, R.; Almarcha, M.D.C.; Garcia-Retortillo, S.; Ivanov, P.C. Network Physiology of Exercise: Vision and Perspectives. Front. Physiol. 2020, 11, 611550. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.; Giles, D.; Draper, N.; Hoos, O.; Gronwald, T. A New Detection Method Defining the Aerobic Threshold for Endurance Exercise and Training Prescription Based on Fractal Correlation Properties of Heart Rate Variability. Front. Physiol. 2021, 11, 596567. [Google Scholar] [CrossRef]
- Hardstone, R.; Poil, S.S.; Schiavone, G.; Jansen, R.; Nikulin, V.V.; Mansvelder, H.D.; Linkenkaer-Hansen, K. Detrended fluctuation analysis: A scale-free view on neuronal oscillations. Front. Physiol. 2012, 3, 450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karasik, R.; Sapir, N.; Ashkenazy, Y.; Ivanov, P.C.; Dvir, I.; Lavie, P.; Havlin, S. Correlation differences in heartbeat fluctuations during rest and exercise. Phys. Rev. E 2002, 66, 062902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, B.; Giles, D.; Draper, N.; Mourot, L.; Gronwald, T. Influence of Artefact Correction and Recording Device Type on the Practical Application of a Non-Linear Heart Rate Variability Biomarker for Aerobic Threshold Determination. Sensors 2021, 21, 821. [Google Scholar] [CrossRef]
- Reis, V.M.; Tillaar, R.V.D.; Marques, M.C. Higher Precision of Heart Rate Compared with VO2 to Predict Exercise Intensity in Endurance-Trained Runners. J. Sports Sci. Med. 2011, 10, 164–168. [Google Scholar]
- Zignoli, A.; Fornasiero, A.; Stella, F.; Pellegrini, B.; Schena, F.; Biral, F.; Laursen, P.B. Expert-level classification of ventilatory thresholds from cardiopulmonary exercising test data with recurrent neural networks. Eur. J. Sport Sci. 2019, 19, 1221–1229. [Google Scholar] [CrossRef]
- Zignoli, A.; Fornasiero, A.; Rota, P.; Muollo, V.; Peyré-Tartaruga, L.; Low, D.; Fontana, F.; Besson, D.; Pühringer, M.; Ring-Dimitriou, S.; et al. Oxynet: A collective intelligence that detects ventilatory thresholds in cardiopulmonary exercise tests. Eur. J. Sport Sci. 2021, 31, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Lipponen, J.A.; Tarvainen, M.P. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J. Med. Eng. Technol. 2019, 43, 173–181. [Google Scholar] [CrossRef]
- Chen, Z.; Ivanov, P.C.; Hu, K.; Stanley, H.E. Effect of nonstationarities on detrended fluctuation analysis. Phys. Rev. E 2002, 65, 041107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Naranjo-Orellana, J.; Nieto-Jiménez, C.; Ruso-Álvarez, J. Non-linear heart rate dynamics during and after three controlled exercise intensities in healthy men. Physiol. Int. 2021, 107, 501–512. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Hausdorff, J.M.; Ivanov, P.C.; Peng, C.K.; Stanley, H.E. Fractal dynamics in physiology: Alterations with disease and aging. Proc. Natl. Acad. Sci. USA 2002, 99, 2466–2472. [Google Scholar] [CrossRef] [Green Version]
- Fossion, R.; Rivera, A.L.; Estañol, B. A physicist’s view of homeostasis: How time series of continuous monitoring reflect the function of physiological variables in regulatory mechanisms. Physiol. Meas. 2018, 39, 084007. [Google Scholar] [CrossRef] [Green Version]
