
Advances in Focused Ultrasound for the Treatment of Brain Tumors

 , , , , ,
, , , , , 
Abstract
:1. Introduction
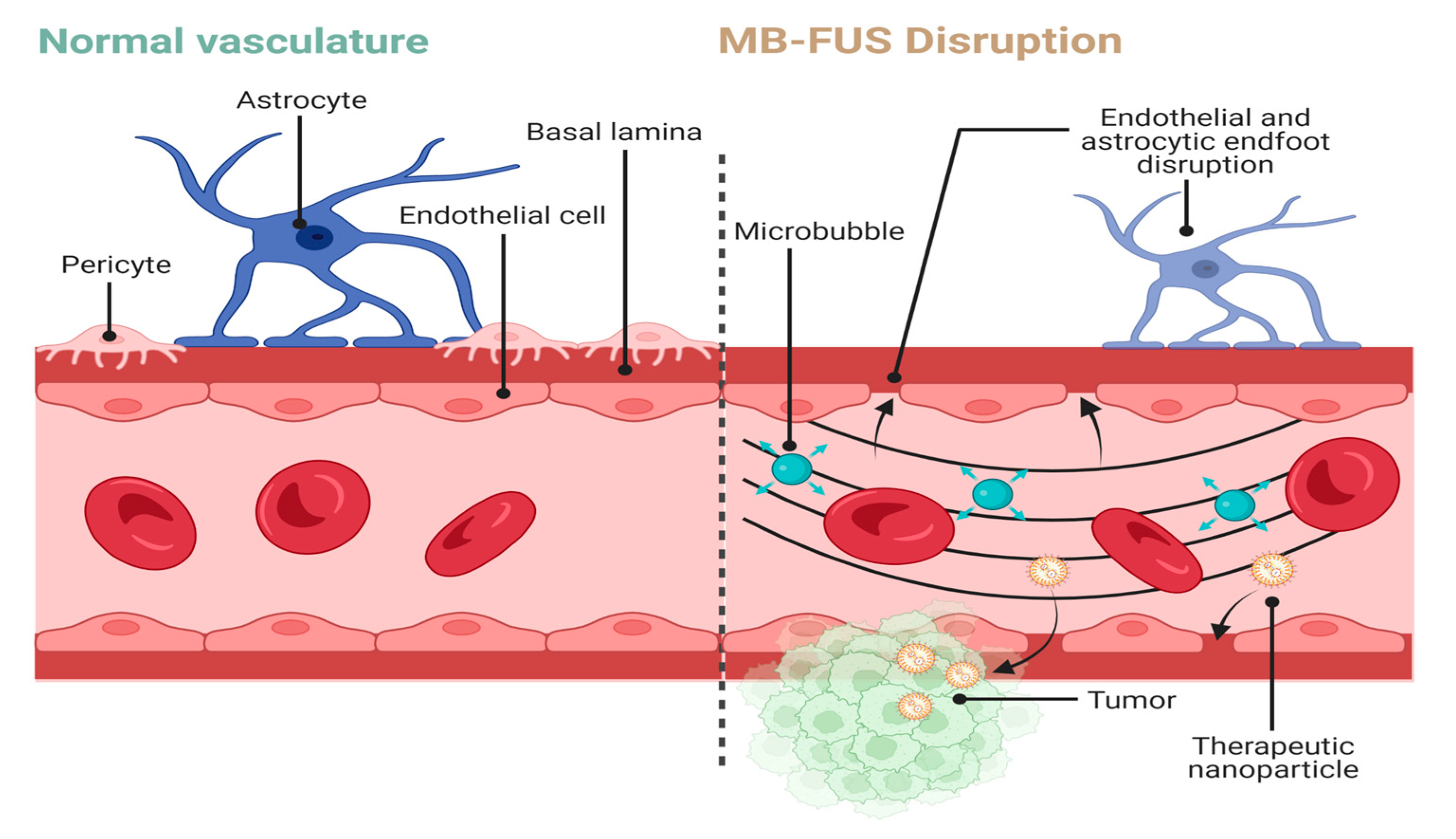
2. Mechanisms behind MB-FUS-Mediated BBB Disruption and Permeabilization
2.1. Microbubble Composition and Characteristics
2.2. Post Low-Intensity FUS Cellular and Biochemical Changes
3. MB-FUS as a Delivery Method (Preclinical)
3.1. Chemotherapy Delivery via MB-FUS
3.2. Immunotherapy Delivery via MB-FUS
3.3. RNA-Based Therapeutic Delivery via MB-FUS
4. MB-FUS as a Delivery Method (Clinical)
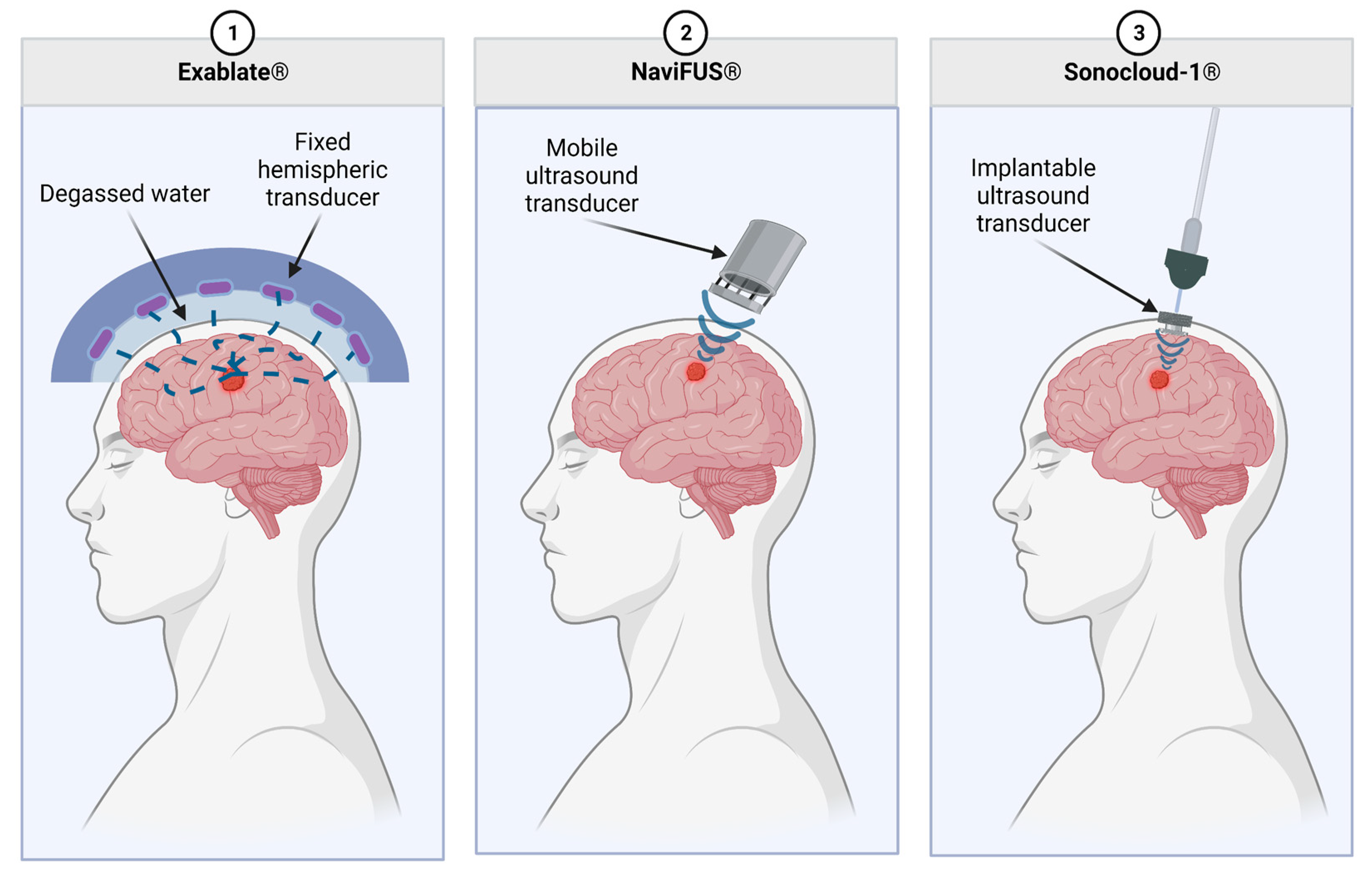
4.1. Focused Ultrasound Commercial Systems
4.2. Chemotherapy Delivery via MB-FUS
4.3. Immunotherapy Delivery via MB-FUS
4.4. Ongoing Trials
5. Safety of MB-FUS
5.1. Inflammation
5.2. Edema
6. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Troxclair, L.; Smetherman, D.; Bluth, E.I. Shades of Gray: A History of the Development of Diagnostic Ultrasound in a Large Multispecialty Clinic. Ochsner. J. 2011, 11, 151–155. [Google Scholar]
- Deffieux, T.; Demené, C.; Tanter, M. Functional Ultrasound Imaging: A New Imaging Modality for Neuroscience. Neuroscience 2021, 474, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Sastry, R.; Bi, W.L.; Pieper, S.; Frisken, S.; Kapur, T.; Wells, W.; Golby, A.J. Applications of Ultrasound in the Resection of Brain Tumors. J. Neuroimaging 2017, 27, 5–15. [Google Scholar] [CrossRef]
- Rabut, C.; Yoo, S.; Hurt, R.C.; Jin, Z.; Li, H.; Guo, H.; Ling, B.; Shapiro, M.G. Ultrasound Technologies for Imaging and Modulating Neural Activity. Neuron 2020, 108, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Iorio-Morin, C.; Yamamoto, K.; Sarica, C.; Zemmar, A.; Levesque, M.; Brisebois, S.; Germann, J.; Loh, A.; Boutet, A.; Elias, G.J.B.; et al. Bilateral Focused Ultrasound Thalamotomy for Essential Tremor (BEST-FUS Phase 2 Trial). Mov. Disord. 2021, 36, 2653–2662. [Google Scholar] [CrossRef] [PubMed]
- Moosa, S.; Martínez-Fernández, R.; Elias, W.J.; Del Alamo, M.; Eisenberg, H.M.; Fishman, P.S. The Role of High-Intensity Focused Ultrasound as a Symptomatic Treatment for Parkinson’s Disease. Mov. Disord. 2019, 34, 1243–1251. [Google Scholar] [CrossRef]
- Elias, W.J.; Lipsman, N.; Ondo, W.G.; Ghanouni, P.; Kim, Y.G.; Lee, W.; Schwartz, M.; Hynynen, K.; Lozano, A.M.; Shah, B.B.; et al. A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor. N. Engl. J. Med. 2016, 375, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Elias, W.J.; Huss, D.; Voss, T.; Loomba, J.; Khaled, M.; Zadicario, E.; Frysinger, R.C.; Sperling, S.A.; Wylie, S.; Monteith, S.J.; et al. A Pilot Study of Focused Ultrasound Thalamotomy for Essential Tremor. N. Engl. J. Med. 2013, 369, 640–648. [Google Scholar] [CrossRef]
- Halpern, C.H.; Santini, V.; Lipsman, N.; Lozano, A.M.; Schwartz, M.L.; Shah, B.B.; Elias, W.J.; Cosgrove, G.R.; Hayes, M.T.; McDannold, N.; et al. Three-Year Follow-up of Prospective Trial of Focused Ultrasound Thalamotomy for Essential Tremor. Neurology 2019, 93, e2284–e2293. [Google Scholar] [CrossRef]
- Pouratian, N.; Baltuch, G.; Elias, W.J.; Gross, R. American Society for Stereotactic and Functional Neurosurgery Position Statement on Magnetic Resonance-Guided Focused Ultrasound for the Management of Essential Tremor. Neurosurgery 2020, 87, E126–E129. [Google Scholar] [CrossRef]
- Sinai, A.; Nassar, M.; Sprecher, E.; Constantinescu, M.; Zaaroor, M.; Schlesinger, I. Focused Ultrasound Thalamotomy in Tremor Dominant Parkinson’s Disease: Long-Term Results. J. Park. Dis 2022, 12, 199–206. [Google Scholar] [CrossRef]
- Abusrair, A.H.; Elsekaily, W.; Bohlega, S. Tremor in Parkinson’s Disease: From Pathophysiology to Advanced Therapies. Tremor Other Hyperkinet. Mov. 2022, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Fernández, R.; Máñez-Miró, J.U.; Rodríguez-Rojas, R.; del Álamo, M.; Shah, B.B.; Hernández-Fernández, F.; Pineda-Pardo, J.A.; Monje, M.H.G.; Fernández-Rodríguez, B.; Sperling, S.A.; et al. Randomized Trial of Focused Ultrasound Subthalamotomy for Parkinson’s Disease. N. Engl. J. Med. 2020, 383, 2501–2513. [Google Scholar] [CrossRef] [PubMed]
