Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”



Abstract
:1. Introduction
1.1. Role of Ejaculatory Control
1.2. The Role of Bother/Distress
1.3. Rationale and Aims
2. Method
2.1. Participants
2.2. Measures
2.2.1. Outcome Measures
2.2.2. Input/Defining Variables
2.2.3. Control Covariates
2.3. Procedure
2.4. Data Cleaning and Analytical Strategy
3. Results
3.1. General Description of the Sample and Subsamples
3.2. Aim 1: Relationships among Ejaculatory Control, Bother/Distress, and ELT
3.2.1. Correlations
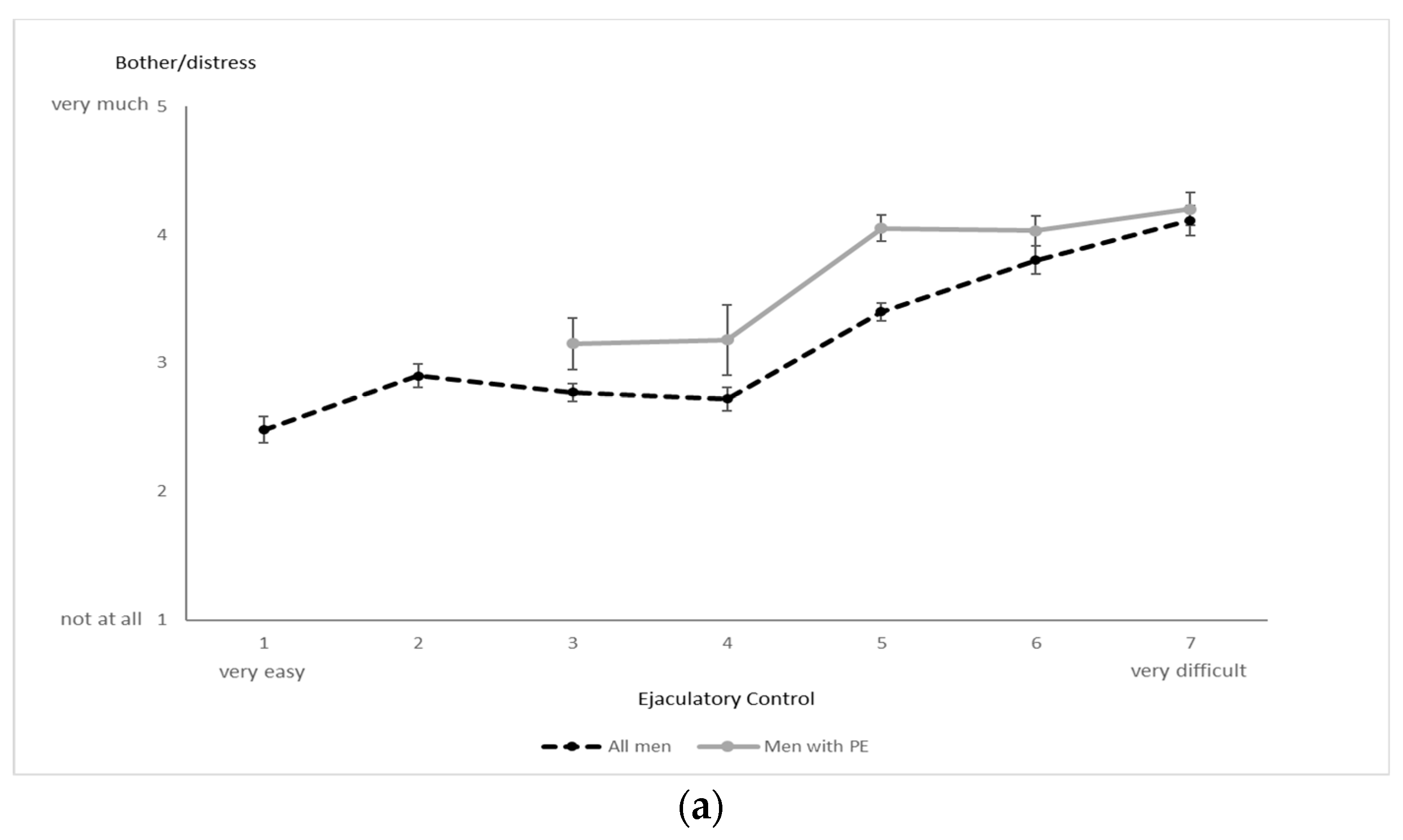
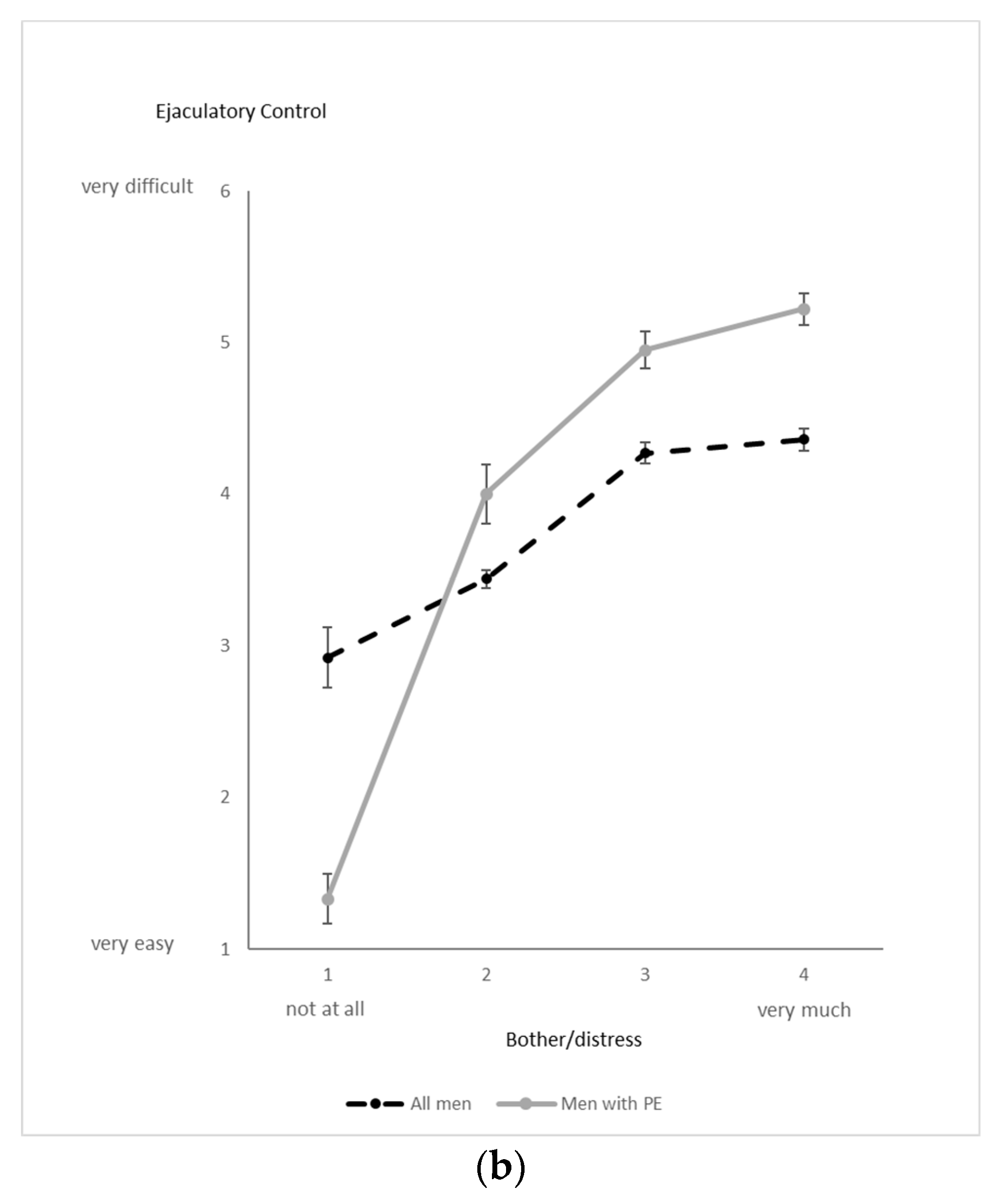
3.2.2. Patterns of Change
3.3. Aim 2: PE Status (PE vs. Non-PE) and Sexual Orientation Comparisons on Control and Bother/Distress
3.3.1. PE vs. Non-PE Men
3.3.2. Sexual Orientation
3.3.3. Covariates
3.4. Aim 3: Comparison of Men with Lifelong vs. Acquired PE
3.5. Aim 4: Partner Response Regarding Ejaculatory Control during Partnered Sex
4. Discussion
4.1. Overall Sample Patterns
4.2. Patterns in Men with and without PE and in Men with Different Sexual Orientations
4.3. Lifelong and Acquired PE
4.4. Partner Response to Poor Ejaculatory Control and Short Ejaculatory Latency
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Document on Social Media Recruiting and Controls
References
- McMahon, C.G.; Althof, S.; Waldinger, M.D.; Porst, H.; Dean, J.; Sharlip, I.; Adaikan, P.G.; Becher, E.; Broderick, G.A.; Buvat, J.; et al. An evidence-based definition of lifelong premature ejaculation: Report of the International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. BJU Int. 2008, 102, 338–350. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Serefoglu, E.C.; McMahon, C.G.; Waldinger, M.D.; Althof, S.E.; Shindel, A.; Adaikan, G.; Becher, E.F.; Dean, J.; Giuliano, F.; Hellstrom, W.J.; et al. An evidence-based unified definition of lifelong and acquired premature ejaculation: Report of the second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. J. Sex. Med. 2014, 2, 41–59. [Google Scholar] [CrossRef] [Green Version]
