
Physiological and Thermal Sensation Responses to Severe Cold Exposure (−20 °C)


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Volunteers
2.2. Experimental Conditions
2.3. Measurements
2.3.1. Physiological Responses
2.3.2. Questionnaires
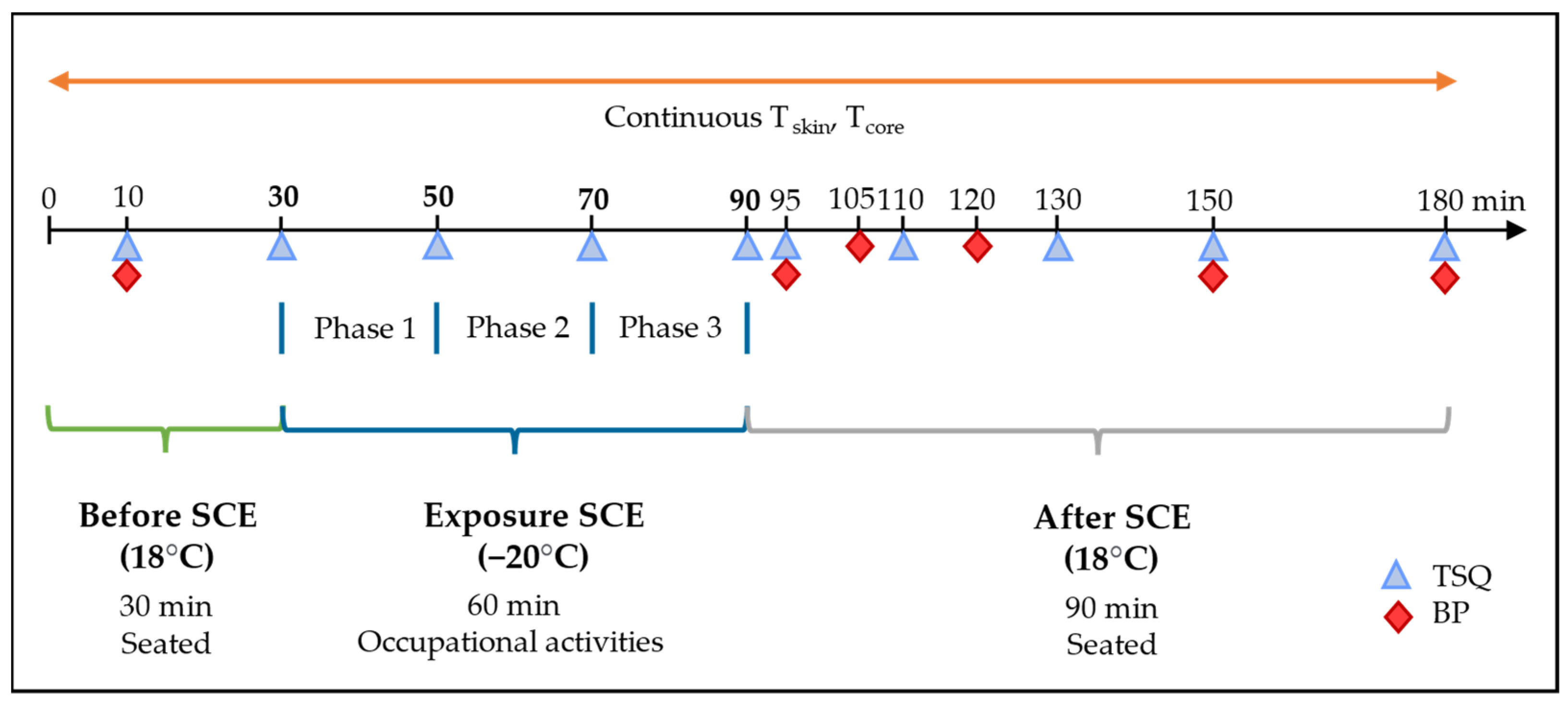
2.4. Experimental Protocol
2.4.1. Initial Contact and Medical Examinations
2.4.2. Before Going into the Climatic Chamber
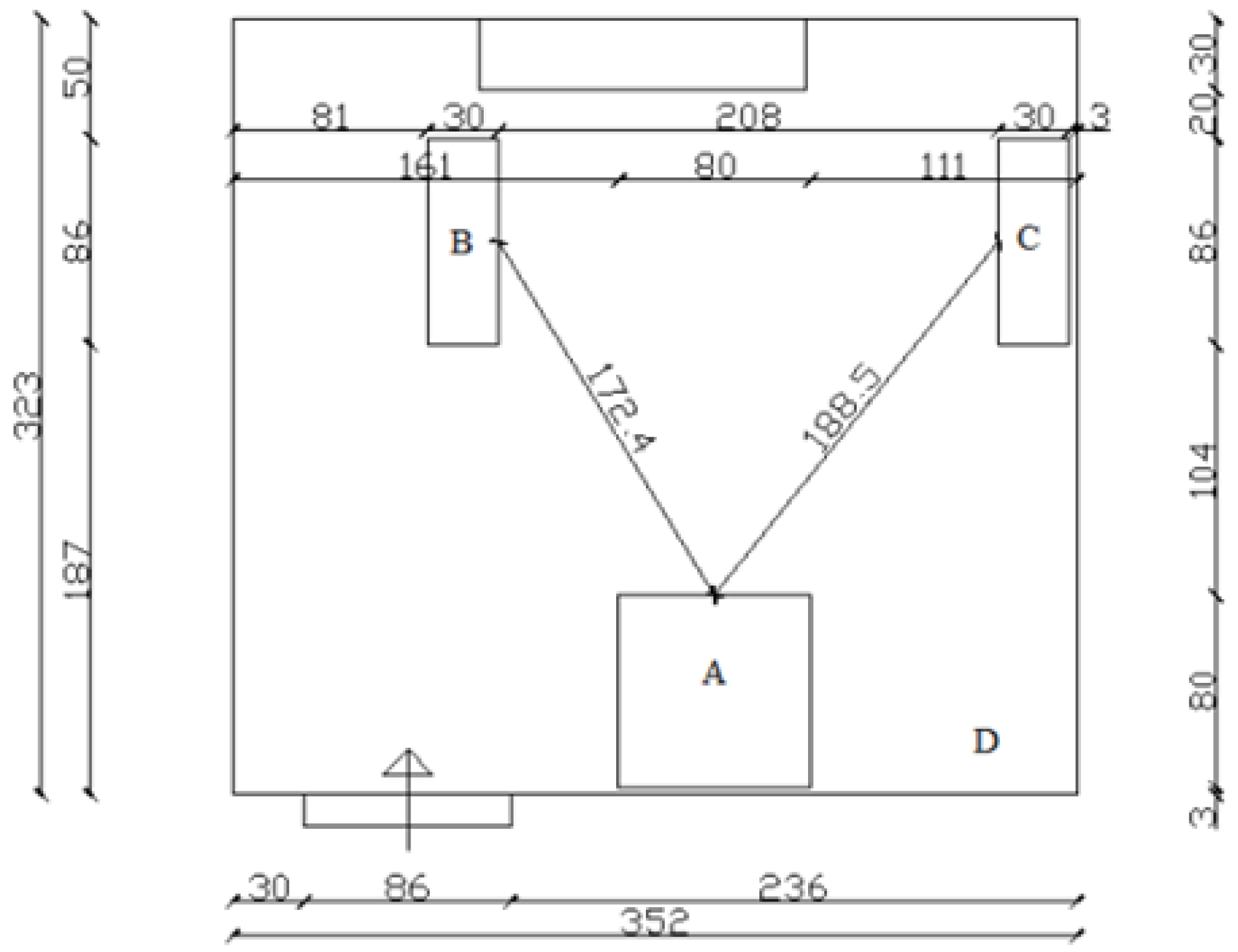
2.4.3. Occupational Activities Inside the Chamber
2.4.4. Following Exposure to SCE
2.5. Data Analyses
3. Results
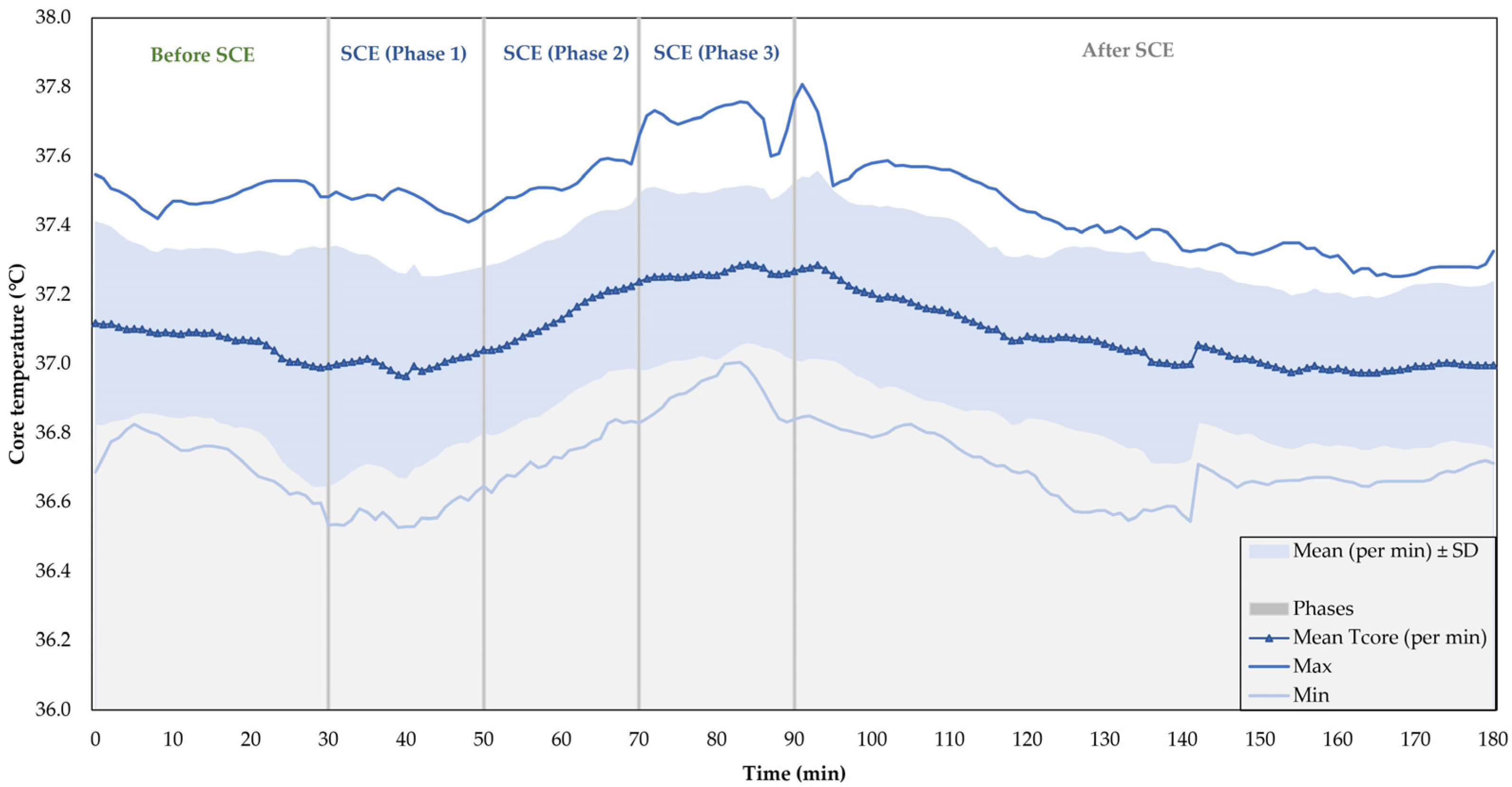
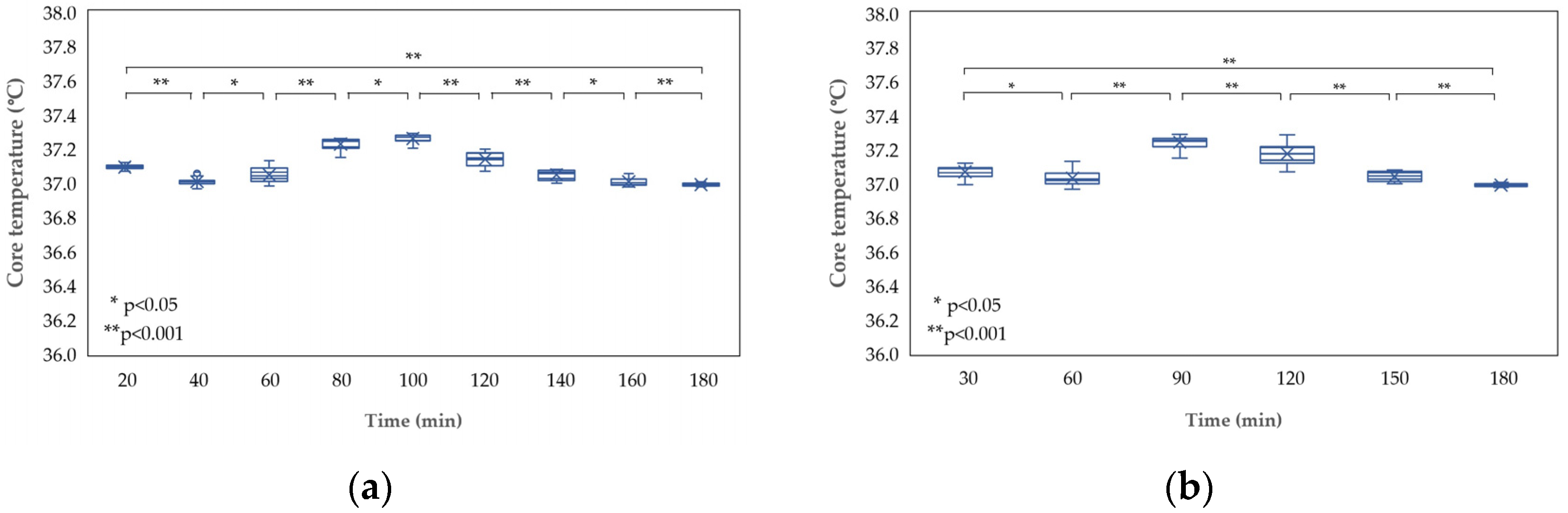
3.1. Core Temperature
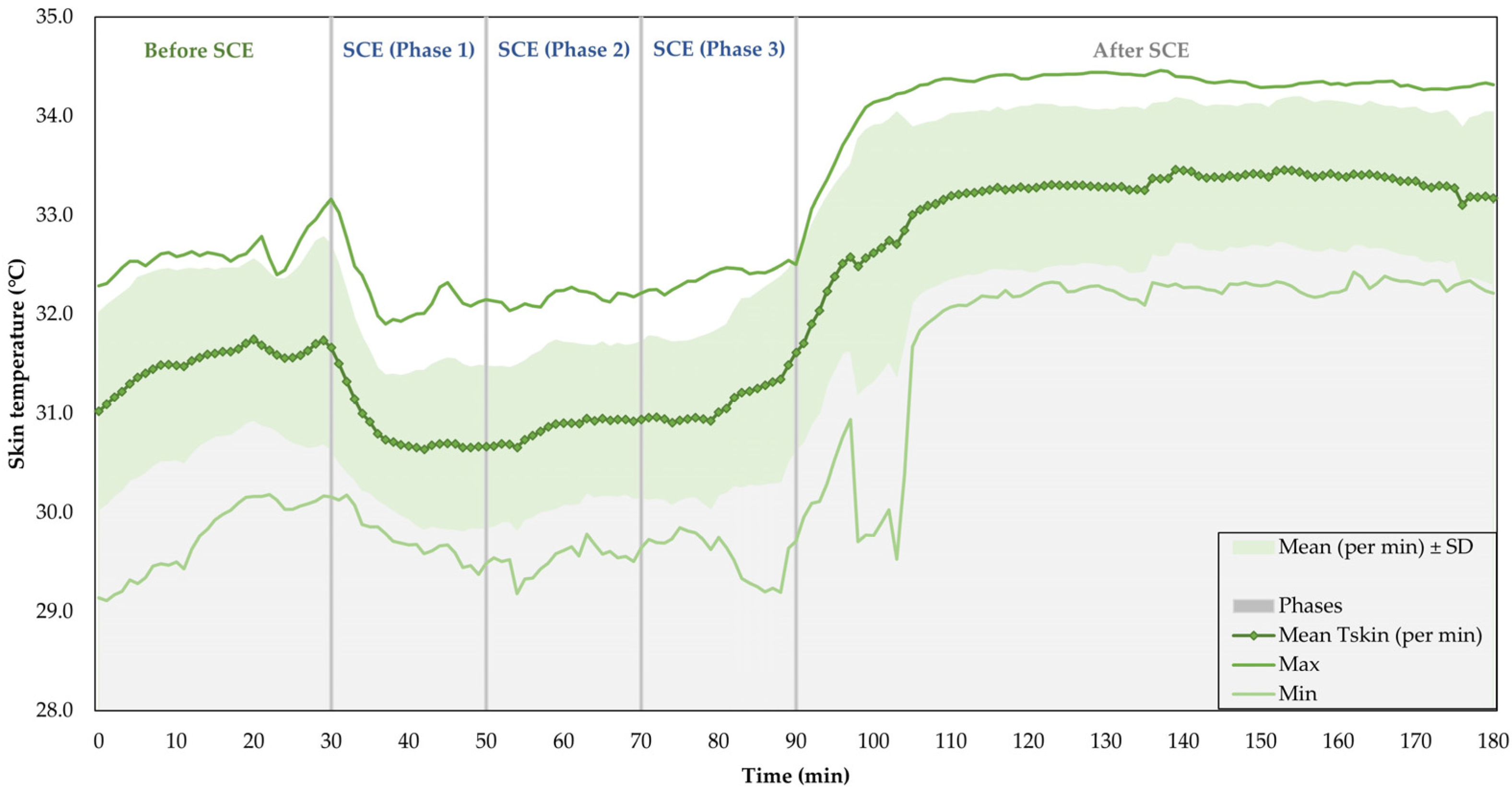
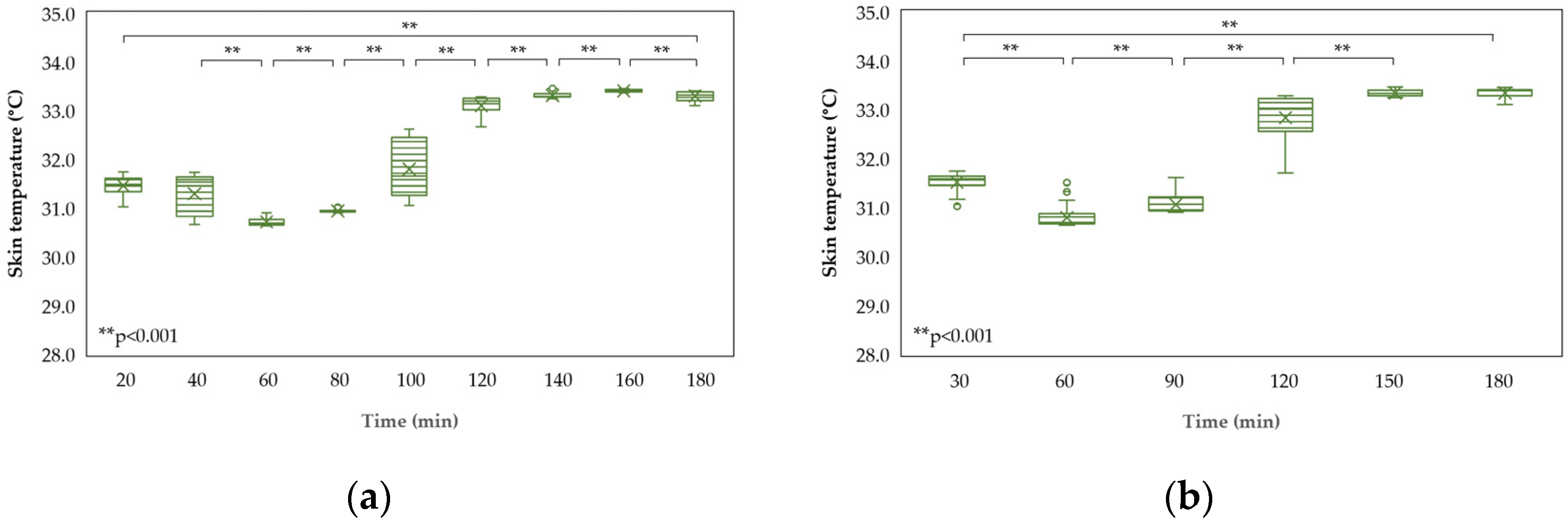
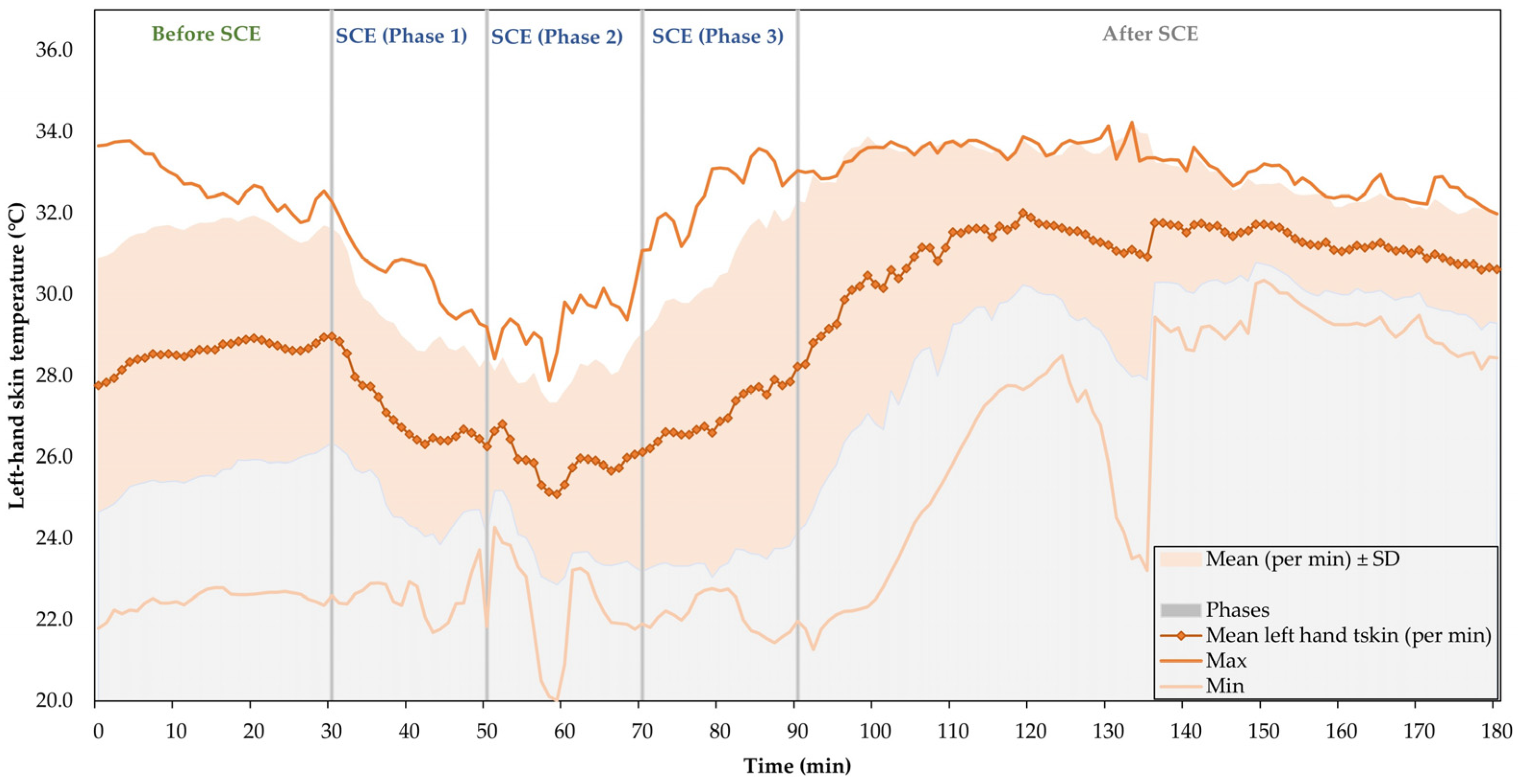
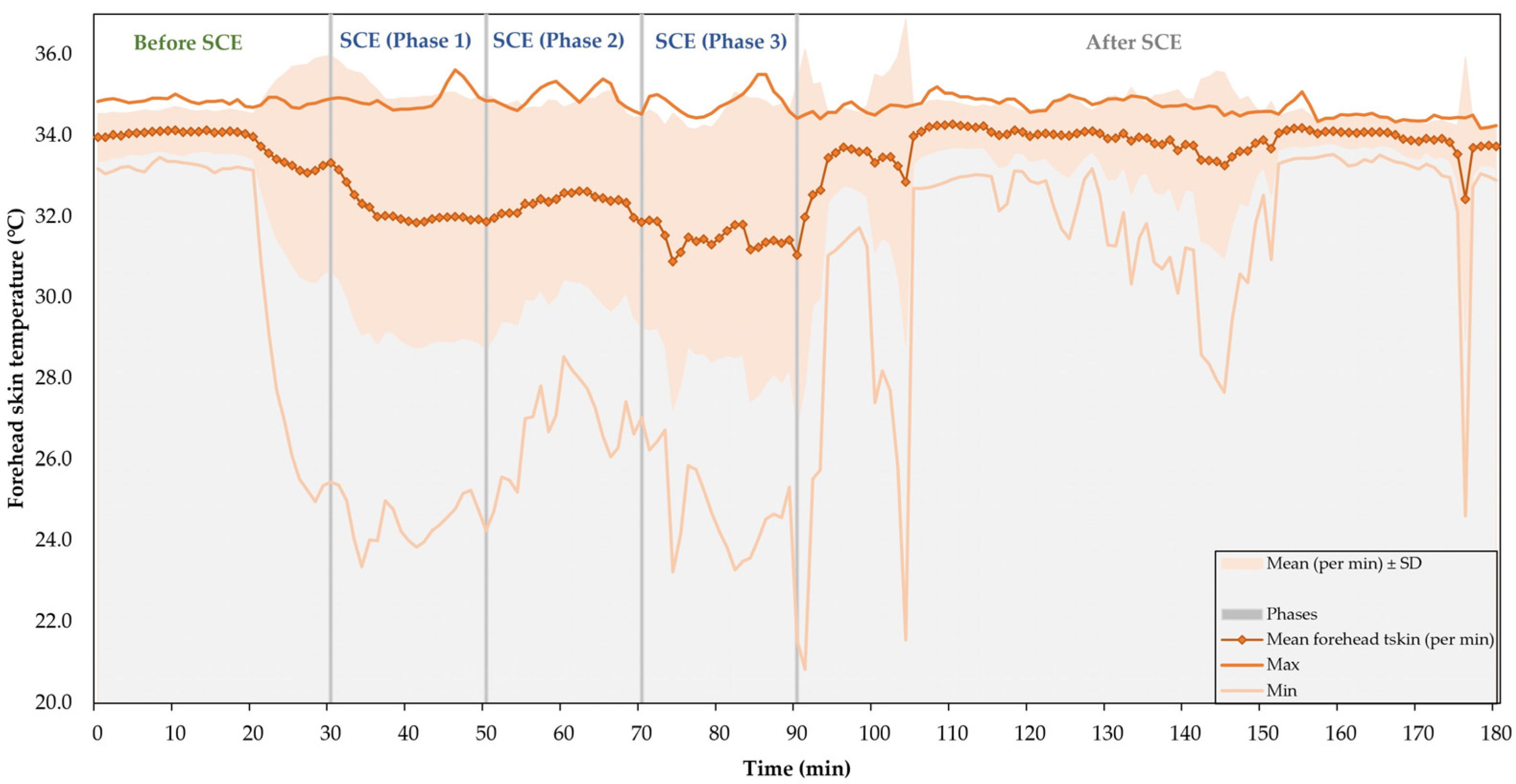
3.2. Skin Temperature
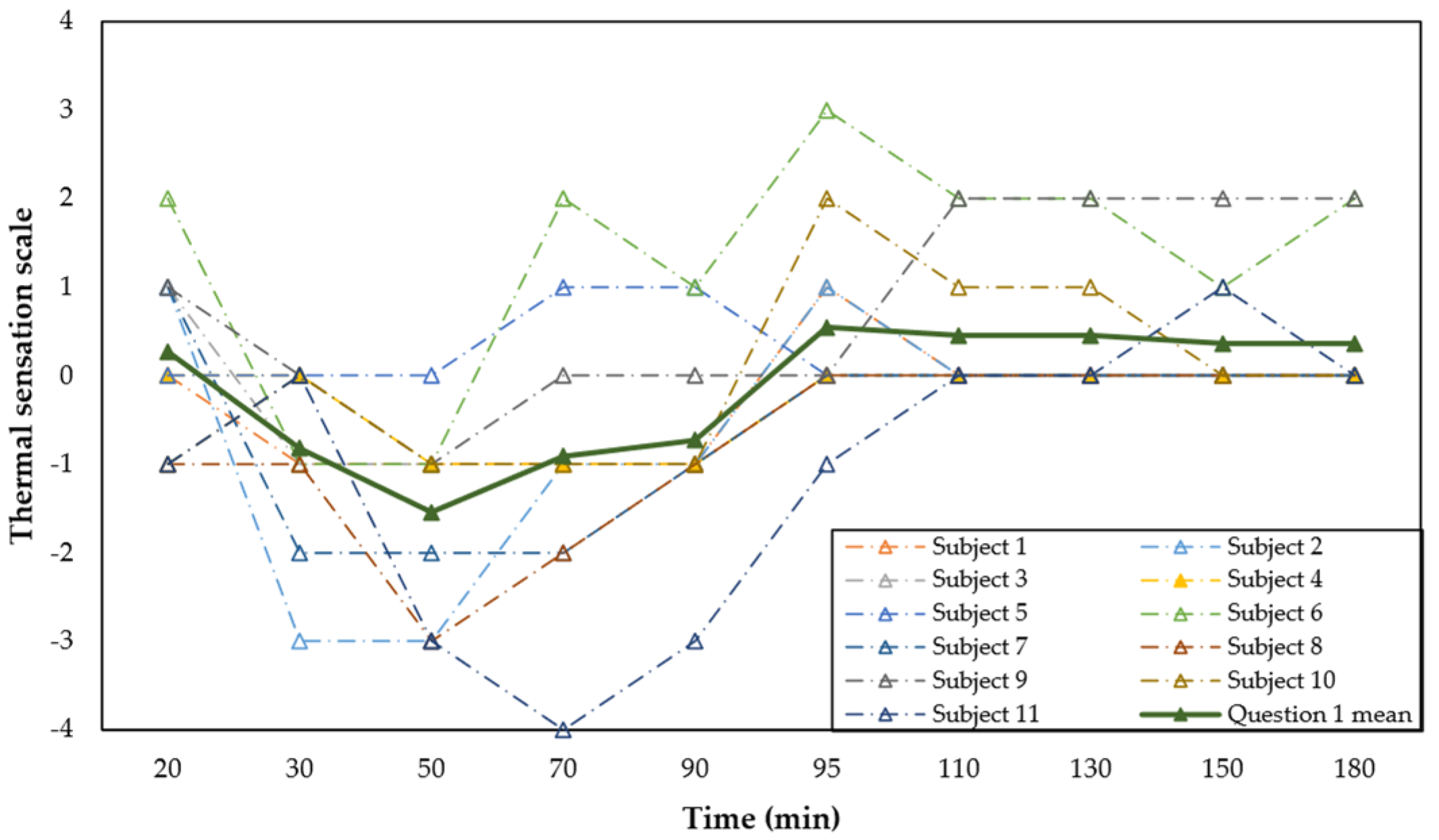
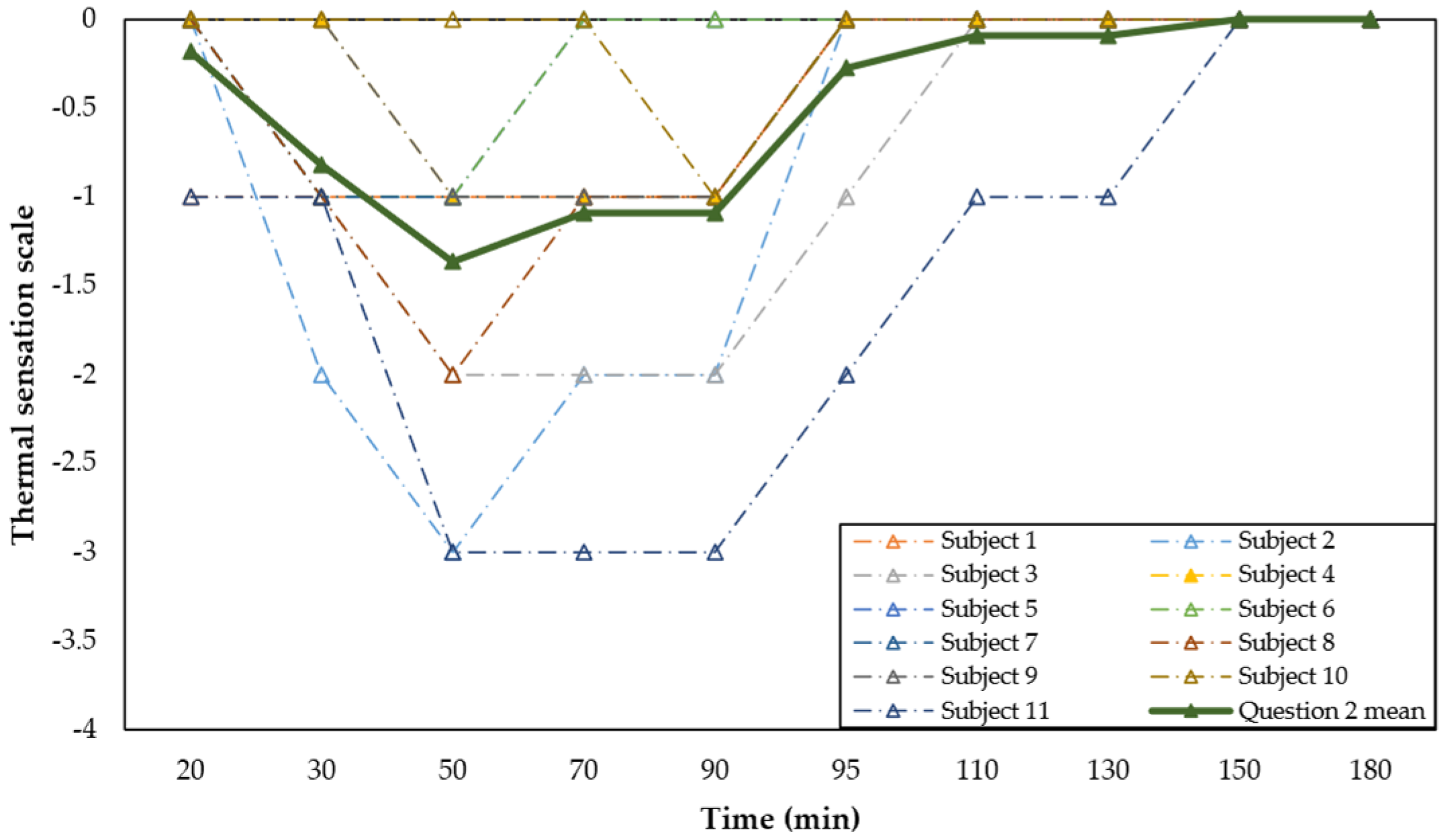
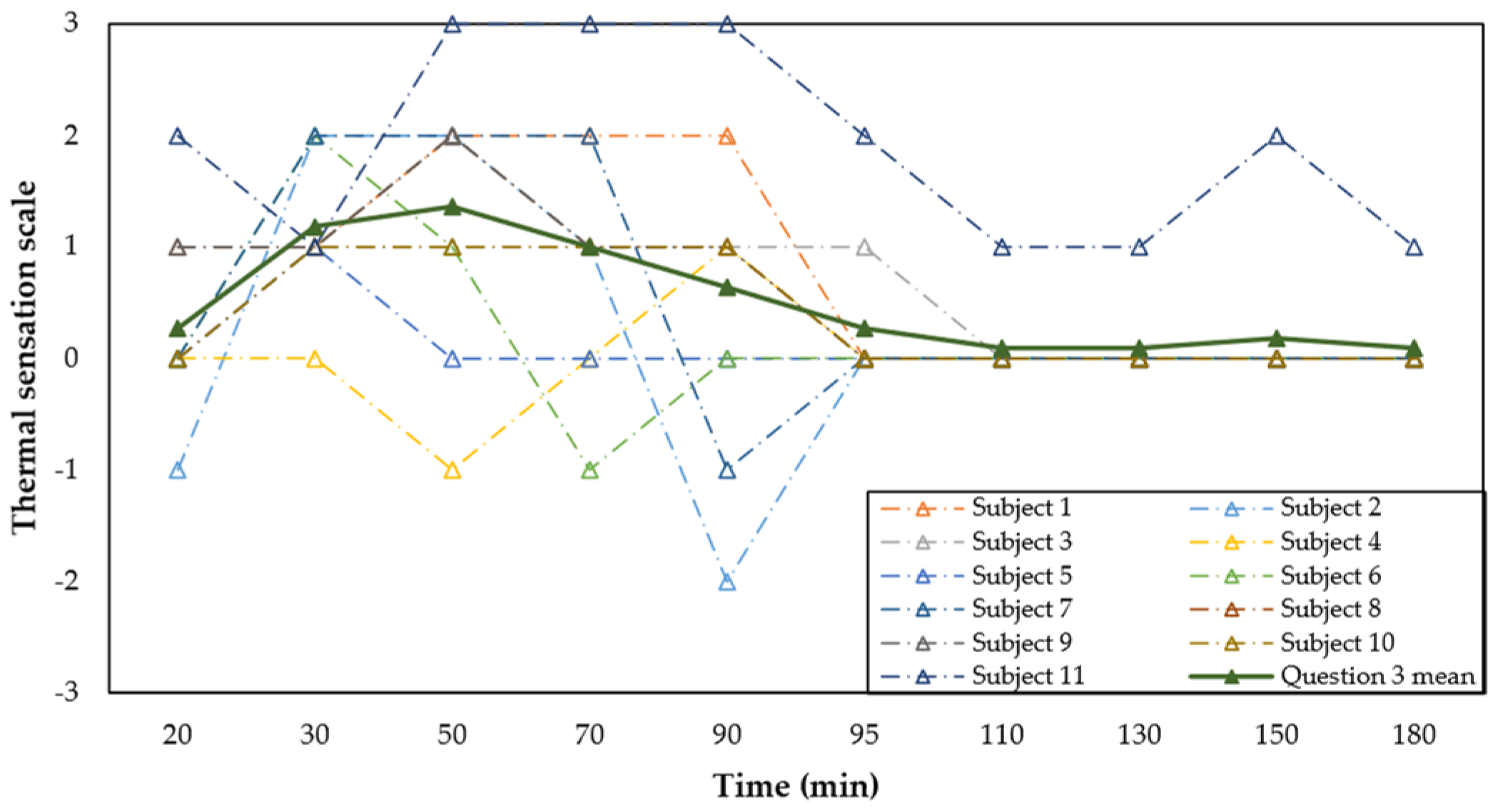
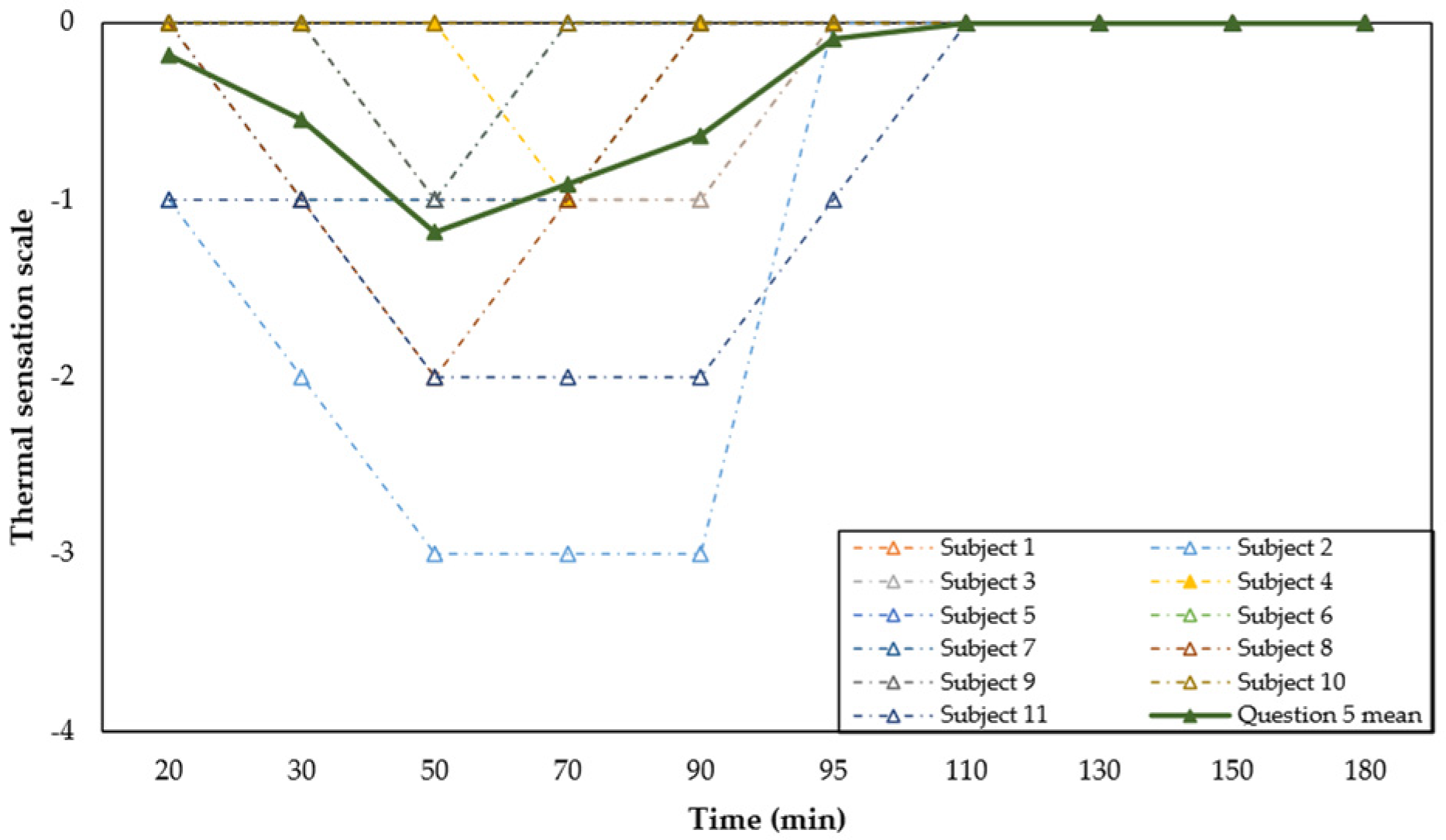
3.3. Thermal Sensation Questionnaire
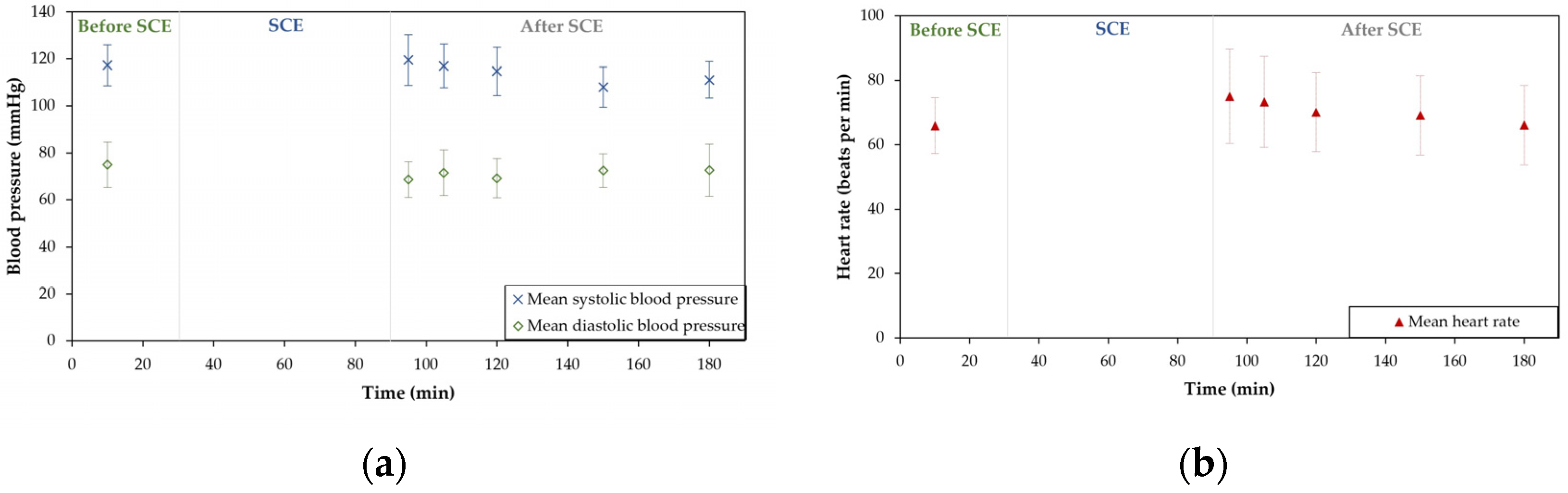
3.4. Blood Pressure