- Bond, A.E.; Shah, B.B.; Huss, D.S.; Dallapiazza, R.F.; Warren, A.; Harrison, M.B.; Sperling, S.A.; Wang, X.-Q.; Gwinn, R.; Witt, J.; et al. Safety and Efficacy of Focused Ultrasound Thalamotomy for Patients With Medication-Refractory, Tremor-Dominant Parkinson Disease. JAMA Neurol. 2017, 74, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Konofagou, E.E.; Tung, Y.-S.; Choi, J.; Deffieux, T.; Baseri, B.; Vlachos, F. Ultrasound-Induced Blood-Brain Barrier Opening. Curr. Pharm. Biotechnol. 2012, 13, 1332–1345. [Google Scholar] [CrossRef]
- Meng, Y.; Hynynen, K.; Lipsman, N. Applications of Focused Ultrasound in the Brain: From Thermoablation to Drug Delivery. Nat. Rev. Neurol. 2021, 17, 7–22. [Google Scholar] [CrossRef]
- Meng, Y.; Pople, C.B.; Lea-Banks, H.; Abrahao, A.; Davidson, B.; Suppiah, S.; Vecchio, L.M.; Samuel, N.; Mahmud, F.; Hynynen, K.; et al. Safety and Efficacy of Focused Ultrasound Induced Blood-Brain Barrier Opening, an Integrative Review of Animal and Human Studies. J. Control. Release 2019, 309, 25–36. [Google Scholar] [CrossRef]
- Stride, E.; Segers, T.; Lajoinie, G.; Cherkaoui, S.; Bettinger, T.; Versluis, M.; Borden, M. Microbubble Agents: New Directions. Ultrasound Med. Biol. 2020, 46, 1326–1343. [Google Scholar] [CrossRef]
- Sprowls, S.A.; Arsiwala, T.A.; Bumgarner, J.R.; Shah, N.; Lateef, S.S.; Kielkowski, B.N.; Lockman, P.R. Improving CNS Delivery to Brain Metastases by Blood-Tumor Barrier Disruption. Trends Cancer 2019, 5, 495–505. [Google Scholar] [CrossRef]
- Stamatovic, S.M.; Johnson, A.M.; Keep, R.F.; Andjelkovic, A.V. Junctional Proteins of the Blood-Brain Barrier: New Insights into Function and Dysfunction. Tissue Barriers 2016, 4, e1154641. [Google Scholar] [CrossRef]
- Guyon, J.; Chapouly, C.; Andrique, L.; Bikfalvi, A.; Daubon, T. The Normal and Brain Tumor Vasculature: Morphological and Functional Characteristics and Therapeutic Targeting. Front. Physiol. 2021, 12, 622615. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi, Y.; Lo, V.P.; Lee, K. Critical Care Management of Cerebral Edema in Brain Tumors. J. Intensive Care Med. 2017, 32, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Harder, B.G.; Blomquist, M.R.; Wang, J.; Kim, A.J.; Woodworth, G.F.; Winkles, J.A.; Loftus, J.C.; Tran, N.L. Developments in Blood-Brain Barrier Penetrance and Drug Repurposing for Improved Treatment of Glioblastoma. Front. Oncol. 2018, 8, 462. [Google Scholar] [CrossRef] [PubMed]
- Bhowmik, A.; Khan, R.; Ghosh, M.K. Blood Brain Barrier: A Challenge for Effectual Therapy of Brain Tumors. BioMed Res. Int. 2015, 2015, 320941. [Google Scholar] [CrossRef]
- Mungur, R.; Zheng, J.; Wang, B.; Chen, X.; Zhan, R.; Tong, Y. Low-Intensity Focused Ultrasound Technique in Glioblastoma Multiforme Treatment. Front. Oncol. 2022, 12, 903059. [Google Scholar] [CrossRef]
- Mehkri, Y.; Woodford, S.; Pierre, K.; Dagra, A.; Hernandez, J.; Reza Hosseini Siyanaki, M.; Azab, M.; Lucke-Wold, B. Focused Delivery of Chemotherapy to Augment Surgical Management of Brain Tumors. Curr. Oncol. 2022, 29, 8846–8861. [Google Scholar] [CrossRef]
- Ranjan, T.; Sengupta, S.; Glantz, M.J.; Green, R.M.; Yu, A.; Aregawi, D.; Chaudhary, R.; Chen, R.; Zuccarello, M.; Lu-Emerson, C.; et al. Cancer Stem Cell Assay-Guided Chemotherapy Improves Survival of Patients with Recurrent Glioblastoma in a Randomized Trial. CR Med. 2023, 4, 101025. [Google Scholar] [CrossRef]
- Agarwala, S.S.; Kirkwood, J.M. Temozolomide, a Novel Alkylating Agent with Activity in the Central Nervous System, May Improve the Treatment of Advanced Metastatic Melanoma. Oncologist 2000, 5, 144–151. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Heldin, C.-H.; Rubin, K.; Pietras, K.; Östman, A. High Interstitial Fluid Pressure—An Obstacle in Cancer Therapy. Nat. Rev. Cancer 2004, 4, 806–813. [Google Scholar] [CrossRef]
