
Protocol for a Randomized Control Trial for Tungiasis Treatment in Homa Bay County, Kenya: Dimeticone versus Sodium Carbonate
 , , and
, , and 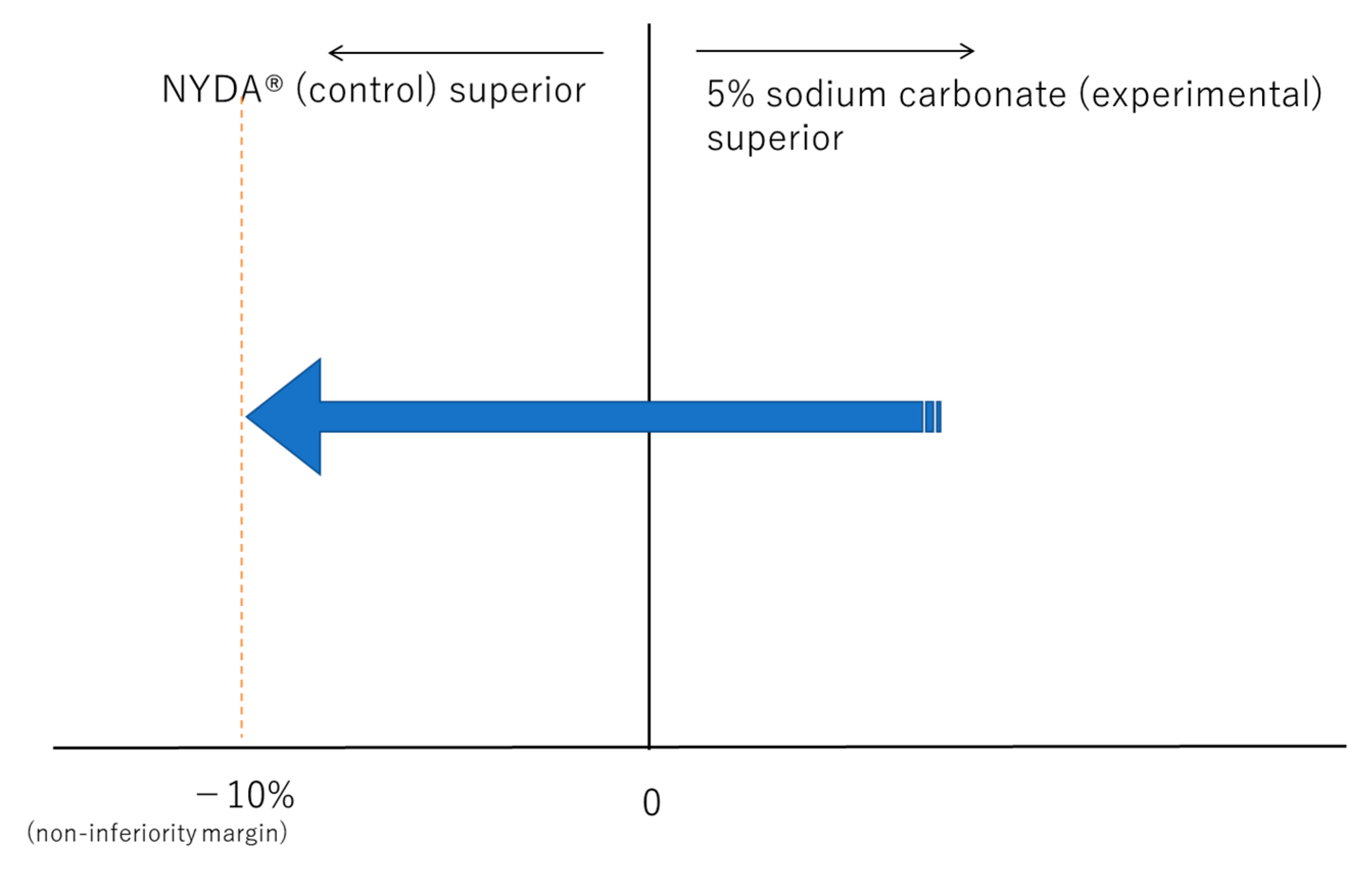{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Treatment Options for Tungiasis
Locally Available Treatments
2. Experimental Design
2.1. Objectives
- (1)
- To compare the cure rates of the two treatments (5% sodium carbonate and dimeticone) within seven days.
