TMJ Dysfunctions Systemic Implications and Postural Assessments: A Review of Recent Literature


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Application Protocol and Website Recording Data
2.2. Target Questions
2.3. Search Strategy
2.4. Collection Data
2.5. Manuscript Selections
2.6. Research Classifications
2.7. Exclusion and Inclusion Criteria
- Investigated relations between TMJ dysfunctions and posture of the human body.
- The following exclusion criteria included:
- Not enough information regarding the topic;
- Animal or in vitro studies;
- Articles published prior to 1 February 2009;
- No access to the title and abstract.
2.8. Strategy for Collecting Data
2.9. Record of the Extracted and Collected Data Extraction
2.10. Risk of Bias Assessment
- Selection bias;
- Performance bias and detection bias;
- Attrition bias;
- Reporting bias;
- Examiner blinding, examiner calibration, standardized follow-up description, standardized residual graft measurement and standardized radiographic assessment.
2.11. Occlusion
2.12. Malocclusion
2.13. TMJ Dysfunctions
2.14. Spinal Disease
2.15. Posturology
3. Results
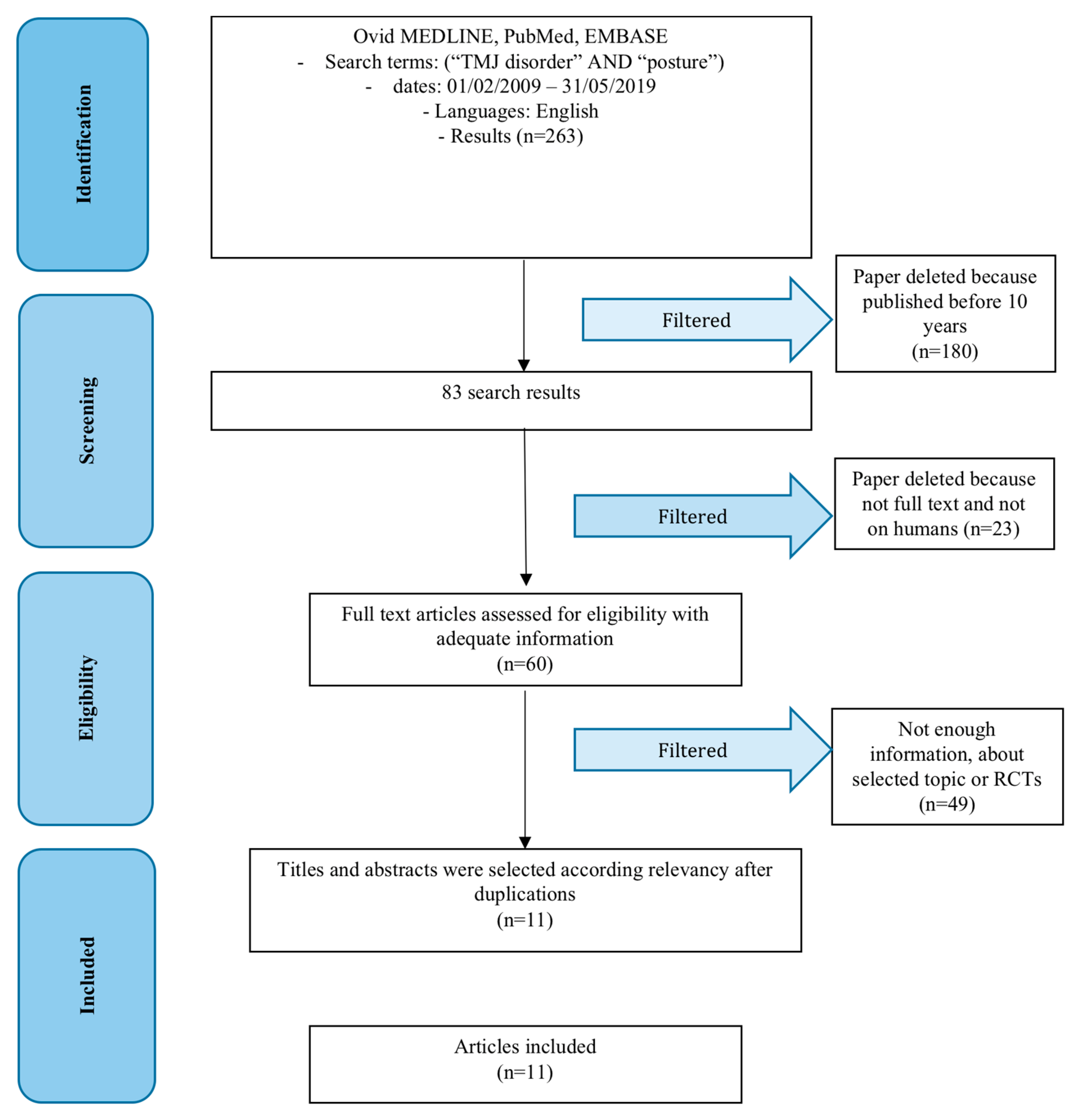
3.1. Study Selection
3.2. Risk of Bias within the Studies
3.3. Synthesis of Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Asbell, M.B. A brief history of orthodontics. Am. J. Orthod. Dentofac. Orthop. 1990, 98, 176–183. [Google Scholar] [CrossRef]
- Ricketts, R.M. Provocations and Perceptions in Cranio-Facial Orthopedics; RMO: Denver, CO, USA, 1989. [Google Scholar]
- Angle, E.H. Malocclusion of the Teeth, 7th ed.; The S.S. White Dental Manufacturing Company: Philadelphia, PA, USA, 1907. [Google Scholar]
- Dolgalev, A.A.; Bragin, E.A. Significance of magnetic resonance tomography and electronic axiography in diagnostics of TMJ dysfunctions. Stomatologiia 2008, 87, 56–60. [Google Scholar]
- Cardonnet, M.; Clauzade, M. Differential diagnosis of TMJ dysfunctions. Cah Prothes. 1987, 15, 125–170. [Google Scholar]
- Ricketts, R.M. Abnormal function of the temporal mandibular joint. Am. J. Orthod. 1955, 41, 435–441. [Google Scholar] [CrossRef]
- Ricketts, R.M. Laminagraphy in the diagnosis of temporomandibular joint disorders. J. Am. Dent. Assoc. 1953, 46, 620–648. [Google Scholar] [CrossRef] [PubMed]
