
Thoracic Inlet in Cervical Spine CT of Blunt Trauma Patients: Prevalence of Pathologies and Importance of CT Interpretation
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
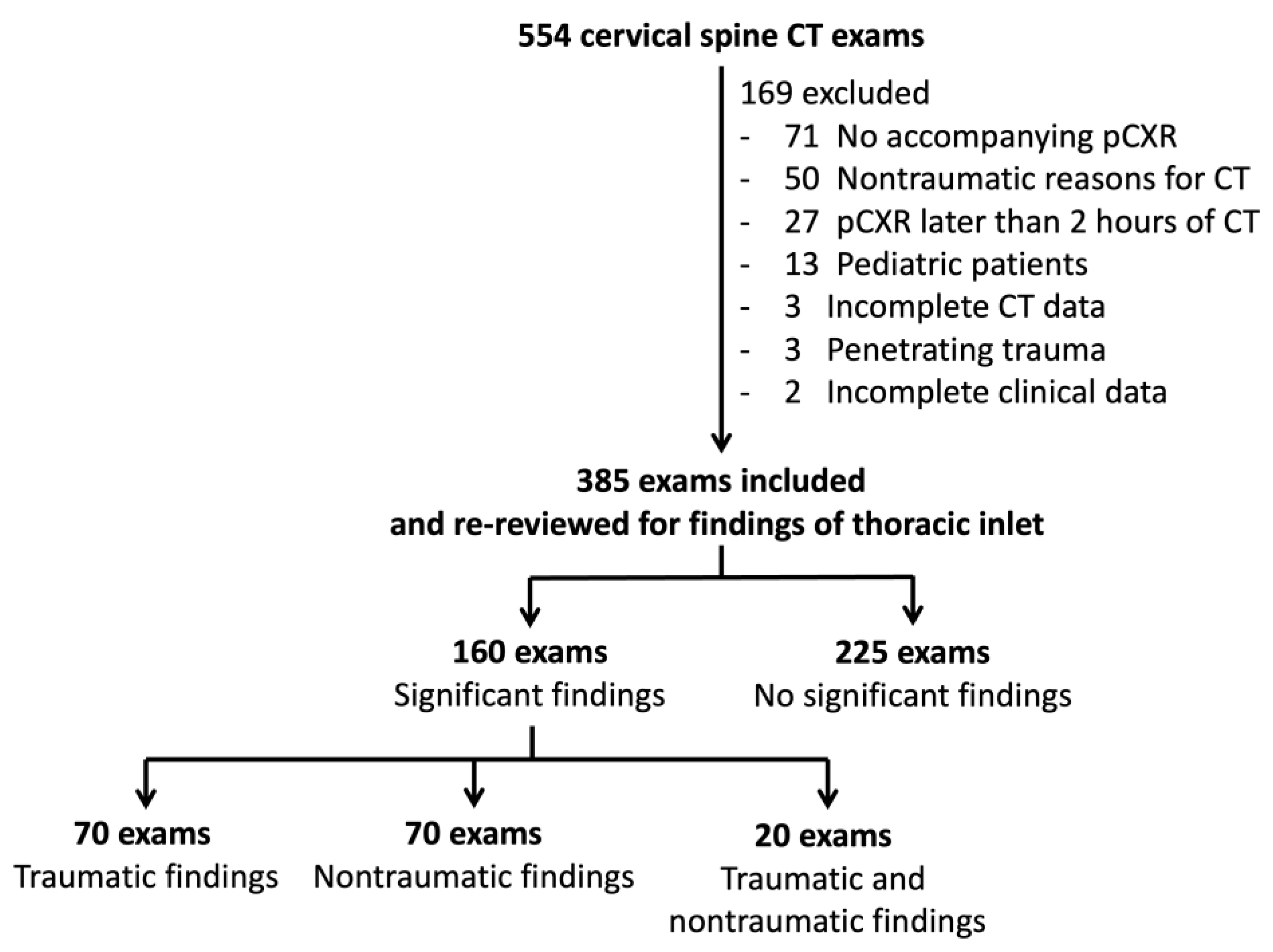
2.1. Study Design and Patients
2.2. Image Acquisition
2.3. Original Reports
2.4. Image Re-Interpretation
2.5. Definitions, Categories, Appearances of Findings and Reference Standard
2.6. Statistical Analysis
3. Results
3.1. Patient and Study Characteristics
3.2. Prevalence and Details of Pathologies of Thoracic Inlet
3.3. Performance of Portable CXR and Original CT Reports
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nguyen, T.T.; Melendez, P.E.; Kaproth-Joslin, K.; Bhatt, A. Non-neoplastic pathology at the crossroads between neck imaging and cardiothoracic imaging. Insights Imaging 2019, 10, 116. [Google Scholar] [CrossRef] [PubMed]
- Chiles, C.; Davis, K.W.; Williams, D.W. Navigating the Thoracic Inlet. RadioGraphics 1999, 19, 1161–1176. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, F.; Salazar, J. Lesions of the thoracic operculum on CT and MRI: Between the neck and the chest. Rev. Colomb. Radiol. 2017, 28, 4782–4791. [Google Scholar]
- Barboza, R.; Fox, J.H.; Shaffer, L.E.T.; Opalek, J.M.; Farooki, S. Incidental Findings in the Cervical Spine at CT for Trauma Evaluation. Am. J. Roentgenol. 2009, 192, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Balogun, S.O. Benefits and Limitations of Portable Chest Radiography. Radiol. Technol. 2021, 92, 301–304. [Google Scholar] [PubMed]
- Hinzpeter, R.; Boehm, T.; Boll, D.; Constantin, C.; Del Grande, F.; Fretz, V.; Leschka, S.; Ohletz, T.; Brönnimann, M.; Schmidt, S.M.M.; et al. Imaging algorithms and CT protocols in trauma patients: Survey of Swiss emergency centers. Eur. Radiol. 2017, 27, 1922–1928. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.M.; Mason, S. The use of whole-body CT for trauma patients: Survey of UK emergency departments. Emerg. Med. J. 2012, 29, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Dreizin, D.; Letzing, M.; Sliker, C.W.; Chokshi, F.H.; Bodanapally, U.; Mirvis, S.E.; Quencer, R.M.; Munera, F. Multidetector CT of Blunt Cervical Spine Trauma in Adults. RadioGraphics 2014, 34, 1842–1865. [Google Scholar] [CrossRef] [PubMed]
- The American College of Surgeons Committee on Trauma. Initial assessment and management. In ATLS Advanced Trauma Life Support Student Course Manual, 10th ed.; American College of Surgeons: Chicago, IL, USA, 2018; pp. 1–21. [Google Scholar]