- (2)
- To assess the safety of the two treatments by determining the incidence of adverse effects.
- (3)
- To compare the acute pathology scores of the two treatments.
- (4)
- To assess the acceptability of the two treatments in the community.
2.2. Justification
2.3. Study Design
2.4. Study Area
2.5. Study Population
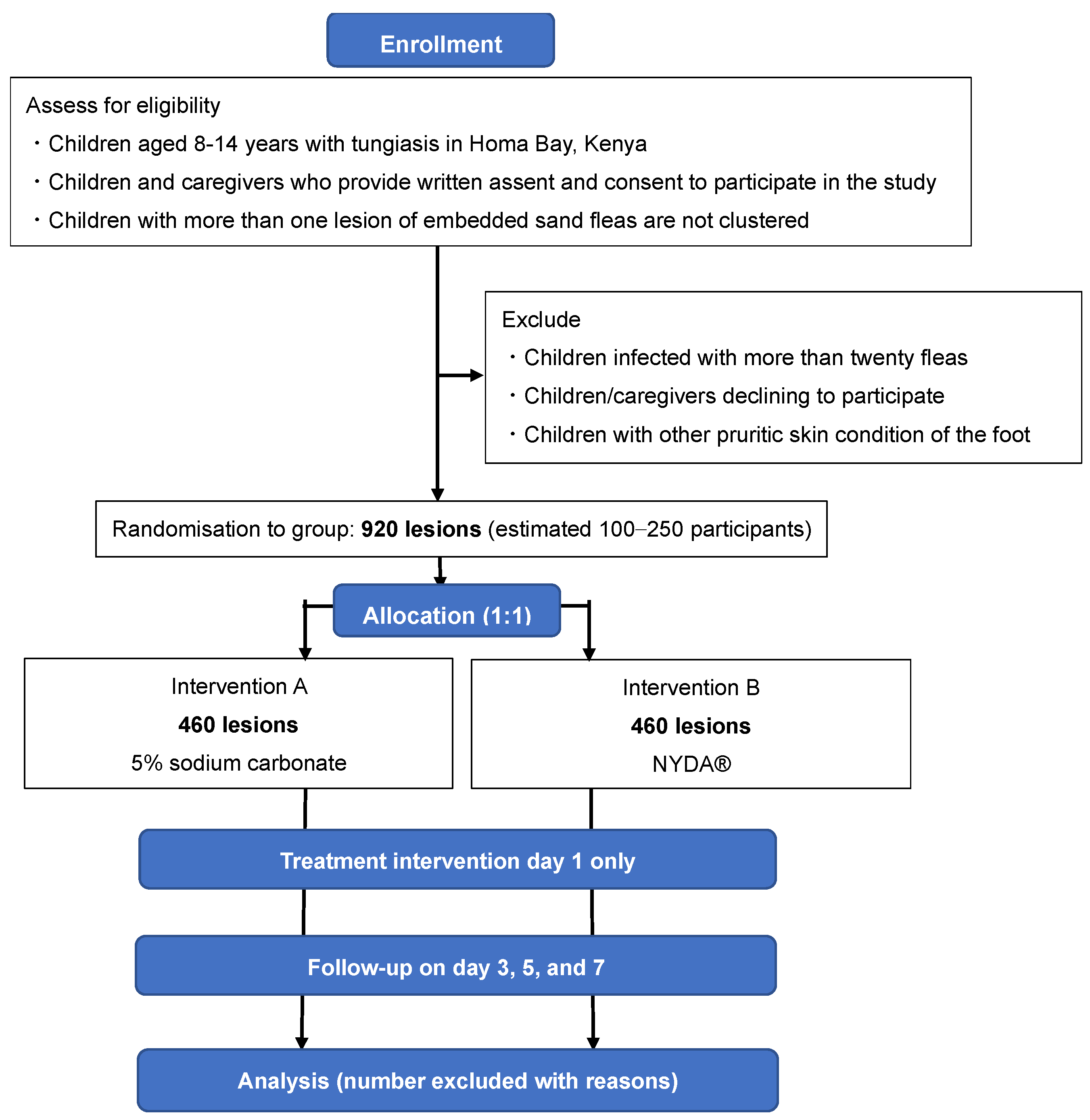
2.5.1. Eligibility Criteria
- Children aged 8 to 14 years who have been infected with tungiasis in Homa Bay, Kenya (the most commonly affected age-group, and who can reliably answer questions).
