1. Introduction
Even in relatively well-developed countries, some women and, subsequently, infants are at risk of suffering from birth complications. This is especially prevalent in the US, where women are at a higher risk of death from childbirth than in comparably developed countries [
1]. Two main reasons have been identified as determinants of birth complications and deaths due to pregnancy complications: (1) risk factors such as health problems before and during the pregnancy and (2) insufficient health behavior during the pregnancy [
2,
3]. Both will be reviewed in the following and investigated in this study.
Health risks for pregnant women are associated with sociodemographic differences, such as low socioeconomic status and low educational level [
4]. This can explain why health outcomes differ between and within comparably developed countries [
1]. In the US, black women have worse pregnancy outcomes due to a lack of access to high-level care and quality of care received in a certain facility compared to white women [
5,
6]. Many complications could be prevented if, on the one hand, pregnant women had access to timely and thorough medical care; thus, the issue concerns both healthcare systems and the effective use of them. On the other hand, pregnant women’s sexual health and health behavior during pregnancy is a second essential factor as it affects the health of the mother-to-be and her unborn child. However, some women are not aware of this or do not change even if they know about it. Thus, it is important to understand this phenomenon better.
Women should change or quit risky behaviors and develop or maintain healthy ones. Such behaviors include diet and healthy eating, physical activity, and abstinence from drugs such as alcohol, tobacco, and caffeine. Further recommended behaviors are the intake of various forms of nutrition, including supplements such as folic acid and vitamins, sticking to a regular sleep pattern, and taking screening tests [
7]. Abstinence from alcohol, tobacco, and other drugs are crucial factors that are imperative for preventing birth defects, mental disabilities, and neurodevelopmental disorders. Moreover, there is a high risk for preterm delivery, low birth weight, stillbirth, and malformation of the infant if women consume alcohol, tobacco, or drugs during pregnancy [
8].
On a positive note, many women change their behavior and reduce smoking, caffeine, and alcohol intake before and during pregnancy, as well as increase their fruit and vegetable consumption during pregnancy [
9,
10]. However, many women maintain unhealthy behaviors regardless of existing evidence and healthcare recommendations promoting the adoption of a healthy lifestyle. Multiple factors can be summarized as non-medical influences on health behavior change, affecting health outcomes in a positive or negative way. Psychosocial variables such as anxiety and stress are negatively correlated with pregnancy outcomes [
11].
To further examine the significance of the interrelation between predictors of health behavior and health-related behaviors during pregnancy, we applied the Compensatory Carry-Over Action Model (CCAM).
