
Reduction in Radiation Exposure in Minimally Invasive Pedicle Screw Placement Using a Tubular Retractor: A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Operating Room Workflow
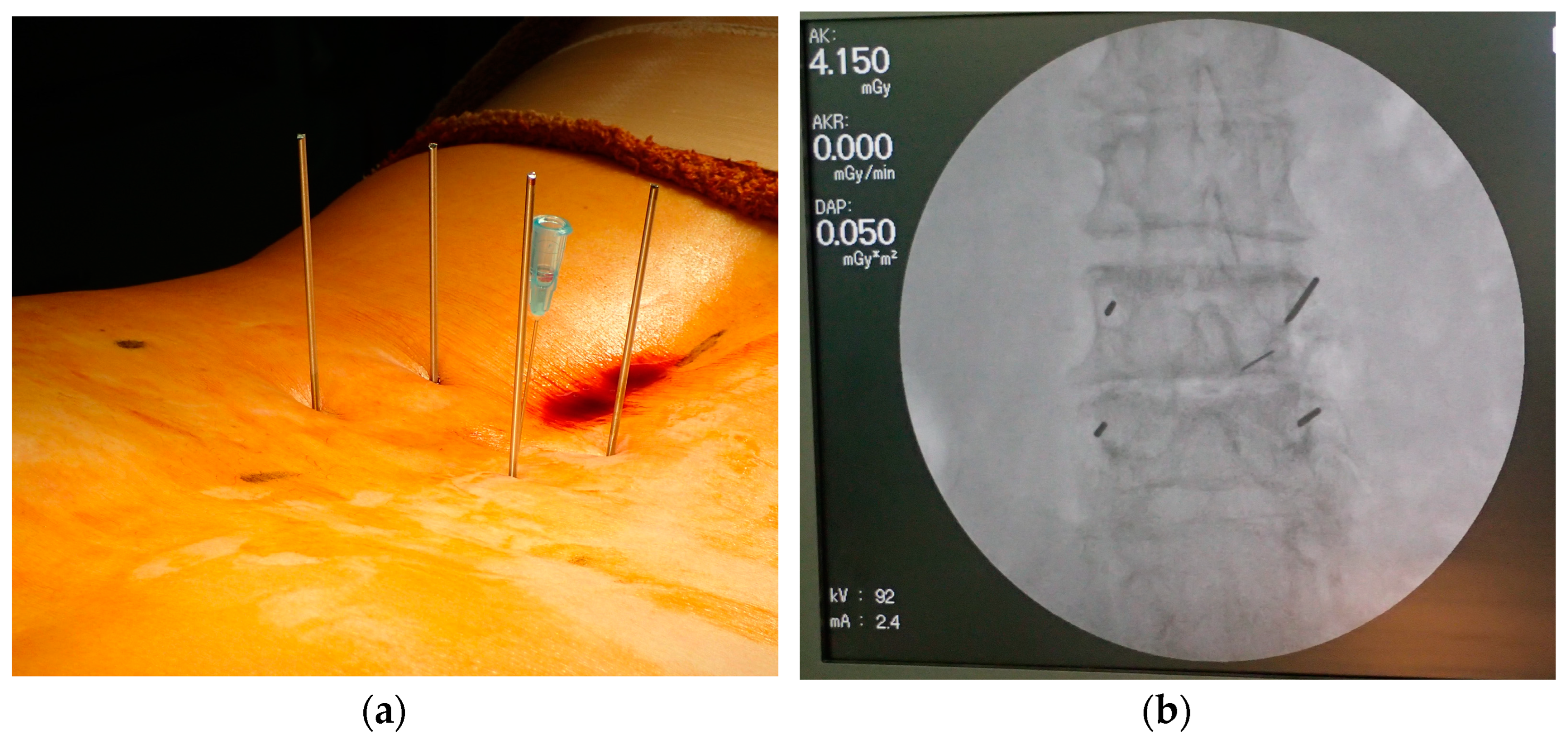
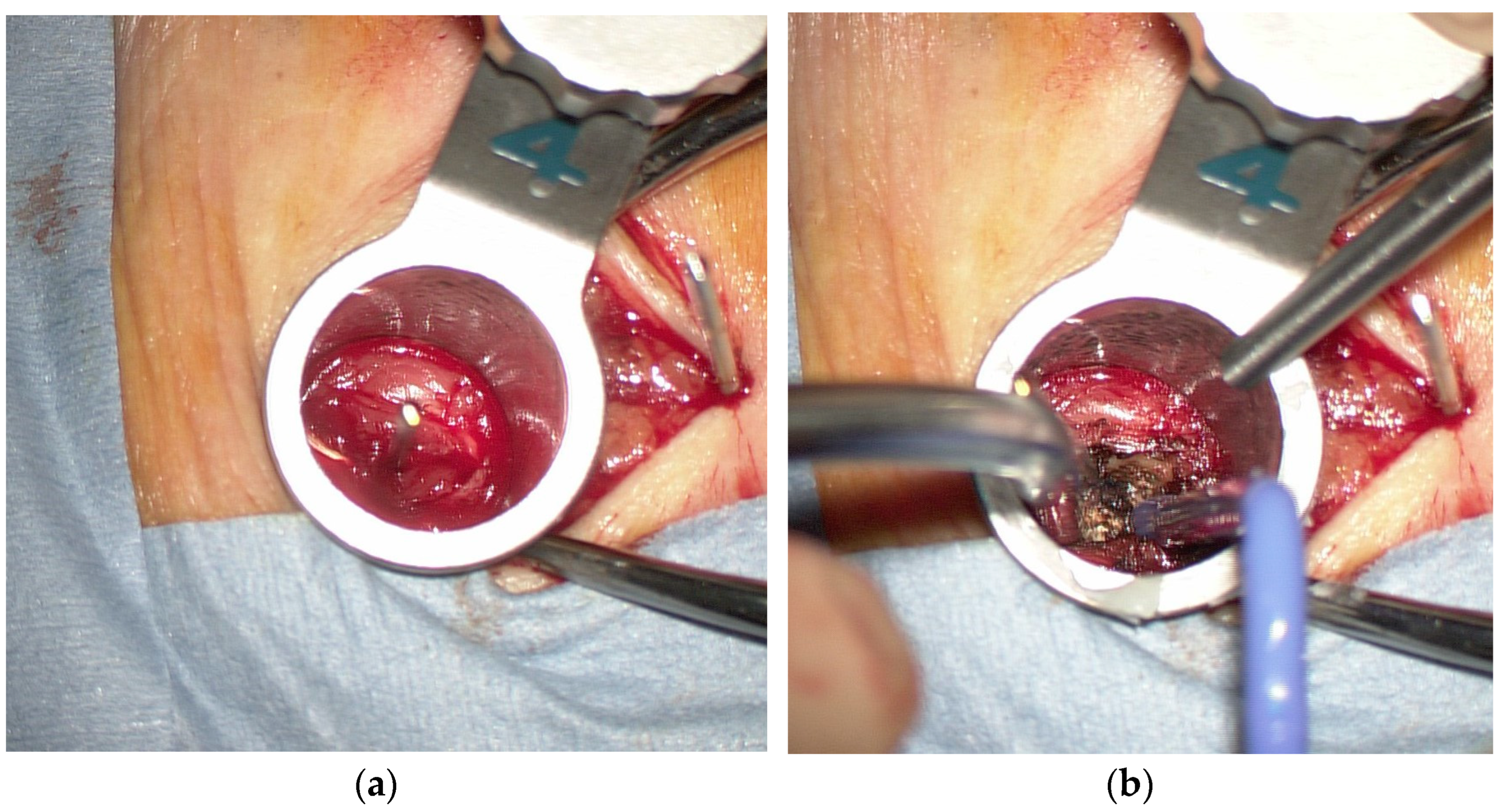
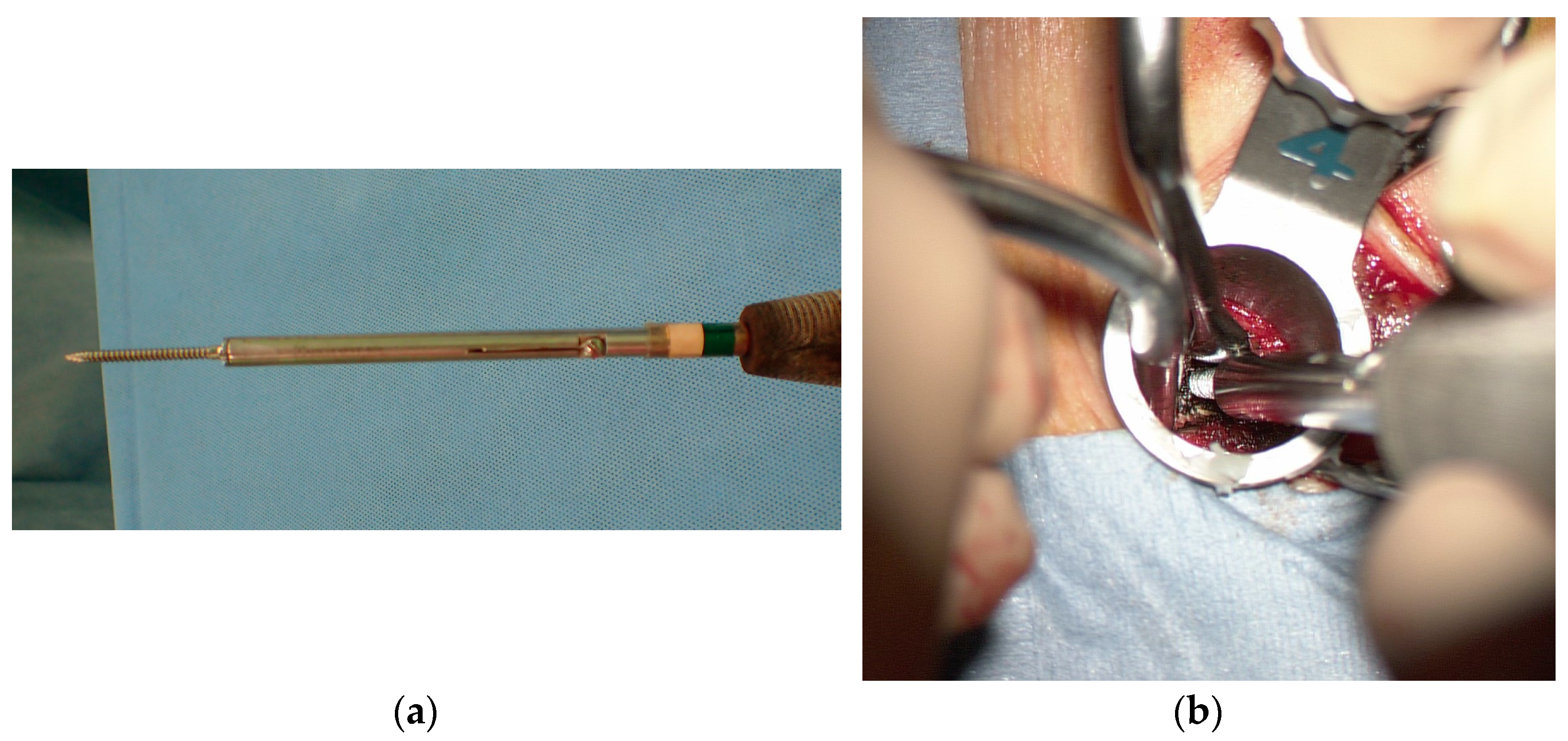
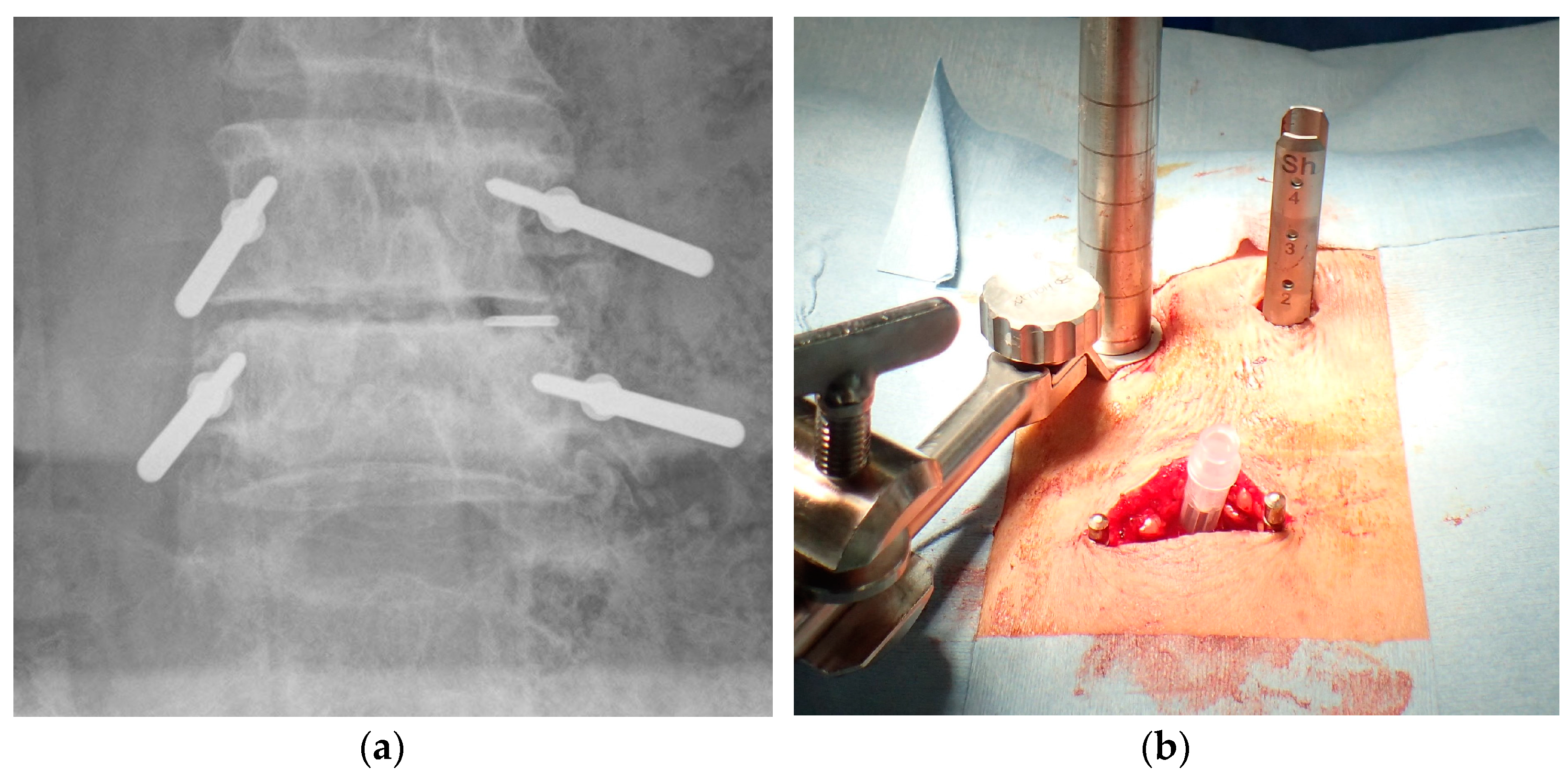
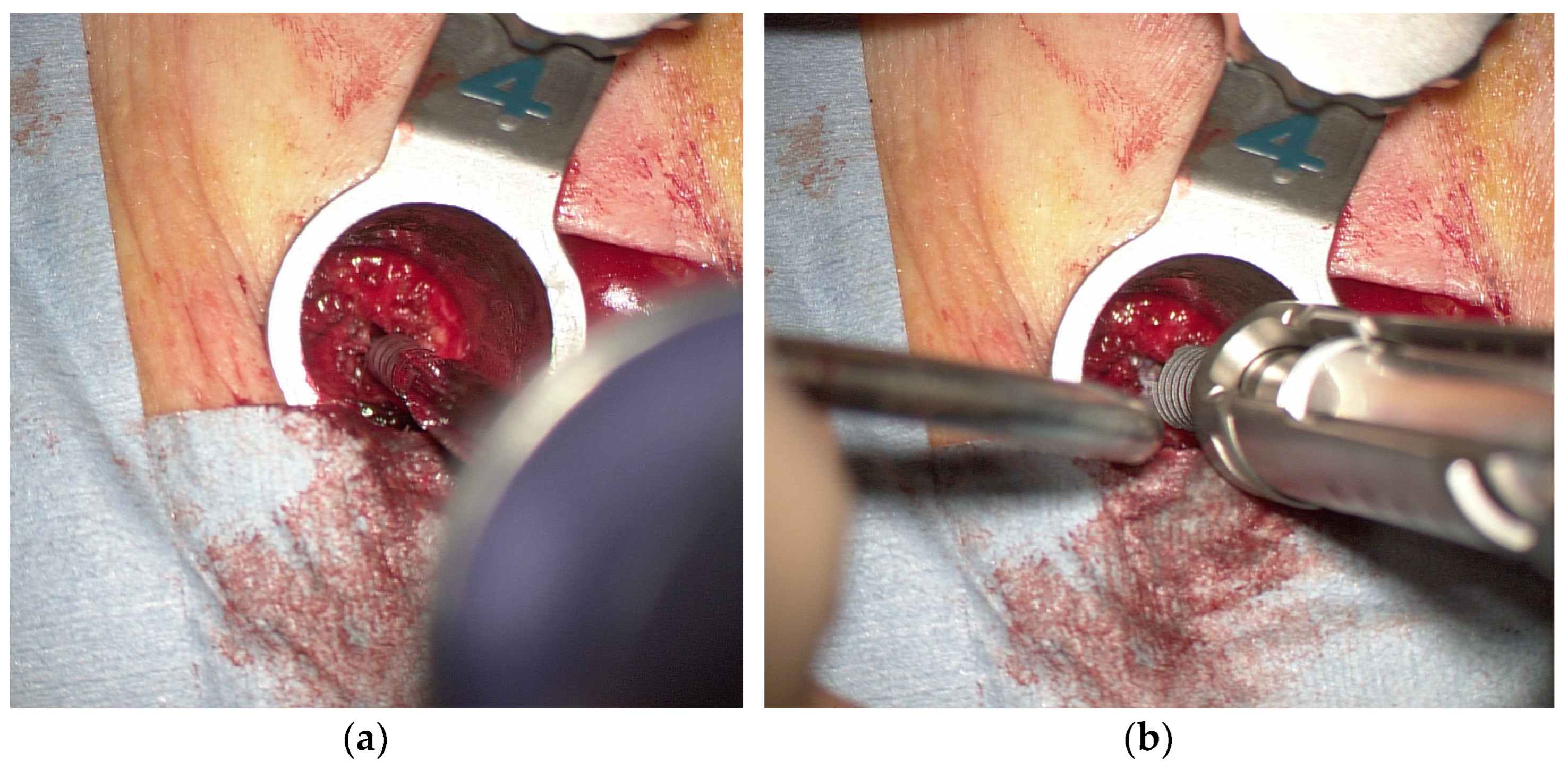
2.3. Surgical Technique
3. Results
3.1. Patient Characteristics
3.2. Radiation Time and Radiation Dose during Surgery
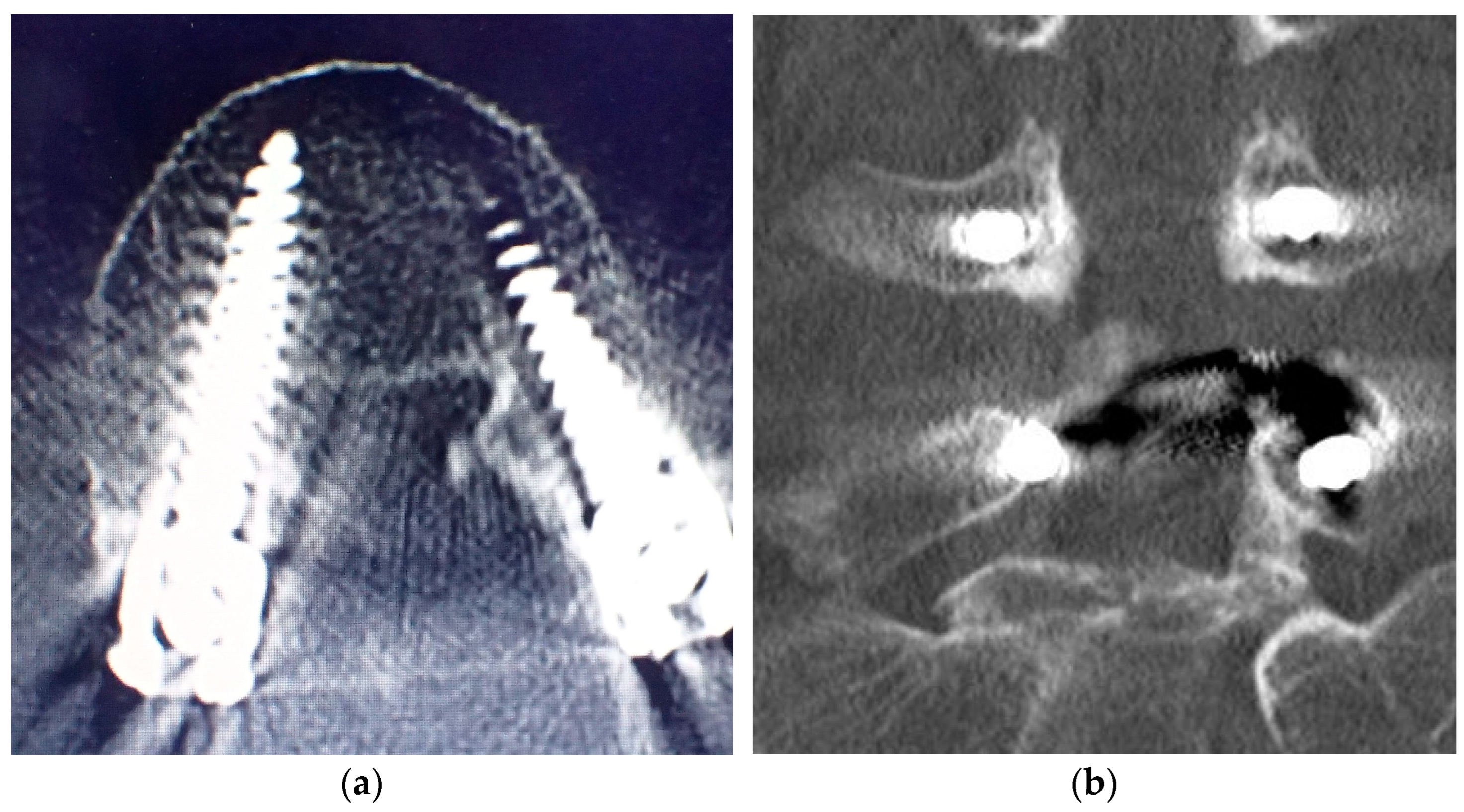
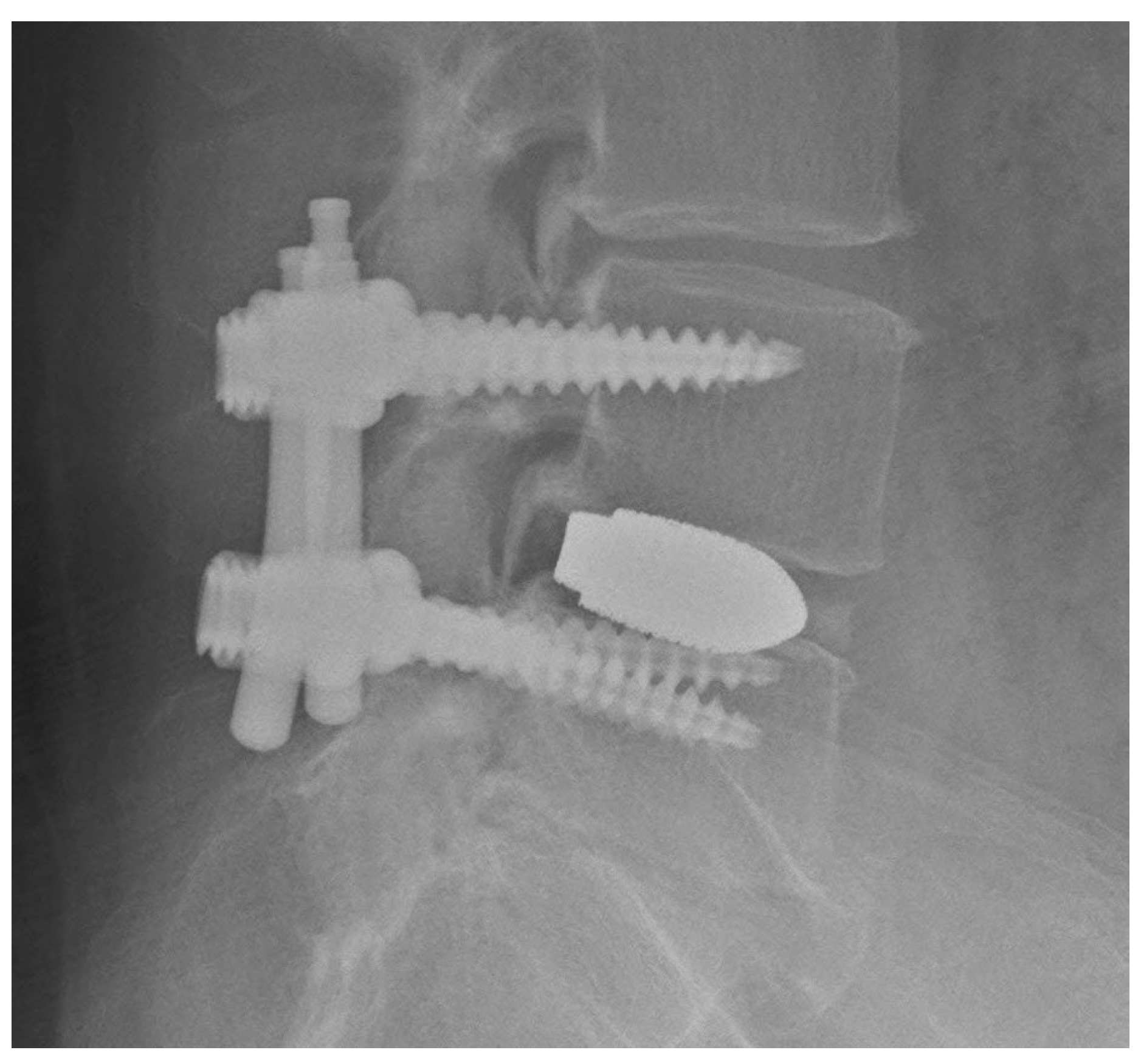
3.3. Pedicle Screw Insertion Accuracy
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mastrangelo, G.; Fedeli, U.; Fadda, E.; Giovanazzi, A.; Scoizzato, L.; Saia, B. Increased cancer risk among surgeons in an orthopaedic hospital. Occup. Med. 2005, 55, 498–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowda, S.R.; Mitchell, C.J.; Abouel-Enin, S.; Lewis, C. Radiation risk amongst orthopaedic surgeons—Do we know the risk? J. Perioper. Pract. 2019, 29, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Ryu, R.C.; Behrens, P.H.; Malik, A.T.; Lester, J.D.; Ahmad, C.S. Are we putting ourselves in danger? Occupational hazards and job safety for orthopaedic surgeons. J. Orthop. 2021, 24, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Bohl, D.D.; Hijji, F.Y.; Massel, D.H.; Mayo, B.C.; Long, W.W.; Modi, K.D.; Narain, A.S.; Manning, B.T.; Ahn, J.; Louie, P.K. Patient knowledge regarding radiation exposure from spinal imaging. Spine J. 2017, 17, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Lee, C.-H.; Kim, K.P. How High are Radiation-Related Risks in Minimally Invasive Transforaminal Lumbar Interbody Fusion Compared with Traditional Open Surgery? J. Spinal Disord. Tech. 2016, 29, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Mroz, T.E.; Abdullah, K.G.; Steinmetz, M.P.; Klineberg, E.O.; Lieberman, I.H. Radiation