

Chronological Course and Clinical Features after Denver Peritoneovenous Shunt Placement in Decompensated Liver Cirrhosis
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Denver Peritoneovenous Shunt Placement
2.3. Clinical Course after PVS (Heart Failure and DIC)
2.4. Chronological Changes of Ascites
2.5. Incidence of Complications and PVS Patency
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Chronological Changes of Clinical Course
3.2.1. Heart Failure Index before and after PVS (BNP, CTR)
3.2.2. Thrombotic Disease Index before and after PVS (D-Dimer, Platelet Count)
3.2.3. Ascites before and after PVS
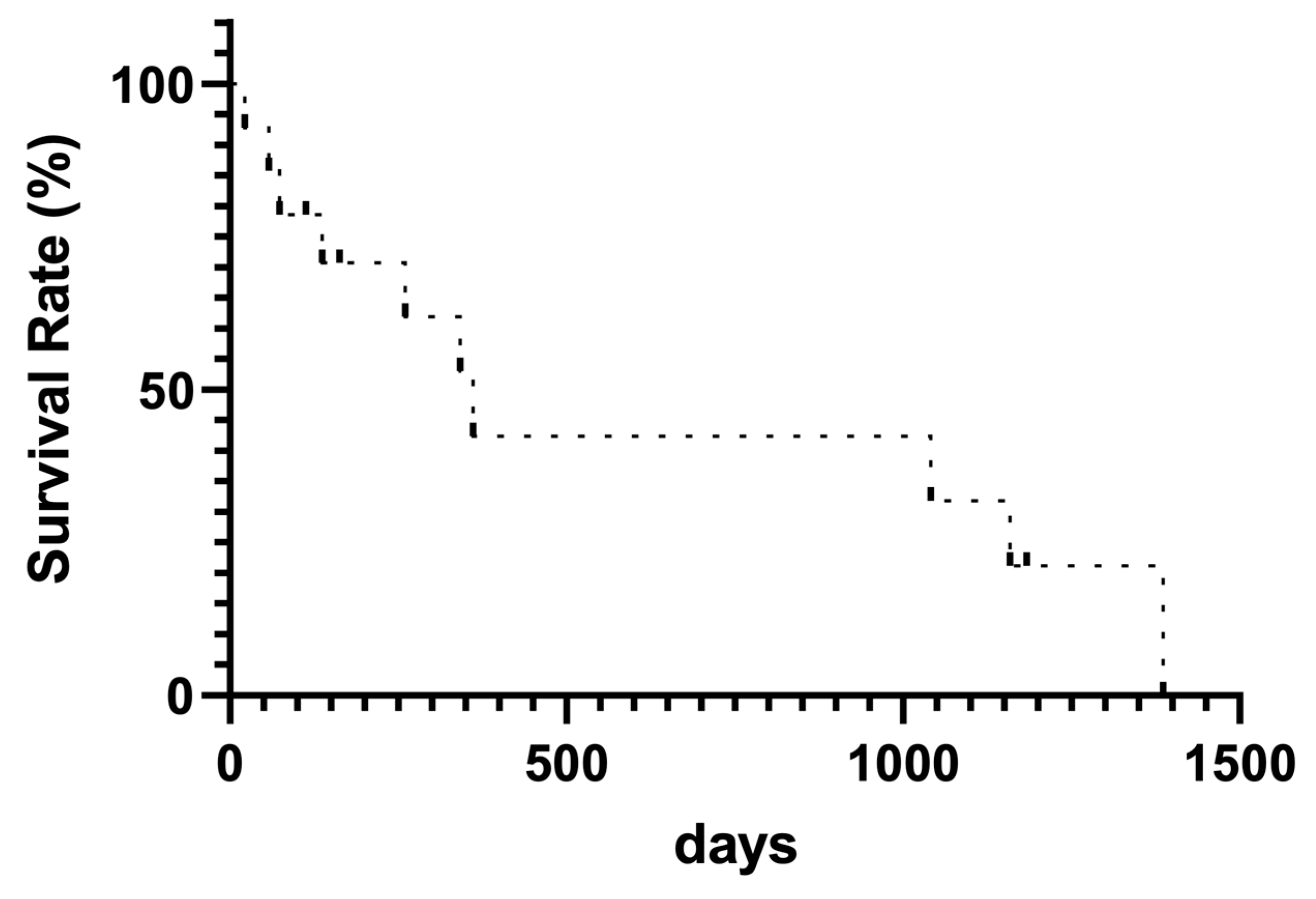
3.3. Complications and PVS Patency
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Piccirillo, M.; Rinaldi, L.; Leongito, M.; Amore, A.; Crispo, A.; Granata, V.; Aprea, P.; Izzo, F. Percutaneous implant of Denver peritoneo-venous shunt for treatment of refractory ascites: A single center retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 3668–3673. [Google Scholar]
- Fukui, H.; Kawaratani, H.; Kaji, K.; Takaya, H.; Yoshiji, H. Management of refractory cirrhotic ascites: Challenges and solutions. Hepat. Med. 2018, 10, 55–71. [Google Scholar] [CrossRef]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for Liver Cirrhosis 2020. J. Gastroenterol. 2021, 56, 593–619. [Google Scholar] [CrossRef]
- Yoshiji, H. Management of cirrhotic ascites: Seven-step treatment protocol based on the Japanese evidence-based clinical practice guidelines for liver cirrhosis 2020. Hepatol. Res. 2023. [Google Scholar] [CrossRef]
- Wong, F. Management of refractory ascites. Clin. Mol. Hepatol. 2023, 29, 16–32. [Google Scholar] [CrossRef]
- Jepsen, P.; Watson, H.; Macdonald, S.; Vilstrup, H.; Jalan, R. MELD remains the best predictor of mortality in outpatients with cirrhosis and severe ascites. Aliment. Pharmacol. Ther. 2020, 52, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiar, M.; Forde, K.A.; Nadolski, G.J.; Soulen, M.C.; Weinberg, E.M. Radiologically Placed Peritoneovenous Shunt is an Acceptable Treatment Alternative for Refractory Ascites Due to End-Stage Liver Disease. J. Vasc. Interv. Radiol. 2021, 32, 1606–1614. [Google Scholar] [CrossRef]