- Dinsmore, W.W.; Wyllie, M.G. PSD502 improves ejaculatory latency, control and sexual satisfaction when applied topically 5 min before intercourse in men with premature ejaculation: Results of a phase III, multicentre, double-blind, placebo-controlled study. BJU Int. 2009, 103, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Buvat, J.; Tesfaye, F.; Rothman, M.; Rivas, D.A.; Giuliano, F. Dapoxetine for the treatment of premature ejaculation: Results from a randomized, double-blind, placebo-controlled phase 3 trial in 22 countries. Eur. Urol. 2009, 55, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Shabsigh, R.; Rowland, D. The Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision as an appropriate diagnostic for premature ejaculation. J. Sex. Med. 2007, 4, 1468–1478. [Google Scholar] [CrossRef] [PubMed]
- Waldinger, M.; McIntosh, J.; Schweitzer, D.H. A five-nation survey to assess the distribution of the intravaginal ejaculation time among the general male population. J. Sex. Med. 2009, 6, 2888–2895. [Google Scholar] [CrossRef]
- Patrick, D.; Althof, S.; Pryor, J.; Rosen, R.; Rowland, D.; Ho, K.; McNulty, P.; Rothman, M.; Jamieson, C. Premature ejaculation: An observational study of men and their partners. J. Sex. Med. 2005, 2, 358–367. [Google Scholar] [CrossRef]
- Patrick, D.A.; Rowland, D.L.; Rothman, M. Interrelationship among measures of premature ejaculation: The central role of perceived control over ejaculation. J. Sex. Med. 2007, 4, 780–788. [Google Scholar] [CrossRef]
- Rowland, D.L.; Kolba, T.N. Understanding the effects of establishing various cut-off criteria in the definition of men with premature ejaculation. J. Sex. Med. 2015, 12, 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- Jern, P.; Gunst, A.; Sandqvist, F.; Sandnabba, N.K.; Santtila, P. Using ecological momentary assessment to investigate associations between ejaculatory latency and control in partnered and non-partnered sexual activities. J. Sex. Res. 2011, 48, 316–324. [Google Scholar] [CrossRef]