4. Discussion
4.1. Physiological Variations
4.2. Thermal Sensation and Localised Skin Temperature
4.3. Practical Implications for Occupational Settings
4.4. Limitations
5. Conclusions
- The results highlighted the influence of local exposure in evaluating thermal comfort in these conditions. When cold sensation increased, so did pain sensations in the body areas where the skin temperature decreased the most. Consequently, validated TSQ models should be developed to add inquiries addressing thermal sensation on specific body areas, such as those included in this work;
- Exposure to severe cold thermal environments remains a relevant risk factor in working settings. This study demonstrated that preventive measures such as adequate clothing insulation and work–rest pacing are fundamental to diminish its effects;
- Future research should monitor changes in performance during different physical exertion activities controlling oesophageal or intra-abdominal Tcore and Tskin on at least eight body areas (or include points on the extremities: fingers and toes), which can also be of great significance for future thermal comfort models.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ray, M.; King, M.; Carnahan, H. A review of cold exposure and manual performance: Implications for safety, training and performance. Saf. Sci. 2019, 115, 1–11. [Google Scholar] [CrossRef]
- Tochihara, Y. Work in artificial cold environments. J. Physiol. Anthropol. Appl. Hum. Sci. 2005, 24, 73–76. [Google Scholar] [CrossRef] [PubMed]
- D’Amato, M.; Molino, A.; Calabrese, G.; Cecchi, L.; Annesi-Maesano, I.; D’Amato, G. The impact of cold on the respiratory tract and its consequences to respiratory health. Clin. Transl. Allergy 2018, 8, 20. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.S.; Lee, J.K.W.; Oksa, J. Thermal stress, human performance, and physical employment standards. Appl. Physiol. Nutr. Metab. 2016, 41, S148–S164. [Google Scholar] [CrossRef]
- Piedrahita, H.; Oksa, J.; Malm, C.; Rintamäki, H. Health problems related to working in extreme cold conditions indoors. Int. J. Circumpolar Health 2008, 67, 279–287. [Google Scholar] [CrossRef]