- Yarmohammadi, H.; Getrajdman, G.I. Symptomatic Fluid Drainage: Peritoneovenous Shunt Placement. Semin. Intervent Radiol. 2017, 34, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Gilbert, J. The development of clinical guidelines on paracentesis for ascites related to malignancy. Palliat. Med. 2002, 16, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Heiss, M.M.; Murawa, P.; Koralewski, P.; Kutarska, E.; Kolesnik, O.O.; Ivanchenko, V.V.; Dudnichenko, A.S.; Aleknaviciene, B.; Razbadauskas, A.; Gore, M.; et al. The trifunctional antibody catumaxomab for the treatment of malignant ascites due to epithelial cancer: Results of a prospective randomized phase II/III trial. Int. J. Cancer 2010, 127, 2209–2221. [Google Scholar] [CrossRef] [PubMed]
- Reinglas, J.; Amjadi, K.; Petrcich, B.; Momoli, F.; Shaw-Stiffel, T. The Palliative Management of Refractory Cirrhotic Ascites Using the PleurX (©) Catheter. Can. J. Gastroenterol. Hepatol. 2016, 2016, 4680543. [Google Scholar] [CrossRef]
- Sugawara, S.; Sone, M.; Arai, Y.; Sakamoto, N.; Aramaki, T.; Sato, Y.; Inaba, Y.; Takeuchi, Y.; Ueno, T.; Matsueda, K.; et al. Radiological insertion of Denver peritoneovenous shunts for malignant refractory ascites: A retrospective multicenter study (JIVROSG-0809). Cardiovasc. Intervent. Radiol. 2011, 34, 980–988. [Google Scholar] [CrossRef]
- Oriuchi, N.; Nakajima, T.; Mochiki, E.; Takeyoshi, I.; Kanuma, T.; Endo, K.; Sakamoto, J. A new, accurate and conventional five-point method for quantitative evaluation of ascites using plain computed tomography in cancer patients. Jpn. J. Clin. Oncol. 2005, 35, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Leveen, H.H.; Christoudias, G.; Ip, M.; Luft, R.; Falk, G.; Grosberg, S. Peritoneo-venous shunting for ascites. Ann. Surg. 1974, 180, 580–591. [Google Scholar] [CrossRef] [PubMed]
- White, M.A.; Agle, S.C.; Padia, R.K.; Zervos, E.E. Denver peritoneovenous shunts for the management of malignant ascites: A review of the literature in the post LeVeen Era. Am. Surg. 2011, 77, 1070–1075. [Google Scholar] [CrossRef]
- Segawa, T.; Kato, K.; Kawashima, K.; Suzuki, T.; Ehara, S. The influence of a peritoneovenous shunt for cirrhotic and malignant intractable ascites on renal function. Acta Radiol. Open 2018, 7, 2058460118764208. [Google Scholar] [CrossRef] [PubMed]
- EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J. Hepatol. 2010, 53, 397–417. [CrossRef] [PubMed]
- Biggins, S.W.; Angeli, P.; Garcia-Tsao, G.; Ginès, P.; Ling, S.C.; Nadim, M.K.; Wong, F.; Kim, W.R. Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 74, 1014–1048. [Google Scholar] [CrossRef]
- Solà, E.; Solé, C.; Ginès, P. Management of uninfected and infected ascites in cirrhosis. Liver Int. 2016, 36 Suppl 1, 109–115. [Google Scholar] [CrossRef]
