Comparison of Dual-Energy X-ray Absorptiometry (DXA) Versus a Multi-Frequency Bioelectrical Impedance (InBody 770) Device for Body Composition Assessment after a 4-Week Hypoenergetic Diet

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Body Composition
2.3. Diet and Exercise
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Antonio, J.; Ellerbroek, A.; Silver, T.; Orris, S.; Scheiner, M.; Gonzalez, A.; Peacock, C.A. A high protein diet (3.4 g/kg/d) combined with a heavy resistance training program improves body composition in healthy trained men and women—A follow-up investigation. J. Int. Soc. Sports Nutr. 2015, 12, 39. [Google Scholar] [CrossRef]
- Antonio, J.; Ellerbroek, A.; Silver, T.; Vargas, L.; Peacock, C. The effects of a high protein diet on indices of health and body composition—A crossover trial in resistance-trained men. J. Int. Soc. Sports Nutr. 2016, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Antonio, J.; Peacock, C.A.; Ellerbroek, A.; Fromhoff, B.; Silver, T. The effects of consuming a high protein diet (4.4 g/kg/d) on body composition in resistance-trained individuals. J. Int. Soc. Sports Nutr. 2014, 11, 19. [Google Scholar] [CrossRef]
- Aragon, A.A.; Schoenfeld, B.J.; Wildman, R.; Kleiner, S.; VanDusseldorp, T.; Taylor, L.; Earnest, C.P.; Arciero, P.J.; Wilborn, C.; Kalman, D.S.; et al. International society of sports nutrition position stand: Diets and body composition. J. Int. Soc. Sports Nutr. 2017, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Cholewa, J.M.; Hudson, A.; Cicholski, T.; Cervenka, A.; Barreno, K.; Broom, K.; Barch, M.; Craig, S.A.S. The effects of chronic betaine supplementation on body composition and performance in collegiate females: A double-blind, randomized, placebo controlled trial. J. Int. Soc. Sports Nutr. 2018, 15, 37. [Google Scholar] [CrossRef] [PubMed]
- Escalante, G.; Alencar, M.; Haddock, B.; Harvey, P. The effects of phosphatidic acid supplementation on strength, body composition, muscular endurance, power, agility, and vertical jump in resistance trained men. J. Int. Soc. Sports Nutr. 2016, 13, 24. [Google Scholar] [CrossRef] [PubMed]