exposure to the surgeon during percutaneous pedicle screw placement. Clin. Spine Surg. 2011, 24, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Parent, E.; Wong, J.; Narvacan, K.; San, C.; Lou, E. Does image guidance decrease pedicle screw-related complications in surgical treatment of adolescent idiopathic scoliosis: A systematic review update and meta-analysis. Eur. Spine J. 2020, 29, 694–716. [Google Scholar] [CrossRef]
- Du, J.P.; Fan, Y.; Wu, Q.N.; Zhang, J.; Hao, D.J. Accuracy of Pedicle Screw Insertion among 3 Image-Guided Navigation Systems: Systematic Review and Meta-Analysis. World Neurosurg. 2018, 109, 24–30. [Google Scholar] [CrossRef]
- Fatima, N.; Massaad, E.; Hadzipasic, M.; Shankar, G.M.; Shin, J.H. Safety and accuracy of robot-assisted placement of pedicle screws compared to conventional free-hand technique: A systematic review and meta-analysis. Spine J. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Siccoli, A.; Klukowska, A.M.; Schröder, M.L.; Staartjes, V.E. A Systematic Review and Meta-Analysis of Perioperative Parameters in Robot-Guided, Navigated, and Freehand Thoracolumbar Pedicle Screw Instrumentation. World Neurosurg. 2019, 127, 576–587. [Google Scholar] [CrossRef]
- Staartjes, V.E.; Klukowska, A.M.; Schröder, M.L. Pedicle Screw Revision in Robot-Guided, Navigated, and Freehand Thoracolumbar Instrumentation: A Systematic Review and Meta-Analysis. World Neurosurg. 2018, 116, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, R.J.; Raley, D.A. Complications with K-wire insertion for percutaneous pedicle screws. Clin. Spine Surg. 2014, 27, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Fomekong, E.; Pierrard, J.; Danse, E.; Tombal, B.; Raftopoulos, C. An Unusual Case of Ureteral Perforation in Minimally Invasive Pedicle Screw Instrumentation: Case Report and Review of the Literature. World Neurosurg. 