
Assessment of the Integrity and Function of Human Term Placental Explants in Short-Term Culture


Abstract
:1. Introduction
2. Materials and Methods
2.1. Detailed Protocol of Placenta Villi Culture
- Subjects and Samples: The placentas were donated by pregnant women aged between 23 and 33 years old; the inclusion criteria were pregnant women without comorbidities like hypertension, preeclampsia, or diabetes, who did not take medication, and who underwent scheduled cesarean sections instead of delivery induction. These women delivered via cesarean section after reaching 37 weeks of gestation, and their babies were also in good health. Neither the pregnant women nor their children should have been actively experiencing infectious processes. Exclusion criteria included maternal, fetal, or placental pathologies. The research protocols adhered to the principles of the Declaration of Helsinki and received approval from the Bioethics Committee of the Institute of Medical Research, Faculty of Medicine, University of Antioquia (Acta No. 015, dated 24 September 2020). All participants willingly participated in the study and provided informed consent by signing the documents approved by the Bioethics Committee. A total of twelve human term placentas (>37 weeks of gestation) were included in this study.
- Collection of placentas from donors: To collect the samples, the nursing staff from the Department of Gynecology and Obstetrics at Clinica El Rosario in Medellín provided the research team with a database containing candidates scheduled for cesarean surgical procedures who met all the inclusion criteria outlined in the Subjects and Samples section. Subsequently, these candidates were contacted by a member of the research team, who thoroughly explained the purpose of this study and requested their voluntary participation as placenta donors. Participation was confirmed through the signing of informed consent forms. Once the placenta, along with the umbilical cord, was delivered, it was immediately placed in a red bag and stored in an airtight plastic container. The placenta was then promptly transported to the laboratory (BSL II) to be processed within two hours following the cesarean delivery, as described below.
2.2. Explants Culture
2.2.1. Materials
- Hermetic box;
- Red biohazard disposal bags (Merck S.A., Darmstadt, Germany);
- Surgical tools: scalpel holder (Halomedicals Systems Limited, Port Harcourt, Nigeria); style scalpel blade (Fisherbrand™); high precision #10 dissection forceps (Thermo Fisher Scientific, Waltham, MA, USA); sharp-pointed dissecting scissors (Thermo Fisher Scientific, Waltham, MA, USA);
- Aluminum tray;
- Sterile glass Petri dishes VWR®;
- 6-well plates (Thermo Fisher ScientificTM);
- Blue cap bottle with blue lid, 500 mL (Sigma Aldrich, St. Louis, MI, USA);
- Pasteur pipettes 3 mL graduated (Thermo Fisher Scientific, Waltham, MA, USA);
- Serological pipette 10 mL graduated (Merck S.A., Darmstadt, Germany);
- Micropipette of 1000 mL and 200 mL graduated (Thermo Fisher Scientific, Waltham, MA, USA);
- Waste container;
- Pipette tips with multi guard barrier tips 100–1000 μL natural, sterile (SorensonTM, Bioscience, Inc., Los Angeles, CA, USA) (Sigma Aldrich, St. Louis, MI, USA);
- Falcon™ 50 mL conical centrifuge tubes (Thermo Fisher Scientific, Waltham, MA, USA);
- Eppendorf microcentrifuge tubes 1,5 mL—clear color, safe lock caps, and DNA and RNA free (Bio-Seen) (Sigma Aldrich, St. Louis, MI, USA);
- Paper filters (Advantec A020F047A) (Sigma Aldrich, St. Louis, MI, USA).
2.2.2. Reagents
- Antiseptic alcohol (ethanol 70%).
- Phosphate-buffered saline (PBS) 1× sterile 0780-50L (Sigma Aldrich, St. Louis, MI, USA).
- Antibiotic penicillin–streptomycin solution stabilized, with 10,000 units of penicillin and streptomycin/mL, 0.1 μm filtered, BioReagent, (Sigma Aldrich, St. Louis, MI, USA).
- Fetal bovine serum (FBS) F0926-500mL (Sigma Aldrich, St. Louis, MI, USA).
- Dulbecco’s modified Eagle’s medium/nutrient mixture F-12 Ham. Cell culture tested with L-glutamine and 15 mM of HEPES, without NaHCO3. Use at 15.6 g/L (DMEM/F-12) (Sigma Aldrich, St. Louis, MI, USA).
- Sodium bicarbonate-S6014 (Sigma Aldrich, St. Louis, MI, USA)
- 10% neutral formalin at room temperature 10%/ethanol 70% at 4 °C.
- Sodium hypochlorite solution (5000 ppm).
2.2.3. Equipment
- Flow hood Nuaire Class II Type A2.
- CO2 Incubator Wiggens WCI-180.
- Inverted microscope Nikon Eclipse TS 100.
- Optical microscope Leica DM 500.
- Stereoscope Leica S6 with 1.25 × 20 zoom and a 60° viewing angle.
- Centrifuge Hermle Labnet Z 383 K.
2.2.4. Protocol for Culture of Human Placental Explants
- Area disinfection: ensure proper cleaning and disinfection of the safety cabinet using antiseptic alcohol.
- Prepare a set of sterile instruments: scissors, forceps, Pasteur pipettes, serological pipettes, and micropipettes.
- Intra-cabin placenta container: have an aluminum tray available that can hold the placenta when placed in the cabinet.
- Culture dishes: to culture the HPEs, new 6-well dishes are required; the number of dishes will depend on the researcher’s needs and objectives.
- Prepare culture dishes for seeding: Before commencing the villus isolation process, add 1.5 mL of FBS to each well of the 6-well dishes and incubate at 37 °C for 2 h. After the incubation, remove 1.3 mL of FBS, leaving a thin layer where the HPEs will be seeded. (Note: be cautious not to wash too vigorously to prevent the removal matrix of nutrients from the bottom of the well).
- Washing solution: in a sterile glass bottle with a blue screw cap, combine 500 mL of filtered sterile 1× PBS with 5 mL of antibiotic.