- Jain, R.K. Barriers to Drug Delivery in Solid Tumors. Sci. Am. 1994, 271, 58–65. [Google Scholar] [CrossRef]
- Jin, Q.; Kang, S.-T.; Chang, Y.-C.; Zheng, H.; Yeh, C.-K. Inertial Cavitation Initiated by Polytetrafluoroethylene Nanoparticles under Pulsed Ultrasound Stimulation. Ultrason. Sonochem. 2016, 32, 1–7. [Google Scholar] [CrossRef]
- Treat, L.H.; McDannold, N.; Zhang, Y.; Vykhodtseva, N.; Hynynen, K. Improved Anti-Tumor Effect of Liposomal Doxorubicin after Targeted Blood-Brain Barrier Disruption by MRI-Guided Focused Ultrasound in Rat Glioma. Ultrasound. Med. Biol. 2012, 38, 1716–1725. [Google Scholar] [CrossRef]
- Bunevicius, A.; McDannold, N.J.; Golby, A.J. Focused Ultrasound Strategies for Brain Tumor Therapy. Oper. Neurosurg. 2020, 19, 9–18. [Google Scholar] [CrossRef]
- Hersh, A.M.; Bhimreddy, M.; Weber-Levine, C.; Jiang, K.; Alomari, S.; Theodore, N.; Manbachi, A.; Tyler, B.M. Applications of Focused Ultrasound for the Treatment of Glioblastoma: A New Frontier. Cancers 2022, 14, 4920. [Google Scholar] [CrossRef]
- Choi, J.J.; Feshitan, J.A.; Baseri, B.; Wang, S.; Tung, Y.-S.; Borden, M.A.; Konofagou, E.E. Microbubble-Size Dependence of Focused Ultrasound-Induced Blood-Brain Barrier Opening in Mice in Vivo. IEEE Trans. Biomed. Eng. 2010, 57, 145–154. [Google Scholar] [CrossRef]
- Wu, S.-K.; Chu, P.-C.; Chai, W.-Y.; Kang, S.-T.; Tsai, C.-H.; Fan, C.-H.; Yeh, C.-K.; Liu, H.-L. Characterization of Different Microbubbles in Assisting Focused Ultrasound-Induced Blood-Brain Barrier Opening. Sci. Rep. 2017, 7, 46689. [Google Scholar] [CrossRef]
- Burgess, A.; Hynynen, K. Drug Delivery across the Blood-Brain Barrier Using Focused Ultrasound. Expert. Opin. Drug Deliv. 2014, 11, 711–721. [Google Scholar] [CrossRef]
- Song, K.-H.; Harvey, B.K.; Borden, M.A. State-of-the-Art of Microbubble-Assisted Blood-Brain Barrier Disruption. Theranostics 2018, 8, 4393–4408. [Google Scholar] [CrossRef]
- Bader, K.B.; Holland, C.K. Gauging the Likelihood of Stable Cavitation from Ultrasound Contrast Agents. Phys. Med. Biol. 2013, 58, 127–144. [Google Scholar] [CrossRef]
- Hersh, D.S.; Wadajkar, A.S.; Roberts, N.; Perez, J.G.; Connolly, N.P.; Frenkel, V.; Winkles, J.A.; Woodworth, G.F.; Kim, A.J. Evolving Drug Delivery Strategies to Overcome the Blood Brain Barrier. Curr. Pharm. Des. 2016, 22, 1177–1193. [Google Scholar] [CrossRef]
- Marty, B.; Larrat, B.; Van Landeghem, M.; Robic, C.; Robert, P.; Port, M.; Le Bihan, D.; Pernot, M.; Tanter, M.; Lethimonnier, F.; et al. Dynamic Study of Blood-Brain Barrier Closure after Its Disruption Using Ultrasound: A Quantitative Analysis. J. Cereb. Blood Flow Metab. 2012, 32, 1948–1958. [Google Scholar] [CrossRef]
- Arsiwala, T.A.; Sprowls, S.A.; Blethen, K.E.; Fladeland, R.A.; Wolford, C.P.; Kielkowski, B.N.; Glass, M.J.; Wang, P.; Wilson, O.; Carpenter, J.S.; et al. Characterization of Passive Permeability after Low Intensity Focused Ultrasound Mediated Blood–Brain Barrier Disruption in a Preclinical Model. Fluids Barriers CNS 2022, 19, 72. [Google Scholar] [CrossRef] [PubMed]
- Kadry, H.; Noorani, B.; Cucullo, L. A Blood–Brain Barrier Overview on Structure, Function, Impairment, and Biomarkers of Integrity. Fluids Barriers CNS 2020, 17, 69. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, Z.I.; Kim, S.; Jikaria, N.; Qureshi, F.; Milo, B.; Lewis, B.K.; Bresler, M.; Burks, S.R.; Frank, J.A. Disrupting the Blood-Brain Barrier by Focused Ultrasound Induces Sterile Inflammation. Proc. Natl. Acad. Sci. USA 2017, 114, E75–E84. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Nazeri, A.; Baek, H.; Ye, D.; Yang, Y.; Yuan, J.; Rubin, J.B.; Chen, H. A Review of Bioeffects Induced by Focused Ultrasound Combined with Microbubbles on the Neurovascular Unit. J. Cereb. Blood Flow Metab. 2022, 42, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Englander, Z.K.; Wei, H.-J.; Pouliopoulos, A.N.; Bendau, E.; Upadhyayula, P.; Jan, C.-I.; Spinazzi, E.F.; Yoh, N.; Tazhibi, M.; McQuillan, N.M.; et al. Focused Ultrasound Mediated Blood–Brain Barrier Opening Is Safe and Feasible in a Murine Pontine Glioma Model. Sci. Rep. 2021, 11, 6521. [Google Scholar] [CrossRef]