- Kaewlai, R.; Avery, L.L.; Asrani, A.V.; Novelline, R.A. Multidetector CT of Blunt Thoracic Trauma. RadioGraphics 2008, 28, 1555–1570. [Google Scholar] [CrossRef] [PubMed]
- Mirka, H.; Ferda, J.; Baxa, J. Multidetector computed tomography of chest trauma: Indications, technique and interpretation. Insights Imaging 2012, 3, 433–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ergun, T.; Lakadamyali, H. The prevalence and clinical importance of incidental soft-tissue findings in cervical CT scans of trauma population. Dentomaxillofac. Radiol. 2013, 42, 20130216. [Google Scholar] [CrossRef] [PubMed]
- Beheshtian, E.; Sahraian, S.; Yousem, D.M.; Khan, M.K. Incidental findings on cervical spine computed tomography scans: Over-looked and unimportant? Neuroradiology 2018, 60, 1175–1180. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, A.; Yousefifard, M.; Mohammad Kazemi, H.; Rasouli, H.R.; Asady, H.; Moghadas Jafari, A.; Hosseini, M. Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax: A Systematic Review and Me-ta-Analysis. Tanaffos 2014, 13, 29–40. [Google Scholar] [PubMed]
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.L.; Clement, C.M.; Lesiuk, H.; De Maio, V.J.; Laupacis, A.; Schull, M.; McKnight, R.D.; Verbeek, R.; et al. The Canadian C-Spine Rule for Radiography in Alert and Stable Trauma Patients. JAMA 2001, 286, 1841–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, J.R.; Mower, W.R.; Wolfson, A.B.; Todd, K.H.; Zucker, M.I. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N. Engl. J. Med. 2000, 343, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Paluska, T.R.; Sise, M.J.; Sack, D.I.; Sise, C.B.; Egan, M.C.; Biondi, M. Incidental CT Findings in Trauma Patients: Incidence and Implications for Care of the Injured. J. Trauma Inj. Infect. Crit. Care 2007, 62, 157–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottesman, M.; Patel, R.R.; Parnes, G.; Ortiz, A.O. Preparing for the Unexpected: A Review of Incidental Extraspinal Findings on Computed Tomography/Magnetic Resonance Imaging of the Spine. Radiol. Clin. N. Am. 2021, 59, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Applewhite, B.P.; Buch, K.; Yoon, B.C.; Lang, M.; Li, M.D.; Rincon, S.P.; Mehan, W.A. Lung apical findings in coronavirus disease (COVID-19) infection on neck and cervical spine CT. Emerg. Radiol. 2020, 27, 731–735. [Google Scholar] [CrossRef]
- Worldometer. Total Coronavirus Cases in Thailand. Available online: https://www.worldometers.info/coronavirus/country/thailand/ (accessed on 7 November 2021).