- Complete culture medium: In a sterile 1000 mL bottle with a blue screw cap, reconstitute the F-12 Ham medium by adding 1.5 g of bicarbonate in distilled and sterile water until the total volume reaches 1 L. Mix for 30 min and then filter it using a vacuum system with paper filters. Next, transfer 45 mL of the prepared F-12 medium to a 50 mL Falcon tube. Add 5 mL of FBS (final concentration 10%) and 500 μL of antibiotics (final concentration 1×). Seal the Falcon tube with parafilm and store it at 4 °C. When using it, allow it to equilibrate to room temperature or warm at 37 °C for 10 min.
2.3. Procedure
- Inside a Biosafety Level II laboratory, remove the placental tissue from the red bag and place it on an aluminum tray for vigorous washing with tap water.
- Make sure that the fetal side along the umbilical cord is facing upwards; remove the amnion membrane by hands to obtain the cotyledons more easily and subsequently the chorionic villi.
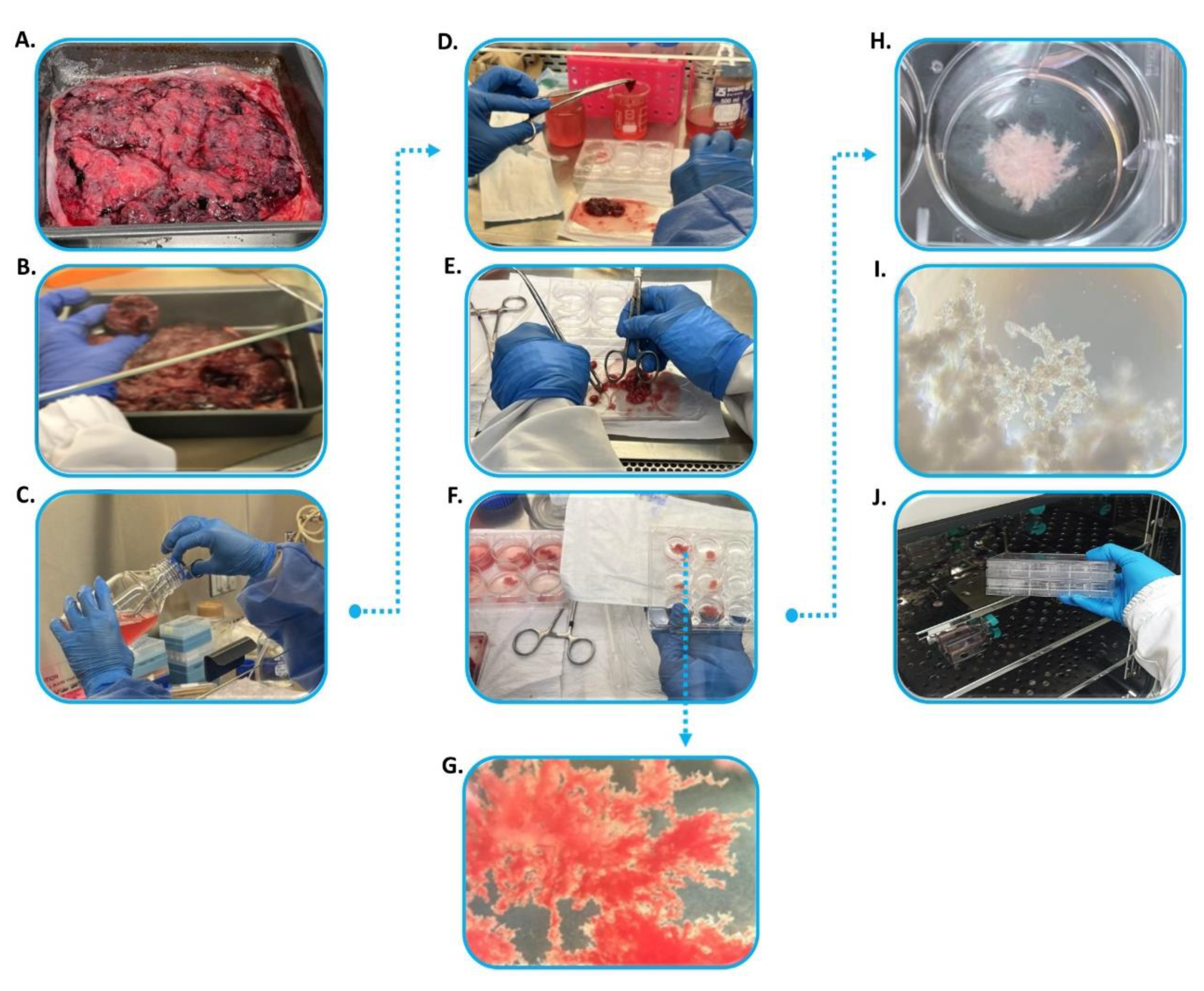
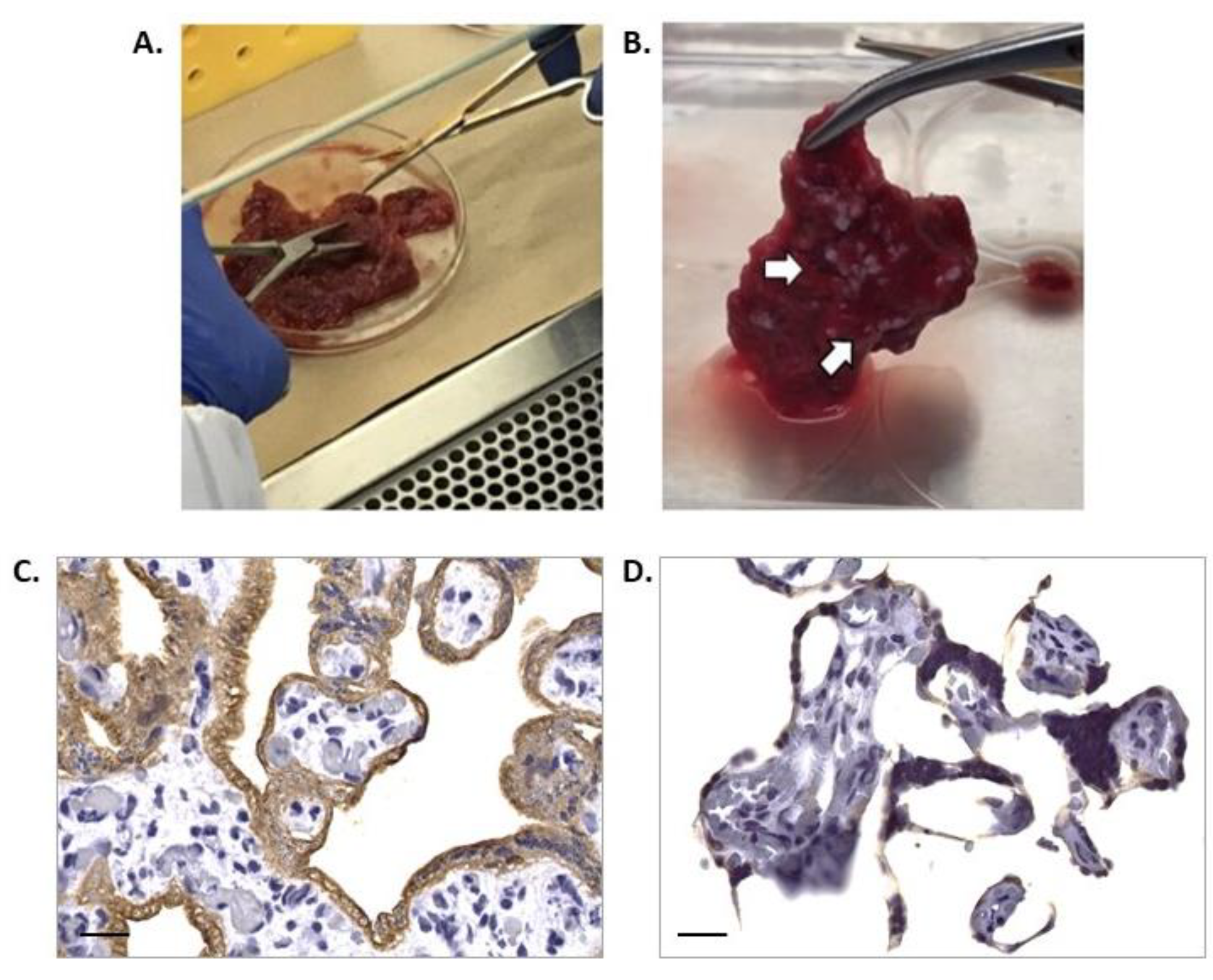
- Wash the maternal side of the surface containing cotyledons to remove large blood clots and necrosis areas using tap water. At this point, the delivered tissue should appear in good condition, having a ‘healthy’ pinkish color and lacking large blood clots and greenish necrotic centers (Figure 2A). The condition of the tissue is also dependent on how quickly it is delivered for processing [7].
- Introduce the washed tissue, placed on an aluminum tray, into a sterile laminar flow cabin for cotyledons dissection. The dissection can be performed manually, using a blade or scalpel, to obtain two or three cotyledons in different positions between the distal and central portions of the maternal surface. These cotyledons should have dimensions of around 3 × 3 cm and 2 cm in depth (Figure 2B). All cotyledons dissected must originate from healthy, pinkish region.
- Transfer the cotyledons to a glass jar containing a washing solution (sterile PBS 1× plus antibiotic 1%) (Figure 2C).
- Wash the cotyledons inside the Falcon tubes containing 50 mL of washing solution, performing approximately 10 inversions to thoroughly clean the tissue and remove any excess blood and clots that may have formed.