- Ye, D.; Zhang, X.; Yue, Y.; Raliya, R.; Biswas, P.; Taylor, S.; Tai, Y.; Rubin, J.B.; Liu, Y.; Chen, H. Focused Ultrasound Combined with Microbubble-Mediated Intranasal Delivery of Gold Nanoclusters to the Brain. J. Control. Release 2018, 286, 145–153. [Google Scholar] [CrossRef]
- Burgess, A.; Hynynen, K. Noninvasive and Targeted Drug Delivery to the Brain Using Focused Ultrasound. ACS Chem. Neurosci. 2013, 4, 519–526. [Google Scholar] [CrossRef]
- Fan, C.-H.; Liu, H.-L.; Ting, C.-Y.; Lee, Y.-H.; Huang, C.-Y.; Ma, Y.-J.; Wei, K.-C.; Yen, T.-C.; Yeh, C.-K. Submicron-Bubble-Enhanced Focused Ultrasound for Blood–Brain Barrier Disruption and Improved CNS Drug Delivery. PLoS ONE 2014, 9, e96327. [Google Scholar] [CrossRef]
- Tung, Y.-S.; Marquet, F.; Teichert, T.; Ferrera, V.; Konofagou, E.E. Feasibility of Noninvasive Cavitation-Guided Blood-Brain Barrier Opening Using Focused Ultrasound and Microbubbles in Nonhuman Primates. Appl. Phys. Lett. 2011, 98, 163704. [Google Scholar] [CrossRef]
- McDannold, N.; Arvanitis, C.D.; Vykhodtseva, N.; Livingstone, M.S. Temporary Disruption of the Blood-Brain Barrier by Use of Ultrasound and Microbubbles: Safety and Efficacy Evaluation in Rhesus Macaques. Cancer Res. 2012, 72, 3652–3663. [Google Scholar] [CrossRef]
- Lapin, N.A.; Gill, K.; Shah, B.R.; Chopra, R. Consistent Opening of the Blood Brain Barrier Using Focused Ultrasound with Constant Intravenous Infusion of Microbubble Agent. Sci. Rep. 2020, 10, 16546. [Google Scholar] [CrossRef]
- Chien, C.-Y.; Xu, L.; Pacia, C.P.; Yue, Y.; Chen, H. Blood–Brain Barrier Opening in a Large Animal Model Using Closed-Loop Microbubble Cavitation-Based Feedback Control of Focused Ultrasound Sonication. Sci. Rep. 2022, 12, 16147. [Google Scholar] [CrossRef]
- Wei, H.-J.; Upadhyayula, P.S.; Pouliopoulos, A.N.; Englander, Z.K.; Zhang, X.; Jan, C.-I.; Guo, J.; Mela, A.; Zhang, Z.; Wang, T.J.C.; et al. Focused Ultrasound-Mediated Blood-Brain Barrier Opening Increases Delivery and Efficacy of Etoposide for Glioblastoma Treatment. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 539–550. [Google Scholar] [CrossRef]
- Timbie, K.F.; Afzal, U.; Date, A.; Zhang, C.; Song, J.; Wilson Miller, G.; Suk, J.S.; Hanes, J.; Price, R.J. MR Image-Guided Delivery of Cisplatin-Loaded Brain-Penetrating Nanoparticles to Invasive Glioma with Focused Ultrasound. J. Control. Release 2017, 263, 120–131. [Google Scholar] [CrossRef]
- Wei, K.-C.; Chu, P.-C.; Wang, H.-Y.J.; Huang, C.-Y.; Chen, P.-Y.; Tsai, H.-C.; Lu, Y.-J.; Lee, P.-Y.; Tseng, I.-C.; Feng, L.-Y.; et al. Focused Ultrasound-Induced Blood–Brain Barrier Opening to Enhance Temozolomide Delivery for Glioblastoma Treatment: A Preclinical Study. PLoS ONE 2013, 8, e58995. [Google Scholar] [CrossRef]
- Song, Z.; Huang, X.; Wang, J.; Cai, F.; Zhao, P.; Yan, F. Targeted Delivery of Liposomal Temozolomide Enhanced Anti-Glioblastoma Efficacy through Ultrasound-Mediated Blood–Brain Barrier Opening. Pharmaceutics 2021, 13, 1270. [Google Scholar] [CrossRef]
- McDannold, N.; Zhang, Y.; Supko, J.G.; Power, C.; Sun, T.; Vykhodtseva, N.; Golby, A.J.; Reardon, D.A. Blood-Brain Barrier Disruption and Delivery of Irinotecan in a Rat Model Using a Clinical Transcranial MRI-Guided Focused Ultrasound System. Sci. Rep. 2020, 10, 8766. [Google Scholar] [CrossRef]
