
Different Ultrasound Shear Wave Elastography Techniques as Novel Imaging-Based Approaches for Quantitative Evaluation of Hepatic Steatosis—Preliminary Findings
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. US Examinations
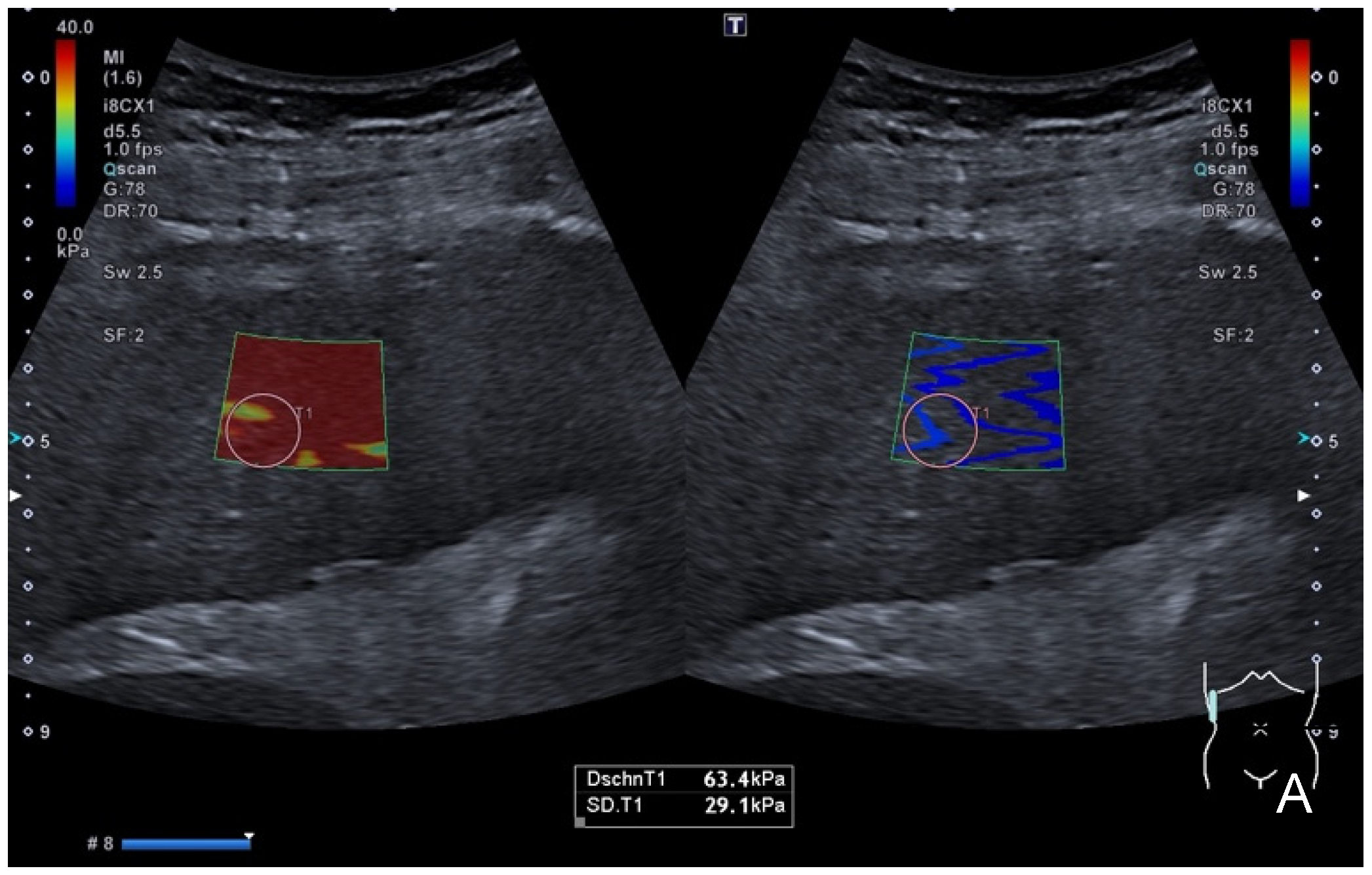
2.3. Shear-Wave Elastography
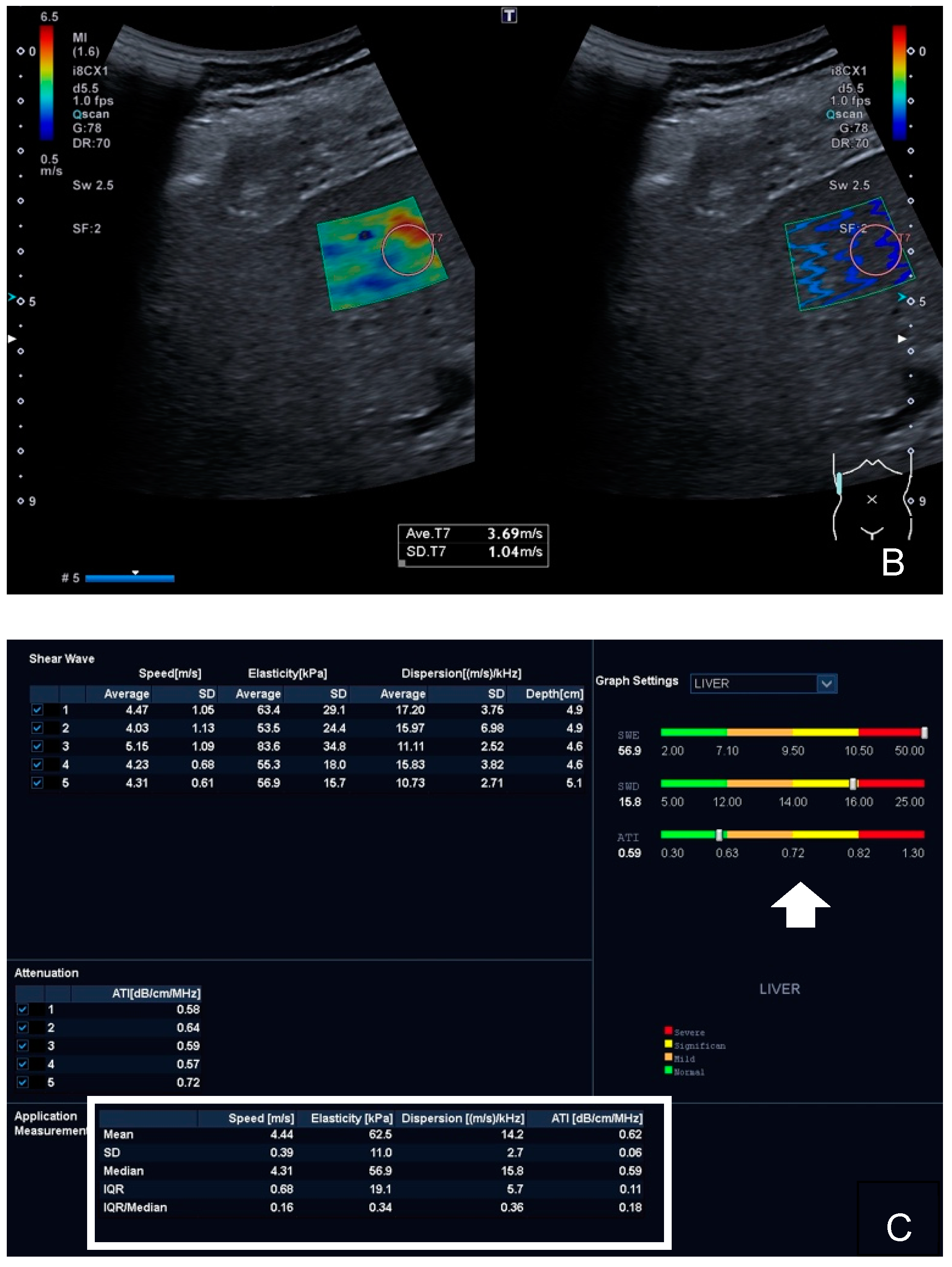
2.4. Shear-Wave Dispersion
2.5. Attenuation Imaging Technique
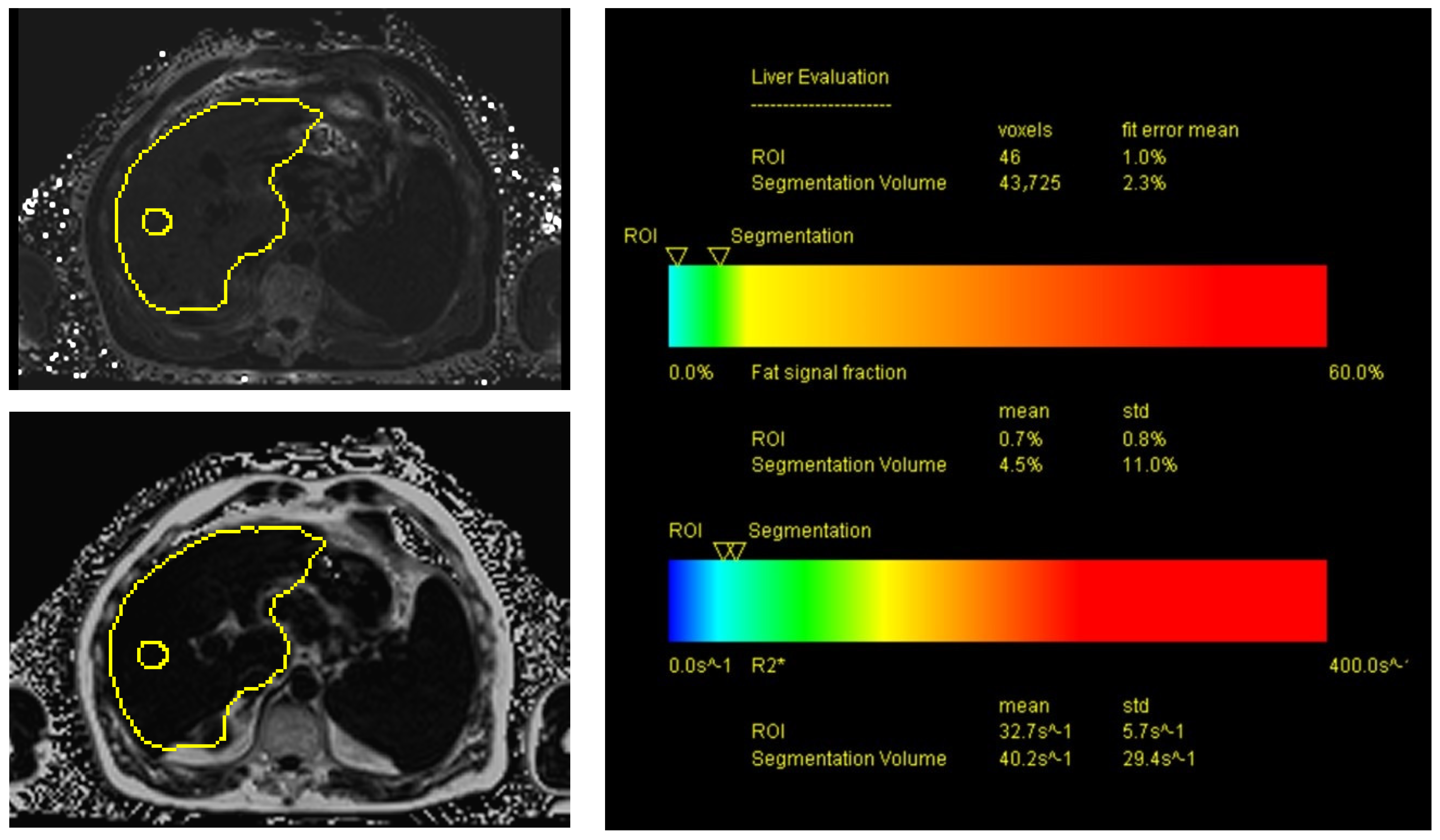
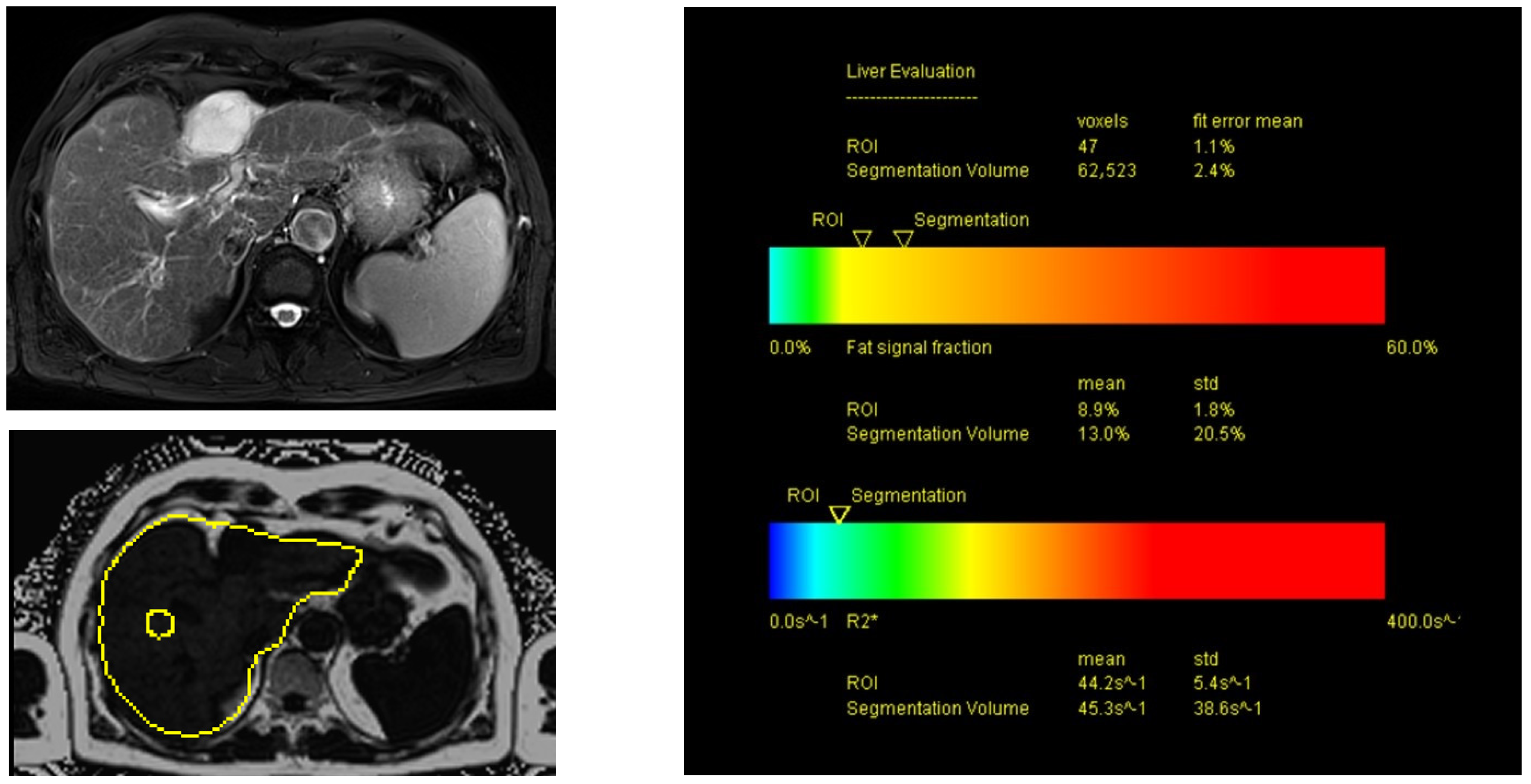
2.6. MRI of the Liver Using Proton Density Fat Fraction (PDFF) Sequences
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.M.; D’Onofrio, M.; Drakonaki, E.E.; et al. Efsumb guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: Basic principles and technology. Ultraschall Med. 2013, 34, 169–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosgrove, D.; Piscaglia, F.; Bamber, J.; Bojunga, J.; Correas, J.M.; Gilja, O.H.; Klauser, A.S.; Sporea, I.; Calliada, F.; Cantisani, V.; et al. Efsumb guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: Clinical applications. Ultraschall Med. 2013, 34, 238–253. [Google Scholar] [PubMed] [Green Version]
- Lupsor-Platon, M.; Serban, T.; Silion, A.I.; Tirpe, A.; Florea, M. Hepatocellular carcinoma and non-alcoholic fatty liver disease: A step forward for better evaluation using ultrasound elastography. Cancers 2020, 12, 2778. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, E.; de Ledinghen, V.; Cassinotto, C.; Chu, W.C.; Leung, V.Y.; Ferraioli, G.; Filice, C.; Castera, L.; Vilgrain, V.; Ronot, M.; et al. Assessment of biopsy-proven liver fibrosis by two-dimensional shear wave elastography: An individual patient data-based meta-analysis. Hepatology 2018, 67, 260–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, P.; Wagner, M.; Castera, L.; Hong, C.W.; Johnson, C.L.; Sirlin, C.B.; Taouli, B. Quantitative elastography methods in liver disease: Current evidence and future directions. Radiology 2018, 286, 738–763. [Google Scholar] [CrossRef] [PubMed]
- Osman, A.M.; El Shimy, A.; Abd El Aziz, M.M. 2D shear wave elastography (SWE) performance versus vibration-controlled transient elastography (VCTE/fibroscan) in the assessment of liver stiffness in chronic hepatitis. Insights Imaging 2020, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.N.; Fowler, K.J.; Ozturk, A.; Potu, C.K.; Louie, A.L.; Montes, V.; Henderson, W.C.; Wang, K.; Andre, M.P.; Samir, A.E.; et al. Liver fibrosis imaging: A clinical review of ultrasound and magnetic resonance elastography. J. Magn. Reson. Imaging 2020, 51, 25–42. [Google Scholar] [CrossRef]
- Ozturk, A.; Grajo, J.R.; Gee, M.S.; Benjamin, A.; Zubajlo, R.E.; Thomenius, K.E.; Anthony, B.W.; Samir, A.E.; Dhyani, M. Quantitative hepatic fat quantification in non-alcoholic fatty liver disease using ultrasound-based techniques: A review of literature and their diagnostic performance. Ultrasound Med. Biol. 2018, 44, 2461–2475. [Google Scholar] [CrossRef]