- Stjernbrandt, A.; Hoftun Farbu, E. Occupational cold exposure is associated with neck pain, low back pain, and lumbar radiculopathy. Ergonomics 2022, 65, 1276–1285. [Google Scholar] [CrossRef]
- Mäkinen, T.M.; Hassi, J. Health problems in cold work. Ind. Health 2009, 47, 207–220. [Google Scholar] [CrossRef]
- Mäkinen, T.M.; Raatikka, V.-P.; Rytkönen, M.; Jokelainen, J.; Rintamäki, H.; Ruuhela, R.; Näyhä, S.; Hassi, J. Factors affecting outdoor exposure in winter: Population-based study. Int. J. Biometeorol. 2006, 51, 27–36. [Google Scholar] [CrossRef]
- Mäkinen, T.M. Human cold exposure, adaptation, and performance in high latitude environments. Am. J. Hum. Biol. Off. J. Hum. Biol. Assoc. 2007, 19, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xue, P.; Gao, L.; Du, J.; Liu, J. Physiological and thermal response to real-life transient conditions during winter in severe cold area. Build. Environ. 2019, 157, 284–296. [Google Scholar] [CrossRef]
- Gordon, K.; Blondin, D.P.; Friesen, B.J.; Tingelstad, H.C.; Kenny, G.P.; Haman, F. Seven days of cold acclimation substantially reduces shivering intensity and increases nonshivering thermogenesis in adult humans. J. Appl. Physiol. 2019, 126, 1598–1606. [Google Scholar] [CrossRef]