- Transfer the cotyledon into a 100 mm Petri dish containing 10–20 mL of washing solution to obtain the HPEs (Figure 2D). Dissect the cotyledon into small blocks fragments measuring around 4 mm. If capillaries are present, remove them using sterile forceps and scissors.
- Hold the villi using a blunt surface to prevent tissue breakage and obtain thin pieces with dimensions of approximately 2–3 mm at most (Figure 2E). Avoid dissecting larger pieces than ∼2 mm thickness; although they are easier to cut, their viability in culture can be compromised due to necrosis at their center, as a consequence of nutrient deficiency in the middle of the block [7].
- Remove erythrocyte excess by sequential washing the thin villous pieces in three wells of a six-well dish containing the washing solution (Figure 2F).
- During the washing process, perform a morphological inspection of the HPEs under a stereoscope to ensure tissue integrity (Figure 2G).
- A maximum of three placenta villi can be washed in the same well. At this point the villous should exhibit a light pink color (Figure 2H).
- To culture the HPEs, prepare the culture matrix in advance by adding 1.5 mL of FBS at the bottom of the culture wells and pre-incubate for 2 h at 37 °C.
- Following the matrix incubation, take out the six-well plate(s) from the incubator and remove 1 mL of the FBS added. Then, seed the HPEs (no more than three per well) and add 2 mL of complete F-12 (Figure 2H).
- Confirm the placental villi integrity under optical microscopy (Figure 2I) and culture under standard conditions, with 5% CO2 at 37 °C for a period of 72 h, with daily medium (F12 10% FBS) changes (Figure 2J). Make sure to remove the medium carefully by the walls of plates during changes to avoid releasing the adhesion layer formed by the trophoblast.
- Expose the placental villi to an external stimulus of interest. We recommend initiating treatments after 48–72 h of culture due to lower LDH activity (See Section 2.4.1.) and to ensure the prevention of bacterial or fungal contamination. Furthermore, this period is optimal for collecting supernatant samples to analyze metabolites of interest, such as LDH, hCG, other hormones, cytokines, and angiogenic factors.
- Dispose the remaining minced explants in a biohazard waste bag. All liquid waste should be collected in a beaker containing sodium hypochlorite solution and appropriately discarded.