- Wei, H.; Song, B. Elastography for longitudinal assessment of liver fibrosis after antiviral therapy: A review. J. Clin. Transl. Hepatol. 2020, 8, 445–453. [Google Scholar] [CrossRef]
- Hu, X.; Qiu, L.; Liu, D.; Qian, L. Acoustic radiation force impulse (arfi) elastography for noninvasive evaluation of hepatic fibrosis in chronic hepatitis b and c patients: A systematic review and meta-analysis. Med. Ultrason. 2017, 19, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Ferraioli, G.; Soares Monteiro, L.B. Ultrasound-based techniques for the diagnosis of liver steatosis. World J. Gastroenterol. 2019, 25, 6053–6062. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi Burgio, M.; Ronot, M.; Reizine, E.; Rautou, P.E.; Castera, L.; Paradis, V.; Garteiser, P.; Van Beers, B.; Vilgrain, V. Quantification of hepatic steatosis with ultrasound: Promising role of attenuation imaging coefficient in a biopsy-proven cohort. Eur. Radiol. 2020, 30, 2293–2301. [Google Scholar] [CrossRef] [PubMed]
- Sporea, I.; Baldea, V.; Lupusoru, R.; Bende, F.; Mare, R.; Lazar, A.; Popescu, A.; Sirli, R. Quantification of steatosis and fibrosis using a new system implemented in an ultrasound machine. Med. Ultrason. 2020, 22, 265–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osaki, A.; Kubota, T.; Suda, T.; Igarashi, M.; Nagasaki, K.; Tsuchiya, A.; Yano, M.; Tamura, Y.; Takamura, M.; Kawai, H.; et al. Shear wave velocity is a useful marker for managing nonalcoholic steatohepatitis. World J. Gastroenterol. 