- von Bertalanffy, L. An outline on General System Theory. Br. J. Philos. Sci. 1950, 2, 134–165. [Google Scholar] [CrossRef]
- von Bertalanffy, L. The Theory of Open Systems in Physics and Biology. Science 1950, 111, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Rosenwinkel, E.T.; Bloomfield, D.M.; Arwady, M.A.; Goldsmith, R.L. Exercise and autonomic function in health and cardiovascular disease. Cardiol. Clin. 2001, 19, 369–387. [Google Scholar] [CrossRef]
- Kannankeril, P.J.; Goldberger, J.J. Parasympathetic effects on cardiac electrophysiology during exercise and recovery. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H2091–H2098. [Google Scholar] [CrossRef] [Green Version]
- Billman, G.E. Cardiac autonomic neural remodeling and susceptibility to sudden cardiac death: Effect of endurance exercise training. Am. J. Physiol. Circ. Physiol. 2009, 297, H1171–H1193. [Google Scholar] [CrossRef] [Green Version]
- Seely, A.J.; Macklem, P.T. Complex systems and the technology of variability analysis. Crit. Care 2004, 8, R367–R384. [Google Scholar] [CrossRef] [Green Version]
- Cassirame, J.; Chevrolat, S.; Mourot, L. Effects of R-R time series accuracy on heart rate variability indexes. Mov. Sport Sci. Sci. Mot. 2019, 106, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Giles, D.A.; Draper, N. Heart Rate Variability During Exercise: A Comparison of Artefact Correction Methods. J. Strength Cond. Res. 2018, 32, 726–735. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Nr. | Age [yrs] | TV [hrs/wk] | BW [kg] | VO2MAX [mL/kg/min] | VT2 [bpm] | HRVT2 [bpm] |
|---|---|---|---|---|---|---|
| 1 | 19 | 3–6 | 82 | 58 | 179 | 180 |
| 2 | 19 | 3–6 | 82 | 57 | 183 | 183 |
| 3 | 20 | 3–6 | 82 | 47 | 194 | 187 |
| 4 | 22 | 1–3 | 73 | 45 | 170 | 188 |
| 5 | 23 | >6 | 77 | 71 | 148 | 160 |
| 6 | 24 | 3–6 | 69 | 64 | 166 | 144 |
| 7 | 24 | >6 | 65 | 54 | 177 | 173 |
| 8 | 24 | 3–6 | 76 | 47 | 182 | 176 |
| 9 | 25 | >6 | 78 | 54 | 169 | 170 |
| 10 | 26 | >6 | 69 | 72 | 192 | 194 |
| 11 | 30 | 1–3 | 92 | 46 | 160 | 143 |
| 12 | 30 | >6 | 73 | 74 | 172 | 161 |
| 13 | 32 | 1–3 | 65 | 49 | 186 | 182 |
| 14 | 36 | >6 | 75 | 57 | 180 | 171 |
| 15 | 50 | 3–6 | 94 | 41 | 159 | 150 |
| Mean (SD) | 27 (±8) | - | 77 (±8) | 56 (±10) | 174 (±12) | 171 (±16) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogers, B.; Giles, D.; Draper, N.; Mourot, L.; Gronwald, T. Detection of the Anaerobic Threshold in Endurance Sports: Validation of a New Method Using Correlation Properties of Heart Rate Variability. J. Funct. Morphol. Kinesiol. 2021, 6, 38. https://doi.org/10.3390/jfmk6020038
Rogers B, Giles D, Draper N, Mourot L, Gronwald T. Detection of the Anaerobic Threshold in Endurance Sports: Validation of a New Method Using Correlation Properties of Heart Rate Variability. Journal of Functional Morphology and Kinesiology. 2021; 6(2):38. https://doi.org/10.3390/jfmk6020038
Chicago/Turabian StyleRogers, Bruce, David Giles, Nick Draper, Laurent Mourot, and Thomas Gronwald. 2021. "Detection of the Anaerobic Threshold in Endurance Sports: Validation of a New Method Using Correlation Properties of Heart Rate Variability" Journal of Functional Morphology and Kinesiology 6, no. 2: 38. https://doi.org/10.3390/jfmk6020038