- Lopez, H.L.; Ziegenfuss, T.N.; Hofheins, J.E.; Habowski, S.M.; Arent, S.M.; Weir, J.P.; Ferrando, A.A. Eight weeks of supplementation with a multi-ingredient weight loss product enhances body composition, reduces hip and waist girth, and increases energy levels in overweight men and women. J. Int. Soc. Sports Nutr. 2013, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J.; Aragon, A.A.; Wilborn, C.D.; Krieger, J.W.; Sonmez, G.T. Body composition changes associated with fasted versus non-fasted aerobic exercise. J. Int. Soc. Sports Nutr. 2014, 11, 54. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.M.; Pierson, R.N. Jr.; Heymsfield, S.B. The five-level model: A new approach to organizing body-composition research. Am. J. Clin. Nutr. 1992, 56, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.M.; Ma, R.; Pierson, R.N., Jr.; Heymsfield, S.B. Five-level model: Reconstruction of body weight at atomic, molecular, cellular, and tissue-system levels from neutron activation analysis. Basic. Life Sci. 1993, 60, 125–128. [Google Scholar] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fieding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. The authors reply: Letter on: “Pitfalls in the measurement of muscle mass: A need for a reference standard” by Clark et al. J. Cachexia Sarcopenia Muscle 2018, 9, 1272–1274. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Shaw, K.A.; Srikanth, V.K.; Fryer, J.L.; Blizzard, L.; Dwyer, T.; Venn, A.J. Dual energy X-ray absorptiometry body composition and aging in a population-based older cohort. Int. J. Obes (Lond.) 2007, 31, 279–284. [Google Scholar] [CrossRef]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef] [PubMed]
- Wingo, B.C.; Barry, V.G.; Ellis, A.C.; Gower, B.A. Comparison of segmental body composition estimated by bioelectrical impedance analysis and dual-energy X-ray absorptiometry. Clin. Nutr. ESPEN 2018, 28, 141–147. [Google Scholar] [CrossRef]