1.1. The Compensatory Carry-Over-Action Model
The CCAM [
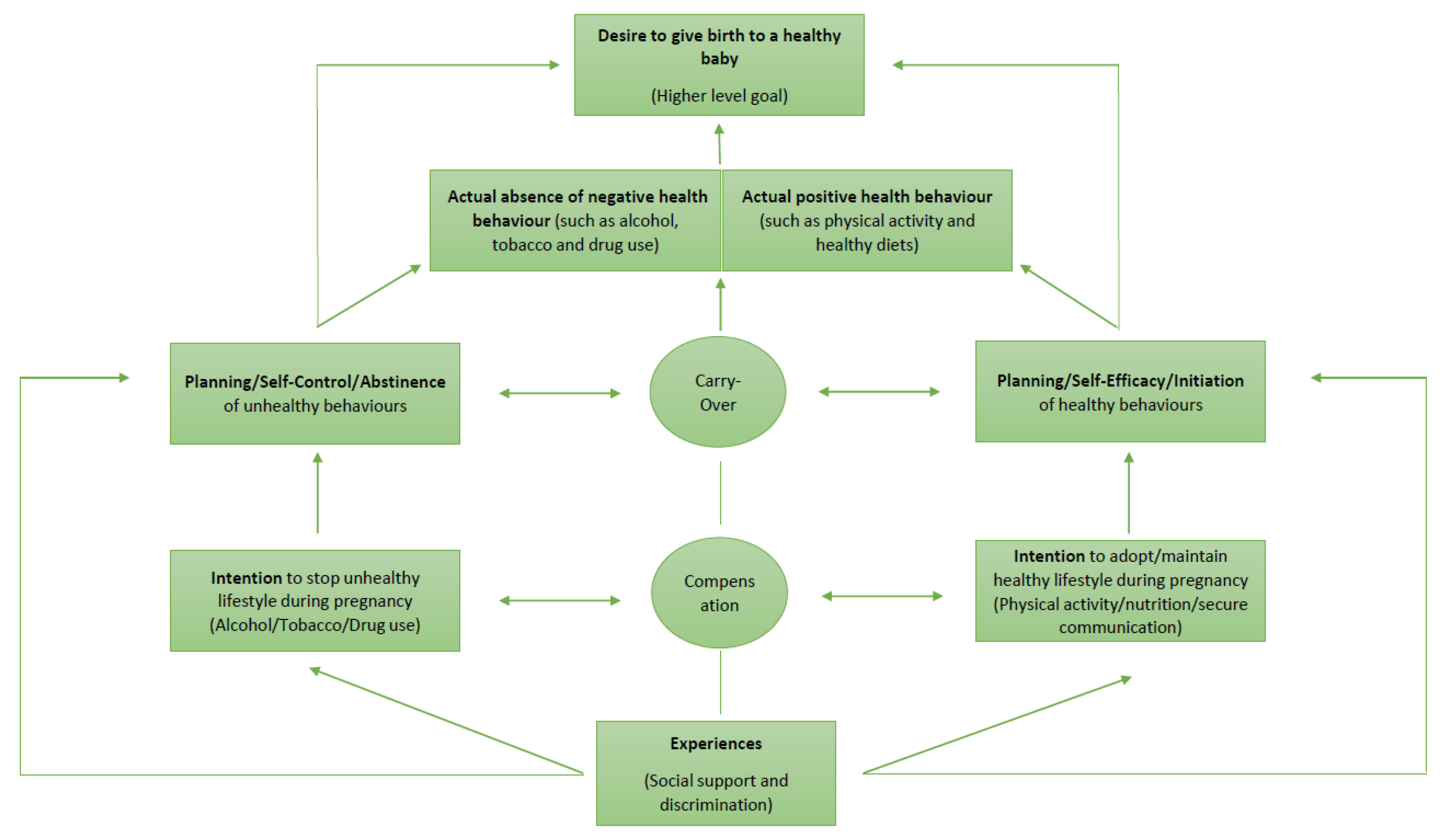
12] determines the mechanisms of multiple health behavior changes that are required during pregnancy. It explains how altering one health behavior can affect multiple behavior changes in different areas of life and how these behaviors are interrelated. The main difference with the other models is that the CCAM assumes that higher-level goals can be achieved by different behaviors (e.g., remaining fit and delivering a healthy baby). Hence, an individual needs to intend, plan, and implement the necessary behaviors. The model is characterized by carry-over mechanisms, which suggest that the resources from one health behavior can be carried over to another or that one behavior can initiate another one (e.g., being more physically active can lead to more energy for the uptake of a healthy diet). Alongside the carry-over mechanisms, there are compensatory mechanisms taking place which explain the cognitive dissonance between behaviors and justify the unhealthy ones (e.g., not changing an unhealthy diet as being physically active is perceived as “enough” to achieve higher-level goals).
The CCAM can be applied to pregnancy (see a schematic overview in
Figure 1). The desire to give birth to a healthy baby would serve as a higher-level goal in this case. Different health behaviors, such as a healthy diet and physical activity, are conducive to this goal. Other health behaviors are risky and viewed as unhealthy, including smoking and alcohol and drug use during pregnancy.
In the first phase, a pregnant woman has to make the resolution to adopt or maintain healthy behaviors and quit the unhealthy ones. If she has the intention to do so, she needs to initiate, plan, and put them into action and stop them. Those will then lead to actual health behavior securing her own and the baby’s well-being. Social-cognitive determinants of health (such as intention, planning and self-efficacy) are crucial for the intended health behaviors and work in interrelation. Between those implemented health behaviors, carry-over and compensatory mechanisms are taking place. However, as this was not explicitly researched before on the basis of the CCAM, the current study aims to fill this gap.
1.2. Social Support
In the CCAM, resources have been postulated to facilitate health behavior. In the framework used for the current research, “experiences” of support and discrimination were added explicitly to the model in order to investigate their effects: a crucial resource is social support. For example, a lack of social support during pregnancy could lead to feeling strained and a higher likelihood of unhealthy behaviors or difficulties in implementing healthy behaviors. During pregnancy, social support is strongly connected to mental health, which can be key for good pregnancy outcomes [
13]. In a study by Feldmann et al. [
14] from the year 2000, social support seemed to be a predictor of the infant’s birth weight.