- Hirjak, D.; Machon, V.; Beno, M.; Galis, B.; Kupcova, I. Surgical treatment of condylar head fractures, the way to minimize the postraumatic TMJ ankylosis. Bratisl. Lek. Listy 2017, 118, 17–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, E., 3rd; Walker, R.V. Treatment of Malocclusion and TMJ Dysfunction Secondary to Condylar Fractures. Craniomaxillofac. Trauma Reconstr. 2009, 2, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Zachariades, N.; Mezitis, M.; Mourouzis, C.; Papadakis, D.; Spanou, A. Fractures of the mandibular condyle: A review of 466 cases. Literature review, reflections on treatment and proposals. J. Craniomaxillofac. Surg. 2006, 34, 421–432. [Google Scholar] [CrossRef]
- Rallis, G.; Mourouzis, C.; Ainatzoglou, M.; Mezitis, M.; Zachariades, N. Plate osteosynthesis of condylar fractures: A retrospective study of 45 patients. Quintessence Int. 2003, 34, 45–49. [Google Scholar]
- Defabianis, P. TMJ fractures in children and adolescents: treatment guidelines. J. Clin. Pediatr. Dent. 2003, 27, 191–199. [Google Scholar]
- Choi, B.H.; Yi, C.K.; Yoo, J.H. MRI examination of the TMJ after surgical treatment of condylar fractures. Int. J. Oral Maxillofac. Surg. 2001, 30, 296–299. [Google Scholar] [CrossRef]
- Gupta, S. Surgery: Diverse interventions. Nature 2015, 526, S6–S7. [Google Scholar] [CrossRef]
- Isola, G.; Cicciu, M.; Fiorillo, L.; Matarese, G. Association between Odontoma and Impacted Teeth. J. Craniofac. Surg. 2017, 28, 755–758. [Google Scholar] [CrossRef]
- Laino, L.; Cicciù, M.; Fiorillo, L.; Crimi, S.; Bianchi, A.; Amoroso, G.; Monte, I.P.; Herford, A.S.; Cervino, G. Surgical Risk on Patients with Coagulopathies: Guidelines on Hemophiliac Patients for Oro-Maxillofacial Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1386. [Google Scholar] [CrossRef]
- Rullo, R.; Scalzone, P.; Laino, L.; Russo, A.; Festa, V.M.; Fiorillo, L.; Cicciu, M. Solitary Plasmacytoma of the Mandible: Early Diagnosis and Surgical Management. J. Craniofac. Surg. 2019. [Google Scholar] [CrossRef]
- Cervino, G.; Cicciù, M.; Biondi, A.; Bocchieri, S.; Herford, A.S.; Laino, L.; Fiorillo, L. Antibiotic Prophylaxis on Third Molar Extraction: Systematic Review of Recent Data. Antibiotics 2019, 8, 53. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Monte, I.P.; De Stefano, R.; Laino, L.; Crimi, S.; Bianchi, A.; Herford, A.S.; Biondi, A.; Cicciù, M. Advances in Antiplatelet Therapy for Dentofacial Surgery Patients: Focus on Past and Present Strategies. Materials 2019, 12, 1524. [Google Scholar] [CrossRef]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef]