2010, 16, 2918–2925. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Abe, M.; Yoshimasu, Y.; Kasai, Y.; Sakamaki, K.; Hara, T.; Itoi, T. The role of multiparametric us of the liver for the evaluation of nonalcoholic steatohepatitis. Radiology 2020, 296, 532–540. [Google Scholar] [CrossRef]
- Bae, J.S.; Lee, D.H.; Lee, J.Y.; Kim, H.; Yu, S.J.; Lee, J.H.; Cho, E.J.; Lee, Y.B.; Han, J.K.; Choi, B.I. Assessment of hepatic steatosis by using attenuation imaging: A quantitative, easy-to-perform ultrasound technique. Eur. Radiol. 2019, 29, 6499–6507. [Google Scholar] [CrossRef] [PubMed]
- Barry, C.T.; Mills, B.; Hah, Z.; Mooney, R.A.; Ryan, C.K.; Rubens, D.J.; Parker, K.J. Shear wave dispersion measures liver steatosis. Ultrasound Med. Biol. 2012, 38, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Yoshimasu, Y.; Kasai, Y.; Itoi, T. Clinical utilization of shear wave dispersion imaging in diffuse liver disease. Ultrasonography 2020, 39, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Ferraioli, G.; Maiocchi, L.; Raciti, M.V.; Tinelli, C.; De Silvestri, A.; Nichetti, M.; De Cata, P.; Rondanelli, M.; Chiovato, L.; Calliada, F.; et al. Detection of liver steatosis with a novel ultrasound-based technique: A pilot study using mri-derived proton density fat fraction as the gold standard. Clin. Transl. Gastroenterol. 2019, 10, e00081. [Google Scholar] [CrossRef]