Women with low social support tend to have babies with lower birth weight while women with large networks have infants of higher weight. In addition, low social support leads to a higher risk of preterm delivery [
15]. There is evidence suggesting that social support promotes higher levels of compliance with health professionals’ recommendations, which can lead to a better implementation of healthy behaviors [
16]. Lastly, low levels of education, low socioeconomic status, and high parity are found to be associated with low social support [
17]. However, the interrelations need to be understood better especially in relation to health behavior and other factors impacting birth outcomes. One such factor is discrimination.
1.3. Discrimination
In addition to a lack of social support, discrimination can pose an important barrier against the adoption of health behavior. Discrimination must be seen as two-fold in pregnant women. It has been found that both racial and pregnancy discrimination can impact women and, with that, birth outcomes [
18,
19]. Since the last century, the data on racial discrimination have drawn more attention and importance to understanding discrimination as a psychosocial stressor. In general, discrimination is associated with negative health behaviors [
20]. Evidence on this matter is growing and indicates that a large disparity between black and white women exists.
Research has shown that Hispanic, Black, and non-acculturated women have a higher risk of complications during pregnancy and birth. This difference is not likely to be related to biological differences but rather to social factors, environmental exposure, and health behavior patterns [
21]. A study by Mustillo et al. in the year 2011 [
22] examined perceived racism, and its influence on pregnancy outcomes. The findings showed that 50% of black women that experienced racism had a preterm delivery and 61% of them had a baby with low birth weight. In comparison, the percentages for white women were 5% and 0%. Other studies support the positive correlation between preterm deliveries and experienced discrimination [
23,
24]. A more recent study conducted by Alhusen et al. in 2016 [
25] confirmed the finding that preterm delivery and low birth weight were a consequence of racial discrimination. Racial discrimination should thus be seen as an independent risk factor.
In addition to racial and ethnic discrimination, pregnancy discrimination also has an impact as it is still experienced by many women and is seen as indirect sex discrimination [
26]. Pregnancy discrimination can indirectly affect the health of the mother-to-be and the baby [
19]. Pregnancy discrimination has been found to relate to perceived stress, increased levels of postpartum depressive symptoms, and lower birth weights, independently of racial discrimination [
19]. Thus, it seems likely that pregnancy discrimination has an impact on health behavior independently of racial discrimination. Accordingly, this should be addressed as a potential barrier to health behavior as the concrete mechanisms are not clear.
1.4. Research Objectives
Taken together, there is still a lack of knowledge regarding the impact of social support as well as discrimination on the wide range of health behaviors, particularly regarding how intention, planning, and implementation of health behaviors change in relation to psychosocial variables. Therefore, the research question of this study is: how do predictors of health behavior, specifically intention, planning, self-efficacy, social support, and discrimination interrelate with different health behaviors during pregnancy? To research this, the CCAM was applied to pregnant women and their health behavior for the first time, choosing a qualitative approach to better understand the subjective perspective of the study participants.
2. Materials and Methods
This research is based on qualitative interviews with the aim of understanding the predictors and interrelations of the health behaviors of pregnant women with the theoretical backdrop of the CCAM. A qualitative study design was chosen because no empirical–statistical generalizability or inference on a population was aimed for but, rather, the exemplary and differentiated description of selected cases [
27].
Accordingly, the study design is purely descriptive as it highlights the possible health behavior changes of ten pregnant women. For this qualitative study, ten interviews were conducted with pregnant women from different cultural backgrounds. A semi-structured interview guide with open questions was designed to ensure detailed information on and in-depth experiences of the participants’ pregnancy behavior and lifestyle (see
Appendix A). The structure was based on the literature, the theoretical backdrop of the CCAM, and the researchers’ knowledge of the subject. The development of the questions for the interview to generate suitable answers to the research question was established through the discussions of the researchers.
Purposeful sampling [
27] was performed to obtain the most available information for the selected cases. Qualitative studies, especially those using content analytic methods, are conducted to explore or explain the subjective meaning. These studies are embedded within constructivist frameworks. Specifically, they seek subjective views and opinions and not objective facts [
27]. The case selection was purposefully not random in order to acquire a representative sample to obtain as much knowledge as possible regarding the research question. Specifically, a selection of typical and critical cases was executed [
27] out of a convenience sample which was recruited.
The order of the questions was adapted during the interview, depending on the narrative flow of the participants. The interviews were conducted in English, over Zoom, and lasted from 25 min to 39 min; the mean duration was 31.75 min. Prior to the interview, the participants were informed about the purpose of the study and the data management and security, as well as the analysis. Moreover, a signed consent form was obtained, which stated that participation was voluntary and anonymous and that the acquired data would only be used for research purposes.