- Lombardi, T.; Bernardello, F.; Berton, F.; Porrelli, D.; Rapani, A.; Camurri Piloni, A.; Fiorillo, L.; Di Lenarda, R.; Stacchi, C. Efficacy of Alveolar Ridge Preservation after Maxillary Molar Extraction in Reducing Crestal Bone Resorption and Sinus Pneumatization: A Multicenter Prospective Case-Control Study. Biomed. Res. Int. 2018, 2018, 9352130. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Romeo, U.; Bianchi, A.; Crimi, S.; D’Amico, C.; De Stefano, R.; Troiano, G.; Santoro, R.; et al. Molecular Biomarkers Related to Oral Carcinoma: Clinical Trial Outcome Evaluation in a Literature Review. Dis. Markers 2019, 2019, 11. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Savovic, J.; Turner, R.M.; Mawdsley, D.; Jones, H.E.; Beynon, R.; Higgins, J.P.T.; Sterne, J.A.C. Association Between Risk-of-Bias Assessments and Results of Randomized Trials in Cochrane Reviews: The ROBES Meta-Epidemiologic Study. Am. J. Epidemiol. 2018, 187, 1113–1122. [Google Scholar] [CrossRef]
- Whiting, P.; Savovic, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; Group, R. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. Recenti Prog. Med. 2018, 109, 421–431. [Google Scholar] [CrossRef]
- Holzl, M.; Behrmann, R.; Biesinger, E.; von Heymann, W.; Hulse, R.; Goessler, U.R.; Arens, C. Selected ENT symptoms in functional disorders of the upper cervical spine and temporomandibular joints. Hno 2019, 67, 1–9. [Google Scholar] [CrossRef]
- Sperry, M.M.; Ita, M.E.; Kartha, S.; Zhang, S.; Yu, Y.H.; Winkelstein, B. The Interface of Mechanics and Nociception in Joint Pathophysiology: Insights From the Facet and Temporomandibular Joints. J. Biomech. Eng. 2017, 139. [Google Scholar] [CrossRef]
- List, T.; Jensen, R.H. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia Int. J. Headache 2017, 37, 692–704. [Google Scholar] [CrossRef]
- Butts, R.; Dunning, J.; Perreault, T.; Mettille, J.; Escaloni, J. Pathoanatomical characteristics of temporomandibular dysfunction: Where do we stand? (Narrative review part 1). J. Bodyw. Mov. Ther. 2017, 21, 534–540. [Google Scholar] [CrossRef]
- Butts, R.; Dunning, J.; Pavkovich, R.; Mettille, J.; Mourad, F. Conservative management of temporomandibular dysfunction: A literature review with implications for clinical practice guidelines (Narrative review part 2). J. Bodyw. Mov. Ther. 2017, 21, 541–548. [Google Scholar] [CrossRef]
- Costa, Y.M.; Conti, P.C.; de Faria, F.A.; Bonjardim, L.R. Temporomandibular disorders and painful comorbidities: clinical association and underlying mechanisms. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 288–297. [Google Scholar] [CrossRef]
- Gazit, Y.; Jacob, G.; Grahame, R. Ehlers-Danlos Syndrome-Hypermobility Type: A Much Neglected Multisystemic Disorder. Rambam. Maimonides Med. J. 2016, 7. [Google Scholar] [CrossRef]