2.4. Methodological Approaches for Integrity and Function Validation
2.4.1. Measurement of Viability through Lactate Dehydrogenase (LDH) Activity Detection
2.4.2. Detection of Endocrine Mediators and Angiogenic Factors to Assess HPEs Functionality
2.4.3. Histochemical Staining and Analysis
2.4.4. Immunohistochemistry Staining and Analysis
2.4.5. Evaluation of Apoptosis Using TUNEL Assay
2.4.6. Measurement of Cytokines by Flow Cytometry
2.5. Statistics
3. Results
3.1. Macroscopic Evaluation of Placental Tissue Integrity
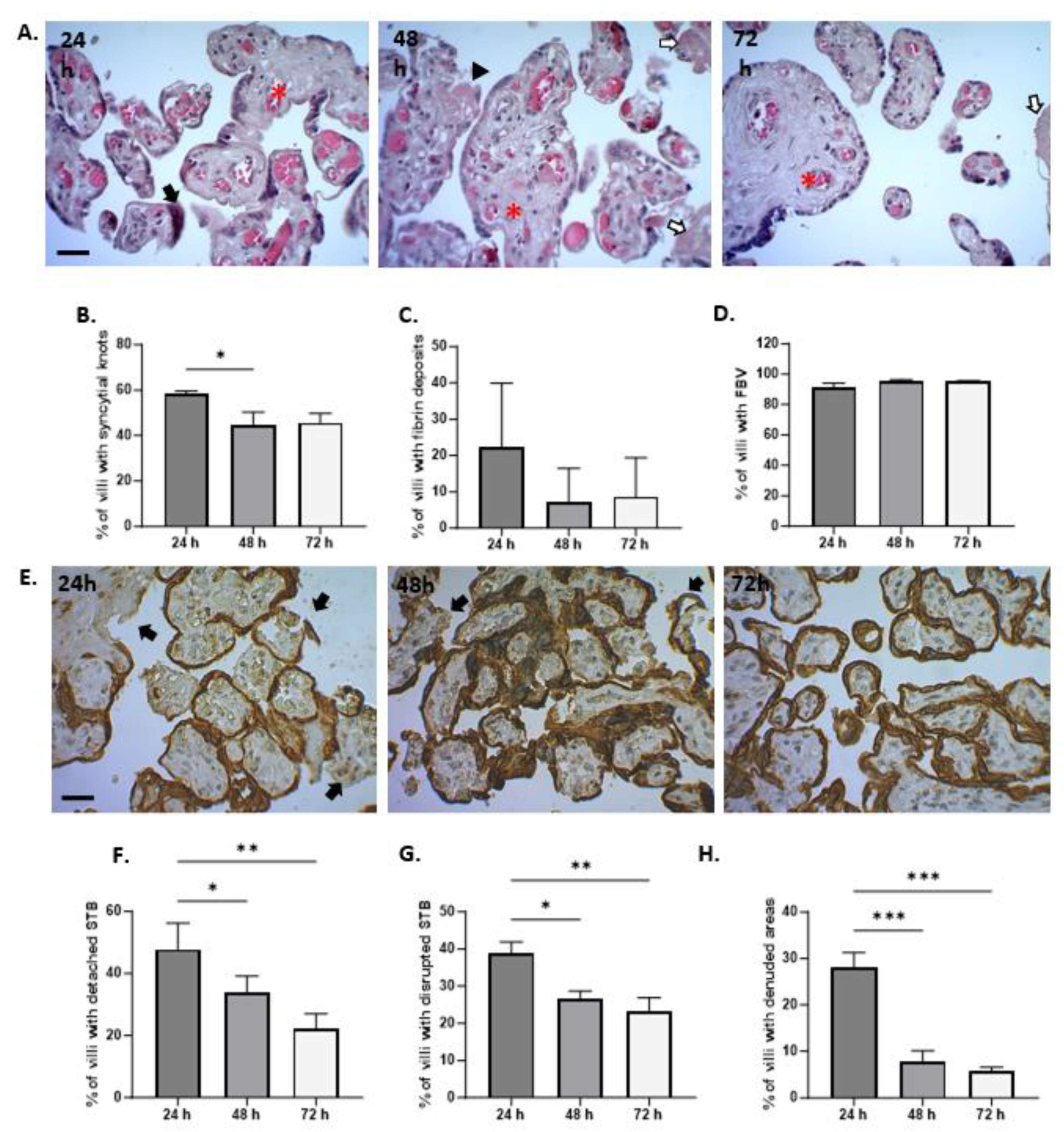
3.2. Microscopic Evaluation of HPEs Integrity
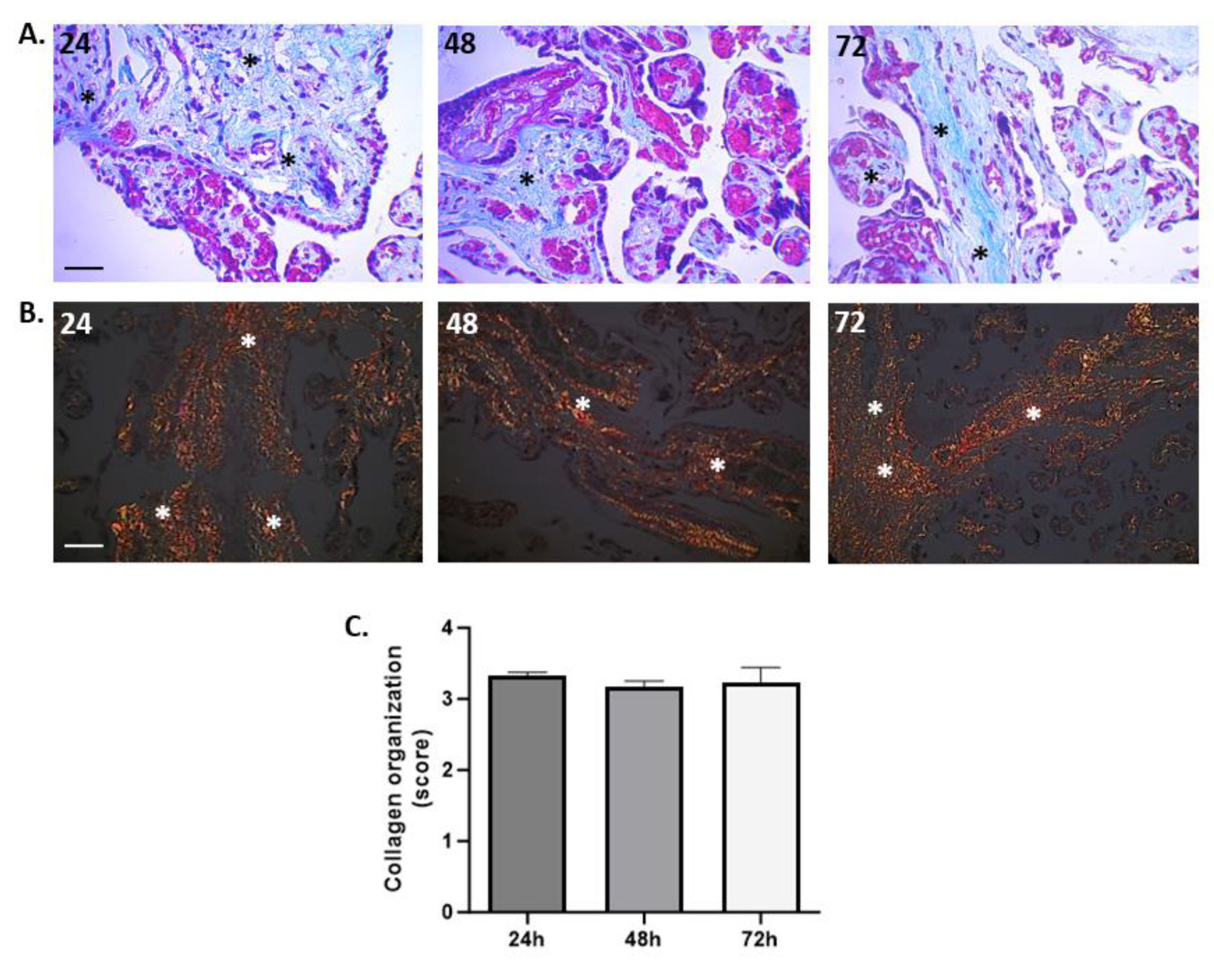
3.3. Organization of Collagen Fibers
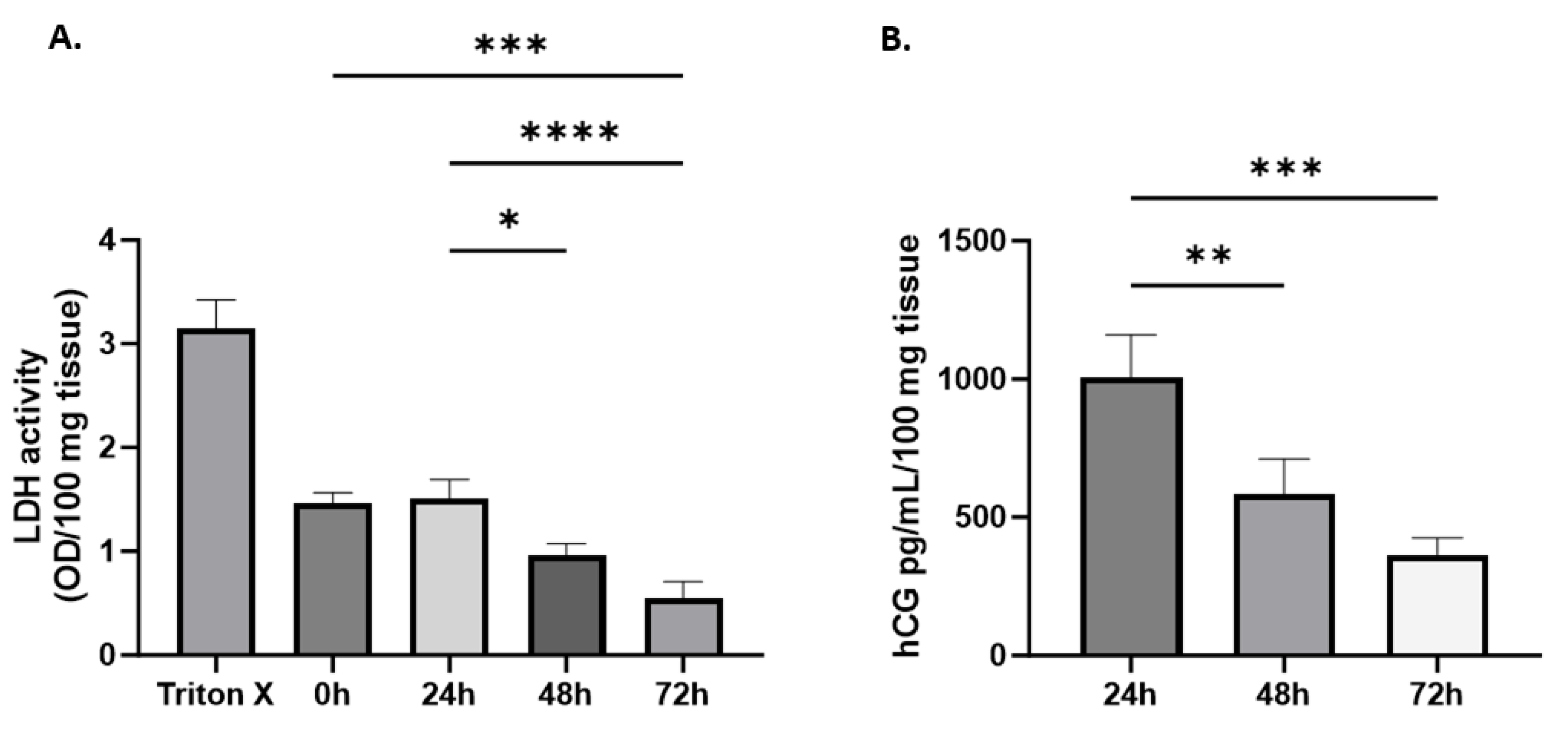
3.4. Tissue Viability and Endocrine Function in HPEs
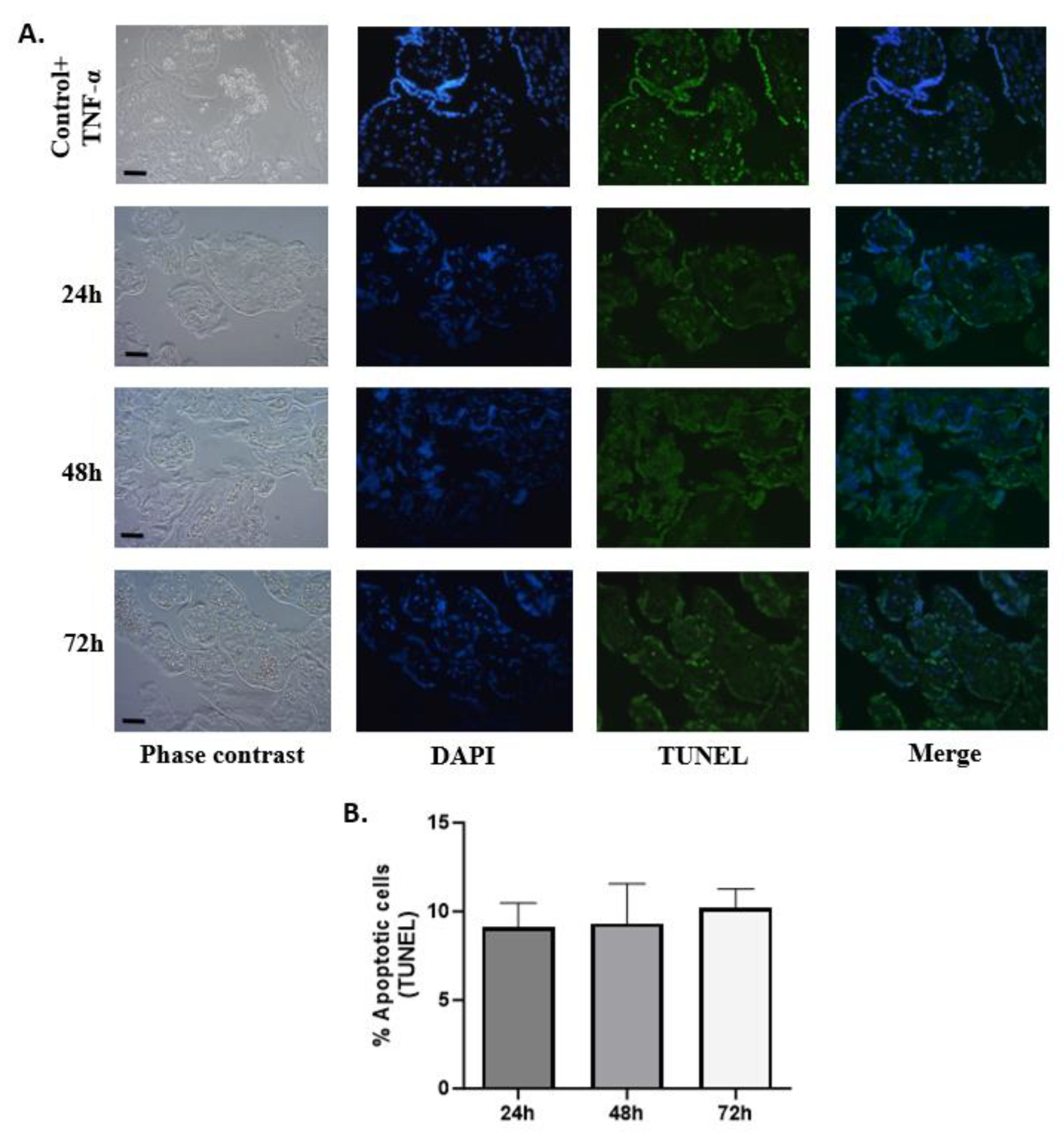
3.5. DNA Fragmentation in HPEs Cells Using TUNEL Assay
3.6. Production and Release of Cytokines and Angiogenic Factors
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Turco, M.Y.; Moffett, A. Development of the human placenta. Development 2019, 146, dev163428. [Google Scholar] [CrossRef] [PubMed]
- Ander, S.E.; Diamond, M.S.; Coyne, C.B. Immune responses at the maternal-fetal interface. Sci. Immunol. 2019, 4, eaat6114. [Google Scholar] [CrossRef] [PubMed]
- Dusza, H.M.; van Boxel, J.; van Duursen, M.B.M.; Forsberg, M.M.; Legler, J.; Vähäkangas, K.H. Experimental human placental models for studying uptake, transport and toxicity of micro- and nanoplastics. Sci. Total Environ. 2023, 860, 160403. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, M.A.; Fernando, R.C.; Gardner, L.; Hollinshead, M.S.; Burton, G.J.; Moffett, A.; Turco, M.Y. Establishment and differentiation of long-term trophoblast organoid cultures from the human placenta. Nat. Protoc. 2020, 15, 3441–3463. [Google Scholar] [CrossRef] [PubMed]
- Simán, C.M.; Sibley, C.P.; Jones, C.J.; Turner, M.A.; Greenwood, S.L. The functional regeneration of syncytiotrophoblast in cultured explants of term placenta. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 280, R1116–R1122. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.K.; Genbacev, O.; Turner, M.A.; Aplin, J.D.; Caniggia, I.; Huppertz, B. Human placental explants in culture: Approaches and assessments. Placenta 2005, 26, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Grivel, J.C.; Margolis, L. Use of human tissue explants to study human infectious agents. Nat. Protoc. 2009, 4, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Crocker, I.P.; Tansinda, D.M.; Jones, C.J.; Baker, P.N. The influence of oxygen and tumor necrosis factor-alpha on the cellular kinetics of term placental villous explants in culture. J. Histochem. Cytochem. 2004, 52, 749–757. [Google Scholar] [CrossRef]