- Gao, J.; Zhang, X.; Su, P.; Shi, K.; Tang, D.; Hao, Z.; Zhou, J.; Liang, C. Prevalence and impact of premature ejaculation in outpatients complaining of ejaculating prematurely: Using the instruments of intravaginal ejaculatory latency time and patient-reported outcome measures. Int. J. Impot. Res. 2014, 26, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Sansone, A.; Aversa, A.; Corona, G.; Fisher, A.D.; Isidori, A.M.; La Vignera, S.; Limoncin, E.; Maggi, M.; Merico, M.; Jannini, E.A. Management of premature ejaculation: A clinical guideline from the Italian Society of Andrology and Sexual Medicine (SIAMS). J. Endocrinol. Investig. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rowland, D.L.; Patrick, D.L.; Rothman, M.; Gagnon, D.D. The psychological burden of premature ejaculation. J. Urol. 2007, 177, 1065–1070. [Google Scholar] [CrossRef] [PubMed]
- Rowland, D.; Perelman, M.; Althof, S.; Barada, J.; McCullough, A.; Bull, S.; Jamieson, C.; Ho, K.F. Self-reported premature ejaculation and aspects of sexual functioning and satisfaction. J. Sex. Med. 2004, 1, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Grenier, G.; Byers, E.S. The relationships among ejaculatory control, ejaculatory latency, and attempts to prolong heterosexual intercourse. Arch. Sex. Behav. 1997, 26, 27–47. [Google Scholar] [CrossRef]
- Rosen, R.C.; Althof, S. Impact of premature ejaculation: The psychological, quality of life, and sexual relationship consequences. J. Sex. Med. 2008, 5, 1296–1307. [Google Scholar] [CrossRef]
- Revicki, D.; Howard, K.; Hanlon, J.; Mannix, S.; Greene, A.; Rothman, M. Characterizing the burden of premature ejaculation from a patient and partner perspective: A multi-country qualitative analysis. Health Qual. Life Outcomes 2008, 6. [Google Scholar] [CrossRef] [Green Version]
- Burri, A.; Giuliano, F.; McMahon, C.; Porst, H. Female partner’s perception of premature ejaculation and its impact on relationship breakups, relationship quality, and sexual satisfaction. J. Sex. Med. 2014, 11, 2243–2255. [Google Scholar] [CrossRef]
