2.1. A Brief Description of Nurse
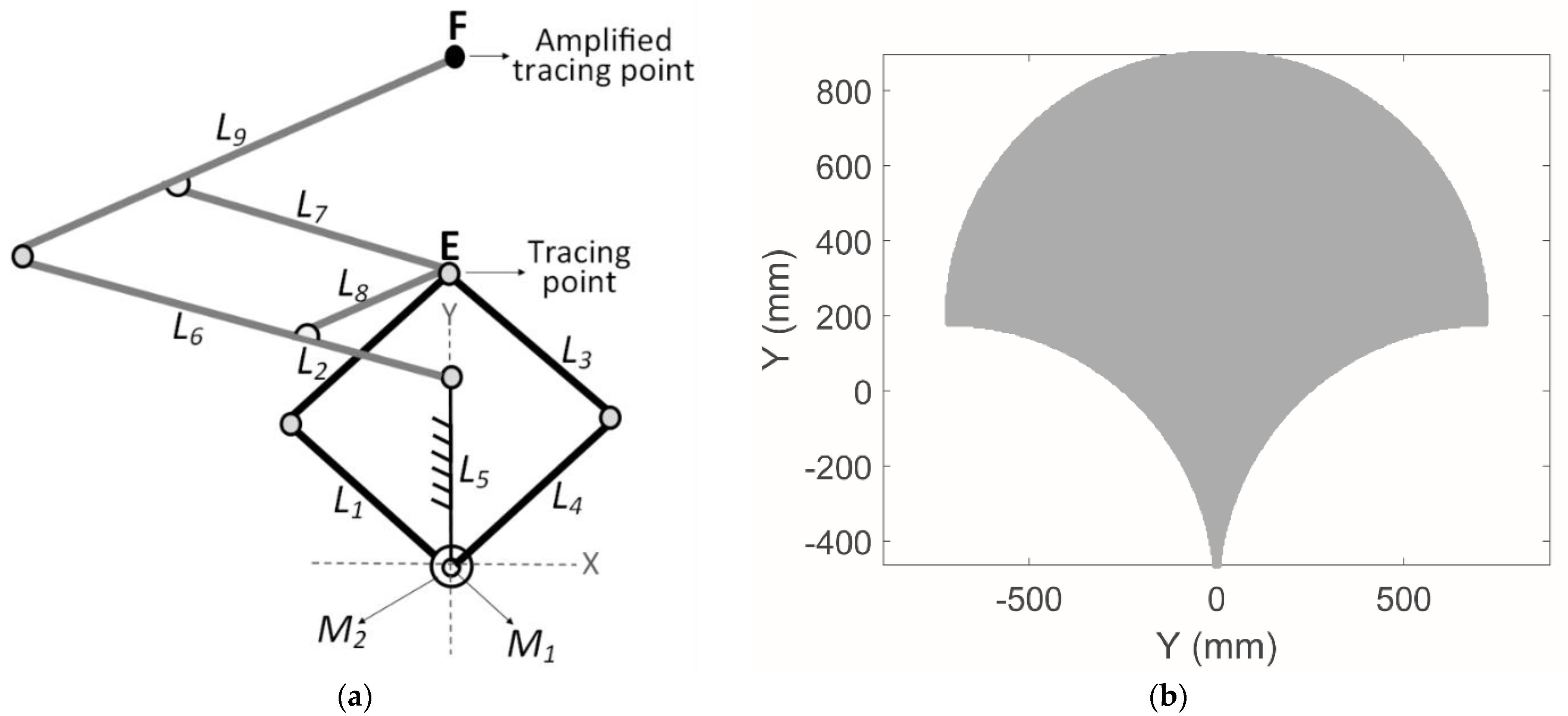
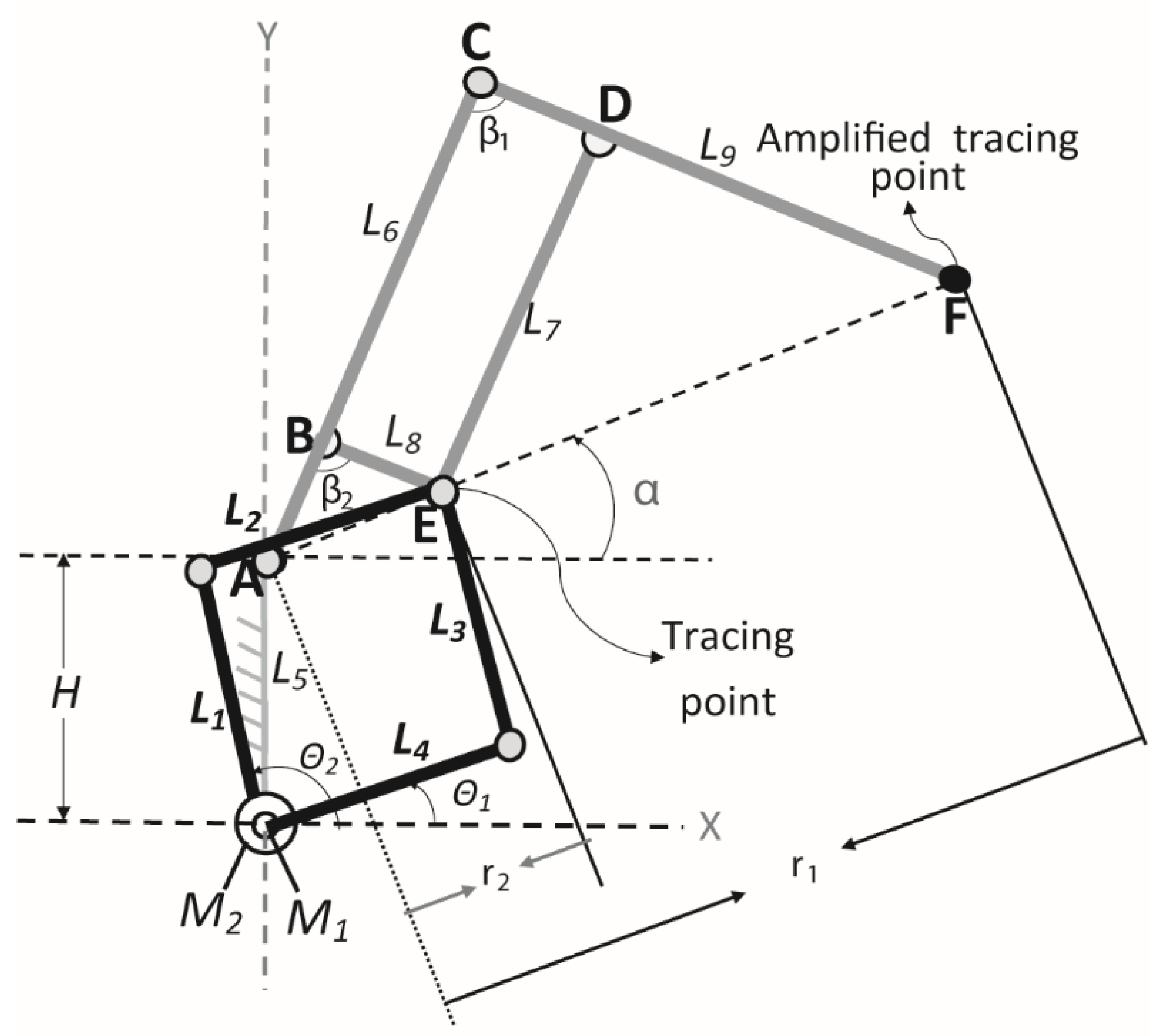
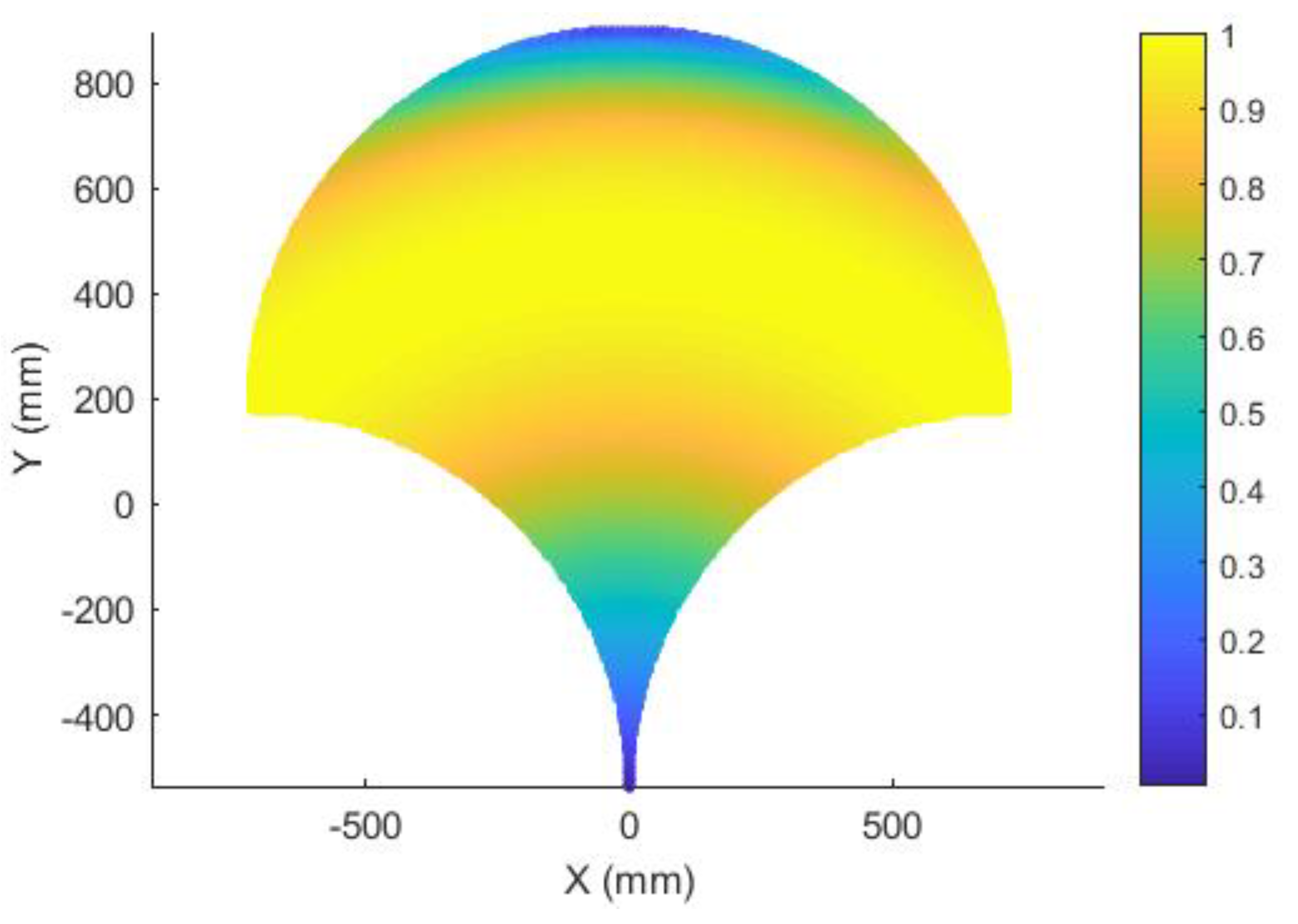
Figure 1a shows a scheme of the Nurse device and
Figure 1b shows its workspace. The mechanism is composed by mobile links
L1,
L2,
L3,
L4,
L6,
L7,
L8,
L9 and fixed link
L5. The point
E, in
Figure 1a, is a tracing point that is follow by the tracing point
F with an amplification scale of 4. The mechanism has two active joints actuated by motors
M1 and
M2.
Nurse was numerically characterized in [
25] and a lab prototype was experimentally characterized in [
26]. In [
25], the authors showed, through a dynamic analysis and an FEM analysis (finite element analysis), that Nurse is a feasible device for arm rehabilitation. In [
26], the authors showed, through an experimental characterization, that Nurse is capable of reproducing different rehabilitation exercises.