2.1. Data Analysis
To describe the interview data, an explanatory content analysis was used. The interviews were audio-recorded and subsequently transcribed. The sentences or words of the transcribed interviews were labelled into broad categories, such as Health Behavior, Social Support, and Discrimination. As the answering of a specific research question was sought, the categories were pre-defined and intrinsic to the question in order to follow an explanatory approach. However, a mixed approach was chosen to include both deductive and inductive results. The categories were further divided as new themes emerged during the interviews. Health Behavior was subdivided into Change of Health Behavior, No Change of Health Behavior, and Forced Change of Health Behavior. Determinants of Health Behavior were added to the respective categories (e.g., if intention, planning, or self-efficacy was mentioned). Social Support was divided into High Social Support and Lack of Social Support. For Discrimination, the subthemes of Racial Discrimination, Pregnancy Discrimination, and No Discrimination were used. The coded sentences or words were assigned to the area where behavior change occurred, such as diet, physical activity, alcohol, smoking, supplementation, hygiene, and COVID-19 pandemic. Lastly, those subthemes were compared descriptively to each other with regard to their social-cognitive determinants. The results are presented with significant quotations from the participants.
2.2. Participant Characteristics
The selection of the participants was conducted through convenience sampling. The first selection requirement for the participants was for them to have an international or diverse background. Then, the participants were chosen because they were all pregnant with their first child and also gave birth, both during the COVID-19 pandemic, especially in the first lockdown. They represented a heterogeneous group. They all had different nationalities, came from different family backgrounds, and gave birth in different countries, which was important for understanding and comparing different “experiences” of discrimination and social support, as included in the CCAM (see
Table 1). Therefore, all ten participants who were approached met the inclusion criteria for this study.
All of the participants spoke the language of the country they delivered their babies in. As the healthcare system varies in each country, each participant had a distinct health insurance and a different experience with the healthcare personnel. All ten participants were between 20 and 39 years old, with a mean age of 28.6 years. Study Participants 2, 4, 7, and 9 were people of color (
Table 1). All infants were born in good health, whereby it should be noted that Participants 7 and 9 gave birth to a baby with a lower birth weight. All the participants except Participants 2 and 7 had a partner during pregnancy and birth, who was also the father of the baby. Participants 2 and 7 did not have a partner during this time and had no contact with the father of the baby (
Table 1).
3. Results
The interviews revealed the following information. The important quotations of the participants are discussed in this section. An overview is presented in
Table 2.
3.1. Health Behavior
There were different approaches and a wide range of changes regarding health behavior (see
Table 3). Participant 2 reported that she did not change any health behaviors and maintained an unhealthy lifestyle even though she knew that she had unhealthy habits. Although she reported perceiving a certain risk for her child, she could not clearly formulate an intention nor planned her behavior accordingly. She highlighted taking her vitamins and supplements regularly and felt that supplementation was sufficient as a compensatory mechanism. In contrast, Participant 1 changed everything and was overcautious because the over-arching goal was quite salient for her: “I tried more so especially during pregnancy to avoid antiseptic alcohol as much and washing my hands more. So, I didn’t want getting the alcohol in my system” (Participant 1). Her intention and implementation of these health behaviors were successful as she ate only home-cooked meals, while avoiding fish along with white cheeses and went to yoga and swimming classes. She reported a high level of behavioral planning, thinking in detail about the food she wanted to avoid and the exercises she considered healthy during the pregnancy. Her health behavior changes materialized in different behavioral domains which seemed to be driven by the higher-level goal of remaining healthy.
Participants 4 and 9 were diagnosed with gestational diabetes during the pregnancy. Both were encouraged to change their health behaviors because of their unhealthy lifestyle before pregnancy. Following the perceived risk related to their detected diabetes, they both presented the intention to change their behavior. They also started planning their physical activity and diet. They went for walks or visited the gym regularly; moreover, they followed a strict diet (
Table 2). Participant 3 was eating healthily and went running regularly before pregnancy. Although she had the intention to continue doing so, the side-effects of being pregnant such as nausea and migraines prevented her from doing it, negatively affecting her previously high self-efficacy, as she stated explicitly in the interview. In addition, she had a bleeding at 8 weeks of being pregnant, and it did not feel safe anymore to go running. Lastly, she quit vaping as soon as she found out that she was pregnant. All the participants took supplements, including different vitamins and folic acid. No one reported smoking or drinking alcohol during pregnancy (
Table 2). In the case of cessation, this was reported as rather easy by all respective participants, indicating a high self-efficacy. Planning was not mentioned as the women perceived these behaviors as just needing to quit instead of extensively developed, i.e., reduced.