- Rowland, D.L.; Strassberg, D.S.; de Gouveia Brazao, C.A.; Slob, A.K. Ejaculatory latency and control in men with premature ejaculation: An analysis across sexual activities using multiple sources of information. J. Psychosom. Res. 2000, 48, 69–77. [Google Scholar] [CrossRef]
- Cote-Leger, P.; Rowland, D.L. Global perspectives on the three criteria for premature ejaculation: An observational study of ejaculatory latency, ejaculatory control and bother/distress. Andrologia 2020, 52. [Google Scholar] [CrossRef]
- Côté-Léger, P.; Rowland, D.L. Estimations of typical, ideal, premature ejaculation, and actual latencies by men and female sexual partners of men during partnered sex. J. Sex. Med. 2020, 17, 1448–1456. [Google Scholar] [CrossRef]
- Rosen, R.C.; McMahon, C.G.; Niederberger, C.; Broderick, G.A.; Jamieson, C.; Gagnon, D.D. Correlates to the clinical diagnosis of premature ejaculation: Results from a large observational study of men and their partners. J. Urol. 2007, 177, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.K.; Cho, S.T.; Lee, Y.S.; Lee, Y.G.; Oh, C.Y.; Yoo, C.; Cho, J.S.; Shin, T.Y.; Lee, S.K.; Lee, S.H.; et al. Can estimated intravaginal ejaculatory latency time be used interchangeably with stopwatch-measured intravaginal ejaculatory latency time for the diagnosis of lifelong premature ejaculation? Urology 2015, 85, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Symonds, T.; Perelman, M.; Althof, S.; Giuliano, F.; Martin, M.; Abraham, L.; Crossland, A.; Morris, M.; May, K. Further evidence of the reliability and validity of the premature ejaculation diagnostic tool. Int. J. Impot. Res. 2007, 19, 521–525. [Google Scholar] [CrossRef] [Green Version]
- Siddharth, K. Statistical Outliers. 2009. Available online: https://explorable.com/statistical-outliers (accessed on 18 March 2020).
- International Classification of Diseases, 11th Revision. World Health Organization. Available online: https://www.who.int/classifications/icd/en/ (accessed on 12 October 2020).