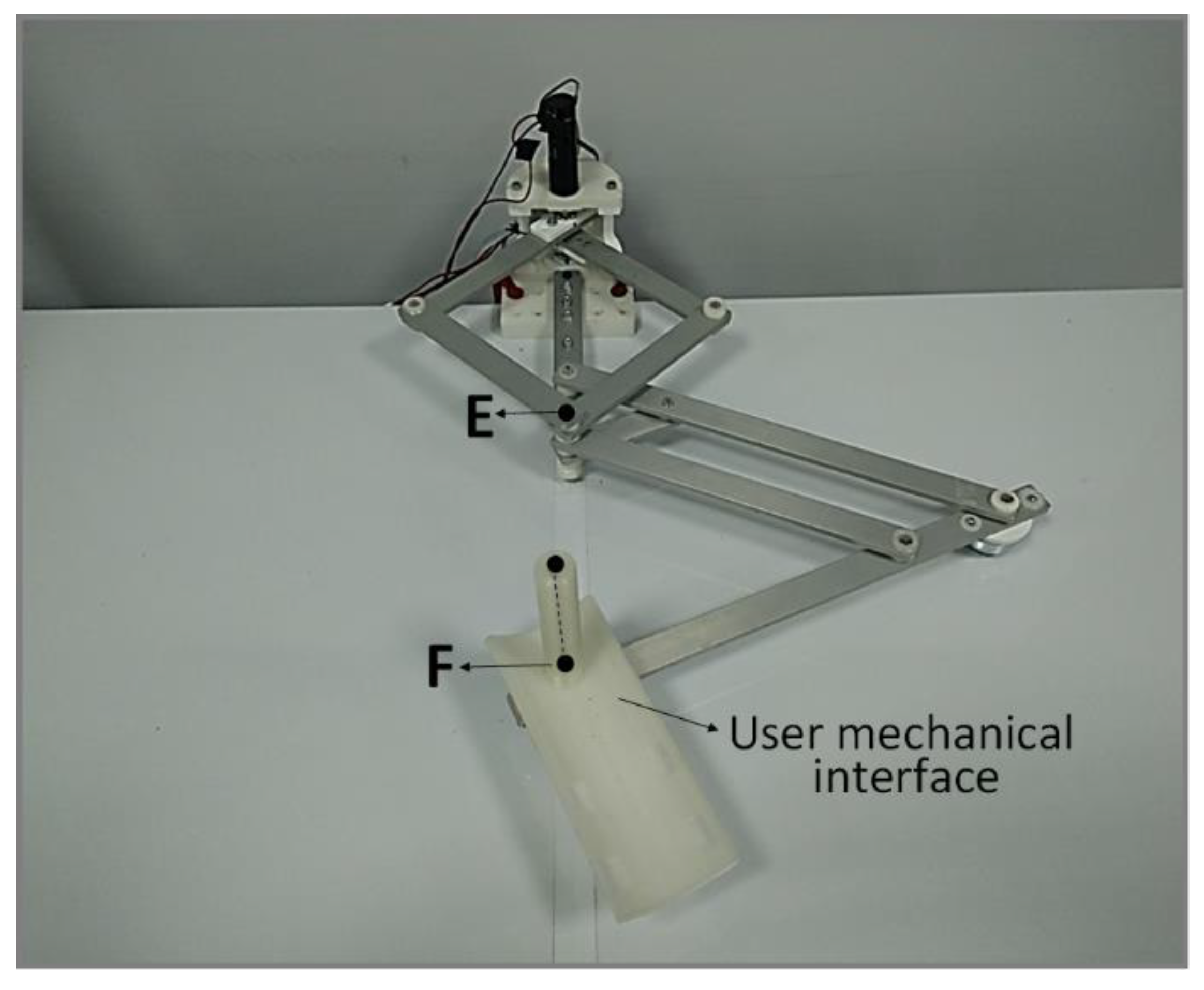
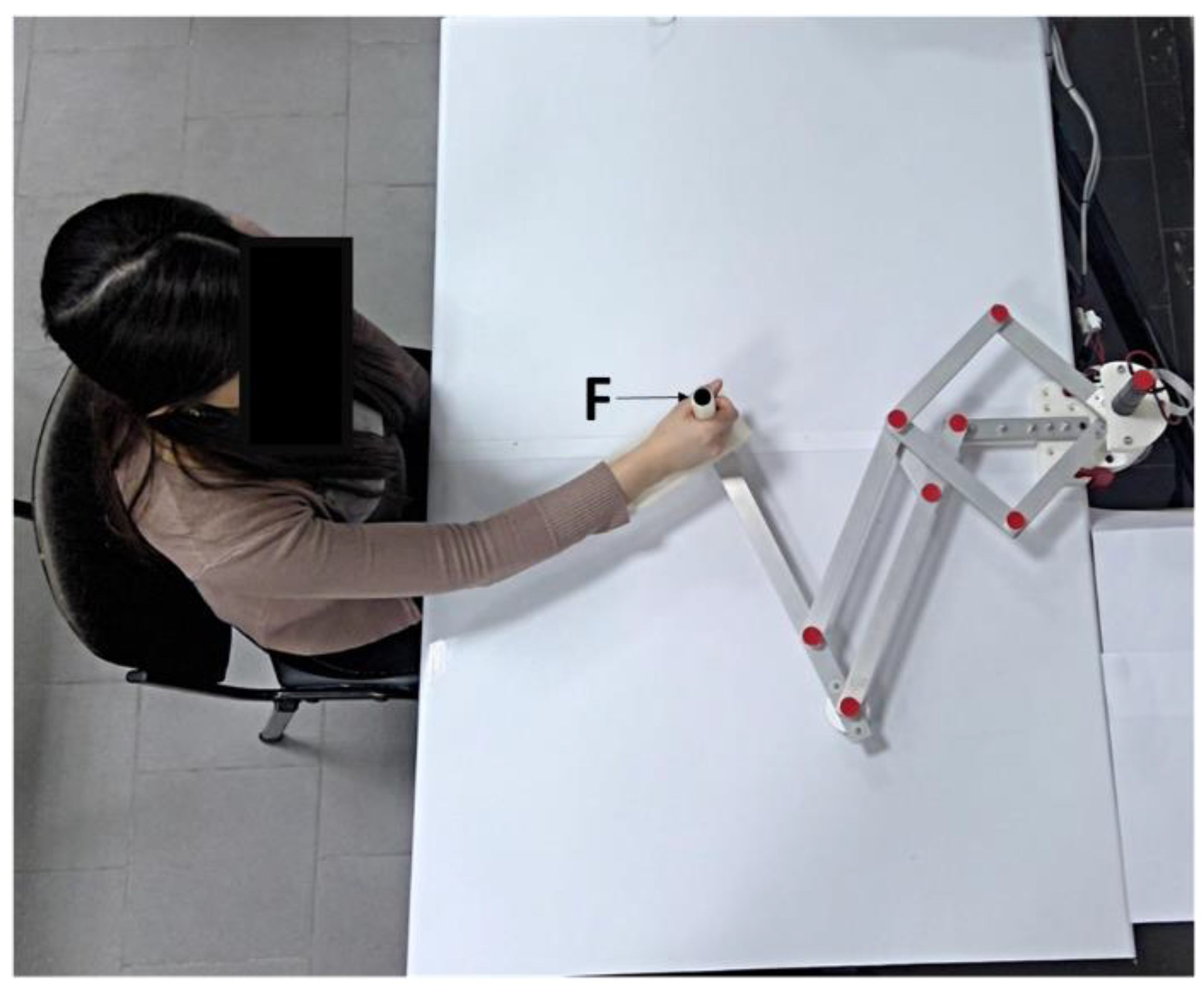
Figure 2 shows a lab prototype of Nurse and
Figure 3 illustrates the user–mechanism interaction. The mechanism structure of Nurse weighs 2.6 kg and fits into a box of 35 × 45 × 30 cm when it is in a contracted position [
25,
26]. The planar mechanism linkage of Nurse is supported by two wheels that are placed under the tracing point
E and the amplified tracing point
F. The trajectory of the user mechanical interface is defined by the amplified tracing point
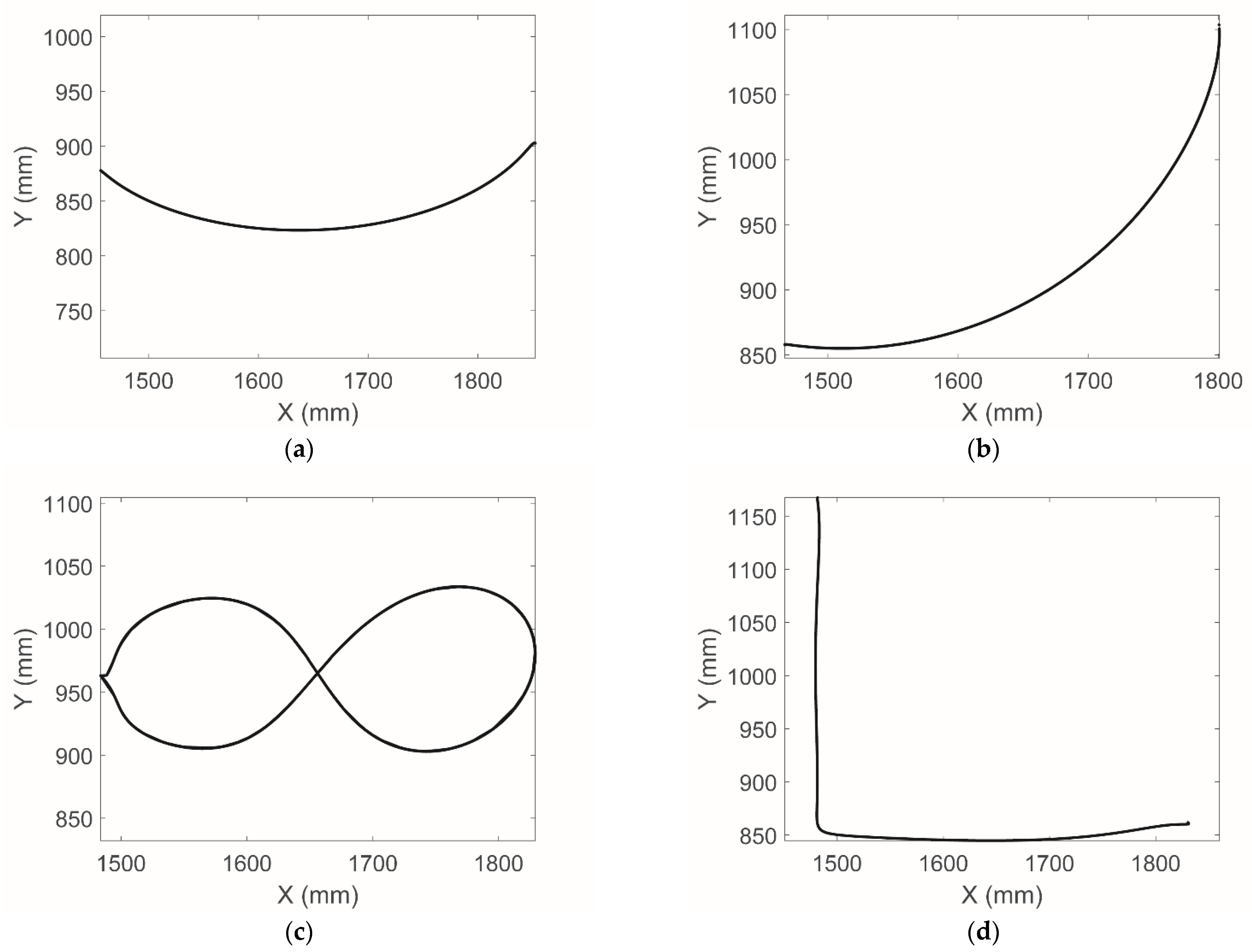
F. Nurse is capable of reproducing different trajectories for upper limb rehabilitation on a plane, including the trajectories for arm rehabilitation designed by the authors in [
23], see
Figure 4.
Figure 4 shows four arm rehabilitation trajectories that were used for the experimental characterization of Nurse in [
26]. In
Figure 4, Trajectory 1 exercises the shoulder joint, Trajectory 2 the exercises the elbow joint, and Trajectory 3 and 4 exercise the elbow and shoulder joint at the same time. Although Nurse has several safety features, such as digital and physical emergency buttons, over current protections and the possibility of remembering the trajectories customized by the therapist for a particular patient, further safety analysis should be performed before experimenting with humans. Furthermore, a characterization of the workspace based on a transmission index is required for a better device performance.
2.2. Performance Analysis
To ensure safe and efficient use of the Nurse device, the torque of the actuators needs to be transmitted to the operator’s arm with a smooth and controlled behavior. While a safe behavior is intrinsic to mechanisms with compliant elements or driven by flexible tendons [
28], rigid-link mechanisms such as Nurse require a careful motion planning and force transmission analysis [
29]. Since the pantograph mechanism only amplifies the behavior of the actuated 5-bar linkage that generates the motion, the critical components for force transmission are links L
1 and L
4, as the two links that are directly actuated by the rotational motors, and L
1 and L
4, which transmit motion from the motors to path generating point E, as per
Figure 1.