- Stone, T.M.; Wingo, J.E.; Nickerson, B.S.; Esco, M.R. Comparison of Bioelectrical Impedance Analysis and Dual-Energy X-Ray Absorptiometry for Estimating Bone Mineral Content. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J.; Nickerson, B.S.; Wilborn, C.D.; Urbina, S.L.; Hayward, S.B.; Krieger, J.; Aragon, A.A.; Tinsley, G.M. Comparison of Multifrequency Bioelectrical Impedance vs. Dual-Energy X-ray Absorptiometry for Assessing Body Composition Changes After Participation in a 10-Week Resistance Training Program. J. Strength Cond. Res. 2018. [Google Scholar] [CrossRef]
- Demura, S.; Sato, S.; Kitabayashi, T. Percentage of total body fat as estimated by three automatic bioelectrical impedance analyzers. J. Physiol. Anthropol. Appl. Hum. Sci. 2004, 23, 93–99. [Google Scholar] [CrossRef]
- Ramirez-Velez, R.; Tordecilla-Sanders, A.; Correa-Bautista, J.E.; Gonzalez-Ruiz, K.; Gonzalez-Jimenez, E.; Triana-Reina, H.R.; Garcia-Hermoso, A.; Schmidt-RioValle, J. Validation of multi-frequency bioelectrical impedance analysis versus dual-energy X-ray absorptiometry to measure body fat percentage in overweight/obese Colombian adults. Am. J. Hum. Biol. 2018, 30. [Google Scholar] [CrossRef]
- Moon, J.R. Body composition in athletes and sports nutrition: An examination of the bioimpedance analysis technique. Eur. J. Clin. Nutr. 2013, 67, S54–S59. [Google Scholar] [CrossRef] [PubMed]
- Gaba, A.; Kapus, O.; Cuberek, R.; Botek, M. Comparison of multi- and single-frequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for assessment of body composition in post-menopausal women: Effects of body mass index and accelerometer-determined physical activity. J. Hum. Nutr. Diet. 2015, 28, 390–400. [Google Scholar] [CrossRef]
- Faria, S.L.; Faria, O.P.; Cardeal, M.D.; Ito, M.K. Validation study of multi-frequency bioelectrical impedance with dual-energy X-ray absorptiometry among obese patients. Obes. Surg. 2014, 24, 1476–1480. [Google Scholar] [CrossRef] [PubMed]