Participants 5 and 8 also experienced many pregnancy side effects, similar to Participant 3. Participant 5 stated that she could not eat or drink at all because of the nausea and heartburn, while Participant 8 fainted very often during her pregnancy and tried to eat and drink more to fight her fainting spells. Both could not really change their health behavior due to the pregnancy side effects, although they had the intention to do so. At the beginning, self-efficacy was high as they both tried to change their diet, exercise more, and get into a better routine, but it quickly decreased due to the side effects. Participant 5 said in retrospect that she wished she had done more to actually change.
Participants 6 and 10 considered themselves as lucky as they did not experience a lot of side-effects. Therefore, they did not feel the need to change their health behaviors drastically, but they did adjust a little bit. Participant 6 planned her diet beforehand as she wanted to incorporate some coffee and cut out other things. In contrast, Participant 10 was on a strict diet to lose some weight before her pregnancy; when she found out that she was pregnant, she changed back to her normal standard of eating healthily (
Table 2). She also booked her aqua aerobics classes as soon as she was aware of being pregnant. She acted so promptly not only because of her pregnancy but also because she was afraid that due to the COVID-19 pandemic, there would be only a restricted number of spots available. Continuing this topic of exercise, half of the women mentioned that they would have liked to go to pregnancy yoga or aqua aerobics but that they were either afraid to mingle with too many people or that there were simply not enough or very restricted possibilities to do so during the COVID-19 pandemic.
Consequently, the women’s health behaviors were affected by the COVID-19 pandemic. In addition to taking precautions and hygiene routines seriously and displaying avoidance behavior, they felt unsafe and were afraid that something would happen to them or their baby, as pregnant women belong to a higher risk group: “Oh, I went to the grocery store, I hope I’m going to be okay. I hope I won’t have COVID because it can affect my baby. It’ll be on me if I get sick during pregnancy and something happens. So, all of those little phobias where you’re scared to do things or you scared that it would affect your baby” (Participant 4). “The thing is even before due to COVID I’ve been kinda locked in the house. And then with the pregnancy I even became more strict with who I was seeing. So I basically haven’t been out of the house because I’m just more cautious now” (Participant 5).
The participants also described positive effects of the pandemic. Six of the participants were working from home and mentioned that those working conditions were beneficial for their pregnant state. They could take breaks, adjust their working hours and did not need to take public transportation or the car to go to work. As they phrased it: “I’m convinced because I worked on the big Pilates ball instead of a chair, I’m convinced my pregnancy and my birth was better because I could spend 8 h on a ball rather than on a chair. Yeah, so, I think the pandemic had some positives for the pregnancy as well” (Participant 3); “It allowed me to maintain my consistent routine” (Participant 2).
3.2. Social Support
The participants drew their knowledge and support from a wide range of sources. For example, Participant 1, who displayed a comprehensive behavior change, mentioned her family as well as a birth Doula as the main people of support. She felt very supported and informed about everything that could happen. In contrast, Participant 2, who described low self-efficacy and planning, as well as health behavior change, had no family, friend, or partner support. She was not prepared for birth, pointing out that everything was unexpected and that it did not resemble what she had previously seen on TV. The other participants described good support from their partners and family. Even though Participants 4 and 9 mentioned that their partner could have done more, they felt supported overall throughout their pregnancies. All the participants communicated a lack of support from their friends. Participant 8, especially, felt very hurt that her friends did not reach out at all to her.
As all participants were pregnant during the pandemic, they all mentioned that they could not enjoy their pregnancy fully as almost no one saw them pregnant: “It’s like being pregnant in closed walls” (Participant 3). Most of them underestimated the impact of the pandemic: “Getting pregnant during the pandemic, I thought it was going to be easy but for me turned out to be one of the hardest things just because I didn’t have that support, that family support, the friends support” (Participant 4). All of them felt supported from a medical perspective, although there were restrictions because of COVID-19. They also stated that it was very exhausting always having to follow the new COVID-19 regulations and translate them into what it meant for them. As the partner was not always allowed to accompany them to medical appointments, they felt rather on their own during the pregnancy. “It’s something you think about a lot. I’ve raised loads of complaints with various different hospitals. I’ve considered changing to a few hospitals but just have a blanket policy for the entire hospital and they don’t want to change it.” (Participant 6); “Especially after the birth you need your partner to be there. A birth is already hard enough” (Participant 8).