- Sessler, D.I. Thermoregulatory defense mechanisms. Crit. Care Med. 2009, 37, S203–S210. [Google Scholar] [CrossRef]
- Arnold, J.T.; Hemsley, Z.; Hodder, S.G.; Havenith, G.; Lloyd, A.B. Reliability and validity of methods in the assessment of cold-induced shivering thermogenesis. Eur. J. Appl. Physiol. 2020, 120, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Dumont, L.; Lessard, R.; Semeniuk, K.; Chahrour, H.; McCormick, J.J.; Acosta, F.M.; Blondin, D.P.; Haman, F. Thermogenic responses to different clamped skin temperatures in cold-exposed men and women. American Journal of Physiology-Regulatory. Integr. Comp. Physiol. 2022, 323, R149–R160. [Google Scholar] [CrossRef] [PubMed]
- Oksa, J.; Ducharme, M.B.; Rintamaki, H. Combined effect of repetitive work and cold on muscle function and fatigue. J. Appl. Physiol. 2002, 92, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Golmohammadi, R.; Darvishi, E. The combined effects of occupational exposure to noise and other risk factors—A systematic review. Noise Health 2019, 21, 125–141. [Google Scholar] [CrossRef] [PubMed]
- Marzoque, H.J.; Cunha, R.F.d.; Lima, C.M.G.; Nogueira, R.L.; Machado, V.E.d.A.; de Alencar Nääs, I. Work Safety in slaughterhouses: General aspects. Res. Soc. Dev. 2021, 10, e55310111980. [Google Scholar] [CrossRef]
- Raimundo, A.M.; Oliveira, A.V.M.; Gaspar, A.R.; Quintela, D.A. Thermal conditions in freezing chambers and prediction of the thermophysiological responses of workers. Int. J. Biometeorol. 2015, 59, 1623–1632. [Google Scholar] [CrossRef] [PubMed]
- Farbu, E.H.; Skandfer, M.; Nielsen, C.; Brenn, T.; Stubhaug, A.; Höper, A.C. Working in a cold environment, feeling cold at work and chronic pain: A cross-sectional analysis of the Tromsø Study. BMJ Open 2019, 9, e031248. [Google Scholar] [CrossRef]
- Pettersson, H.; Olsson, D.; Järvholm, B. Occupational exposure to noise and cold environment and the risk of death due to myocardial infarction and stroke. Int. Arch. Occup. Environ. Health 2020, 93, 571–575. [Google Scholar] [CrossRef]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Bach, A.J.; Maley, M.J.; Minett, G.M.; Stewart, I.B. Occupational