- Rosemurgy, A.S.; Zervos, E.E.; Clark, W.C.; Thometz, D.P.; Black, T.J.; Zwiebel, B.R.; Kudryk, B.T.; Grundy, L.S.; Carey, L.C. TIPS versus peritoneovenous shunt in the treatment of medically intractable ascites: A prospective randomized trial. Ann. Surg. 2004, 239, 883–889; discussion 889–891. [Google Scholar] [CrossRef]
- Soyama, A.; Eguchi, S.; Egawa, H. Liver transplantation in Japan. Liver Transpl. 2016, 22, 1401–1407. [Google Scholar] [CrossRef]
- Smith, E.M.; Jayson, G.C. The current and future management of malignant ascites. Clin. Oncol. (R. Coll. Radiol.) 2003, 15, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, K.; Takahashi, M.; Fujii, T.; Kunisue, H.; Kanaya, Y.; Maruyama, S.; Yokoyama, N.; Nakao, A.; Soda, M.; Shimizu, N. Improved quality of life for malignant ascites patients by Denver peritoneovenous shunts. Anticancer. Res. 2006, 26, 2393–2395. [Google Scholar] [PubMed]
- Yarmohammadi, H.; Brody, L.A.; Erinjeri, J.P.; Covey, A.M.; Boas, F.E.; Ziv, E.; Maybody, M.; Gonzalez-Aguirre, A.J.; Brown, K.T.; Sheinfeld, J.; et al. Therapeutic Application of Percutaneous Peritoneovenous (Denver) Shunt in Treating Chylous Ascites in Cancer Patients. J. Vasc. Interv. Radiol. 2016, 27, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Will, V.; Rodrigues, S.G.; Berzigotti, A. Current treatment options of refractory ascites in liver cirrhosis—A systematic review and meta-analysis. Dig. Liver Dis. 2022, 54, 1007–1014. [Google Scholar] [CrossRef]
- Bieligk, S.C.; Calvo, B.F.; Coit, D.G. Peritoneovenous shunting for nongynecologic malignant ascites. Cancer 2001, 91, 1247–1255. [Google Scholar] [CrossRef]
- Faught, W.; Kirkpatrick, J.R.; Krepart, G.V.; Heywood, M.S.; Lotocki, R.J. Peritoneovenous shunt for palliation of gynecologic malignant ascites. J. Am. Coll. Surg. 1995, 180, 472–474. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Patients (N = 14) | |
|---|---|
| Age (years, SD) | 66.2 (15.6) |
| Male sex (n, %) | 8 (57.1) |
| Height (m, SD) | 1.59 (0.02) |
| Body Weight (kg, SD) | 67.2 (5.0) |
| HCV/AIH/SLD/others | 3/2/6/3 |
| HCC (%) | 3 (21.4) |
| Albumin (g/dL, SD) | 2.77 (0.23) |
| Total Bilirubin (mg/dL, SD) | 1.46 (0.28) |
| D-dimer (μg/mL, range) | 14.8 (0.5–72.2) |
| BNP (pg/mL, range) | 78.9 (7.3–300.2) |
| No. | Age | Etiology | Existence date | PVS Occlusion | Ascites Volume | Abdominal Paracentesis (Times/Month) | Diuretic | Lifetime Date | Cause of Death | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | After | |||||||||||||||