- Children and caregivers who provide written assent and consent to participate in the study.
- Children who have more than one lesion of embedded sand-fleas that are independent (not clustered) and easily observable, on both feet.
2.5.2. Exclusion Criteria
- Children infected with more than twenty fleas. These are defined as severe cases [25] and need to be immediately referred to the nearest health facility for treatment or to the medical doctor cooperating in this research, for consultation.
- Children/caregivers who decline to participate.
- Children with other pruritic skin-conditions on the foot.
2.6. Outcome Measures
2.7. Non-Inferiority Margin Settings
- Estimating the risk ratio of standard intervention:
- 2.
- Setting the risk difference of standard intervention using the lower limit of the effect estimate:
- 3.
- Setting the retention rate and calculating the non-inferiority margin (Wangge et al. [30]):
- 4.
- Range of interpretation: ±10%.
2.8. Sample-Size Calculation
3. Procedure
3.1. Sampling and Recruitment
3.2. Randomisation, Allocation, and Blinding
3.3. Recruitment Strategy
3.4. Study Tools
- − Questionnaire for study participants: a structured questionnaire;
- − Case observation/record form;
- − Adverse event/effect record form.
3.5. Data Collection and Storage
3.6. Pre-Study
4. Expected Results
4.1. Statistical Analysis
4.2. Monitoring Plan for the Study
4.3. Early Termination of the Study (Stopping Rule)
4.4. Adverse Events/Effects
4.5. Hazards and Risks Associated with the Study
4.6. Confidentiality
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heukelbach, J.; de Oliveira, F.A.; Hesse, G.; Feldmeier, H. Tungiasis: A neglected health problem of poor communities. Trop. Med. Int. Health 2001, 6, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Eisele, M.; Heukelbach, J.; Van Marck, E.; Mehlhorn, H.; Meckes, O.; Franck, S.; Feldmeier, H. Investigations on the biology, epidemiology, pathology and control of Tunga penetrans in Brazil: I. Natural history of tungiasis in man. Parasitol. Res. 2003, 90, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Nagy, N.; Abari, E.; D’Haese, J.D.; Calheiros, C.; Heukelbach, J.; Mencke, N.; Feldmeier, H.; Mehlhorn, H. Investigations on the life cycle and morphology of Tunga penetrans in Brazil. Parasitol. Res. 2007, 101 (Suppl. S2), S233–S242. [Google Scholar] [CrossRef] [PubMed]
- Linardi, P.M.; Calheiros, C.M.L.; Campelo-Junior, E.B.; Duarte, E.M.; Heukelbach, J.; Feldmeier, H. Occurrence of the off-host life stages of Tunga penetrans (Siphonaptera) in various environments in Brazil. Ann. Trop. Med. Parasitol. 2010, 104, 337–345. [Google Scholar] [CrossRef]
- Feldmeier, H.; Heukelbach, J.; Ugbomoiko, U.S.; Sentongo, E.; Mbabazi, P.; von Samson-Himmelstjerna, G.; Krantz, I.; International Expert Group for Tungiasis. Tungiasis—A neglected disease with many challenges for global public health. PLOS Negl. Trop. Dis. 2014, 8, e3133. [Google Scholar] [CrossRef] [Green Version]
- Muehlen, M.; Heukelbach, J.; Wilcke, T.; Winter, B.; Mehlhorn, H.; Feldmeier, H. Investigations on the biology, epidemiology, pathology and control of Tunga penetrans in Brazil II. Prevalence, parasite load and topographic distribution of lesions in the population of a traditional fishing village. Parasitol. Res. 2003, 90, 449–455. [Google Scholar] [CrossRef]
- Ahadi Kenya Trust. The Jigger Menace in Kenya Report; Ahadi Kenya Trust: Nairobi, Kenya, 2011; Volume 2, Available online: http://www.jigger-ahadi.org/reports.html (accessed on 24 December 2019).