From a kinematic point of view, Nurse is characterized by two degrees of freedom actuated by two coaxial rotational motors (M
1 and M
2 in
Figure 1), which directly define the motion of point E that is then amplified in point F by the pantograph. Thus, the architecture of the 5-bar linkage is characteristic of planar parallel mechanisms, with two independently actuated limbs (first limb:
L1 to
L2, second limb:
L4 to
L3) that converge in point
E. As reported in [
25], the motion of point
E can be described as:
where the geometrical parameter H = L
1 = L
2 = L
3 = L
4 = L
5 is fixed, and the angles
and
represent the actuation of M
1 and M
2, respectively. The position of point E can be defined by an angle
, as illustrated in
Figure 5, which can be evaluated as:
and a distance
r2, which can be computed from Equations (1) and (2) as:
The forward kinematics of the full mechanism (up to point
F) can be then obtained from the distance
r1 from the amplification factor of the pantograph
k as:
The position of point
F is thus given as:
This structure results in a non-linear relationship between the torques in the actuators and the force transmitted to point
E (and, through that, to the extremity of the pantograph
F). For this reason, an analysis of the performance of the 5-bar linkage is here proposed to characterize the transmission behavior of Nurse. The Transmission Index (TI) quantifies the relationship between the transmission wrench screw and the output twist screw, as explained by Chen and Angeles in [
30]. The TI is widely recognized as one of the best indices to evaluate the static performance of parallel mechanisms [
31] and to analyze their behavior in their reachable workspace [
32], as singularities can be identified from discontinuities and null values for the TI. Some examples of applying the TI to parallel architectures are reported in [
33,
34,
35]. In particular, the procedure developed in [
34,
35] is adopted in this research to evaluate the TI, with reference to the kinematic scheme of the motion-generating 5-bar linkage of Nurse in
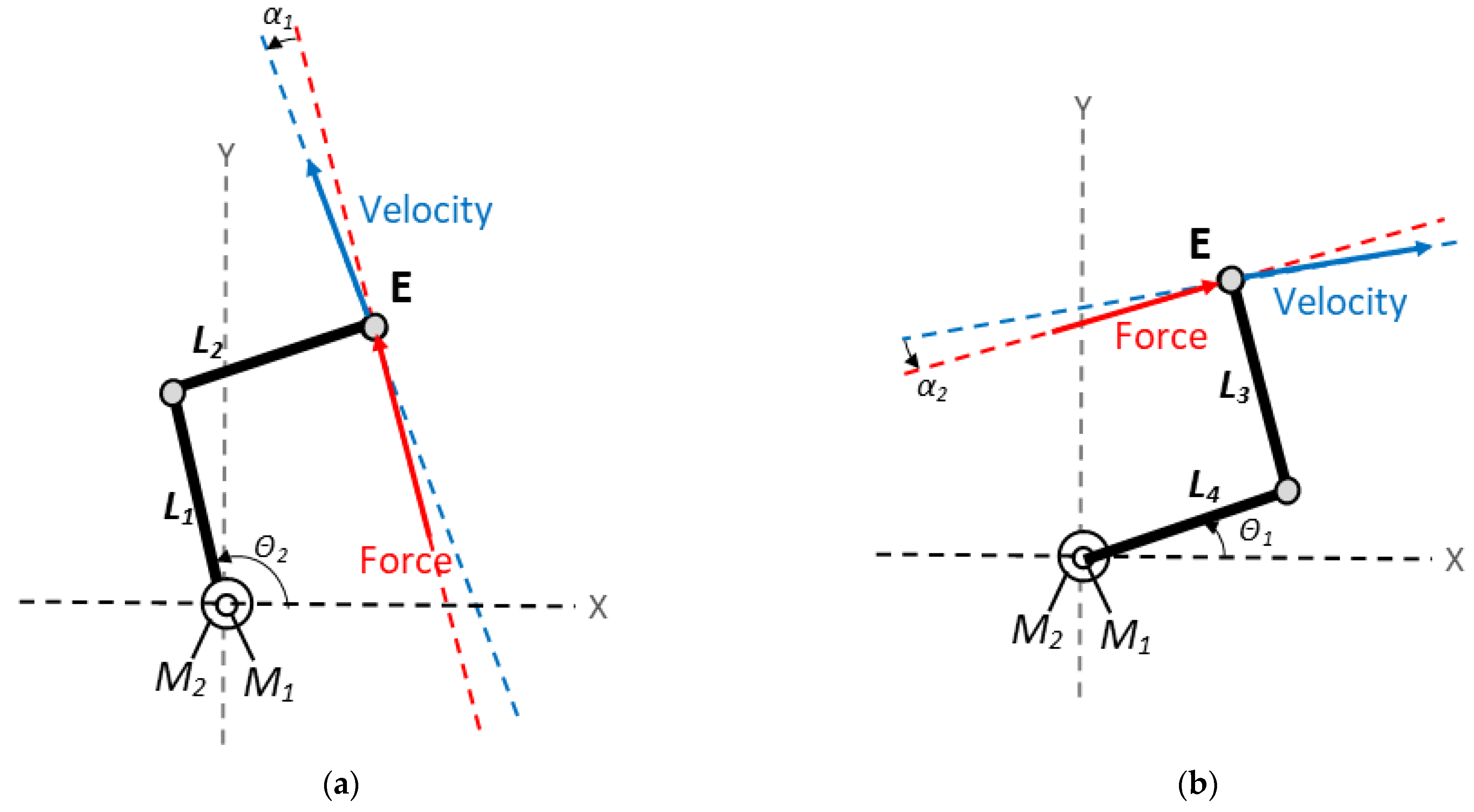
Figure 6. This procedure requires the determination of a pressure angle
, which is defined as the angle the direction of the force applied to a link and the resulting motion and can be evaluated for each degree of freedom of the mechanism with the following steps:
Locking the actuators of all the limbs of the parallel mechanism except for the one corresponding to the degree of freedom under analysis (limb i).
Substituting the non-locked actuator and its limb with the corresponding unit force transmitted to the end-effector.
Evaluating the instantaneous velocity corresponding to the motion of the end-effector resulting from the unit force applied in the previous point.
The pressure angle
, relative to limb
i and obtained as the angle between the force of point 2 and the velocity of point 3, can be used to obtain the force transmission efficiency
in that limb as:
After evaluating
for each limb, the output transmission index of the mechanism can be determined as:
In Nurse’s 5-bar linkage, the links L2 and L3 can only transmit forces along the link’s direction under the assumption of static balance with negligible friction and inertial effects. Thus, the direction of the unit force that these links can transmit to the end-effector is defined by the orientation of the link itself, which is for link L2 (always parallel to input link L4) and for link L3 (always parallel to input link L1).
When one of the parallel limbs of the 5-bar linkage is removed and the remaining actuator motion fixed, the only movable limb is L2 if removing the limb defined by L4 and L3, or L3 if removing the limb defined by L1 and L2. These movable limbs can only rotate around the revolute joints that connect them to their respective input links, resulting in an instantaneous velocity that is normal to the orientation of the link. Thus, the instantaneous velocity obtained when removing the limb defined by L4 and L3 is defined by an orientation of , whereas the instantaneous velocity obtained when removing the limb defined by L1 and L2 is defined by an orientation of .
