
Detection of Hyperdense Arterial Sign in Acute Ischemic Stroke with Dual-Energy Computed Tomography: Optimal Combination with X-ray Energy and Slice Thickness
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
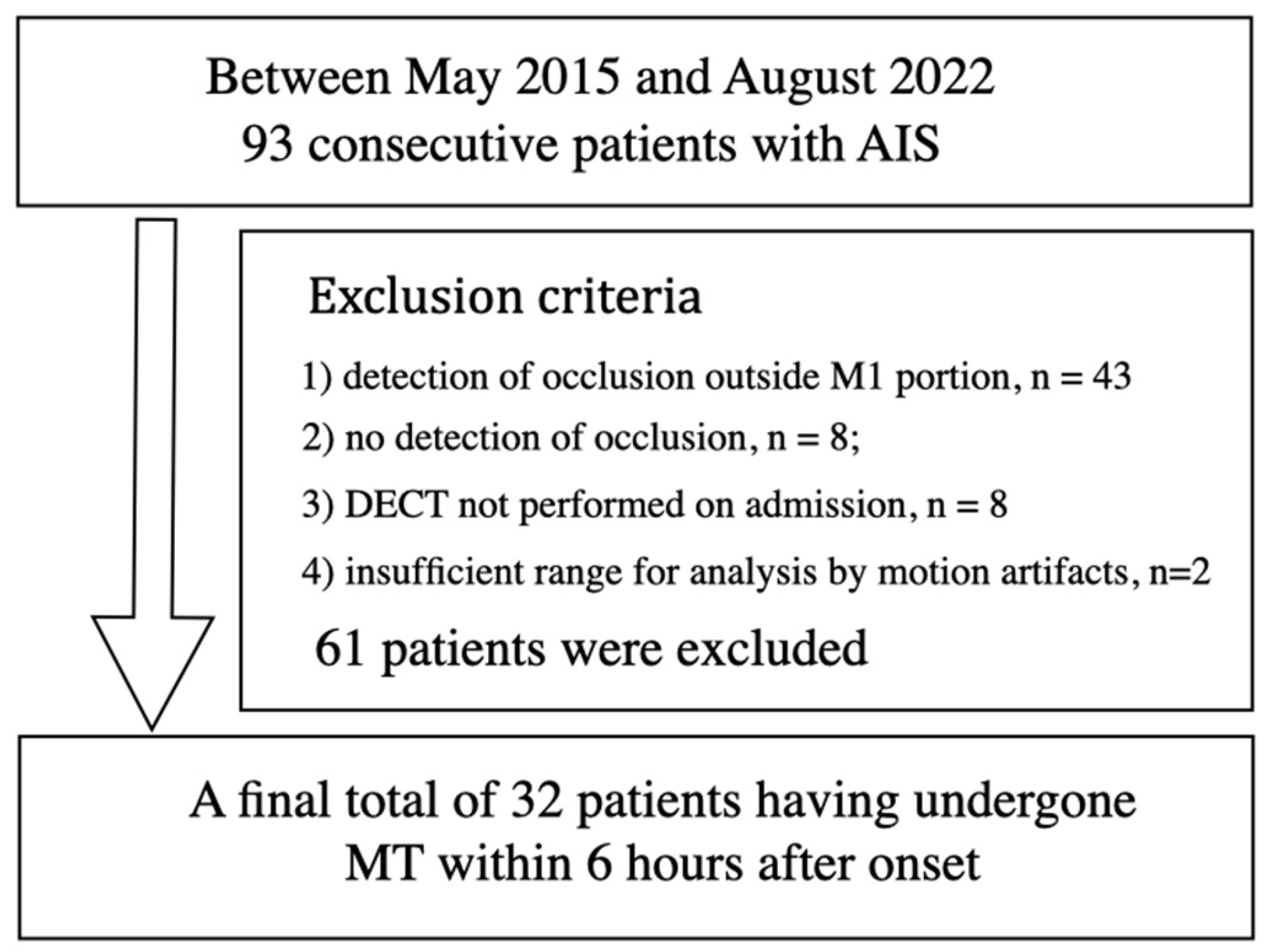
2.1. Patients
2.2. Dual-Energy CT
2.3. Modified CNR of HAS Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institute of Neurological Disorders; Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Goyal, M.; van der Lugt, A.; Menon, B.K.; Majoie, C.B.; Dippel, D.W.; Campbell, B.C.; Nogueira, R.G.; Demchuk, A.M.; Tomasello, A.; et al. Time to Treatment with Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis. JAMA 2016, 316, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Menon, B.K.; Campbell, B.C.; Levi, C.; Goyal, M. Role of imaging in current acute ischemic stroke workflow for endovascular therapy. Stroke 2015, 46, 1453–1461. [Google Scholar] [CrossRef]
- Gacs, G.; Fox, A.J.; Barnett, H.J.; Vinuela, F. CT visualization of intracranial arterial thromboembolism. Stroke 1983, 14, 756–762. [Google Scholar] [CrossRef]
- von Kummer, R.; Meyding-Lamade, U.; Forsting, M.; Rosin, L.; Rieke, K.; Hacke, W.; Sartor, K. Sensitivity and prognostic value of early CT in occlusion of the middle cerebral artery trunk. AJNR Am. J. Neuroradiol. 1994, 15, 9–15. [Google Scholar]
- Leys, D.; Pruvo, J.P.; Godefroy, O.; Rondepierre, P.; Leclerc, X. Prevalence and significance of hyperdense middle cerebral artery in acute stroke. Stroke 1992, 23, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Tomsick, T.; Brott, T.; Barsan, W.; Broderick, J.; Haley, E.C.; Spilker, J. Thrombus localization with emergency cerebral, C.T. AJNR Am. J. Neuroradiol. 1992, 13, 257–263. [Google Scholar] [PubMed]
- Kim, E.Y.; Lee, S.K.; Kim, D.J.; Suh, S.H.; Kim, J.; Heo, J.H.; Kim, D.I. Detection of thrombus in acute ischemic stroke: Value of thin-section non-contrast-computed tomography. Stroke 2005, 36, 2745–2747. [Google Scholar] [CrossRef]
- Riedel, C.H.; Jensen, U.; Rohr, A.; Tietke, M.; Alfke, K.; Ulmer, S.; Jansen, O. Assessment of thrombus in acute middle cerebral artery occlusion using thin-slice nonenhanced Computed Tomography reconstructions. Stroke 2010, 41, 1659–1664. [Google Scholar] [CrossRef]