3.3. Discrimination
Two of the four participants of color who reported mostly unhealthy behavior (
Table 2) and low social support stated clearly that they experienced racial discrimination every day: “Security would stop us while walking to our building. I just can’t help but thinking like if we were a white couple would they have stopped us? They’re just assuming that because we’re black we can’t afford to live here” (Participant 2). The other two were not sure as they thought and hoped that everyone was treated this way. Participant 3 also expressed having experienced discrimination because she has a mixed background and felt rejected by people: “With my mixed ethnic background, I do not feel understood and sometimes there are negative comments towards that. People don’t understand mixed” (Participant 3). Participant 5 also stated that she does experience discrimination towards her mixed background, as well as her gender.
None of them described any discrimination due to their pregnancy. There were no inappropriate comments made on their bodies nor did they have the impression that they would not be taken seriously. All of the participants thought that, as they did not see many people, this was due to the pandemic. The participants that worked during pregnancy were doing so remotely. According to the participants, they did not experience that kind of discrimination because of their remote working situation: “If I didn’t tell somebody that I am pregnant they wouldn’t know ‘cause they can’t see me. So, it’s a lot easier to avoid being discriminated against due to pregnancy for that reason” (Participant 1). “I know of people who outside of COVID have said they had inappropriate comments to them like on the way to work or at work but I’ve been at home” (Participant 3).
3.4. Higher Level Goals and Social-Cognitive Determinants of Behavior Change in Concert
With regard to the theoretical model, the reports by the women clearly indicate that all the women were worried about giving birth to a healthy baby as a higher-level goal and would not risk their child’s health by their own behavior (
Figure 2). They were very aware of the different health behavior options. The social-cognitive determinants facilitated other healthy behaviors but also caused negative behaviors in other areas (carry-over and compensatory mechanisms) in the cases where intention, planning, and self-efficacy were low.
Social support in general, perceptions of discrimination, and coping with all the pregnancy- and COVID-related challenges were reported as being very intimidating (
Figure 2).
To aggregate the findings with regard to the predictions of the CCAM for interrelations or co-occurrence of the different behaviors, the findings are cross-tabulated in
Table 4.
Summarizing
Table 3 and
Table 4, all the women reported higher-level goals and most had a high intention to change health behavior and self-efficacy of health behavior, while planning and actual behavior change and health behavior prior to the pregnancy onset was less likely. The ones with no intention to change also exhibited less favorable patterns with the other social-cognitive predictors of behavior change. The women who previously performed health behaviors revealed a greater health pattern with the maintaining or even the expanding of their healthy lifestyles. Transfer and compensation can be seen behind different behavioral domains with the meeting or the violating of the behavioral recommendation.
4. Discussion
This qualitative study with ten women aimed at examining the interrelation between social support, discrimination, and health behaviors based on the Compensatory Carry-Over Action Model (CCAM). The results reflect the theoretical assumptions of the CCAM. All the women interviewed wanted to reach their higher-level goal, which was both the health of the baby and their own health. This higher-level goal was prevalent in all the women. However, all the other variables varied between the women. While most of the women demonstrated obviously healthy profiles, one woman revealed a rather unhealthy pattern and suggestions for improvements. Carry-over mechanisms took place between the implemented health behaviors as one adoption led to another, or the lack of an adoption of a healthy behavior could be a barrier towards the implementation of another. This means that there was not only a change towards healthy eating habits but also towards exercising if a positive change was induced. The compensatory mechanism justified the unhealthy behaviors with a beneficial behavior. Supplementation can be viewed as a compensatory mechanism for the maintenance of unhealthy behaviors. It can also serve as a possible explanation as to why some women did not change their health behavior accordingly.
The requirements presented in the CCAM to actually change health behavior to meet the higher-level goal of a healthy baby are intention, planning, and self-efficacy regarding healthy behaviors. However, three participants described low levels of these social-cognitive determinants. Even though the intention to be more physically active was reported by one woman, the unexpected pregnancy side-effects made it difficult to implement healthy behaviors and negatively affected her planning and self-efficacy. Physical or emotional symptoms that may accompany pregnancy, such as nausea, bleeding, etc., and/or insecurity or fear hinder the adoption of healthy behaviors by having a detrimental effect on the social-cognitive determinants, although the intention to changing or maintain health behaviors was in most cases existent. This finding is supported by other studies stating that intended health behaviors cannot be followed because of nausea, backache, and fatigue [
28,
29]. This may indicate that an intention–behavior gap exists in pregnancy for multiple health behaviors even if a higher-level goal is clear.