- Kempeneers, P.; Andrianne, R.; Cuddy, M.; Blairy, S. Sexual cognitions, trait anxiety, sexual anxiety, and distress in men with different subtypes of premature ejaculation and in their partners. J. Sex. Marital Ther. 2017, 44, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, U.; Schedlowski, M.; Krüger, T.H.C. Cognitive and partner-related factors in rapid ejaculation: Differences between dysfunctional and functional men. World J. Urol. 2005, 23, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Ventus, D.; Ristila, M.; Gunst, A.; Karna, A.; Arver, S.; Piha, J.; Jern, P. A longitudinal analysis of premature ejaculation symptoms raises concern regarding the appropriateness of a “Lifelong” subtype. Eur. Urol. Focus 2017, 3, 243–245. [Google Scholar] [CrossRef]
- Catania, J.A.; Dolcini, M.M.; Orellana, R.; Narayanan, V. Non-probability and probability-based sampling strategies in sexual science. J. Sex. Res. 2015, 52, 396–411. [Google Scholar] [CrossRef]
- Manzo, A.N.; Burke, J.M. Increasing response rate in web-based/internet surveys. In Handbook of Survey Methodology for the Social Sciences; Gideon, L., Ed.; Springer: New York, NY, USA, 2012; pp. 327–343. [Google Scholar]
- Ong, A.D.; Weiss, D.J. The impact of anonymity on responses to sensitive questions. J. Appl. Soc. Psychol. 2000, 30, 1691–1708. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Source | N | % Sample |
|---|---|---|
| Facebook Paid Ads | 626 | 58.07% |
| Giveaway Websites | 136 | 12.62% |
| Amazon Mechanical Turk | 98 | 9.09% |
| Reddit Organic | 98 | 9.09% |
| Reddit Paid Ads | 80 | 7.42% |
| Facebook Organic | 21 | 1.95% |
| Other or Unknown | 19 | 1.76% |
| Region | N | % Sample |
|---|---|---|
| North America | 299 | 27.74% |
| Sub-Saharan Africa | 262 | 24.30% |
| South Asia | 137 | 12.71% |
| Europe | 125 | 11.60% |
| Latin America | 113 | 10.48% |
| Oceania | 86 | 7.98% |
| Middle East | 36 | 3.34% |
| Unknown | 14 | 1.30% |
| East Asia | 4 | 0.37% |
| Central and Western Asia | 2 | 0.19% |
| Group | Men | Women | Men with PE | Men No PE 2 | Straight Men | Non-Straight Men |
|---|---|---|---|---|---|---|
| N | 572 | 499 | 154 | 321 | 398 | 174 |
| Age (mean + SD) | 33.27 (11.92) | 33.61 (11.07) | 34.95 (12.42) | 33.47 (11.78) | 34.35 (12.43) 3 | 30.82 (10.27) |
| Relationship Status 4 | ||||||
| (N and % of group) | ||||||
| Not in a relationship | 164 (28.67%) | 98 (19.84%) | 35 (22.73%) | 88 (27.41%) | 103 (25.88%) | 61 (35.06%) |
| Married | 180 (31.47%) | 159 (32.19%) | 65 (42.21%) | 102 (31.78%) | 143 (35.93%) | 37 (21.26%) |
| Relationship but not married | 209 (36.54%) | 225 (45.54%) | 49 (31.82%) | 122 (38.01%) | 142 (35.68%) | 67 (38.51%) |
| Polyamorous relationship or marriage | 11 (1.92%) | 7 (1.42%) | 4 (2.60%) | 4 (1.25%) | 6 (1.51%) | 5 (2.87%) |
| Other | 8 (1.39%) | 10 (2.02%) | 1 (0.65%) | 5 (1.56%) | 4 (1.01%) | 4 (2.30%) |
| Number (% of total) of Lifetime Sexual Partners 4 | ||||||
| 0 | 36 (6.38%) | 26 (5.23%) | 8 (5.26%) | 9 (2.82%) | 29 (7.29%) | 7 (4.02%) |