Thus, the pressure angles corresponding to these two cases are:
From Equation (10), the pressure angles are always equal in modulus (even if their sign can vary, depending on how they were defined). This means that the efficiency of the two limbs, defined as
as per Equation (8), is always the same due to the symmetry of the system. Therefore, the TI of the system in a given configuration can be computed as:
2.3. Operation Safety
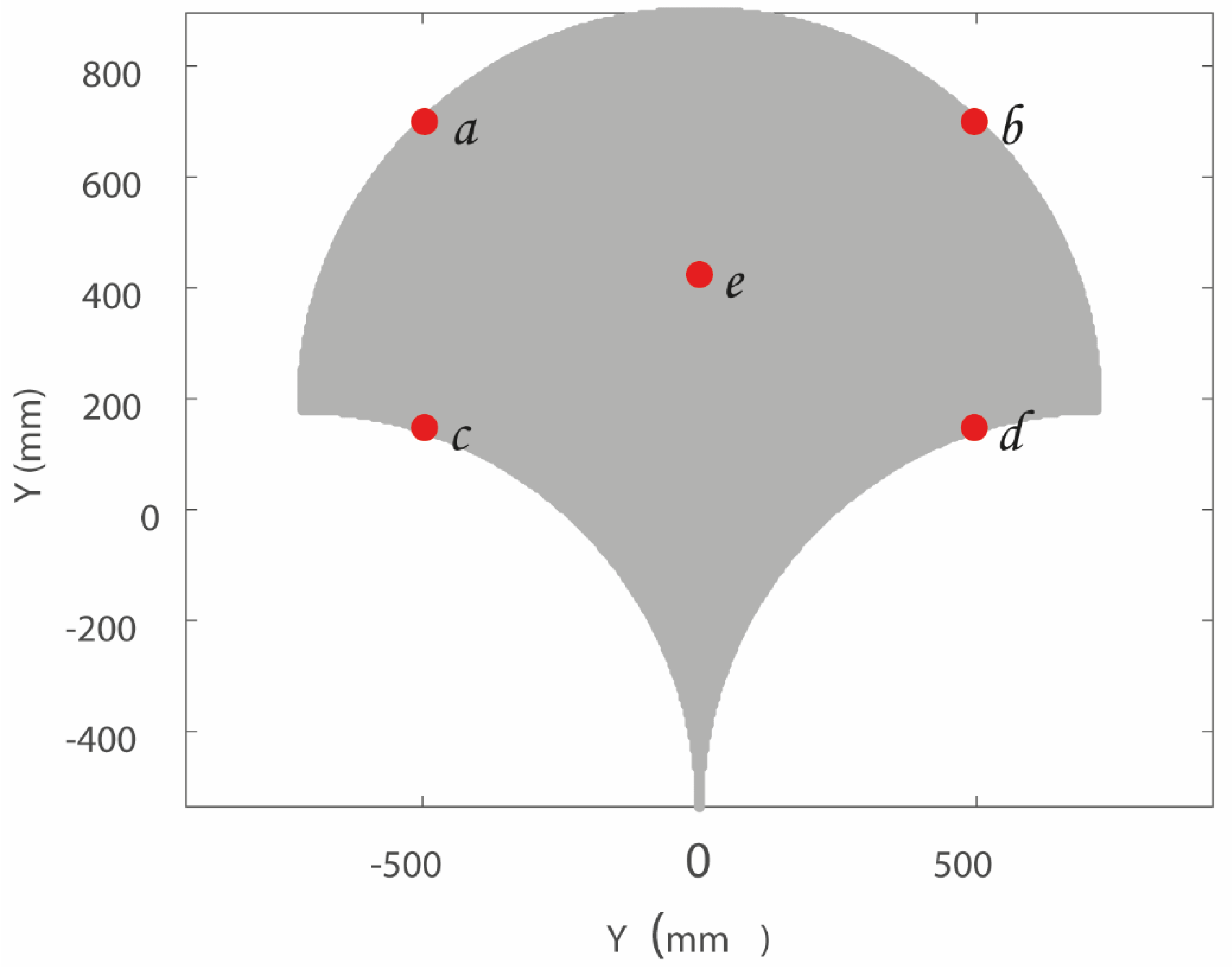
A linear static FEM (finite element method) analysis has been performed in order to assess the produced stress on the human arm when Nurse device reaches critical positions within its workspace. Five critical positions within a mechanism workspace can be chosen by tracing an imaginary rectangle covering most of the workspace (Norm ISO 9283 [
36]). The central point and the four corners of the imaginary rectangle are five critical positions.
Figure 7 shows five critical positions within the Nurse workspace, where point
a, point
b, point
c, and point
d are the corners of the imaginary rectangle and point
e is the central point of the rectangle.
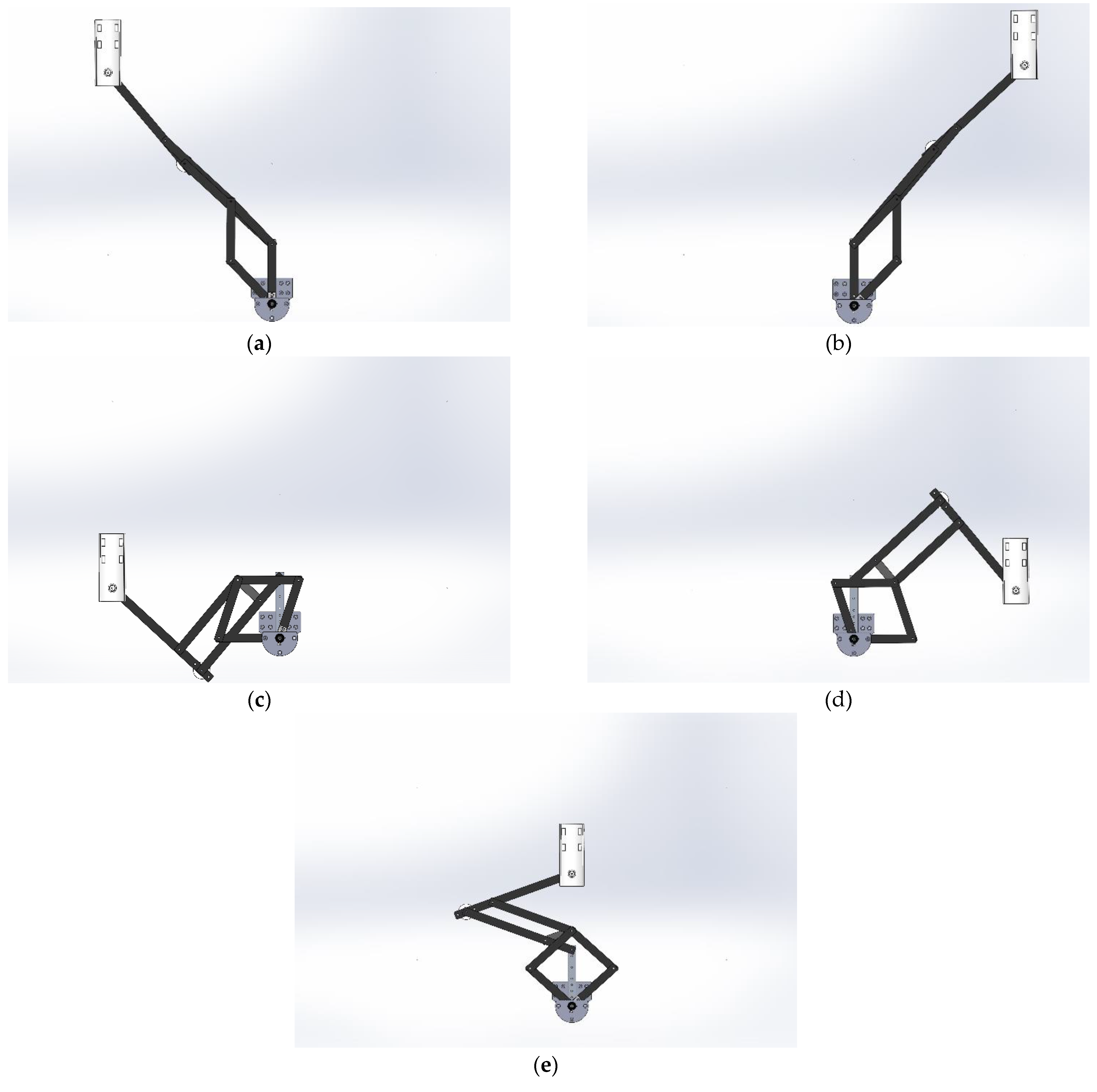
Figure 8 shows a CAD (computer-aided design) of the Nurse device that emulates the real lab prototype.