- Goncalves, J.M.; Casart, Y.C.; Camejo, M.I. Nitric oxide and oxidative stress in placental explant cultures. Syst. Biol. Reprod. Med. 2016, 62, 11–16. [Google Scholar] [CrossRef]
- Turner, M.A.; Roulstone, C.J.; Desforges, M.; Cretney, M.; Champion, E.; Lacey, H.; Greenwood, S.L. The extent and variability of effects of culture conditions on the secretion of human chorionic gonadotrophin and interleukin-6 by human, term placental explants in culture. Placenta 2006, 27, 98–102. [Google Scholar] [CrossRef]
- Mayhew, T.M.; Barker, B.L. Villous trophoblast: Morphometric perspectives on growth, differentiation, turnover and deposition of fibrin-type fibrinoid during gestation. Placenta 2001, 22, 628–638. [Google Scholar] [CrossRef] [PubMed]
- Eliesen, G.A.M.; van Hove, H.; Meijer, M.H.; van den Broek, P.H.H.; Pertijs, J.; Roeleveld, N.; van Drongelen, J.; Russel, F.G.M.; Greupink, R. Toxicity of anticancer drugs in human placental tissue explants and trophoblast cell lines. Arch. Toxicol. 2021, 95, 557–571. [Google Scholar] [CrossRef] [PubMed]
- Gibson-Corley, K.N.; Olivier, A.K.; Meyerholz, D.K. Principles for valid histopathologic scoring in research. Vet. Pathol. 2013, 50, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Liempi, A.; Castillo, C.; Medina, L.; Galanti, N.; Maya, J.D.; Parraguez, V.H.; Kemmerling, U. Comparative ex vivo infection with Trypanosoma cruzi and Toxoplasma gondii of human, canine and ovine placenta: Analysis of tissue damage and infection efficiency. Parasitol. Int. 2020, 76, 102065. [Google Scholar] [CrossRef]
- Gavrieli, Y.; Sherman, Y.; Ben-Sasson, S.A. Identification of programmed cell death in situ via specific labeling of nuclear DNA fragmentation. J. Cell Biol. 1992, 119, 493–501. [Google Scholar] [CrossRef]
- Huang, Q.; Yang, Y.; Luo, C.; Wen, Y.; Liu, R.; Li, S.; Chen, T.; Sun, H.; Tang, L. An efficient protocol to generate placental chorionic plate-derived mesenchymal stem cells with superior proliferative and immunomodulatory properties. Stem Cell Res. Ther. 2019, 10, 301. [Google Scholar] [CrossRef]
- Roberts, V.H.; Gaffney, J.E.; Lewandowski, K.S.; Schabel, M.C.; Morgan, T.K.; Frias, A.E. A standardized method for collection of human placenta samples in the age of functional magnetic resonance imaging. Biotechniques 2019, 67, 45–49. [Google Scholar] [CrossRef]
- Maxwell, C.; Huppertz, B.; Kingdom, J. Fibroblast growth factor-4 induces cytotrophoblast proliferation in floating first trimester villous explants denuded of overlying syncytium. J. Soc. Gynecol. Investig. 2003, 10, 268A. [Google Scholar]