- Volgyi, E.; Tylavsky, F.A.; Lyytikainen, A.; Suominen, H.; Alen, M.; Cheng, S. Assessing body composition with DXA and bioimpedance: Effects of obesity, physical activity, and age. Obesity (Silver Spring) 2008, 16, 700–705. [Google Scholar] [CrossRef]
- Sillanpaa, E.; Hakkinen, A.; Hakkinen, K. Body composition changes by DXA, BIA and skinfolds during exercise training in women. Eur. J. Appl. Physiol. 2013, 113, 2331–2341. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, V.; Voci, S.M.; Mendes-Netto, R.S.; da Silva, D.G. The relative validity of a food record using the smartphone application MyFitnessPal. Nutr. Diet. 2018, 75, 219–225. [Google Scholar] [CrossRef]
- Esco, M.R.; Snarr, R.L.; Leatherwood, M.D.; Chamberlain, N.A.; Redding, M.L.; Flatt, A.A.; Moon, J.R.; Williford, H.N. Comparison of total and segmental body composition using DXA and multifrequency bioimpedance in collegiate female athletes. J. Strength Cond. Res. 2015, 29, 918–925. [Google Scholar] [CrossRef]
- Nascimento, M.A.; Silva, D.R.P.; Ribeiro, A.S.; Pina, F.L.C.; Gerage, A.M.; Gobbo, L.A.; Mayhew, J.L.; Cyrino, E.S. Agreement Between Bioelectrical Impedance and Dual-Energy X-Ray Absorptiometry to Track Changes in Fat-Free Mass After Resistance Training in Older Women. J. Strength Cond. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Karelis, A.D.; Chamberland, G.; Aubertin-Leheudre, M.; Duval, C. Ecological mobility in A, Parkinson g: Validation of a portable bioelectrical impedance analyzer for the assessment of body composition. Appl. Physiol. Nutr. Metab. 2013, 38, 27–32. [Google Scholar] [CrossRef]
- Anderson, L.J.; Erceg, D.N.; Schroeder, E.T. Utility of multifrequency bioelectrical impedance compared with dual-energy x-ray absorptiometry for assessment of total and regional body composition varies between men and women. Nutr. Res. 2012, 32, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Sami, N.; Sweeney, F.C.; Dieli-Conwright, C.M. Body Composition with Dual-Energy X-Ray Absorptiometry and Bioelectrical Impedance Analysis in Breast Cancer Survivors. Nutr. Clin. Pract. 2018. [Google Scholar] [CrossRef]