- Hsu, P.K.; Wu, L.S.; Yen, H.H.; Huang, H.P.; Chen, Y.Y.; Su, P.Y.; Su, W.W. Attenuation imaging with ultrasound as a novel evaluation method for liver steatosis. J. Clin. Med. 2021, 10, 965. [Google Scholar] [CrossRef]
- Jeon, S.K.; Lee, J.M.; Joo, I.; Yoon, J.H.; Lee, D.H.; Lee, J.Y.; Han, J.K. Prospective evaluation of hepatic steatosis using ultrasound attenuation imaging in patients with chronic liver disease with magnetic resonance imaging proton density fat fraction as the reference standard. Ultrasound Med. Biol. 2019, 45, 1407–1416. [Google Scholar] [CrossRef]
- Ferraioli, G.; Maiocchi, L.; Savietto, G.; Tinelli, C.; Nichetti, M.; Rondanelli, M.; Calliada, F.; Preda, L.; Filice, C. Performance of the attenuation imaging technology in the detection of liver steatosis. J. Ultrasound Med. 2021, 40, 1325–1332. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Lee, J.Y.; Bae, J.S.; Yi, N.J.; Lee, K.W.; Suh, K.S.; Kim, H.; Lee, K.B.; Han, J.K. Shear-wave dispersion slope from us shear-wave elastography: Detection of allograft damage after liver transplantation. Radiology 2019, 293, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Caussy, C.; Alquiraish, M.H.; Nguyen, P.; Hernandez, C.; Cepin, S.; Fortney, L.E.; Ajmera, V.; Bettencourt, R.; Collier, S.; Hooker, J.; et al. Optimal threshold of controlled attenuation parameter with mri-pdff as the gold standard for the detection of hepatic steatosis. Hepatology 2018, 67, 1348–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Lee, R.; Trujillo, M. Reliability of performing multiparametric ultrasound in adult livers. J. Ultrasound Med. 2022, 41, 699–711. [Google Scholar] [CrossRef]