- Baergen, R.N. Indications for submission and macroscopic examination of the placenta. APMIS 2018, 126, 544–550. [Google Scholar] [CrossRef]
- Parks, W. Increased Syncytial Knot Formation: A Practical Guide; Springer: Cham, Switzerland, 2019; pp. 131–137. [Google Scholar] [CrossRef]
- Burton, G.J.; Clindova-Davies, T.; Wa, Y.H.; Jauniaux, E. Hypoxia and Reproductive Health: Oxygen and development of the human placenta. Soc. Reprod. Fertil. 2021, 161, F53–F65. [Google Scholar] [CrossRef]
- Nelson, D.M. Apoptotic changes occur in syncytiotrophoblast of human placental villi where fibrin type fibrinoid is deposited at discontinuities in the villous trophoblast. Placenta 1996, 17, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Huppertz, B.; Frank, H.G.; Reister, F.; Kingdom, J.; Korr, H.; Kaufmann, P. Apoptosis cascade progresses during turnover of human trophoblast: Analysis of villous cytotrophoblast and syncytial fragments in vitro. Lab. Investig. 1999, 79, 1687–1702. [Google Scholar] [PubMed]
- Caniggia, I.; Grisaru-Gravnosky, S.; Kuliszewsky, M.; Post, M.; Lye, S.J. Inhibition of TGF-beta 3 restores the invasive capability of extravillous trophoblasts in preeclamptic pregnancies. J. Clin. Investig. 1999, 103, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Crocker, I.P.; Tanner, O.M.; Myers, J.E.; Bulmer, J.N.; Walraven, G.; Baker, P.N. Syncytiotrophoblast degradation and the pathophysiology of the malaria-infected placenta. Placenta 2004, 25, 273–282. [Google Scholar] [CrossRef] [PubMed]
- James, J.L.; Lissaman, A.; Nursalim, Y.N.S.; Chamley, L.W. Modelling human placental villous development: Designing cultures that reflect anatomy. Cell Mol. Life Sci. 2022, 79, 384. [Google Scholar] [CrossRef] [PubMed]
- Pidoux, G.; Gerbaud, P.; Laurendeau, I.; Guibourdenche, J.; Bertin, G.; Vidaud, M.; Evain-Brion, D.; Frendo, J.L. Large variability of trophoblast gene expression within and between human normal term placentae. Placenta 2004, 25, 469–473. [Google Scholar] [CrossRef]
- Yockey, L.J.; Iwasaki, A. Interferons and Proinflammatory Cytokines in Pregnancy and Fetal Development. Immunity 2018, 49, 397–412. [Google Scholar] [CrossRef]
- Hayashi, M.; Ueda, Y.; Ohkura, T.; Inaba, N. Interleukin-6 concentrations in the placenta and blood in normal pregnancies and preeclampsia. Horm. Metab. Res. 2005, 37, 419–424. [Google Scholar] [CrossRef]
- Faye, A.; Pornprasert, S.; Dolcini, G.; Ave, P.; Taïeb, J.; Taupin, J.L.; Derrien, M.; Huerre, M.; Barré-Sinoussi, F.; Chaouat, G.; et al. Evaluation of the placental environment with a new in vitro model of histocultures of early and term placentae: Determination of cytokine and chemokine expression profiles. Placenta 2005, 26, 262–267. [Google Scholar] [CrossRef]