| Before | After | Before | After | F | S | T | F | S | T | |||||||
| 1 | 60s | Extrahepatic PVO | 864 | Yes | 3600 | 960 | 2 | 0 | 140 | 100 | – | 40 | 100 | – | 1159 | Colon cancer |
| 2 | 60s | AIH | 23 | Yes | N/A | 3 | 0 | 60 | – | 7.5 | 60 | – | 15 | 58 | LF | |
| 3 | 60s | SLD | 1386 | No | N/A | 3 | 0 | 40 | – | 3.75 | 80 | 50 | 7.5 | 1386 | LF | |
| 4 | 70s | AIH | 74 | Yes | N/A | 4 | 2 | 20 | – | 3.75 | 20 | – | 3.75 | 74 | LF | |
| 5 | 70s | SLD | 212 | Yes | 4140 | 820 | 2 | 0 | 80 | 25 | 7.5 | – | 25 | – | 1041 | Infection |
| 6 | 60s | SLD | 1184 | No | 1920 | 1420 | 3 | 0 | – | – | – | – | – | – | – | – |
| 7 | 60s | SLD | 133 | No | N/A | 3 | 0 | 20 | – | 7.5 | – | – | – | 137 | LF | |
| 8 | 70s | HCV | 22 | Yes | N/A | 4 | 0 | 40 | 50 | 7.5 | 40 | – | – | 22 | CI | |
| 9 | 60s | HCV | 62 | yes | 2900 | 0 | 3 | 0 | 80 | 50 | 7.5 | 80 | 50 | 7.5 | 260 | GB rupture |
| 10 | 60s | HCV | 361 | No | 2500 | 1480 | 4 | 0 | 40 | – | 7.5 | 20 | – | 7.5 | 361 | SBP |
| 11 | 70s | SLD | 38 | No | N/A | 4 | 2 | 40 | 100 | 7.5 | 10 | 50 | 7.5 | 342 | CHF | |
| 12 | 70s | PBC | 342 | No | 4720 | 1560 | 3 | 0 | 20 | 50 | 7.5 | 0 | 50 | 7.5 | – | – |
| 13 | 40s | SLD | 22 | No | 3160 | 0 | 3 | 0 | 40 | 100 | 7.5 | 20 | – | 3.75 | – | – |
| 14 | 40s | SLD | 113 | No | 4180 | 1180 | 4 | 0 | 40 | 100 | 7.5 | 20 | 100 | 7.5 | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koyama, S.; Nogami, A.; Yoneda, M.; Cheng, S.; Koike, Y.; Takeuchi, Y.; Iwaki, M.; Kobayashi, T.; Saito, S.; Utsunomiya, D.; et al. Chronological Course and Clinical Features after Denver Peritoneovenous Shunt Placement in Decompensated Liver Cirrhosis. Tomography 2024, 10, 471-479. https://doi.org/10.3390/tomography10040036
Koyama S, Nogami A, Yoneda M, Cheng S, Koike Y, Takeuchi Y, Iwaki M, Kobayashi T, Saito S, Utsunomiya D, et al. Chronological Course and Clinical Features after Denver Peritoneovenous Shunt Placement in Decompensated Liver Cirrhosis. Tomography. 2024; 10(4):471-479. https://doi.org/10.3390/tomography10040036
Chicago/Turabian StyleKoyama, Shingo, Asako Nogami, Masato Yoneda, Shihyao Cheng, Yuya Koike, Yuka Takeuchi, Michihiro Iwaki, Takashi Kobayashi, Satoru Saito, Daisuke Utsunomiya, and et al. 2024. "Chronological Course and Clinical Features after Denver Peritoneovenous Shunt Placement in Decompensated Liver Cirrhosis" Tomography 10, no. 4: 471-479. https://doi.org/10.3390/tomography10040036