2018, 111, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Carmignani, A.; Lentini, S.; Acri, E.; Vazzana, G.; Campello, M.; Volpe, P.; Acri, I.E.; Spinelli, F. Combined thoracic endovascular aortic repair and neurosurgical intervention for injury due to posterior spine surgery. J. Card. Surg. 2013, 28, 163–167. [Google Scholar] [CrossRef]
- Tong, X.; Gu, P.; Yu, D.; Guo, F.; Lin, X. An endovascular treatment of a thoracic aortic injury caused by a misplaced pedicle screw: Case report and review of the literature. J. Formos. Med. Assoc. 2015, 114, 464–468. [Google Scholar] [CrossRef] [Green Version]
- Nayar, G.; Blizzard, D.J.; Wang, T.Y.; Cook, S.; Back, A.G.; Vincent, D.; Karikari, I.O. Pedicle screw placement accuracy using ultra-low radiation imaging with image enhancement versus conventional fluoroscopy in minimally invasive transforaminal lumbar interbody fusion: An internally randomized controlled trial. J. Neurosurg. Spine 2018, 28, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.Y.; Farber, S.H.; Perkins, S.S.; Back, A.G.; Byrd, S.A.; Chi, D.; Vincent, D.; Karikari, I.O. Internally Randomized Control Trial of Radiation Exposure Using Ultra-Low Radiation Imaging versus Traditional C-Arm Fluoroscopy for Patients Undergoing Single-Level Minimally Invasive Transforaminal Lumbar Interbody Fusion. Spine 2017, 42, 217–223. [Google Scholar] [CrossRef]
- Godzik, J.; Nayar, G.; Hunter, W.D.; Tumialán, L.M. Decreasing Radiation Emission in Minimally Invasive Spine Surgery Using Ultra-Low-Radiation Imaging with Image Enhancement: A Prospective Cohort Study. World Neurosurg. 2019, 122, e805–e811. [Google Scholar] [CrossRef]
- Clark, J.C.; Jasmer, G.; Marciano, F.F.; Tumialán, L.M. Minimally invasive transforaminal lumbar interbody fusions and fluoroscopy: A low-dose protocol to minimize ionizing radiation. Neurosurg. Focus 2013, 35, E8. [Google Scholar] [CrossRef] [Green Version]