- Hanna, N.; Bonifacio, L.; Weinberger, B.; Reddy, P.; Murphy, S.; Romero, R.; Sharma, S. Evidence for interleukin-10-mediated inhibition of cyclo-oxygenase-2 expression and prostaglandin production in preterm human placenta. Am. J. Reprod. Immunol. 2006, 55, 19–27. [Google Scholar] [CrossRef]
- Hanna, N.; Hanna, I.; Hleb, M.; Wagner, E.; Dougherty, J.; Balkundi, D.; Padbury, J.; Sharma, S. Gestational age-dependent expression of IL-10 and its receptor in human placental tissues and isolated cytotrophoblasts. J. Immunol. 2000, 164, 5721–5728. [Google Scholar] [CrossRef] [PubMed]
- Moussa, M.; Roques, P.; Fievet, N.; Menu, E.; Maldonado-Estrada, J.G.; Brunerie, J.; Frydman, R.; Fritel, X.; Herve, F.; Chaouat, G. Placental cytokine and chemokine production in HIV-1-infected women: Trophoblast cells show a different pattern compared to cells from HIV-negative women. Clin. Exp. Immunol. 2001, 125, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Nevo, O.; Soleymanlou, N.; Wu, Y.; Xu, J.; Kingdom, J.; Many, A.; Zamudio, S.; Caniggia, I. Increased expression of sFlt-1 in in vivo and in vitro models of human placental hypoxia is mediated by HIF-1. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 291, R1085–R1093. [Google Scholar] [CrossRef] [PubMed]
- Iliodromiti, Z.; Antonakopoulos, N.; Sifakis, S.; Tsikouras, P.; Daniilidis, A.; Dafopoulos, K.; Botsis, D.; Vrachnis, N. Endocrine, paracrine, and autocrine placental mediators in labor. Hormones 2012, 11, 397–409. [Google Scholar] [CrossRef]
- Garcia-Ruíz, G.; Flores-Espinosa, P.; Preciado-Martínez, E.; Bermejo-Martínez, L.; Espejel-Nuñez, A.; Estrada-Gutierrez, G.; Maida-Claros, R.; Flores-Pliego, A.; Zaga-Clavellina, V. In vitro progesterone modulation on bacterial endotoxin-induced production of IL-1β, TNFα, IL-6, IL-8, IL-10, MIP-1α, and MMP-9 in pre-labor human term placenta. Reprod. Biol. Endocrinol. 2015, 13, 115. [Google Scholar] [CrossRef]
- Patel, N.; Alsat, E.; Igout, A.; Baron, F.; Hennen, G.; Porquet, D.; Evain-Brion, D. Glucose inhibits human placental GH secretion, in vitro. J. Clin. Endocrinol. Metab. 1995, 80, 1743–1746. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histological Findings | Definition | Appearance (Scale Bar 25 μm) | Staining |
|---|---|---|---|
| Tissue infarction | The ischemic area of the villi due to the interruption of blood flow. |  | H&E |
| Syncytial node | Aggregates of syncytial nuclei on the surface of the villi. |  | H&E |