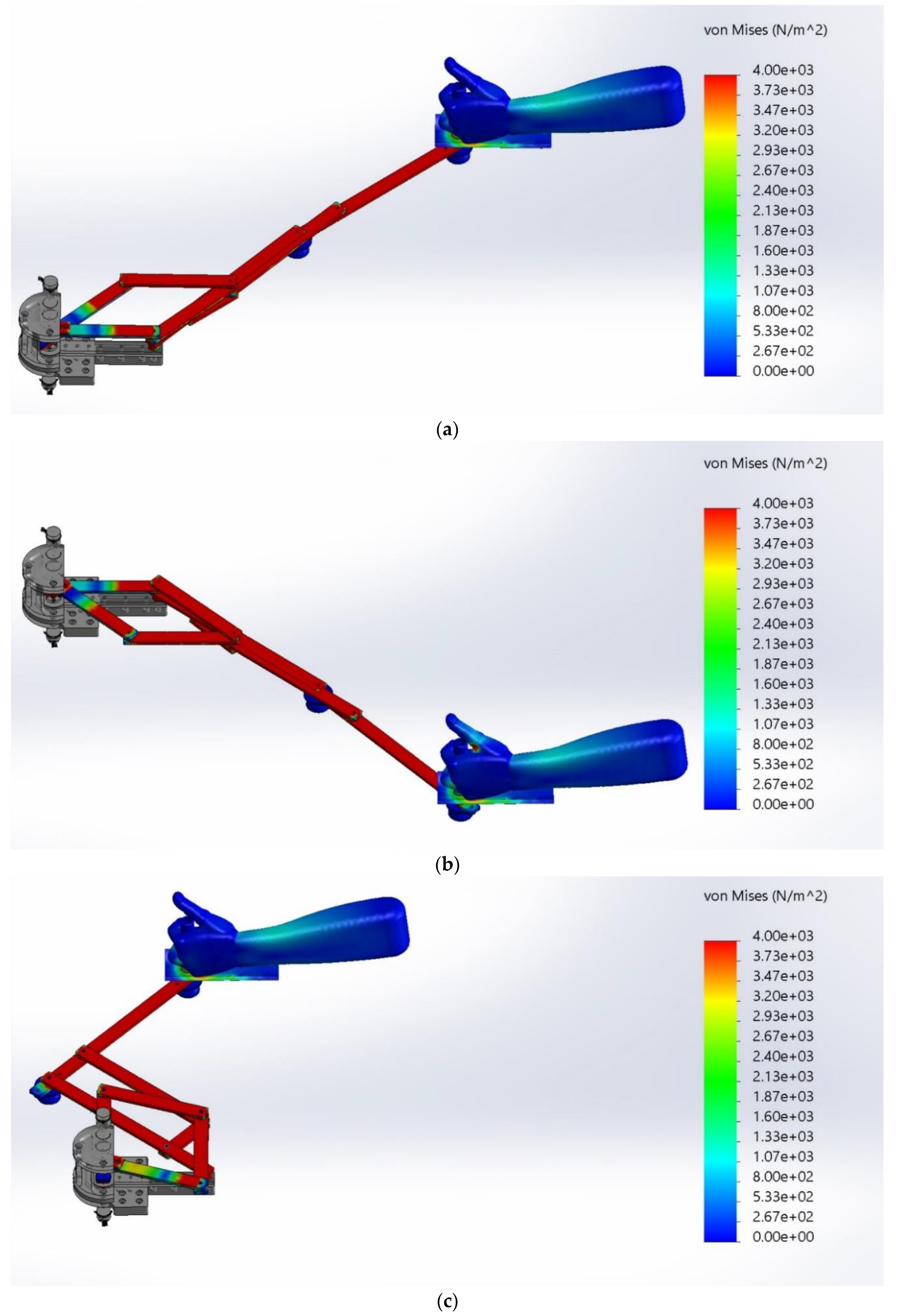
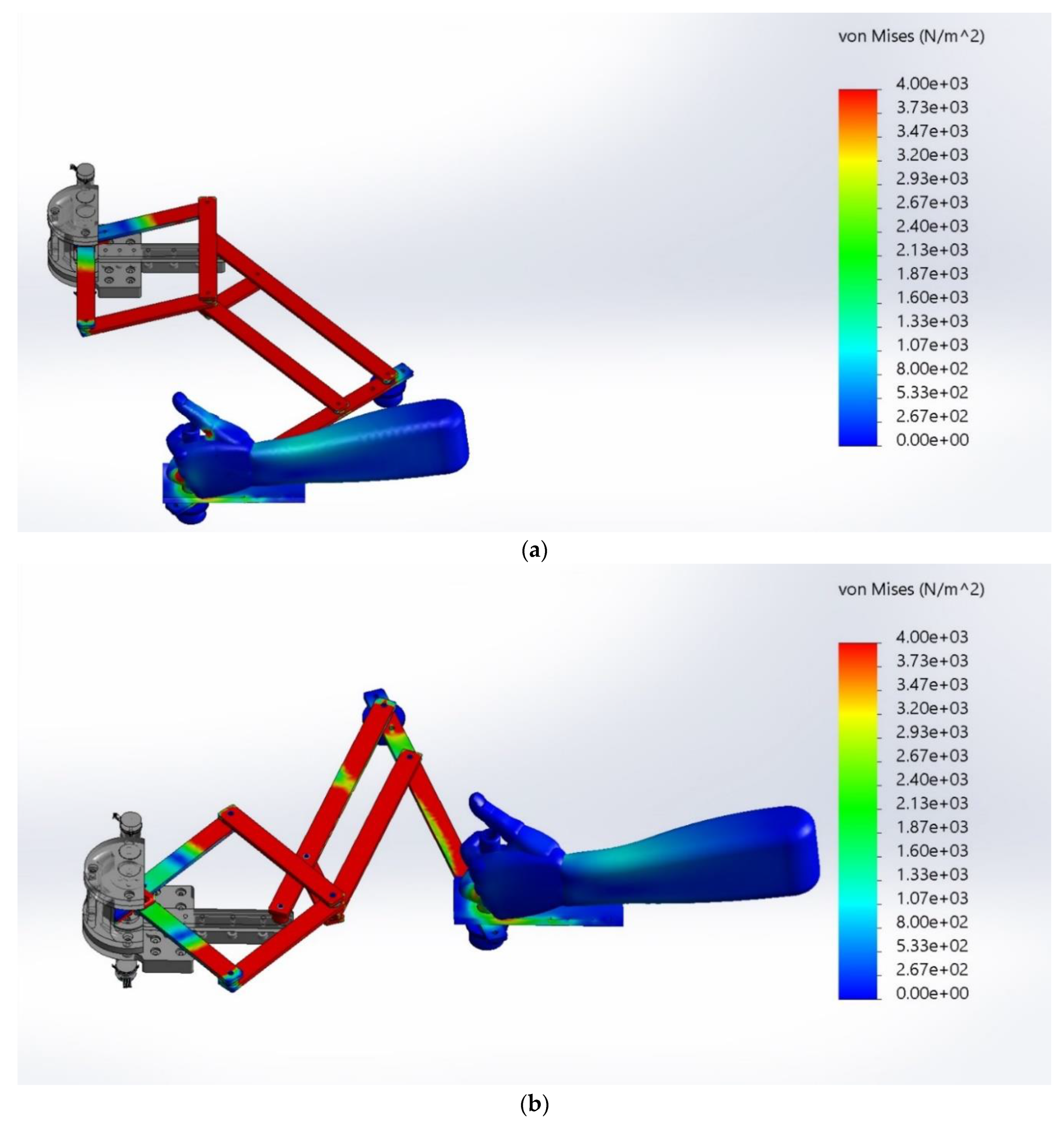
Figure 9a–e show the Nurse device on the positions
a (−496, 700),
b (496, 700),
c (−496, 148),
d (496, 148),
e (0, 424), respectively.