A study conducted by Dunney and Murphy in the year 2015 [
30] showed that 80% of women have unhealthy behaviors during the first and third trimester of pregnancy. In those time periods, most women experience pregnancy side effects. Pregnancy side effects include the diagnosis of various diseases or complications such as gestational diabetes. In that case, the women are externally required to change particular health behaviors. A recent study from Nagpal and Mottola [
31] shows that physical activity during pregnancy has a positive effect on chronic diseases, such as obesity, type 2 diabetes, and cardiovascular complications. Another study proclaims that the intention of physical activity alongside perceived behavioral control and self-control are positively correlated with an active behavior pattern [
32]. Thus, the intention of health behaviors is an important factor for implementation and beneficial for the pregnancy itself and the outcome but needs to be translated into action via different mechanisms, as our study suggests. Behavior-change models such as the CCAM can help to understand these mechanisms better.
Another explanation for maintaining unhealthy behaviors in this study was the lack of social support and experiences with racial discrimination in everyday life, referring to predictors of health behavior. Perreira’s study [
33] indicates that pregnant women who experienced discrimination tend to use more negative coping strategies, such as alcohol and tobacco abuse. As prevention is associated with health inequity, perceptions of discrimination might be an important pathway in which health behaviors are affected. In turn, the CCAM offers action points to avoid negative consequences or to balance these experiences. Even if a health behavior is affected by discrimination, enhancing carry-over and compensation mechanisms can be addressed to overcome difficulties. Social-cognitive determinants, such as planning and self-efficacy, should be addressed to reduce the negative impact of discrimination. Benett and Pavilion found [
34] that perceived chronic everyday discrimination is associated with health-compromising behaviors, such as smoking and alcohol and food abuse during pregnancy. Two participants of the current study (3 and 5) reported their experience of discrimination in their daily life because of their mixed background, and both suffered a lot of pregnancy side effects and suboptimal health behavior. Many other studies support these findings [
35]. Paradies states that perceived racism is a risk factor for negative mental health and negative health-related behaviors. Perceived racial discrimination can interrelate with the intention to engage in health behaviors and explain the continuation of unhealthy behaviors. Congruently, it has been found that in North America, black women are 3–4 times more likely to suffer a pregnancy or birth-related death than white women. This is due to disparities in the availability of high-quality hospitals and differential treatment within hospitals [
36]. Two of the women of color who disclosed in the interview experiencing racial discrimination every day delivered a baby with lower birth weight. This is in line with studies which have shown that experiences of racial discrimination and low birth weight are correlated (e.g., [
22,
25]).
Another explanation is a lack of social support during pregnancy, as experienced by a few of our participants. The same women who reported frequent racial discrimination also reported a lack of social support. The participants reported a link between social support and other predictors of health behavior. Thus, this is indicating another pathway that might potentially buffer or enable the negative effects of health behavior and outcomes. In the study by Crone et al. [
37], women who reported a lack of social support during pregnancy were more likely to use tobacco, alcohol, and food as coping mechanisms. Furthermore, they were eating fewer fruits and vegetables and had less knowledge about pregnancies than women that reported high levels of social support. Pregnant women who experienced higher social support were more likely to use prenatal vitamins, had a better quality of diet, and were smoking less [
17]. A source of support that was frequently mentioned and seemed related to the uptake of health behaviors was partner support. Most women described good support from their partner, although they felt rather on their own during the pregnancy if the partner was not allowed to attend medical examinations or the birthing process. However, the lack of partner support seemed to be most detrimental if no other support by family and friends was perceived. Two women who said that their partner could have been more involved were still satisfied with the overall support given by families, hence offering a possible compensation option.
A reason for the relation between support and health behavior might be related to the reduction in stress, anxiety, and depression when receiving social support [
38,
39]. This is imperative as social support enables better planning and maintaining of healthy behaviors. Those findings are relevant in the context of the COVID-19 pandemic, as many women reported less social support than they expected and needed. This was explicitly attributed to the pandemic by the interviewees. However, the pandemic could also increase health behaviors due to the online setting of work. More room and time were generated for physical activity, healthy cooking and breaks, sufficient sleep, and hygiene routines. These behaviors were all beneficial for health and were a key cornerstone of a healthy lifestyle during pregnancy. The limited contact with people and working remotely presumably helped reduce pregnancy discrimination, thus showing how the predictors of health behaviors were directly impacted by the pandemic. Be that as it may, the effects of the pandemic on the predictors of health behavior and actual behavior change during pregnancy still need to be further explored in future research.