| Fibrin deposits | Accumulation of fibrin in the stroma of the villus or around it. |  | H&E |
| Capillaries | Number of capillaries per villus. |  | H&E |
| Membrane detachment | Represents a space observed between the trophoblast membrane and the villus; there is no complete union between them. |  | CK-7 |
| Membrane disrupted | Represents a membrane break; loss of continuity of the trophoblast membrane. |  | CK-7 |
| Membrane denudation | Represents a villus partially or completely devoid of trophoblast membrane. |  | CK-7 |
| Score | Organization of Collagen I | Appearance |
|---|---|---|
| 1 | Absence of collagen birefringence |  |
| 2 | Low collagen birefringence |  |
| 3 | Moderate collagen birefringence |  |
| 4 | Strong collagen birefringence |  |
| Cytokines [pg/mL] | 24 h | 48 h | 72 h | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Min. | Max. | Mean ± SEM | Min. | Max. | Mean ± SEM | Min. | Max. | Mean ± SEM | |
| IL-6 | 2541 | 46,410 | 18,373 ± 4416 | 7504 | 4733 | 25,133 ± 4106 | 1974 | 47,314 | 25,067 ± 4244 |
| IFN-γ | 47.2 | 41.5 | 44.6 ± 9.0 | 135.7 | 105.8 | 141.7 ± 6.9 | 79.25 | 70.29 | 72.19 ± 10.9 |
| IL-4 | 40.1 | 115.3 | 69.2 ± 8.3 | 40.1 | 115.3 | 69.2 ± 8.3 | 40.2 | 115.4 | 69.2 ± 8.3 |
| IL-17 | 26.0 | 68.9 | 43.6 ± 4.6 | 22.7 | 69.1 | 41.1 ± 5.0 | 23.3 | 70.8 | 42.7 ± 5.0 |
| IL-10 | 4.5 | 18.9 | 8.5 ± 1.4 | 4.4 | 21.4 | 9.2 ± 1.7 | 3.4 | 16.5 | 8.7 ± 1.2 |
| IL-2 | 4.2 | 12.2 | 7.0± 0.8 | 3.7 | 11.1 | 6.8 ± 0.8 | 4.0 | 11.8 | 6.9 ± 0.9 |
| Angiogenic factors [pg/mL] | |||||||||
| sFLT-1 | 3574.0 | 11,275.0 | 7502 ± 998 | 3371.0 | 12,245.0 | 7490 ± 1147 | 2431.0 | 12,111.0 | 7013 ± 1143 |
| Endoglin | 32.01 | 98.7 | 62.9 ± 9.4 | 34.59 | 94.37 | 60.1 ± 8.7 | 30.57 | 105.2 | 58.9 ± 10.1 |
| Ang-1 | 48.01 | 59.21 | 53.7 ± 4.2 | 48.12 | 57.61 | 51.5 ± 3.4 | 45.86 | 54.84 | 49.9 ± 3.5 |
| VEGF | 32.7 | 67.3 | 44.3 ± 7.8 | 35.3 | 88.5 | 59.8 ± 13.2 | 31.6 | 76.3 | 48.2 ± 9.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Guzmán, C.; García, A.M.; Marín, P.; Vásquez, A.M. Assessment of the Integrity and Function of Human Term Placental Explants in Short-Term Culture. Methods Protoc. 2024, 7, 16. https://doi.org/10.3390/mps7010016
López-Guzmán C, García AM, Marín P, Vásquez AM. Assessment of the Integrity and Function of Human Term Placental Explants in Short-Term Culture. Methods and Protocols. 2024; 7(1):16. https://doi.org/10.3390/mps7010016
Chicago/Turabian StyleLópez-Guzmán, Carolina, Ana María García, Paula Marín, and Ana María Vásquez. 2024. "Assessment of the Integrity and Function of Human Term Placental Explants in Short-Term Culture" Methods and Protocols 7, no. 1: 16. https://doi.org/10.3390/mps7010016