- Johnson TR Dual-energy CT: General principles. AJR Am. J. Roentgenol. 2012, 199, S3–S8. [CrossRef]
- McCollough, C.H.; Leng, S.; Yu, L.; Fletcher, J.G. Dual- and Multi-Energy CT: Principles, Technical Approaches, and Clinical Applications. Radiology 2015, 276, 637–653. [Google Scholar] [CrossRef]
- Schmidt, B.; Flohr, T. Principles and applications of dual source, C.T. Phys. Med. 2020, 79, 36–46. [Google Scholar] [CrossRef]
- Postma, A.A.; Das, M.; Stadler, A.A.; Wildberger, J.E. Dual energy CT: What the neuroradiologist should know. Curr. Radiol. Rep. 2015, 3, 16. [Google Scholar] [CrossRef]
- Yu, L.; Christner, J.A.; Leng, S.; Wang, J.; Fletcher, J.G.; McCollough, C.H. Virtual monochromatic imaging in dual-source dual-energy CT: Radiation dose and image quality. Med. Phys. 2011, 38, 6371–6379. [Google Scholar] [CrossRef]
- Yu, L.; Leng, S.; McCollough, C.H. Dual-energy CT-based monochromatic imaging. AJR Am. J. Roentgenol. 2012, 199 (Suppl. 5), S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, K.; Itoh, T.; Naruto, N.; Takashima, S.; Tanaka, K.; Kuroda, S. A novel imaging technique (X-map) to identify acute ischemic lesions using noncontrast dual-energy computed tomography. J. Stroke Cerebrovasc. Dis. 2017, 26, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Itoh, T.; Noguchi, K. Evaluation of the Quantitative Performance of Non-enhanced Dual-energy CT X-map in Detecting Acute Ischemic Brain Stroke: A Model Observer Study using Computer. Phys. Med. 2022, 104, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, M.F.; Marais, O.; Min, A.; Ferguson, D.; Jalal, S.; Khosa, F.; O’Keeffe, M.; O’Connell, T.; Schmiedeskamp, H.; Krauss, B.; et al. Unenhanced Dual-Energy Computed Tomography: Visualization of Brain Edema. Investig. Radiol. 2017, 53, 63–69. [Google Scholar] [CrossRef]
- Grams, A.E.; Djurdjevic, T.; Rehwald, R.; Schiestl, T.; Dazinger, F.; Steiger, R.; Knoflach, M.; Gizewski, E.R.; Glodny, B. Improved visualisation of early cerebral infarctions after endovascular stroke therapy using dual-energy computed tomography oedema maps. Eur. Radiol. 2018, 28, 4534–4541. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rank | VMI Settings-Slice Thickness | Mean CNR of HAS | SD | 95% Confidence Interval Lower Limit to Upper Limit | |