- Johnson, A.F. Statistics in medicine. T. Colton. Clin. Chem. 1975, 21, 789–790. [Google Scholar] [CrossRef]
- Lee, D.H.; Cho, E.J.; Bae, J.S.; Lee, J.Y.; Yu, S.J.; Kim, H.; Lee, K.B.; Han, J.K.; Choi, B.I. Accuracy of two-dimensional shear wave elastography and attenuation imaging for evaluation of patients with nonalcoholic steatohepatitis. Clin. Gastroenterol. Hepatol. 2021, 19, 797–805.e797. [Google Scholar] [CrossRef]
- Idilman, I.S.; Li, J.; Yin, M.; Venkatesh, S.K. Mr elastography of liver: Current status and future perspectives. Abdom. Radiol. 2020, 45, 3444–3462. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Lee, J.M.; Joo, I.; Lee, D.H.; Yoon, J.H.; Kang, H.J.; Ahn, S.J. Reproducibility of ultrasound attenuation imaging for the noninvasive evaluation of hepatic steatosis. Ultrasonography 2020, 39, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Tada, T.; Iijima, H.; Kobayashi, N.; Yoshida, M.; Nishimura, T.; Kumada, T.; Kondo, R.; Yano, H.; Kage, M.; Nakano, C.; et al. Usefulness of attenuation imaging with an ultrasound scanner for the evaluation of hepatic steatosis. Ultrasound Med. Biol. 2019, 45, 2679–2687. [Google Scholar] [CrossRef]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Yoshimasu, Y.; Kasai, Y.; Furuichi, Y.; Itoi, T. Viscoelasticity measurement in rat livers using shear-wave us elastography. Ultrasound Med. Biol. 2018, 44, 2018–2024. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Yu, D.; Li, G.; Wen, L.; Zhang, S. Comparison of the diagnostic performance of shear wave elastography with shear wave dispersion for pre-operative staging of hepatic fibrosis in patients with hepatocellular carcinoma. Eur. J. Radiol. 2022, 154, 110459. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.L.; Zhao, Q.Y.; Lin, C.S.; Hu, Z.X.; Zhang, T.; Gao, Z.L. Transient elastography and ultrasonography: Optimal evaluation of liver fibrosis and cirrhosis in patients with chronic hepatitis b concurrent with nonalcoholic fatty liver disease. Biomed. Res. Int. 2019, 2019, 3951574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirmoazen, A.M.; Khurana, A.; El Kaffas, A.; Kamaya, A. Quantitative ultrasound approaches for diagnosis and monitoring hepatic steatosis in nonalcoholic fatty liver disease. Theranostics 2020, 10, 4277–4289. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Gao, X.; Zhang, P.; Guo, Y.; Lin, H.; Diao, X.; Liu, Y.; Dong, C.; Hu, Y.; Chen, S.; et al. Dynamic mechanical analysis to assess viscoelasticity of liver tissue in a rat model of nonalcoholic fatty liver disease. Med. Eng. Phys. 2017, 44, 79–86. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
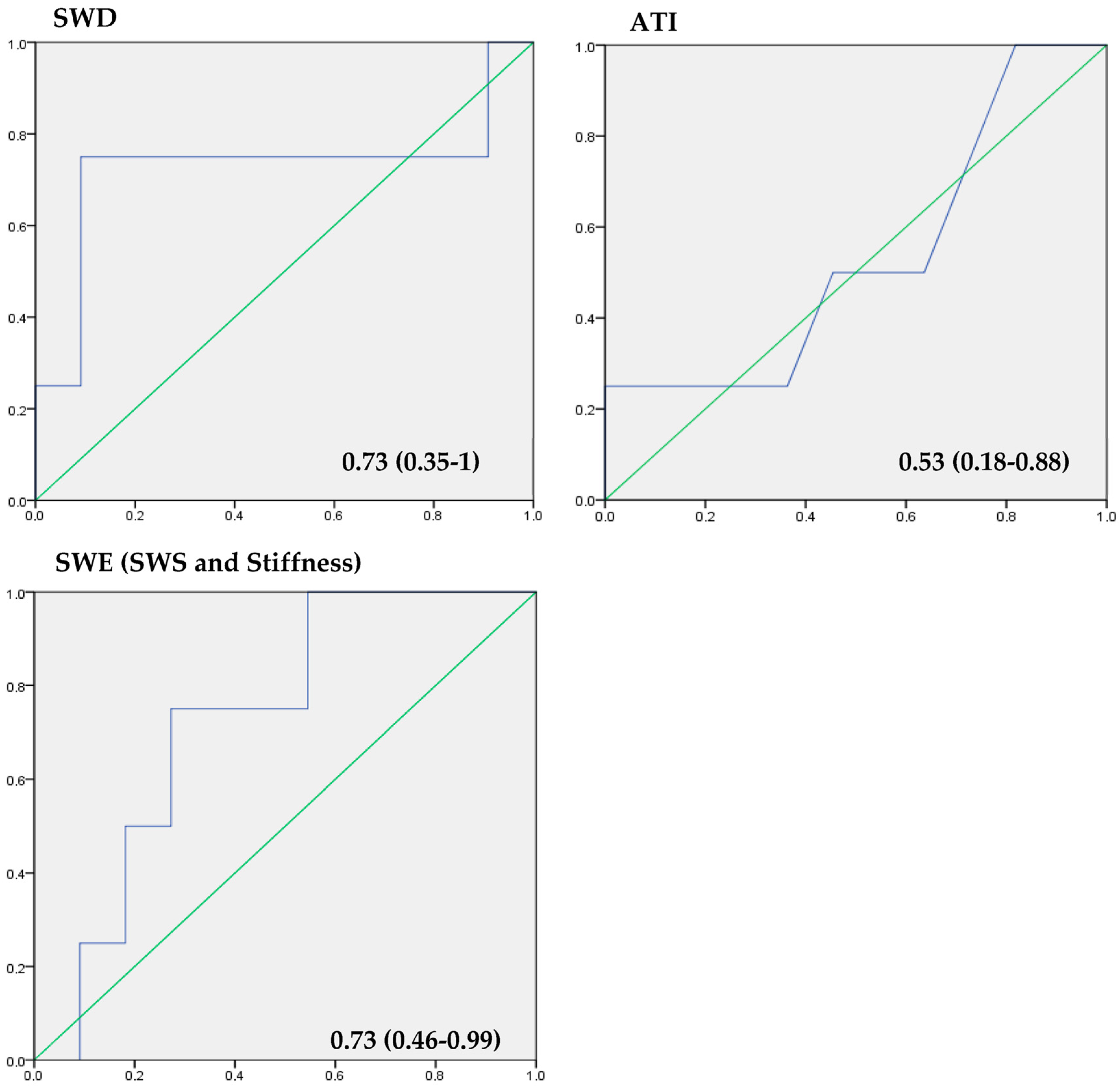
| Mean ± SD (Range) | AUC (95% CI) | Sensitivity | Specificity | r | p-Value | Cut-Off Value | |
|---|---|---|---|---|---|---|---|
| SWE (m/s) | 2.8 ± 0.76 (1.24–4.43) | 0.73 (0.46–0.99) | 75% | 72.7% | 0.27 | >0.05 | 2.5 |