- Brenner, D.J.; Hall, E.J. Computed Tomography—An Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Kelleher, M.S.; Gao, G.; Rolen, M.F.; Bokhari, S.J. Completion CT of Chest, Abdomen, and Pelvis after Acute Head and Cervical Spine Trauma: Incidence of Acute Traumatic Findings in the Setting of Low-Velocity Trauma. Radiology 2016, 279, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traub, M.; Stevenson, M.; McEvoy, S.; Briggs, G.; Lo, S.K.; Leibman, S.; Joseph, T. The use of chest computed tomography versus chest X-ray in patients with major blunt trauma. Injury 2007, 38, 43–47. [Google Scholar] [CrossRef]
- Tillou, A.; Gupta, M.; Baraff, L.J.; Schriger, D.L.; Hoffman, J.R.; Hiatt, J.R.; Cryer, H.M. Is the use of pan-computed tomography for blunt trauma justified? A prospective evaluation. J. Trauma 2009, 67, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Lumbreras, B.; Donat, L.; Hernández-Aguado, I. Incidental findings in imaging diagnostic tests: A systematic review. Br. J. Radiol. 2010, 83, 276–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, M.K.; Francois, M.P.; Yoeli, G.; Doughlin, G.K.; Lee, S.-W. Incidental findings in blunt trauma patients: Prevalence, follow-up documentation, and risk factors. Emerg. Radiol. 2017, 24, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Sener, R.N.; Ripeckyj, G.T.; Otto, P.M.; Rauch, R.A.; Jinkins, J.R. Recognition of abnormalities on computed scout images in CT ex-aminations of the head and spine. Neuroradiology 1993, 35, 229–231. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group 1 | Group 2 | |||||
|---|---|---|---|---|---|---|
| All Patients (n = 385) | 1.1 Trauma (n = 70) | 1.2 Significant Nontraumatic (n = 70) | 1.3 Trauma and Significant Nontraumatic (n = 20) | 2. No Trauma or Significant Nontraumatic (n = 225) | p-Value between Group 1 and Group 2 ** | |
| Demographics & clinical data | ||||||
| Male gender | 280 | 56 (80) | 48 (68.6) | 15 (75) | 161 (71.6) | 0.620 |
| Age (years; mean, SD) | 47.6 (22.1) | 37.6 (17.7) | 55.3 (21.0) | 54.9 (26.6) | 47.7 (22.2) | 0.902 |
| Trauma mechanism | 0.374 | |||||
| Fall from standing | 102 | 2 | 29 | 6 | 65 | |
| Fall from height | 22 | 4 | 2 | 1 | 15 | |
| Motorcycle collision | 177 | 50 | 21 | 6 | 100 | |
| Car collision | 17 | 7 | 1 | 1 | 8 | |
| Pedestrian/ bike accident | 27 | 3 | 7 | 2 | 15 | |
| Assault | 17 | - | 4 | 1 | 12 | |
| Others | 23 | 4 | 6 | 3 | 10 | |
| High-energy trauma mechanism (n = 362) | 243 | 64 | 31 | 10 | 138 | 0.185 |
| Time lapse from trauma onset (hours; median, range, IQR) | 1 (1–336, 2) | 1 (1–72, 1) | 1 (1–37, 2) | 1 (1–336, 3) | 1 (1–168, 2) | 0.623 |
| GCS groups | 0.149 | |||||
| Full (GCS = 15) | 190 | 32 | 35 | 4 | 119 | |
| Mild (GCS = 13–14) | 86 | 15 | 15 | 6 | 50 | |