Nevertheless, it is difficult to quit unhealthy behaviors, as the study participants reported. Providing knowledge, materials, and professional support is not always sufficient for a change of behavior. There are other interventions that may be needed in order to accomplish a health behavior change. In this context, health professionals should rather raise awareness of how to mobilize social support and cope with discrimination. Goal-setting and planning will increase self-efficacy and intention, which lead to a more successful change even against the background of perceived discrimination and a lack of social support [
40].
Scheduling healthy behaviors, e.g., making a grocery shopping list before going to the store or planning to exercise in the morning might contribute to breaking unhealthy habits. Still, one of the most important approaches consists in seeking and accepting support. Joining different antenatal classes could broaden the support network and provide information, knowledge, and the sharing of emotions and experiences with others. Women who experienced support, empowerment, communication, and collaboration with their midwives were more likely to have healthy behaviors and felt less anxious [
41]. In this context, a buddy program could be launched where two pregnant women from the same doctor or midwife would be partnered up together in order to motivate, help, and support each other during their pregnancy. The effort put into these interventions could benefit both sides as social support promotes higher levels of compliance with health professionals’ recommendations [
16]. On the other hand, partners could be trained to provide practical and emotional support as the pregnant women in our study mentioned this support as being crucial. In general, empowering the women as early as possible could work in multiple ways. Accordingly, policy and practice should take these aspects into account and help mobilize support and overcome discrimination by means of more rights and support for pregnant women while also empowering the individuals.
When interpreting these results, there are a number of limitations to consider. As the study was conducted in a qualitative fashion, the results could reflect the interviewer’s point of view. However, the interviewer was aware of potential biases beforehand to minimize the risk. In addition, the participants came from a rather small and convenient sample and only four were women of color, thus potentially being subject to another source of bias too. Nevertheless, all the women were from mixed or different ethnic backgrounds to that of the majority of their home country. Potential sources of discrimination and lack of social support, such as income or access to affordable healthcare, were not asked for systematically. Nevertheless, this study is to our knowledge the first to apply a multiple behavior change theory, namely the CCAM, to examine the link between predictors of health behavior and different health behaviors in pregnancy. Future research is needed to better understand this link and to address the above-mentioned limitations. In particular, the causal interrelations need to be further researched with longitudinal and interventional research, supporting vulnerable women in adopting health behaviors and coping with stressors functionally.
5. Conclusions
This study used a qualitative descriptive method to describe the interrelation between predictors of health behavior, specifically intention, planning, self-efficacy, social support and discrimination, and multiple health behaviors during pregnancy. The findings reveal that social support and discrimination indeed interrelate with health behavior during pregnancy by facilitating or hindering social-cognitive determinants. The assumptions of the CCAM were confirmed, as the intention and the planning of healthy behaviors are crucial for their implementation, as are the psychosocial experiences of support or discrimination. Carry-over mechanisms became obvious between different health behaviors (e.g., physical activity and diet) aiming at the higher-level goal of the mother’s and the child’s health.
Engaging in health behaviors helps to buffer the negative health outcomes which become more likely due to discrimination or challenges due to the COVID-19 pandemic. Purposefully, qualitative analysis is subjective due to interview bias and the interpretation of the results; thus, qualitative and quantitative data are needed for further research to support the findings of this study on the underlying social and structural determinants of health behavior. Further quantitative research can address the related burden of disease and/or focus on intervention studies. For example, quantitative data on disease burden, including maternal and neonatal morbidity and mortality, can be used to identify potential questions for qualitative analysis, and vice versa.
Further research and triangulation should aim to foster the understanding of the relationship and interaction of social-cognitive variables and health behavior change. For causal conclusions, triangulation and the testing of the assumptions by employing experimental designs with interventional support and a bigger randomized sample will be needed. For instance, helping women to set goals, translate their goals into action, mobilize social support, and transfer resources from one domain to another should be more effective than just giving lifestyle advice and providing universal feedback—which may even harbor the risk of discrimination. However, this remains an empirical question for future research.
The conclusions on theory refinements are that for pregnancy, the perception of discrimination and limited social support should be considered. The conclusions on practice suggest the need for more support of pregnant women to deal with challenges, translate their goals into action, and mobilize social support. On the societal level, discrimination should be addressed to reduce the challenges for pregnant women.







{kind=link}
{kind=link}