- McDannold, N.; Zhang, Y.; Supko, J.G.; Power, C.; Sun, T.; Peng, C.; Vykhodtseva, N.; Golby, A.J.; Reardon, D.A. Acoustic Feedback Enables Safe and Reliable Carboplatin Delivery across the Blood-Brain Barrier with a Clinical Focused Ultrasound System and Improves Survival in a Rat Glioma Model. Theranostics 2019, 9, 6284–6299. [Google Scholar] [CrossRef]
- Lee, H.; Guo, Y.; Ross, J.L.; Schoen, S.; Degertekin, F.L.; Arvanitis, C. Spatially Targeted Brain Cancer Immunotherapy with Closed-Loop Controlled Focused Ultrasound and Immune Checkpoint Blockade. Sci. Adv. 2022, 8, eadd2288. [Google Scholar] [CrossRef]
- Sabbagh, A.; Beccaria, K.; Ling, X.; Marisetty, A.; Ott, M.; Caruso, H.; Barton, E.; Kong, L.-Y.; Fang, D.; Latha, K.; et al. Opening of the Blood-Brain Barrier Using Low-Intensity Pulsed Ultrasound Enhances Responses to Immunotherapy in Preclinical Glioma Models. Clin. Cancer Res. 2021, 27, 4325–4337. [Google Scholar] [CrossRef] [PubMed]
- Ye, D.; Yuan, J.; Yue, Y.; Rubin, J.B.; Chen, H. Focused Ultrasound-Enhanced Delivery of Intranasally Administered Anti-Programmed Cell Death-Ligand 1 Antibody to an Intracranial Murine Glioma Model. Pharmaceutics 2021, 13, 190. [Google Scholar] [CrossRef]
- Guo, Y.; Lee, H.; Fang, Z.; Velalopoulou, A.; Kim, J.; Thomas, M.B.; Kim, Y.; Coskun, A.F.; Pomeranz Krummel, D.; Sengupta, S.; et al. Single-Cell Analysis Reveals Effective SiRNA Delivery in Brain Tumors with Microbubble-Enhanced Ultrasound and Cationic Nanoparticles. Sci. Adv. 2021, 7, eabf7390. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Zhou, Y.; Chen, J.; Huang, N.; Wang, Z.; Cheng, Y. Gene Therapy for Drug-Resistant Glioblastoma via Lipid-Polymer Hybrid Nanoparticles Combined with Focused Ultrasound. Int. J. Nanomed. 2021, 16, 185–199. [Google Scholar] [CrossRef]
- Lipinski, C.A.; Lombardo, F.; Dominy, B.W.; Feeney, P.J. Experimental and Computational Approaches to Estimate Solubility and Permeability in Drug Discovery and Development Settings. Adv. Drug Deliv. Rev. 1997, 23, 3–25. [Google Scholar] [CrossRef]
- Mitusova, K.; Peltek, O.O.; Karpov, T.E.; Muslimov, A.R.; Zyuzin, M.V.; Timin, A.S. Overcoming the Blood–Brain Barrier for the Therapy of Malignant Brain Tumor: Current Status and Prospects of Drug Delivery Approaches. J. Nanobiotechnology 2022, 20, 412. [Google Scholar] [CrossRef]
- Montecucco, A.; Zanetta, F.; Biamonti, G. Molecular Mechanisms of Etoposide. EXCLI J. 2015, 14, 95–108. [Google Scholar]
- Pitz, M.W.; Desai, A.; Grossman, S.A.; Blakeley, J.O. Tissue Concentration of Systemically Administered Antineoplastic Agents in Human Brain Tumors. J. Neurooncol. 2011, 104, 629–638. [Google Scholar] [CrossRef]
- Rui, Y.; Green, J.J. Overcoming Delivery Barriers in Immunotherapy for Glioblastoma. Drug Deliv. Transl. Res. 2021, 11, 2302–2316. [Google Scholar] [CrossRef]
- Grossman, S.A.; Ye, X.; Lesser, G.; Sloan, A.; Carraway, H.; Desideri, S.; Piantadosi, S. Immunosuppression in Patients with High Grade Gliomas Treated with Radiation and Temozolomide. Clin. Cancer Res. 2011, 17, 5473–5480. [Google Scholar] [CrossRef]
- Quail, D.F.; Joyce, J.A. The Microenvironmental Landscape of Brain Tumors. Cancer Cell 2017, 31, 326–341. [Google Scholar] [CrossRef] [PubMed]
- Sampson, J.H.; Gunn, M.D.; Fecci, P.E.; Ashley, D.M. Brain Immunology and Immunotherapy in Brain Tumours. Nat. Rev. Cancer 2020, 20, 12–25. [Google Scholar] [CrossRef]
- Hao, C.; Chen, G.; Zhao, H.; Li, Y.; Chen, J.; Zhang, H.; Li, S.; Zhao, Y.; Chen, F.; Li, W.; et al. PD-L1 Expression in Glioblastoma, the Clinical and Prognostic Significance: A Systematic Literature Review and Meta-Analysis. Front. Oncol. 2020, 10, 1015. [Google Scholar] [CrossRef]
- Chen, R.Q.; Liu, F.; Qiu, X.Y.; Chen, X.Q. The Prognostic and Therapeutic Value of PD-L1 in Glioma. Front. Pharm. 2019, 9, 1503. [Google Scholar] [CrossRef]
- Liu, J.; Chen, Z.; Li, Y.; Zhao, W.; Wu, J.; Zhang, Z. PD-1/PD-L1 Checkpoint Inhibitors in Tumor Immunotherapy. Front. Pharmacol. 2021, 12, 731798. [Google Scholar] [CrossRef]