| Moderate (GCS = 9–12) | 48 | 6 | 10 | 4 | 28 | |
| Severe (GCS = 3–8) | 61 | 17 | 10 | 6 | 28 | |
| Presence of C-spine injuries | 26 | 6 | 3 | 14 | 3 | 0.817 |
| AIS: Head (median, range, IQR) | 2 (0–5, 2) | 2 (0–5, 1) | 2 (0–5, 1) | 2 (0–5, 1) | 2 (0–5, 2) | 0.068 |
| AIS: Face (median, range, IQR) | 0 (0–4, 1) | 0 (0–4, 2) | 0 (0–3, 1) | 0 (0–4, 1) | 0 (0–4, 1.5) | 0.065 |
| AIS: Thorax (median, range, IQR) | 0 (0–5, 0) | 1 (0–5, 3) | 0 (0–3, 0) | 0 (0–4, 2) | 0 (0–3, 0) | 0.000 |
| AIS: Abdomen (median, range, IQR) | 0 (0–5, 0) | 0 (0–5, 0) | 0 (0–3, 0) | 0 (0–2, 0) | 0 (0–5, 0) | 0.010 |
| AIS: Extremity (median, range, IQR) | 0 (0–4, 1) | 0 (0–3, 2) | 0 (0–3, 1) | 0 (0–4, 2) | 0 (0–4, 1) | 0.039 |
| AIS: External (median, range, IQR) | 0 (0–5, 0) | 0 (0–5, 0) | 1 (0–3, 0) | 1 (0–1, 1) | 1 (0–2, 0) | 0.130 |
| ISS (median, range, IQR) | 10 (0–45, 14) | 18 (1–45, 20) | 10 (1–34, 12) | 11 (1–36, 19) | 9 (0–41, 12) | 0.000 |
| Presentation outside of normal working hours | 276 | 52 | 52 | 9 | 163 | 0.783 |
| Treatment of neck injuries | 0.479 | |||||
| None | 225 | 31 | 48 | 14 | 132 | |
| Cervical collar | 158 | 39 | 22 | 6 | 91 | |
| Surgery | 2 | 0 | 0 | 0 | 2 | |
| Treatment of chest injuries | 0.000 | |||||
| None | 361 | 53 | 69 | 18 | 221 | |
| Unilateral or bilateral ICD | 23 | 16 | 1 | 2 | 4 | |
| TEVAR | 1 | 1 | 0 | 0 | 0 | |
| Hospital admission | 196 | 42 | 37 | 13 | 104 | 0.038 |
| Length of stay (days; median, range, IQR; n = 196) | 6 (0–180, 11) | 10 (0–92, 15) | 4 (0–27, 8) | 8 (0–34, 10) | 5 (0–180, 9) | 0.434 |
| Discharge status (n = 364) | 0.056 | |||||
| Death | 20 | 4 | 6 | 3 | 7 | |
| Transfer | 107 | 24 | 18 | 5 | 60 | |
| Alive | 237 | 39 | 41 | 11 | 146 | |
| Length of follow up (days; median, range, IQR) | 21 (0–540, 194) | 29 (0–474, 185) | 9 (0–532, 290) | 4 (0–287, 96) | 22 (0–540, 200) | 0.915 |
| CT imaging data | ||||||
| C-spine CT including head CT | 360 | 67 | 65 | 20 | 208 | 0.428 |
| Chest CT within 24 h of trauma | 31 | 18 | 3 | 4 | 6 | 0.0001 |
| Official CT report verified by attending radiologist ** | 210 | 37 | 46 | 9 | 118 | 0.380 |
| Reporting radiologist experience >10 years | 183 | 32 | 40 | 8 | 103 | 0.475 |
| Thoracic Inlet Pathologies | N (%) | Corresponding Radiographic Findings |
|---|---|---|
| Traumatic findings | 92 (23.90) | |
| Mediastinal fat stranding | 5 | Abnormal mediastinum |
| Mediastinal hemorrhage | 4 | Abnormal mediastinum |
| Pneumomediastinum | 1 | Pneumomediastinum |
| Pulmonary contusion | 40 | Patchy opacification |
| Pulmonary laceration | 3 | None |
| Pneumothorax | 49 | Pneumothorax |
| Pleural fluid | 9 | Apical cap |
| Extrapleural hematoma | 2 | Apical cap |
| Rib fracture: first | 13 | Rib fracture: first |