- Alcantara, J.; Alcantara, J.D.; Alcantara, J. The Chiropractic Care of Infants with Breastfeeding Difficulties. Explore 2015, 11, 468–474. [Google Scholar] [CrossRef]
- Assouan, C.; Anzouan, K.; Nguessan, N.D.; Millogo, M.; Horo, K.; Konan, E.; Zwetyenga, N. Tuberculosis of the temporomandibular joint. Rev. De Stomatol. De Chir. Maxillo-Faciale Et De Chir. Orale 2014, 115, 88–93. [Google Scholar] [CrossRef]
- Munir, S.; Patil, K.; Miller, E.; Uleryk, E.; Twilt, M.; Spiegel, L.; Doria, A.S. Juvenile idiopathic arthritis of the axial joints: a systematic review of the diagnostic accuracy and predictive value of conventional MRI. Ajr. Am. J. Roentgenol. 2014, 202, 199–210. [Google Scholar] [CrossRef]
- Davis, C.G. Mechanisms of chronic pain from whiplash injury. J. Forensic Leg. Med. 2013, 20, 74–85. [Google Scholar] [CrossRef]
- Sambataro, S.; Cervino, G.; Fiorillo, L.; Cicciu, M. Upper First Premolar Positioning Evaluation for the Stability of the Dental Occlusion: Anatomical Considerations. J. Craniofac. Surg. 2018, 29, 1366–1369. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author (Year) | Risk of Bias | |||
|---|---|---|---|---|
| Unclear | Low | Moderate | High | |
| Holtz et al. (2019) [26] | X | |||
| Sperry et al. (2017) [27] | X | |||
| List et al. (2017) [28] | X | |||
| Butts et al. (2017) [29] | X | |||
| Butts et al. (2017) [30] | X | |||
| Costa et al. (2016) [31] | X | |||
| Gazit et al. (2016) [32] | X | |||
| Alcantara et al. (2015) [33] | X | |||
| Assouan et al. (2014) [34] | X | |||
| Munir et al. (2014) [35] | X | |||
| Davis et al. (2013) [36] | X | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sambataro, S.; Cervino, G.; Bocchieri, S.; La Bruna, R.; Cicciù, M. TMJ Dysfunctions Systemic Implications and Postural Assessments: A Review of Recent Literature. J. Funct. Morphol. Kinesiol. 2019, 4, 58. https://doi.org/10.3390/jfmk4030058
Sambataro S, Cervino G, Bocchieri S, La Bruna R, Cicciù M. TMJ Dysfunctions Systemic Implications and Postural Assessments: A Review of Recent Literature. Journal of Functional Morphology and Kinesiology. 2019; 4(3):58. https://doi.org/10.3390/jfmk4030058
Chicago/Turabian StyleSambataro, Sergio, Gabriele Cervino, Salvatore Bocchieri, Rosario La Bruna, and Marco Cicciù. 2019. "TMJ Dysfunctions Systemic Implications and Postural Assessments: A Review of Recent Literature" Journal of Functional Morphology and Kinesiology 4, no. 3: 58. https://doi.org/10.3390/jfmk4030058