| SWE (kPa) | 20.8 ± 16.8. (4.9–62.5) | 0.73 (0.46–0.99) | 75% | 72.7% | 0.27 | 0.001 * | 20.4 |
| SWD (m/s/kHz) | 16.5 ± 4.58 (10.5–23.1) | 0.73 (0.35–1) | 75% | 90.9% | 0.55 | 0.034 * | 18.5 |
| ATI (dB/cm/MHz) | 0.6 ± 0.12 (0.5–0.8) | 0.53 (0.18 –0.88) | 50% | 54.5% | 0.58 | 0.024 * | 0.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Platz Batista da Silva, N.; Scharf, G.; Lürken, L.; Verloh, N.; Schleder, S.; Stroszczynski, C.; Jung, E.M.; Haimerl, M. Different Ultrasound Shear Wave Elastography Techniques as Novel Imaging-Based Approaches for Quantitative Evaluation of Hepatic Steatosis—Preliminary Findings. Tomography 2023, 9, 681-692. https://doi.org/10.3390/tomography9020054
Platz Batista da Silva N, Scharf G, Lürken L, Verloh N, Schleder S, Stroszczynski C, Jung EM, Haimerl M. Different Ultrasound Shear Wave Elastography Techniques as Novel Imaging-Based Approaches for Quantitative Evaluation of Hepatic Steatosis—Preliminary Findings. Tomography. 2023; 9(2):681-692. https://doi.org/10.3390/tomography9020054
Chicago/Turabian StylePlatz Batista da Silva, Natascha, Gregor Scharf, Lukas Lürken, Niklas Verloh, Stephan Schleder, Christian Stroszczynski, Ernst Michael Jung, and Michael Haimerl. 2023. "Different Ultrasound Shear Wave Elastography Techniques as Novel Imaging-Based Approaches for Quantitative Evaluation of Hepatic Steatosis—Preliminary Findings" Tomography 9, no. 2: 681-692. https://doi.org/10.3390/tomography9020054