| Rib fracture: second | 14 | Rib fracture: second |
| Rib fracture: third | 9 | Rib fracture: third |
| Rib fracture: fourth | 7 | Rib fracture: fourth |
| Clavicle fracture | 8 | Clavicle fracture |
| Acromioclavicular dislocation | 0 | Acromioclavicular dislocation |
| Scapular fracture | 1 | Scapular fracture |
| Significant nontraumatic | 90 (23.38) | |
| Mediastinal vascular dilation | 4 | Abnormal mediastinum |
| Pulmonary nodule(s) | 31 | Pulmonary nodule(s) |
| Pulmonary micronodules | 26 | N/A |
| Groundglass opacity | 6 | N/A |
| Groundglass nodule(s) | 5 | N/A |
| Cavity | 3 | Cavity |
| Atelectasis | 2 | Increased opacity with volume loss |
| Septal thickening * | 24 | N/A |
| Active tuberculosis | 13 | Active tuberculosis |
| Pulmonary malignancy | 2 | Pulmonary malignancy |
| Foreign body | 1 | Radiopaque foreign body |
| Malignant bone lesions | 1 | Lucent bone lesions |
| Non-significant abnormalities | 224 (58.18) | |
| Parenchymal scars | 74 | Parenchymal scars |
| Calcifications | 15 | Calcifications |
| Bronchiectasis | 24 | Bronchiectasis |
| Emphysema | 62 | Emphysema |
| Blebs/bulla | 55 | Blebs/bulla |
| Benign bone lesions | 4 | Lucent bone lesions |
| True Positive | False Positive | False Negative | True Negative | Sensitivity (95% CI) | Specificity (95% CI) | Accuracy (95% CI) | |
|---|---|---|---|---|---|---|---|
| Overall performance | 65 | 45 | 96 | 179 | 40.37 (32.72–48.38) | 79.91 (74.06–84.95) | 63.38 (58.35–68.20) |
| All traumatic findings | 25 | 1 | 67 | 292 | 27.17 (18.42–37.45) | 99.66 (98.11–99.99) | 82.34 (78.15–86.02) |
| All significant nontraumatic findings | 8 | 12 | 13 | 59 | 38.10 (18.11–61.56) | 83.10 (72.34–90.95) | 72.83 (62.55–81.58) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaewlai, R.; Chatpuwaphat, J.; Butnian, K.; Thusneyapan, K.; Panrong, N.; Lertpipopmetha, W.; Wongpongsalee, T. Thoracic Inlet in Cervical Spine CT of Blunt Trauma Patients: Prevalence of Pathologies and Importance of CT Interpretation. Tomography 2022, 8, 2772-2783. https://doi.org/10.3390/tomography8060231
Kaewlai R, Chatpuwaphat J, Butnian K, Thusneyapan K, Panrong N, Lertpipopmetha W, Wongpongsalee T. Thoracic Inlet in Cervical Spine CT of Blunt Trauma Patients: Prevalence of Pathologies and Importance of CT Interpretation. Tomography. 2022; 8(6):2772-2783. https://doi.org/10.3390/tomography8060231
Chicago/Turabian StyleKaewlai, Rathachai, Jitti Chatpuwaphat, Krittachat Butnian, Kittipott Thusneyapan, Nutthanun Panrong, Wanicha Lertpipopmetha, and Thongsak Wongpongsalee. 2022. "Thoracic Inlet in Cervical Spine CT of Blunt Trauma Patients: Prevalence of Pathologies and Importance of CT Interpretation" Tomography 8, no. 6: 2772-2783. https://doi.org/10.3390/tomography8060231