- Tumialán, L.M.; Clark, J.C.; Snyder, L.A.; Jasmer, G.; Marciano, F.F. Prospective Evaluation of a Low-Dose Radiation Fluoroscopy Protocol for Minimally Invasive Transforaminal Lumbar Interbody Fusion. Oper. Neurosurg. 2015, 11, 537–544. [Google Scholar] [CrossRef]
- Yamashita, K.; Ikuma, H.; Tokashiki, T.; Maehara, T.; Nagamachi, A.; Takata, Y.; Sakai, T.; Higashino, K.; Sairyo, K. Radiation Exposure to the Hand of a Spinal Interventionalist during Fluoroscopically Guided Procedures. Asian Spine J. 2017, 11, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, K.; Higashino, K.; Wada, K.; Morimoto, M.; Abe, M.; Takata, Y.; Sakai, T.; Fukui, Y.; Sairyo, K. Radiation Exposure to the Surgeon and Patient during a Fluoroscopic Procedure: How High is the Exposure Dose? A Cadaveric Study. Spine 2016, 41, 1254–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bindal, R.K.; Glaze, S.; Ognoskie, M.; Tunner, V.; Malone, R.; Ghosh, S. Surgeon and patient radiation exposure in minimally invasive transforaminal lumbar interbody fusion. J. Neurosurg. Spine 2008, 9, 570–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funao, H.; Ishii, K.; Momoshima, S.; Iwanami, A.; Hosogane, N.; Watanabe, K.; Nakamura, M.; Toyama, Y.; Matsumoto, M. Surgeons’ exposure to radiation in single-and multi-level minimally invasive transforaminal lumbar interbody fusion; a prospective study. PLoS ONE 2014, 9, e95233. [Google Scholar] [CrossRef] [Green Version]
- Fujibayashi, S.; Murata, K.; Shimizu, T.; Otsuki, B.; Masamoto, K.; Shimizu, Y.; Matsuda, S. An Observational Survey of Nail and Skin of Spine Surgeons—Possible Damage by Occupational Ionizing Radiation Exposure. Spine Surg. Relat. Res. 2021, 5, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Giordano, B.D.; Grauer, J.N.; Miller, C.P.; Morgan, T.L.; Rechtine, G.R.I. Radiation Exposure Issues in Orthopaedics. J. Bone Joint Surg. Am. 2011, 93, e69. [Google Scholar] [CrossRef]