During the simulation, a 1060 aluminum alloy has been used for Nurse bars and wheels and ABS (acrylonitrile butadiene styrene) has been used for the user mechanical interface.
Table 1 shows the main material characteristics of the 1060 aluminum alloy and
Table 2 shows the main characteristics of the ABS. It is important to note that the materials used during simulations correspond to the materials used in practice for the lab prototype of Nurse in
Figure 2 and
Figure 3.
Hyperelastic materials can be used to simulate the biological skeletal muscle behavior [
37]. Particularly, silicone materials have the ability to imitate the distribution of stress in muscle tissue [
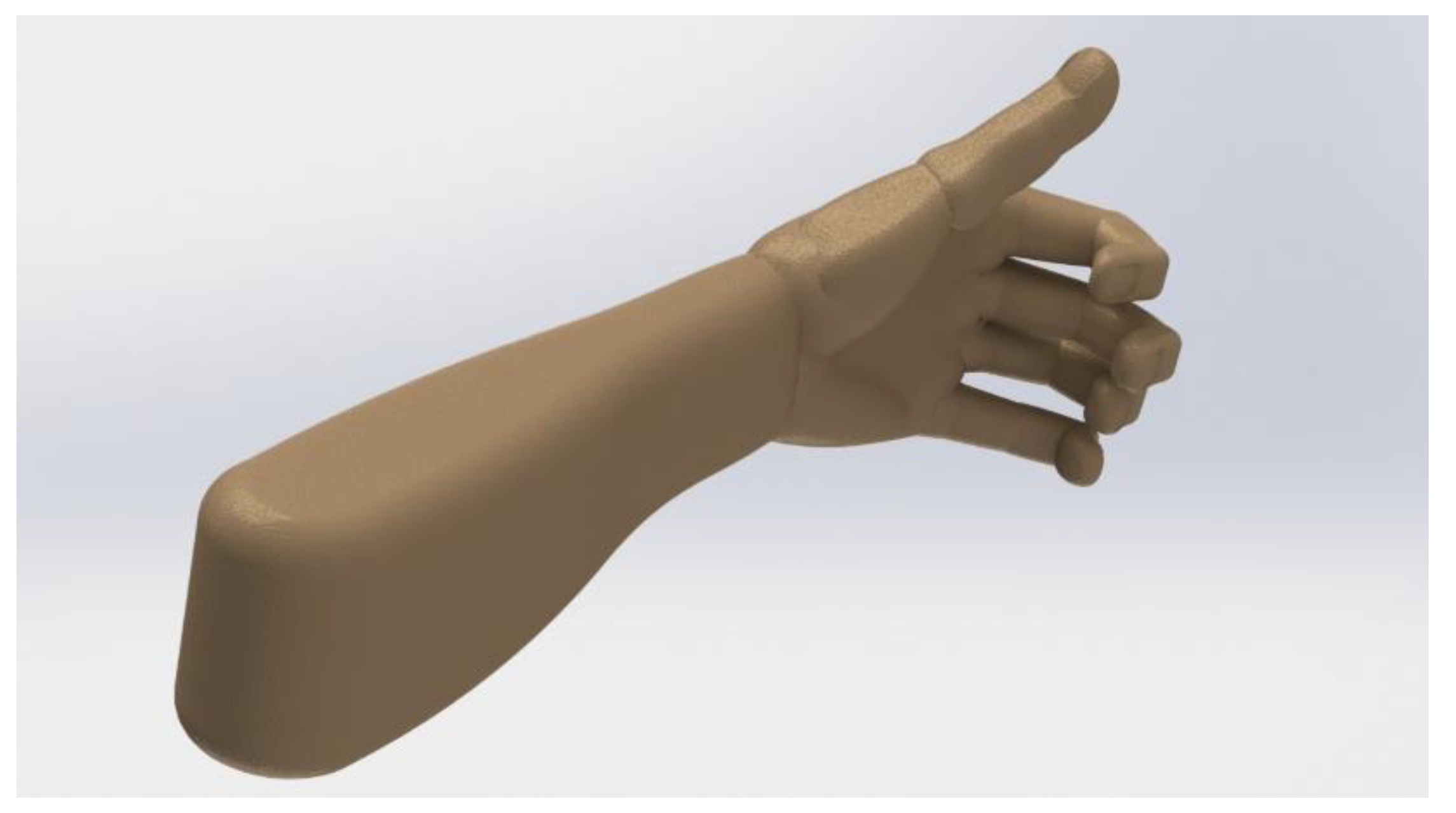
38]. Therefore, to carry out the FEM analysis, a human arm has been simulated using silicone.
Table 3 shows the main material characteristics of the used silicone. The weight of the simulated human arm part (hand + forearm part) has been assumed as 1.18 Kg according to the average weight of a human arm [
39,
40].
Figure 10 shows the simulated human arm. The used CAD model of the human arm with articulated fingers is an open access model available online in [
41].
During the FEM simulation, gravity force acts along the Z axis. In addition, a torque of 3.53 Nm has been used for each motor of Nurse device (
M1 and
M2). The motor torque of 3.53 Nm is the maximum torque required by the motors of Nurse prototype during the reproduction of arm rehabilitation exercises according to the experimental tests published in [
26].
Table 4 shows the main characteristics of the mesh used for the FEM analysis. The Von Mises stress function has been used to measure the three main stresses acting on X, Y, and Z axes of the human arm. The Von Mises stress function σ
vm is expressed as [
42]:
where:
σ1 = principal stress acting on X.
σ2 = principal stress acting on Y.
σ3 = principal stress acting on Z.




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}