- Piatti, P.M.; Monti, F.; Fermo, I.; Baruffaldi, L.; Nasser, R.; Santambrogio, G.; Librenti, M.C.; Galli-Kienle, M.; Pontiroli, A.E.; Pozza, G. Hypocaloric high-protein diet improves glucose oxidation and spares lean body mass: Comparison to hypocaloric high-carbohydrate diet. Metabolism 1994, 43, 1481–1487. [Google Scholar] [CrossRef]
- Wycherley, T.P.; Brinkworth, G.D.; Clifton, P.M.; Noakes, M. Comparison of the effects of 52 weeks weight loss with either a high-protein or high-carbohydrate diet on body composition and cardiometabolic risk factors in overweight and obese males. Nutr. Diabetes 2012, 2, e40. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.R.; Eckerson, J.M.; Tobkin, S.E.; Smith, A.E.; Lockwood, C.M.; Walter, A.A.; Cramer, J.T.; Beck, T.W.; Stout, J.R. Estimating body fat in NCAA Division I female athletes: A five-compartment model validation of laboratory methods. Eur. J. Appl. Physiol. 2009, 105, 119–130. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | 33 ± 10 |
| Height (centimeters) | 169 ± 8 |
| Average hours of aerobic training per week | 5.3 ± 4.2 |
| Average hours of resistance training per week | 4.2 ± 2.7 |
| Average hours of training of other non-traditional exercise (e.g., pilates, yoga) | 2.4 ± 4.2 |
| Average years of exercise training | 13.3 ± 6.1 |
| Pre | Post | p-Value Pre vs. Post | |
|---|---|---|---|
| Energy (kcal) | 1943 ± 555 | 1580 ± 429 | <0.0001 |
| Protein (g) | 130 ± 49 | 140 ± 43 | 0.0907 |
| Carbohydrate (g) | 202 ± 73 | 140 ± 64 | <0.0001 |
| Fat (g) | 68 ± 24 | 51 ± 18 | <0.0001 |
| Energy (kcal/kg/d) | 28 ± 8 | 23 ± 6 | <0.0001 |
| Protein (g/kg/d) | 1.9 ± 0.7 | 2.0 ± 0.6 | 0.0443 |
| Carbohydrate (g/kg/d) | 2.9 ± 1.0 | 2.0 ± 1.0 | <0.0001 |
| Fat (g/kg/d) | 1.0 ± 0.3 | 0.7 ± 0.2 | <0.0001 |
| Pre | Post | p-Value Pre vs. Post | Change | |
|---|---|---|---|---|
| DXA Body Weight (kg) | 71.3 ± 13.3 | 70.2 ± 13.1 | <0.0001 | −1.3 ± 1.3 |
| InBody Body Weight (kg) | 71.6 ± 12.9 | 70.4 ± 12.8 | <0.0001 | −1.1 ± 1.3 |
| p-value for DXA vs. InBody | 0.1351 | <0.0001 | 0.0543 | |
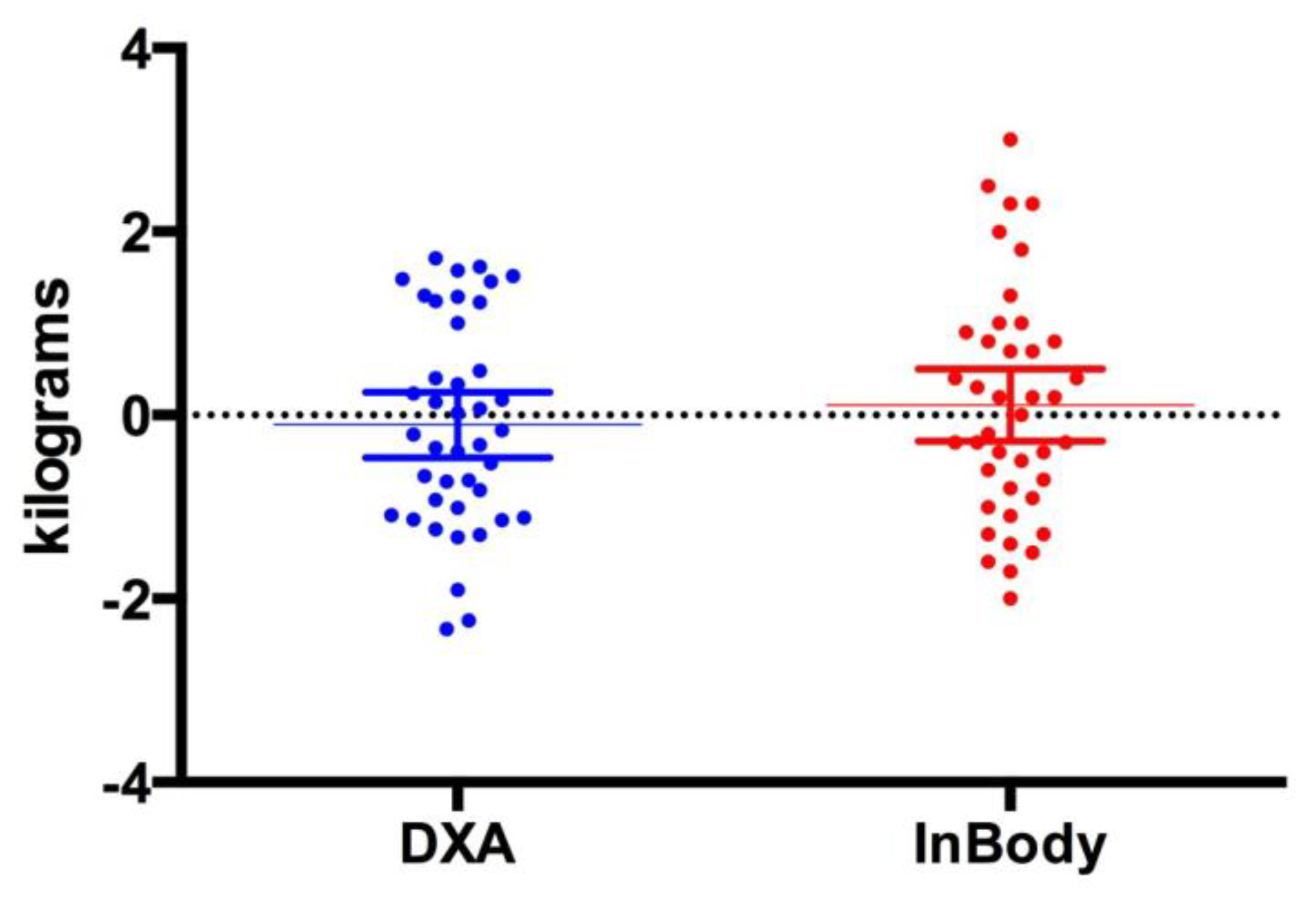