- Bruce, C.O.; Knigin, T.D.; Yolles, S.F. A discussion of the chigoe (Tunga penetrans) based on experiences in British Guiana. Mil. Surg 1942, 82, 446–452. [Google Scholar] [CrossRef]
- Kiire, C.F. The epidemiology and prophylaxis of hepatitis B in sub-Saharan Africa: A view from tropical and subtropical Africa. Gut Gastroent Hepatol. 1996, 38, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madhava, V.; Burgess, C.; Drucker, E. Epidemiology of chronic hepatitis C virus infection in sub-Saharan Africa. Lancet 2002, 2, 293–302. [Google Scholar] [CrossRef]
- Republic of Kenya Ministry of Health. National Policy Guidelines on Prevention and Control of Jigger Infestations. Available online: http://www.jigger-ahadi.org/National%20Policy%20Guidelines%20for%20Prevention%20and%20Control.pdf. (accessed on 1 June 2021).
- Elson, L.; Randu, K.; Feldmeier, H.; Fillinger, U. Efficacy of a mixture of neem seed oil (Azadirachta indica) and coconut oil (Cocos nucifera) for topical treatment of tungiasis. A randomized controlled, proof-of-principle study. PLoS Negl. Trop. Dis. 2019, 13, e0007822, Published 2019 Nov 22. [Google Scholar] [CrossRef]
- Gitau, A.K.; Oyieke, F.A.; Evan, M. Efficacy of Coconut Oil in The Control of Acute Tungiasis. Int. J. New Technol. Res. 2015, 1, 85–92. [Google Scholar]
- Ambenje, D.N.; Otieno, C.A. A rapid appraisal of the efficacy of sodium carbonate in the management of Tunga penetrans infestation at Uuna primary school in Karemo division, Siaya District, Kenya. J. Commun. Med. Health Educ. 2016, 6, 1000394. [Google Scholar]
- Thielecke, M.; Nordin, P.; Ngomi, N.; Feldmeier, H. Treatment of Tungiasis with dimeticone: A proof-of-principle study in rural Kenya. PLoS Negl. Trop Dis. 2014, 8, e3058. [Google Scholar] [CrossRef] [Green Version]
- Tardin Martins, A.C.; Brito, A.R.; Kurizky, P.S.; Gonçalves, R.G.; Santana, Y.R.T.; Carvalho, F.C.A.; Gomes, C.M. The efficacy of topical, oral and surgical interventions for the treatment of tungiasis: A systematic review of the literature. PLoS Negl. Trop Dis. 2021, 15, e0009722. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, Y. [Balneotherapy]. Onsenryouhou; Nanzandou: Tokyo, Japan, 2001; Volume 28. (In Japanese) [Google Scholar]
- Mabelya, L.; van Palenstein Helderman, W.H.; van’t Hof, M.A.; König, K.G. Dental fluorosis and the use of a high fluoride-containing trona tenderizer (magadi). Community Dent Oral Epidemiol. 1997, 25, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Human and Environmental Risk Assessment. Human and Environmental Risk Assessment on Ingredients of Household Cleaning Products Sodium carbonate (CAS No. 497-19-8). Edition 2.0, 2005. Available online: https://www.heraproject.com/files/10-F-05_HERA_sodium_carbonate_revised_version2%20.pdf (accessed on 27 February 2020).