- Kisielewicz, K.; Truszkiewicz, A.; Wach, S.; Wasilewska–Radwańska, M. Evaluation of dose area product vs. patient dose in diagnostic X-ray units. Phys. Med. 2011, 27, 117–120. [Google Scholar] [CrossRef]
- Davoodi, R.; Eydian, M.-R.; Karampour, H.; Nassarpour, M.; Rezazadeh-Farokh, R.; Maraei, A.; Chavideh, M. Application of Dose Area Product (DAP) to Estimate Entrance Surface Dose (ESD) in Pediatric Chest X-rays. Mod. Health Sci. 2020, 3, p1. [Google Scholar] [CrossRef]
- Sakamoto, H.; Nakamura, O.; Yuge, M.; Sano, Y.; Akiyama, S.; Araki, T. A Study of Patient’s Dose Control Using an Area Exposure Product Meter. Jpn. J. Radiol. Technol. 2000, 56, 1256–1265. [Google Scholar] [CrossRef] [Green Version]
- ICRU. Patient Dosimetry for X rays Used in Medical Imaging. J. ICRU 2005, 5, 29. [Google Scholar]
- Gertzbein, S.D.; Robbins, S.E. Accuracy of Pedicular Screw Placement in Vivo. Spine 1990, 15, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Fayed, I.; Tai, A.; Triano, M.; Sayah, A.; Makariou, E.; Voyadzis, J.-M.; Sandhu, F.A. Robot-Assisted Percutaneous Pedicle Screw Placement: Evaluation of Accuracy of the First 100 Screws and Comparison with Cohort of Fluoroscopy-Guided Screws. World Neurosurg. 2020, 143, e492–e502. [Google Scholar] [CrossRef] [PubMed]
- O’Donohoe, T.J.; Dawes, B.H.; Thien, C.; Wang, Y.Y. Accuracy of K-Wireless Insertion of Percutaneous Pedicle Screws Using Computer-Assisted Spinal Navigation: A Systematic Review and Single-Center Experience. World Neurosurg. 2020, 138, e267–e274. [Google Scholar] [CrossRef] [PubMed]
- Ouchida, J.; Kanemura, T.; Satake, K.; Nakashima, H.; Segi, N.; Suzuki, K.; Imagama, S. True accuracy of percutaneous pedicle screw placement in thoracic and lumbar spinal fixation with a CT-based navigation system: Intraoperative and postoperative assessment of 763 percutaneous pedicle screws. J. Clin. Neurosci. 2020, 79, 1–6. [Google Scholar] [CrossRef]