| DXA Fat-free mass (kg) | 52.6 ±10.3 | 52.4 ± 10.1 | 0.5508 | −0.1 ± 1.1 |
| InBody Fat-free mass (kg) | 55.5 ± 11.3 | 55.6 ± 11.0 | 0.5765 | 0.1 ± 1.3 |
| p-value for DXA vs. InBody | <0.0001 | <0.0001 | 0.2271 | |
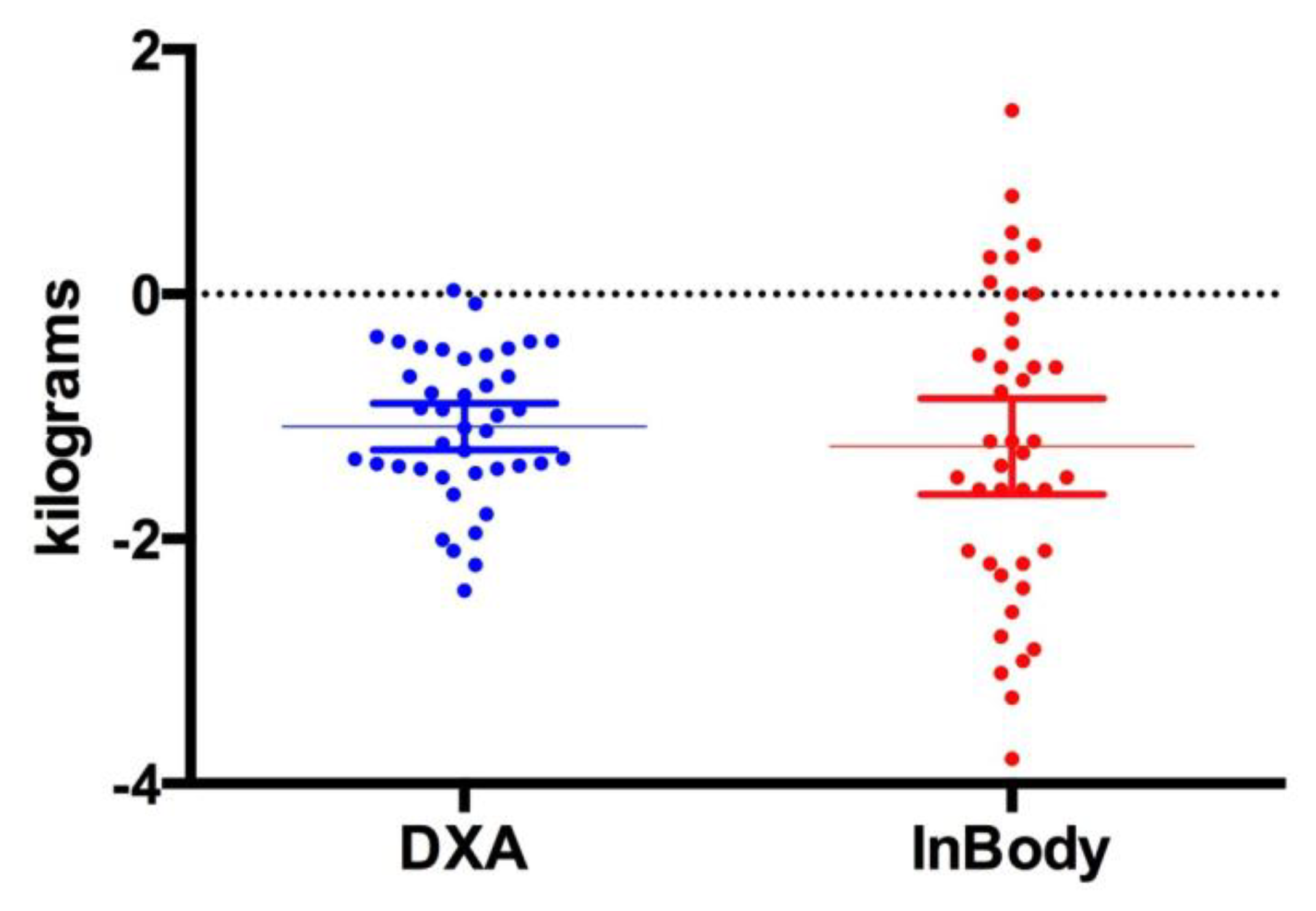
| DXA Fat Mass (kg) | 18.9 ± 6.3 | 17.8 ± 6.3 | <0.0001 | −1.1 ± 0.6 |
| InBody Fat Mass (kg) | 16.1 ± 6.3 | 14.8 ± 6.4 | <0.0001 | −1.2 ± 1.2 |
| p-value for DXA vs. InBody | <0.0001 | <0.0001 | 0.3622 | |
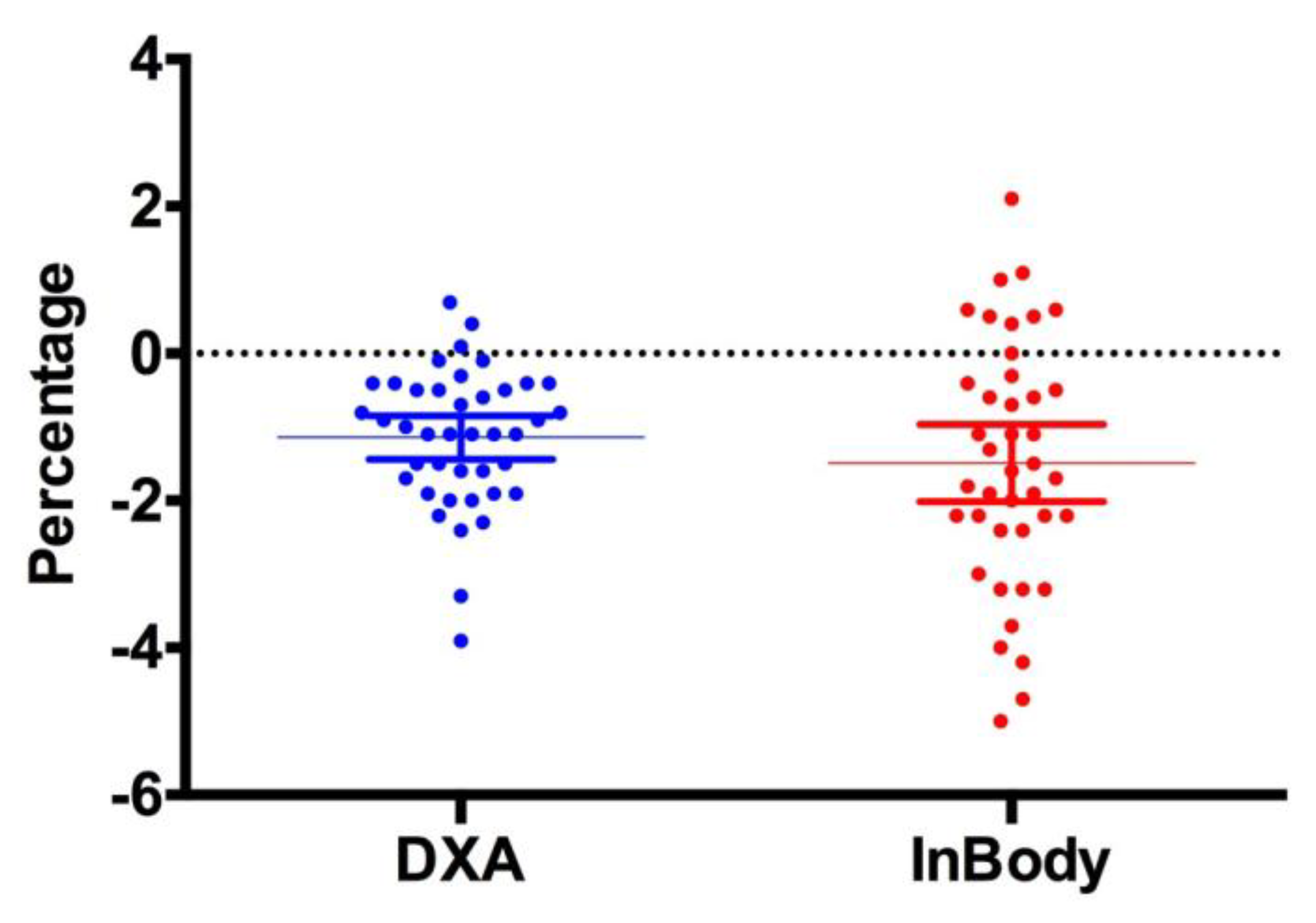
| DXA Body Fat Percent (%) | 26.4 ± 6.4 | 25.2 ± 6.4 | <0.0001 | −1.1 ± 0.9 |
| InBody Body Fat Percent (%) | 22.5 ± 7.5 | 21.0 ± 7.5 | 0.0001 | −1.5 ± 1.7 |
| p-value for DXA vs. InBody | <0.0001 | <0.0001 | 0.1783 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonio, J.; Kenyon, M.; Ellerbroek, A.; Carson, C.; Burgess, V.; Tyler-Palmer, D.; Mike, J.; Roberts, J.; Angeli, G.; Peacock, C. Comparison of Dual-Energy X-ray Absorptiometry (DXA) Versus a Multi-Frequency Bioelectrical Impedance (InBody 770) Device for Body Composition Assessment after a 4-Week Hypoenergetic Diet. J. Funct. Morphol. Kinesiol. 2019, 4, 23. https://doi.org/10.3390/jfmk4020023
Antonio J, Kenyon M, Ellerbroek A, Carson C, Burgess V, Tyler-Palmer D, Mike J, Roberts J, Angeli G, Peacock C. Comparison of Dual-Energy X-ray Absorptiometry (DXA) Versus a Multi-Frequency Bioelectrical Impedance (InBody 770) Device for Body Composition Assessment after a 4-Week Hypoenergetic Diet. Journal of Functional Morphology and Kinesiology. 2019; 4(2):23. https://doi.org/10.3390/jfmk4020023
Chicago/Turabian StyleAntonio, Jose, Madaline Kenyon, Anya Ellerbroek, Cassandra Carson, Victoria Burgess, Denvyr Tyler-Palmer, Jonathan Mike, Justin Roberts, Gerseli Angeli, and Corey Peacock. 2019. "Comparison of Dual-Energy X-ray Absorptiometry (DXA) Versus a Multi-Frequency Bioelectrical Impedance (InBody 770) Device for Body Composition Assessment after a 4-Week Hypoenergetic Diet" Journal of Functional Morphology and Kinesiology 4, no. 2: 23. https://doi.org/10.3390/jfmk4020023