- Han, Y.; Liu, D.; Li, L. PD-1/PD-L1 Pathway: Current Researches in Cancer. Am. J. Cancer Res. 2020, 10, 727–742. [Google Scholar]
- Sheybani, N.D.; Witter, A.R.; Garrison, W.J.; Miller, G.W.; Price, R.J.; Bullock, T.N.J. Profiling of the Immune Landscape in Murine Glioblastoma Following Blood Brain/Tumor Barrier Disruption with MR Image-Guided Focused Ultrasound. J. Neurooncol. 2022, 156, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-T.; Lin, Y.-J.; Chai, W.-Y.; Lin, C.-J.; Chen, P.-Y.; Huang, C.-Y.; Kuo, J.S.; Liu, H.-L.; Wei, K.-C. Neuronavigation-Guided Focused Ultrasound (NaviFUS) for Transcranial Blood-Brain Barrier Opening in Recurrent Glioblastoma Patients: Clinical Trial Protocol. Ann. Transl. Med. 2020, 8, 673. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Nicosia, L.; Xu, Z.; Di Pietro, S.; Monfardini, L.; Bonomo, G.; Varano, G.M.; Prada, F.; Della Vigna, P.; Orsi, F. Focused Ultrasound: Tumour Ablation and Its Potential to Enhance Immunological Therapy to Cancer. Br. J. Radiol. 2018, 91, 20170641. [Google Scholar] [CrossRef]
- Wang, X.; Sun, J. High-Intensity Focused Ultrasound in Patients with Late-Stage Pancreatic Carcinoma. Chin. Med. J. (Engl.) 2002, 115, 1332–1335. [Google Scholar]
- Dowdy, S.F. Overcoming Cellular Barriers for RNA Therapeutics. Nat. Biotechnol. 2017, 35, 222–229. [Google Scholar] [CrossRef]
- Juliano, R.L. The Delivery of Therapeutic Oligonucleotides. Nucleic Acids Res. 2016, 44, 6518–6548. [Google Scholar] [CrossRef]
- Teng, X.-Q.; Qu, J.; Li, G.-H.; Zhuang, H.-H.; Qu, Q. Small Interfering RNA for Gliomas Treatment: Overcoming Hurdles in Delivery. Front. Cell Dev. Biol. 2022, 10, 824299. [Google Scholar] [CrossRef]
- Hannon, G.J. RNA Interference. Nature 2002, 418, 244–251. [Google Scholar] [CrossRef]
- Fire, A.; Xu, S.; Montgomery, M.K.; Kostas, S.A.; Driver, S.E.; Mello, C.C. Potent and Specific Genetic Interference by Double-Stranded RNA in Caenorhabditis Elegans. Nature 1998, 391, 806–811. [Google Scholar] [CrossRef]
- Daneman, R.; Prat, A. The Blood-Brain Barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef]
- Chen, K.-T.; Wei, K.-C.; Liu, H.-L. Theranostic Strategy of Focused Ultrasound Induced Blood-Brain Barrier Opening for CNS Disease Treatment. Front. Pharm. 2019, 10, 86. [Google Scholar] [CrossRef]
- Roberts, J.W.; Powlovich, L.; Sheybani, N.; LeBlang, S. Focused Ultrasound for the Treatment of Glioblastoma. J Neurooncol 2022, 157, 237–247. [Google Scholar] [CrossRef]
- Kyriakou, A.; Neufeld, E.; Werner, B.; Székely, G.; Kuster, N. Full-Wave Acoustic and Thermal Modeling of Transcranial Ultrasound Propagation and Investigation of Skull-Induced Aberration Correction Techniques: A Feasibility Study. J. Ther. Ultrasound. 2015, 3, 11. [Google Scholar] [CrossRef]
- Epelbaum, S.; Burgos, N.; Canney, M.; Matthews, D.; Houot, M.; Santin, M.D.; Desseaux, C.; Bouchoux, G.; Stroer, S.; Martin, C.; et al. Pilot Study of Repeated Blood-Brain Barrier Disruption in Patients with Mild Alzheimer’s Disease with an Implantable Ultrasound Device. Alzheimers Res. Ther. 2022, 14, 40. [Google Scholar] [CrossRef]
- Idbaih, A.; Canney, M.; Belin, L.; Desseaux, C.; Vignot, A.; Bouchoux, G.; Asquier, N.; Law-Ye, B.; Leclercq, D.; Bissery, A.; et al. Safety and Feasibility of Repeated and Transient Blood-Brain Barrier Disruption by Pulsed Ultrasound in Patients with Recurrent Glioblastoma. Clin. Cancer Res. 2019, 25, 3793–3801. [Google Scholar] [CrossRef]
- Assistance Publique—Hôpitaux de Paris. A Study to Evaluate the Safety of Transient Opening of the Blood-Brain Barrier by Low Intensity Pulsed Ultrasound with the SonoCloud Implantable Device in Patients with Recurrent Glioblastoma before Chemotherapy Administration. 2018. Available online: Clinicaltrials.gov (accessed on 18 March 2023).