- Feldmeier, H. Treatment of pediculosis capitis: A critical appraisal of the current literature. Am. J. Clin. Dermatol. 2014, 15, 401–412. [Google Scholar] [CrossRef]
- Richling, I.; Böckeler, W. Lethal effects of treatment with a special dimeticone formula on head lice and house crickets (Orthoptera, Ensifera: Acheta domestica and Anoplura, Phthiraptera: Pediculus humanus). Insights into physical mechanisms. Arzneimittelforschung 2008, 58, 248–254. [Google Scholar] [CrossRef]
- Ihde, E.S.; Boscamp, J.R.; Loh, J.M.; Rosen, L. Safety and efficacy of a 100% dimethicone pediculocide in school-age children. BMC Pediatr. 2015, 15, 70. [Google Scholar] [CrossRef] [Green Version]
- Nair, B. Cosmetic Ingredients Review Expert Panel. Final report on the safety assessment of stearoxy dimethicone, dimethicone, methicone, amino bispropyl dimethicone, aminopropyl dimethicone, amodimethicone, amodimethicone hydroxystearate, behenoxy dimethicone, C24-28 alkyl methicone, C30-45 alkyl Methicone, C30-45 alkyl dimethicone, cetearyl methicone, cetyl dimethicone, dimethoxysilyl ethylenediaminopropyl dimethicone, hexyl methicone, hydroxypropyldimethicone, stearamidopropyl dimethicone, stearyl dimethicone, stearyl methicone, and vinyldimethicone. Int. J. Toxicol. 2003, 22 (Suppl. S2), 11–35. [Google Scholar]
- WHO/PAHO. Report of the WHO Informal Meeting on the Development of a Conceptual Framework for Tungiasis; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Ariza, L.; Wilcke, T.; Jackson, A.; Gomide, M.; Ugbomoiko, U.S.; Feldmeier, H.; Heukelbach, J. A simple method for rapid community assessment of tungiasis. Trop. Med. Int. Health 2010, 15, 856–864. [Google Scholar] [CrossRef]
- Althunian, T.A.; de Boer, A.; Groenwold, R.H.H.; Klungel, O.H. Defining the noninferiority margin and analysing noninferiority: An overview. Br. J. Clin. Pharmacol. 2017, 83, 1636–1642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Pre-authorisation Evaluation of Medicines for Human Use. Guideline on the choice of the non-inferioirity margin, 2005. Doc. Ref. EMEA/CPMP/EWP/2158/99. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-choice-non-inferiority-margin_en.pdf (accessed on 16 January 2023).
- Kaul, S.; Diamond, G.A. Good enough: A primer on the analysis and interpretation of noninferiority trials. Ann. Intern. Med. 2006, 145, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Feldmeier, H.; Eisele, M.; Heukelbach, J. Saboia Moura RC. Severe tungiasis in underprivileged communities: Case series from Brazil. Emerg. Infect. Dis. 2003, 9, 949–955. [Google Scholar] [CrossRef]
- Wangge, G.; Roes, K.C.; de Boer, A.; Hoes, A.W.; Knol, M.J. The challenges of determining noninferiority margins: A case study of noninferiority randomized controlled trials of novel oral anticoagulants. CMAJ 2013, 185, 222–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenfeld, D.A. Sample-size formula for the proportional-hazards regression model. Biometrics 1983, 39, 499–503. [Google Scholar] [CrossRef] [Green Version]
- Nordin, P.; Thielecke, M.; Ngomi, N.; Mudanga, G.M.; Krantz, I.; Feldmeier, H. Treatment of tungiasis with a two-component dimeticone: A comparison between moistening the whole foot and directly targeting the embedded sand fleas. Trop. Med. Heal. 2017, 45, 6. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, K.; Kamiya, Y.; Smith, C.; Kaneko, S.; Ongaya, A.; Amukoye, E. Protocol for a Randomized Control Trial for Tungiasis Treatment in Homa Bay County, Kenya: Dimeticone versus Sodium Carbonate. Methods Protoc. 2023, 6, 12. https://doi.org/10.3390/mps6010012
Suzuki K, Kamiya Y, Smith C, Kaneko S, Ongaya A, Amukoye E. Protocol for a Randomized Control Trial for Tungiasis Treatment in Homa Bay County, Kenya: Dimeticone versus Sodium Carbonate. Methods and Protocols. 2023; 6(1):12. https://doi.org/10.3390/mps6010012
Chicago/Turabian StyleSuzuki, Kana, Yasuhiko Kamiya, Chris Smith, Satoshi Kaneko, Asiko Ongaya, and Evans Amukoye. 2023. "Protocol for a Randomized Control Trial for Tungiasis Treatment in Homa Bay County, Kenya: Dimeticone versus Sodium Carbonate" Methods and Protocols 6, no. 1: 12. https://doi.org/10.3390/mps6010012