- Tajsic, T.; Patel, K.; Farmer, R.; Mannion, R.J.; Trivedi, R.A. Spinal navigation for minimally invasive thoracic and lumbosacral spine fixation: Implications for radiation exposure, operative time, and accuracy of pedicle screw placement. Eur. Spine J. 2018, 27, 1918–1924. [Google Scholar] [CrossRef]
- Wu, Y.; Vázquez-Barquero, A. Stimulus-Evoked Electromyographic Monitoring during Minimally Invasive Transpedicular Implantation of Screws in Lumbosacral Spine: Threshold Value, Methodology and Clinical Effectiveness. World Neurosurg. 2017, 98, 146–151. [Google Scholar] [CrossRef]
- Mikula, A.L.; Williams, S.K.; Anderson, P.A. The use of intraoperative triggered electromyography to detect misplaced pedicle screws: A systematic review and meta-analysis. J. Neurosurg. Spine 2016, 24, 624–638. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Zhang, R.; Chen, B.; Deng, C.; Chen, X.; Shang, X.; Zhang, W. A novel tube technique enables visualization of the anatomy of the facet joints and accurate placement of the jamshidi needles with low radiation exposure. J. Clin. Neurosci. 2020, 76, 214–218. [Google Scholar] [CrossRef]
- Qi, X.; Vives, M.; Hacihaliloglu, I. Ultrasound Guided Pedicle Screw Entry Point Identification for Spinal Fusion Surgery. CAOS 2019, 3, 306–310. [Google Scholar]
- Qi, X.; Vora, N.; Riera, L.; Sarangi, A.; Youssef, G.; Vives, M.; Hacihaliloglu, I. Automatic Scan Plane Identification from 2D Ultrasound for Pedicle Screw Guidance. CAOS 2018, 2, 168–174. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value (%) |
|---|---|
| Number of patients | 24 |
| Mean patient age in years (range) | 64.8 (24–88) |
| Men (%) | 9 (37.5) |
| Women (%) | 15 (62.5) |
| Body Mass Index (kg/m2) (range) | 25.5 (17.3–32.9) |
| Primary diagnosis | |
| Spondylolisthesis | 13 (51) |
| Degenerative disc disease | 5 (22) |
| Disc herniation | 6 (25) |
| Lumbar level | |
| L1/2 | 1 |
| L3/4 | 5 |
| L4/5 | 14 |
| L5/S1 | 4 |
| Factor | Mean Value (Range) |