- Brandes, A.A.; Basso, U.; Vastola, F.; Tosoni, A.; Pasetto, L.M.; Jirillo, A.; Lonardi, S.; Paris, M.K.; Koussis, H.; Monfardini, S.; et al. Carboplatin and Teniposide as Third-Line Chemotherapy in Patients with Recurrent Oligodendroglioma or Oligoastrocytoma: A Phase II Study. Ann. Oncol. 2003, 14, 1727–1731. [Google Scholar] [CrossRef]
- Yung, W.K.; Mechtler, L.; Gleason, M.J. Intravenous Carboplatin for Recurrent Malignant Glioma: A Phase II Study. J. Clin. Oncol. 1991, 9, 860–864. [Google Scholar] [CrossRef]
- Poisson, M.; Péréon, Y.; Chiras, J.; Delattre, J.Y. Treatment of Recurrent Malignant Supratentorial Gliomas with Carboplatin (CBDCA). J. Neurooncol. 1991, 10, 139–144. [Google Scholar] [CrossRef]
- Prados, M.D.; Warnick, R.E.; Mack, E.E.; Chandler, K.L.; Rabbitt, J.; Page, M.; Malec, M. Intravenous Carboplatin for Recurrent Gliomas. A Dose-Escalating Phase II Trial. Am. J. Clin. Oncol. 1996, 19, 609–612. [Google Scholar] [CrossRef]
- Lunardi, P.; Osman Farah, J.; Mastronardi, L.; Puzzilli, F.; Lo Bianco, F.M. Intravenous Administration of High Doses of Carboplatin in Multimodal Treatment of High Grade Gliomas: A Phase II Study. Acta Neurochir. 1996, 138, 215–220. [Google Scholar] [CrossRef]
- Murray, L.J.; Bridgewater, C.H.; Levy, D. Carboplatin Chemotherapy in Patients with Recurrent High-Grade Glioma. Clin. Oncol. (R Coll. Radiol.) 2011, 23, 55–61. [Google Scholar] [CrossRef]
- Roci, E.; Cakani, B.; Brace, G.; Bushati, T.; Rroji, A.; Petrela, M.; Kaloshi, G. Platinum-Based Chemotherapy in Recurrent High-Grade Glioma Patients: Retrospective Study. Med. Arch. 2014, 68, 140–143. [Google Scholar] [CrossRef]
- White, E.; Bienemann, A.; Pugh, J.; Castrique, E.; Wyatt, M.; Taylor, H.; Cox, A.; McLeod, C.; Gill, S. An Evaluation of the Safety and Feasibility of Convection-Enhanced Delivery of Carboplatin into the White Matter as a Potential Treatment for High-Grade Glioma. J. Neurooncol. 2012, 108, 77–88. [Google Scholar] [CrossRef]
- Sonabend, A.M.; Gould, A.; Amidei, C.; Ward, R.; Schmidt, K.A.; Zhang, D.Y.; Gomez, C.; Bebawy, J.F.; Liu, B.P.; Bouchoux, G.; et al. Repeated Blood-Brain Barrier Opening with an Implantable Ultrasound Device for Delivery of Albumin-Bound Paclitaxel in Patients with Recurrent Glioblastoma: A Phase 1 Trial. Lancet. Oncol. 2023, 24, 509–522. [Google Scholar] [CrossRef]
- Cloughesy, T.F.; Mochizuki, A.Y.; Orpilla, J.R.; Hugo, W.; Lee, A.H.; Davidson, T.B.; Wang, A.C.; Ellingson, B.M.; Rytlewski, J.A.; Sanders, C.M.; et al. Neoadjuvant Anti-PD-1 Immunotherapy Promotes a Survival Benefit with Intratumoral and Systemic Immune Responses in Recurrent Glioblastoma. Nat. Med. 2019, 25, 477–486. [Google Scholar] [CrossRef]
- InSightec. A Randomized Pivotal Study Assessing the Efficacy of Targeted Blood-Brain Barrier (BBB) Disruption Using Exablate Focused Ultrasound during the Standard of Care Treatment of Brain Metastases of Non-Small Cell Lung Cancer (NSCLC) Origin. 2022. Available online: Clinicaltrials.gov (accessed on 6 December 2022).
- Lozano, A.M. Safety and Feasibility of Focused Ultrasound-Enabled Liquid Biopsy in Patients with Brain Tumours. 2021. Available online: Clinicaltrials.gov (accessed on 9 April 2023).
- NaviFUS Corporation. An Open Label, Prospective, Pilot Study to Evaluate the Efficacy and Safety of Best Physician’s Choice of Standard of Care Combined with NaviFUS System in Patients with Recurrent Glioblastoma Multiforme. 2021. Available online: Clinicaltrials.gov (accessed on 24 May 2023).
- Assistance Publique—Hôpitaux de Paris. Multisite Open-Label Randomized Phase II Clinical Trial in Newly Diagnosed Glioblastoma Treated by Concurrent Temoradiation and Adjuvant Temozolomide +/- Ultrasound-Induced Blood Brain Barrier Opening. 2022. Available online: Clinicaltrials.gov (accessed on 28 March 2023).
- Lee, Y.; Choi, Y.; Park, E.-J.; Kwon, S.; Kim, H.; Lee, J.Y.; Lee, D.S. Improvement of Glymphatic–Lymphatic Drainage of Beta-Amyloid by Focused Ultrasound in Alzheimer’s Disease Model. Sci. Rep. 2020, 10, 16144. [Google Scholar] [CrossRef]
- Ji, R.; Karakatsani, M.E.; Burgess, M.; Smith, M.; Murillo, M.F.; Konofagou, E.E. Cavitation-Modulated Inflammatory Response Following Focused Ultrasound Blood-Brain Barrier Opening. J. Control. Release 2021, 337, 458–471. [Google Scholar] [CrossRef]
- Jones, R.M.; Kamps, S.; Huang, Y.; Scantlebury, N.; Lipsman, N.; Schwartz, M.L.; Hynynen, K. Accumulated Thermal Dose in MRI-Guided Focused Ultrasound for Essential Tremor: Repeated Sonications with Low Focal Temperatures. J. Neurosurg. 2019, 132, 1802–1809. [Google Scholar] [CrossRef]
- McMahon, D.; Bendayan, R.; Hynynen, K. Acute Effects of Focused Ultrasound-Induced Increases in Blood-Brain Barrier Permeability on Rat Microvascular Transcriptome. Sci. Rep. 2017, 7, 45657. [Google Scholar] [CrossRef]
- Choi, H.J.; Han, M.; Seo, H.; Park, C.Y.; Lee, E.-H.; Park, J. The New Insight into the Inflammatory Response Following Focused Ultrasound-Mediated Blood-Brain Barrier Disruption. Fluids Barriers CNS 2022, 19, 103. [Google Scholar] [CrossRef]
- Pascal, A.; Li, N.; Lechtenberg, K.J.; Rosenberg, J.; Airan, R.D.; James, M.L.; Bouley, D.M.; Pauly, K.B. Histologic Evaluation of Activation of Acute Inflammatory Response in a Mouse Model Following Ultrasound-Mediated Blood-Brain Barrier Using Different Acoustic Pressures and Microbubble Doses. Nanotheranostics 2020, 4, 210–223. [Google Scholar] [CrossRef]
- Pouliopoulos, A.N.; Kwon, N.; Jensen, G.; Meaney, A.; Niimi, Y.; Burgess, M.T.; Ji, R.; McLuckie, A.J.; Munoz, F.A.; Kamimura, H.A.S.; et al. Safety Evaluation of a Clinical Focused Ultrasound System for Neuronavigation Guided Blood-Brain Barrier Opening in Non-Human Primates. Sci. Rep. 2021, 11, 15043. [Google Scholar] [CrossRef]