| 1 | 110 (19.50%) | 111 (22.33%) | 32 (21.05%) | 64 (20.06%) | 80 (20.10%) | 30 (17.24%) |
| Probably < 5 | 143 (25.35%) | 155 (31.19%) | 42 (27.63%) | 74 (23.20%) | 93 (23.37%) | 50 (28.74%) |
| About 6–10 | 112 (19.86%) | 94 (18.91%) | 34 (22.37%) | 61 (19.12%) | 80 (20.10%) | 32 (18.39%) |
| About 11–20 | 62 (10.99%) | 47 (9.46%) | 12 (7.89%) | 44 (13.79%) | 47 (11.81%) | 15 (8.62%) |
| Probably > 20 | 101 (17.91%) | 64 (12.88%) | 24 (15.79%) | 67 (21.00%) | 63 (15.83%) | 38 (21.84%) |
| Did not answer | 8 (1.40%) | 2 (0.40%) | 2 (1.30%) | 2 (0.62%) | 6 (1.51%) | 2 (1.15%) |
| Importance of Sex in the Relationship (mean + SD) 1 | 3.98 (0.97) | 3.82 (1.00) | 4.16 (0.93) | 4.01 (0.91) | 3.96 (1.00) | 4.03 (0.91) |
| All Men | Straight Men | Non-Straight Men | p 1 | Gay Men | p 2 |
|---|---|---|---|---|---|
| (N = 321) | (N = 153) | (N = 56) | |||
| Ejaculatory Control Difficulty 3 | 3.8 (0.10) | 3.6 (0.13) | 0.131 | 3.3 (0.19) | 0.017 |
| Ejaculatory Control Importance 4 | 2.1 (0.05) | 2.3 (0.08) | 0.068 | 2.7 (0.14) | <0.001 |
| Bother/distress if ejaculate quickly 5 | 3.1 (0.09) | 2.9 (0.13) | 0.412 | 3.3 (0.23) | 0.096 |
| Bother/distress if cannot have control 5 | 3.4 (0.08) | 3.1 (0.10) | 0.051 | 2.0 (0.19) | <0.001 |
| PE Men Only | Straight Men | Non-Straight Men | p 1 | ||
| (N = 105) | (N = 45) | ||||
| Ejaculatory Control Difficulty 3 | 5.0 (0.17) | 4.2 (0.28) | 0.015 | * | |
| Ejaculatory Control Importance 4 | 1.8 (0.08) | 1.7 (0.11) | 0.770 | * | |
| Bother/distress if ejaculate quickly 5 | 3.8 (0.14) | 3.6 (0.24) | 0.374 | * | |
| Bother/distress if cannot have control 5 | 4.0 (0.13) | 3.6 (0.20) | 0.061 | * |
| Variable | Lifelong (N = 64) | Acquired (N = 31) | p 1 |
|---|---|---|---|
| Ejaculatory Control Difficulty 2 | 4.9 (0.24) | 4.9 (0.26) | 0.97 |
| Ejaculatory Control Importance 3 | 1.8 (0.10) | 1.5 (0.12) | 0.16 |
| Distress/bother if ejaculate quickly 4 | 3.7 (0.20) | 3.9 (0.25) | 0.69 |
| Distress/bother if cannot have control 4 | 3.9 (0.17) | 3.9 (0.22) | 0.86 |
| EL (min) 5 | 2.0 (1,5) | 3.0 (1,4) | 0.72 |
| Item | MSM 1 (N = 165) | WSM 2 (N = 499) | p 3 |
|---|---|---|---|
| Importance of partner’s control over timing of ejaculation 4 | 2.90 (0.09) | 2.30 (0.05) | p < 0.001 |
| If ejaculation ≤ 1 min, deal breaker in long-term relationship? | |||
| Yes, definitely | 38 (23.0%) | 110 (22.0%) | p = 0.022 |
| Potential factor | 54 (32.7%) | 189 (37.9%) | |
| Not if otherwise satisfying sex life | 42 (25.5%) | 139 (27.9%) | |
| No, does not matter | 31 (18.8%) | 61 (12.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cote-Leger, P.; Rowland, D.L. Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”. Sexes 2020, 1, 72-86. https://doi.org/10.3390/sexes1010007
Cote-Leger P, Rowland DL. Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”. Sexes. 2020; 1(1):72-86. https://doi.org/10.3390/sexes1010007
Chicago/Turabian StyleCote-Leger, Philippe, and David L. Rowland. 2020. "Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”" Sexes 1, no. 1: 72-86. https://doi.org/10.3390/sexes1010007