|---|---|
| Operating time (minutes) | 201.8 (145–246) |
| Fluoroscopic time/case (seconds) | 26.8 (8–56) |
| Radiation dose of DAP (mGy∗m2) | 0.0706 (0.018–0.133) |
| Radiation dose of AK (mGy) | 6.0 (1.071–21.74) |
| Radiation dose of ESD (mGy) | 11.31 (2.199–44.64) |
| Extra time required for this procedure (minutes) | 39 (16–69) |
| Age | <65 Years Old (n = 12) | ≥65 Years Old (n = 12) | |||
|---|---|---|---|---|---|
| Fluoroscopic time (seconds) | 26.5 (8–56) | 24.5 (15–49) | p = 0.582 | ||
| Radiation dose of DAP (mGy∗m2) | 0.061 (0.018–0.128) | 0.058 (0.034–0.26) | p = 0.931 | ||
| Radiation dose of ESD (mGy) | 9.884 (3.002–21.928) | 9.823 (2.199–44.637) | p = 0.908 | ||
| Extra time required for this procedure (minutes) | 40 (27–71) | 33 (16–64) | p = 0.111 | ||
| Gender | Men (n = 9) | Women (n = 15) | |||
| Fluoroscopic time (seconds) | 24 (8–49) | 27 (15–56) | p = 0.881 | ||
| Radiation dose of DAP (mGy∗m2) | 0.057 (0.018–0.102) | 0.061 (0.032–0.26) | p = 0.811 | ||
| Radiation dose of ESD (mGy) | 9.747 (3.002–19.341) | 0.447 (2.199–44.637) | p = 0.743 | ||
| Extra time required for this procedure (minutes) | 33 (27–48) | 39 (16–71) | p = 0.367 | ||
| BMI | <25 kg/m2 (n = 12) | ≥25 kg/m2 (n = 12) | |||
| Fluoroscopic time (seconds) | 24 (15–49) | 26 (8–56) | p = 0.862 | ||
| Radiation dose of DAP (mGy∗m2) | 0.0495 (0.032–0.102) | 0.066 (0.018–0.26) | p = 0.119 | ||
| Radiation dose of ESD (mGy) | 9.232 (5.433–19.341) | 10.59 (2.199–44.637) | p = 0.299 | ||
| Extra time required for this procedure (minutes) | 37 (16–69) | 33 (18–71) | p = 0.977 | ||
| Primary diagnosis | Spondylolisthesis (n = 13) | Degenerative disc disease (n = 5) | Disc herniation (n = 6) | ||
| Fluoroscopic time (seconds) | 25 (15–56) | 28 (15–38) | 24.5 (8–49) | p = 0.798 | |
| Radiation dose of DAP (mGy∗m2) | 0.058 (0.032–0.26) | 0.063 (0.034–0.088) | 0.0535 (0.018–0.102) | p = 0.907 | |