|---|---|---|---|---|---|
| 1 | 60 keV-1 mm | 2.907 | 0.683 | 2.660 | 3.153 |
| 2 | 70 keV-1 mm | 2.886 | 0.668 | 2.644 | 3.126 |
| 3 | 60 keV-2 mm | 2.866 | 0.689 | 2.617 | 3.114 |
| 4 | 80 keV-1 mm | 2.857 | 0.653 | 2.594 | 3.056 |
| 5 | 60 keV-3 mm | 2.841 | 0.691 | 2.591 | 3.089 |
| 6 | 70 keV-2 mm | 2.835 | 0.671 | 2.592 | 3.077 |
| 7 | 90 keV-1 mm | 2.825 | 0.640 | 2.594 | 3.056 |
| 8 | 70 keV-3 mm | 2.808 | 0.672 | 2.565 | 3.050 |
| 9 | 80 keV-2 mm | 2.800 | 0.654 | 2.563 | 3.035 |
| 10 | 100 keV-1 mm | 2.797 | 0.632 | 2.568 | 3.024 |
| Thickness (I) | Thickness (J) | Mean CNR Difference (I-J) | Standard Error | p-Value | 95% Confidence Interval Lower Limit to Upper Limit | |
|---|---|---|---|---|---|---|
| 1.0 mm | 2.0 mm | 0.118 | 0.042 | 0.029 * | 0.007 | 0.229 |
| 3.0 mm | 0.146 | 0.042 | 0.003 * | 0.035 | 0.257 | |
| 2.0 mm | 1.0 mm | −0.118 | 0.042 | 0.029 * | −0.229 | −0.007 |
| 3.0 mm | 0.027 | 0.042 | 10.000 | −0.083 | 0.138 | |
| 3.0 mm | 1.0 mm | −0.146 | 0.042 | 0.003 * | −0.257 | −0.035 |
| 2.0 mm | −0.027 | 0.042 | 10.000 | −0.138 | 0.083 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noguchi, K.; Kido, A.; Naruto, N.; Doai, M.; Itoh, T.; Kashiwazaki, D.; Akioka, N.; Kuroda, S. Detection of Hyperdense Arterial Sign in Acute Ischemic Stroke with Dual-Energy Computed Tomography: Optimal Combination with X-ray Energy and Slice Thickness. Tomography 2024, 10, 360-367. https://doi.org/10.3390/tomography10030028
Noguchi K, Kido A, Naruto N, Doai M, Itoh T, Kashiwazaki D, Akioka N, Kuroda S. Detection of Hyperdense Arterial Sign in Acute Ischemic Stroke with Dual-Energy Computed Tomography: Optimal Combination with X-ray Energy and Slice Thickness. Tomography. 2024; 10(3):360-367. https://doi.org/10.3390/tomography10030028
Chicago/Turabian StyleNoguchi, Kyo, Aki Kido, Norihito Naruto, Mariko Doai, Toshihide Itoh, Daina Kashiwazaki, Naoki Akioka, and Satoshi Kuroda. 2024. "Detection of Hyperdense Arterial Sign in Acute Ischemic Stroke with Dual-Energy Computed Tomography: Optimal Combination with X-ray Energy and Slice Thickness" Tomography 10, no. 3: 360-367. https://doi.org/10.3390/tomography10030028