- Sammartino, F.; Yeh, F.-C.; Krishna, V. Longitudinal Analysis of Structural Changes Following Unilateral Focused Ultrasound Thalamotomy. Neuroimage Clin. 2019, 22, 101754. [Google Scholar] [CrossRef]
- Shin, J.; Kong, C.; Cho, J.S.; Lee, J.; Koh, C.S.; Yoon, M.-S.; Na, Y.C.; Chang, W.S.; Chang, J.W. Focused Ultrasound-Mediated Noninvasive Blood-Brain Barrier Modulation: Preclinical Examination of Efficacy and Safety in Various Sonication Parameters. Neurosurg. Focus. 2018, 44, E15. [Google Scholar] [CrossRef]
- O’Reilly, M.A.; Jones, R.M.; Barrett, E.; Schwab, A.; Head, E.; Hynynen, K. Investigation of the Safety of Focused Ultrasound-Induced Blood-Brain Barrier Opening in a Natural Canine Model of Aging. Theranostics 2017, 7, 3573–3584. [Google Scholar] [CrossRef]
- Harary, M.; Essayed, W.I.; Valdes, P.A.; McDannold, N.; Cosgrove, G.R. Volumetric Analysis of Magnetic Resonance-Guided Focused Ultrasound Thalamotomy Lesions. Neurosurg. Focus 2018, 44, E6. [Google Scholar] [CrossRef]
- Wintermark, M.; Druzgal, J.; Huss, D.S.; Khaled, M.A.; Monteith, S.; Raghavan, P.; Huerta, T.; Schweickert, L.C.; Burkholder, B.; Loomba, J.J.; et al. Imaging Findings in MR Imaging-Guided Focused Ultrasound Treatment for Patients with Essential Tremor. AJNR Am. J. Neuroradiol. 2014, 35, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Lipsman, N.; Schwartz, M.L.; Krishna, V.; Sammartino, F.; Lozano, A.M.; Hynynen, K. Predicting Lesion Size by Accumulated Thermal Dose in MR-Guided Focused Ultrasound for Essential Tremor. Med. Phys. 2018, 45, 4704–4710. [Google Scholar] [CrossRef]
- Mórocz, I.A.; Hynynen, K.; Gudbjartsson, H.; Peled, S.; Colucci, V.; Jólesz, F.A. Brain Edema Development after MRI-Guided Focused Ultrasound Treatment. J. Magn. Reson. Imaging 1998, 8, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.P.; Prada, F.; Xu, Z.; Gatesman, J.; Feng, X.; Sporkin, H.; Gilbo, Y.; DeCleene, S.; Pauly, K.B.; Meyer, C.H. A Preclinical Study of Diffusion-Weighted MRI Contrast as an Early Indicator of Thermal Ablation. Magn. Reson. Med. 2021, 85, 2145–2159. [Google Scholar] [CrossRef]
- Deng, L.-D.; Qi, L.; Suo, Q.; Wu, S.-J.; Mamtilahun, M.; Shi, R.-B.; Liu, Z.; Sun, J.-F.; Tang, Y.-H.; Zhang, Z.-J.; et al. Transcranial Focused Ultrasound Stimulation Reduces Vasogenic Edema after Middle Cerebral Artery Occlusion in Mice. Neural. Regen. Res. 2022, 17, 2058–2063. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Post Low-Intensity FUS Changes | |
|---|---|
| Structural | Deformation of cellular membrane |
| Disruption of junctional complexes | |
| Potentiation of transcytosis Reduction in junctional complexes | |
| Cellular and Biochemical | Downregulation of P-glycoprotein |
| Altered BBB permeability regulatory phosphatidylinositol 3-kinase/Akt pathway Upregulation of cellular adhesion molecules |
| Therapy | Animal Model | Outcome | Reference |
|---|---|---|---|
| Etoposide | Mouse MGPP3 GBM | MB-FUS increased etoposide concentration in brain tumor tissue by eight-fold with subsequent 30% increase in MOS. | [55] |
| Cisplatin | Mouse F98 glioma | MB-FUS increased penetrance of nanoparticles loaded with cisplatin in a mouse model and improved survival compared to cisplatin nanoparticles without MB-FUS. | [56] |
| Temozolomide | Rat 9L gliosarcoma | MB-FUS delivery increases the CSF:plasma ratio of TMZ by 16% and marginally extends median survival. | [57,58] |
| Doxorubicin | Rat 9L gliosarcoma | 24% greater median survival time in rats treated with MB-FUS and doxorubicin compared to nontreated rats (p = 0.0007) | [33] |
| Irinotecan | Rat F98 glioma | FUS-delivered irinotecan did not improve overall survival but was safely delivered. This study did not use microbubbles to aid FUS. | [59] |
| Carboplatin | Rat F98 glioma | Tissue-to-plasma ratios of carboplatin was increased by 2.9 times after MB-FUS. | [60] |
| Anti-PD-1/Nivolumab | Mouse GL261 glioma | MB-FUS enhances the delivery of anti-PD-1 and improves overall survival. | [61] |
| Anti-PD-1/Nivolumab | Mouse GL261 glioma | MB-FUS increased survival in anti-PD-1 mice compared to control. Interestingly, FUS-mediated anti-PD-1 therapy was more effective when performed at a later timepoint when tumors were well-established. | [62] |
| Anti-PD-L1/Pembrolizumab | Mouse GL261 glioma | MB-FUS enhanced intranasal delivery of anti-PD-L1 without testing the treatment efficacy in GL261 mice. | [63] |
| SMO siRNA | Mouse SmoA1-Math1-GFP | MB-FUS delivery of SMO siRNA led to increased medulloblastoma apoptosis as measured by TUNEL staining. | [64] |
| CRISPR/CAS9 targeting MGMT | Mouse T98G NOD-SCID | Mouse model of GBM was treated with CRISPR/Cas9 targeting MGMT to resensitize tumor cells to TMZ. CRISPR/Cas9 delivered by MB-FUS led to increased TMZ sensitivity and improved overall survival compared to TMZ alone. | [65] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rao, R.; Patel, A.; Hanchate, K.; Robinson, E.; Edwards, A.; Shah, S.; Higgins, D.; Haworth, K.J.; Lucke-Wold, B.; Pomeranz Krummel, D.; et al. Advances in Focused Ultrasound for the Treatment of Brain Tumors. Tomography 2023, 9, 1094-1109. https://doi.org/10.3390/tomography9030090
Rao R, Patel A, Hanchate K, Robinson E, Edwards A, Shah S, Higgins D, Haworth KJ, Lucke-Wold B, Pomeranz Krummel D, et al. Advances in Focused Ultrasound for the Treatment of Brain Tumors. Tomography. 2023; 9(3):1094-1109. https://doi.org/10.3390/tomography9030090
Chicago/Turabian StyleRao, Rohan, Anjali Patel, Kunal Hanchate, Eric Robinson, Aniela Edwards, Sanjit Shah, Dominique Higgins, Kevin J. Haworth, Brandon Lucke-Wold, Daniel Pomeranz Krummel, and et al. 2023. "Advances in Focused Ultrasound for the Treatment of Brain Tumors" Tomography 9, no. 3: 1094-1109. https://doi.org/10.3390/tomography9030090