| Radiation dose of ESD (mGy) | 9.878 (2.199–44.637) | 10.734 (5.819–14.999) | 8.951 (3.002–19.341) | p = 0.655 | |
| Extra time required for this procedure (minutes) | 33 (16–71) | 39 (30–64) | 31.5 (27–47) | p = 0.444 | |
| Lumbar Level | L1/2 (n = 1) | L3/4 (n = 5) | L4/5 (n = 14) | L5S1 (n = 4) | |
| Fluoroscopic time (seconds) | 24 | 27 (15–49) | 26 (15–56) | 24.5 (8–28) | p = 0.896 |
| Radiation dose of DAP (mGy∗m2) | 0.044 | 0.061 (0.034–0.102) | 0.0635 (0.032–0.26) | 0.058 (0.018–0.063) | p = 0.662 |
| Radiation dose of ESD (mGy) | 7.593 | 10.447 (5.819–19.341) | 9.812 (2.199–44.637) | 9.894 (3.002–10.734) | p = 0.834 |
| Extra time required for this procedure (minutes) | 47 | 30 (9–64) | 34.5 (16–71) | 39.5 (30–63) | p = 0.714 |
| Vertebral Level | Screws Per Vertebral Level | Number of Breaches | Direction of Breach (n) | Grade of Breach (n) | Breach Rate (%) |
|---|---|---|---|---|---|
| L-1 | 2 | 0 | 0 | ||
| L-2 | 2 | 0 | 0 | ||
| L-3 | 10 | 0 | 0 | ||
| L-4 | 38 | 3 | Medial (1), Lateral (2) | C (2), D (1) | 3.2 |
| L-5 | 36 | 0 | |||
| S-1 | 8 | 0 | 0 | ||
| Total | 96 | 3 | 3.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oki, T.; Lefor, A.K.; Nakamura, K.; Higashi, T.; Oki, I. Reduction in Radiation Exposure in Minimally Invasive Pedicle Screw Placement Using a Tubular Retractor: A Pilot Study. Tomography 2023, 9, 12-24. https://doi.org/10.3390/tomography9010002
Oki T, Lefor AK, Nakamura K, Higashi T, Oki I. Reduction in Radiation Exposure in Minimally Invasive Pedicle Screw Placement Using a Tubular Retractor: A Pilot Study. Tomography. 2023; 9(1):12-24. https://doi.org/10.3390/tomography9010002
Chicago/Turabian StyleOki, Takeshi, Alan Kawarai Lefor, Kentaro Nakamura, Takahiro Higashi, and Isao Oki. 2023. "Reduction in Radiation Exposure in Minimally Invasive Pedicle Screw Placement Using a Tubular Retractor: A Pilot Study" Tomography 9, no. 1: 12-24. https://doi.org/10.3390/tomography9010002