cooling practices of emergency first responders in the United States: A survey. Temperature 2018, 5, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Solanas, È.; López-Ruiz, M.; Wellenius Gregory, A.; Gasparrini, A.; Sunyer, J.; Benavides Fernando, G.; Basagaña, X. Evaluation of the Impact of Ambient Temperatures on Occupational Injuries in Spain. Environ. Health Perspect. 2018, 126, 067002. [Google Scholar] [CrossRef]
- Fu, S.H.; Gasparrini, A.; Rodriguez, P.S.; Jha, P. Mortality attributable to hot and cold ambient temperatures in India: A nationally representative case-crossover study. PLoS Med. 2018, 15, e1002619. [Google Scholar] [CrossRef]
- Wu, J.; Hu, Z.; Han, Z.; Gu, Y.; Yang, L.; Sun, B. Human physiological responses of exposure to extremely cold environments. J. Therm. Biol. 2021, 98, 102933. [Google Scholar] [CrossRef]
- King, M.; Ray, M.; Mulligan, D.; Carnahan, H. Does training in the cold improve cold performance? Int. J. Ind. Ergon. 2020, 76, 102926. [Google Scholar] [CrossRef]
- Li, C.; Wu, J.; Fan, C.; Sun, B.; Hu, Z. Human thermal perception in extremely cold environments: A study of overall and local responses. Energy Build. 2024, 303, 113773. [Google Scholar] [CrossRef]
- Kim, J.-Y.; Jung, K.-Y.; Hong, Y.-S.; Kim, J.-I.; Jang, T.-W.; Kim, J.-M. The relationship between cold exposure and hypertension. J. Occup. Health 2003, 45, 300–306. [Google Scholar] [CrossRef]
- Xiong, J.; Lian, Z.; Zhang, H. Effects of exposure to winter temperature step-changes on human subjective perceptions. Build. Environ. 2016, 107, 226–234. [Google Scholar] [CrossRef]
- Wu, J.; Sun, B.; Hu, Z.; Li, L.; Zhu, H. Physiological responses and thermal sensation during extremely cold exposure (−20 °C). Build. Environ. 2021, 206, 108338. [Google Scholar] [CrossRef]
- Zlatar, T.; Baptista, J.; Costa, J. Physical Working Performance in Cold Thermal Environment: A Short Review. In Occupational Safety and Hygiene III; Taylor & Francis Group: London, UK, 2015; pp. 401–404. [Google Scholar]
- Zlatar, T.; Torres Costa, J.; Vaz, M.; Santos Baptista, J. Influence of severe cold thermal environment on core and skin temperatures: A systematic review. Work 2019, 62, 337–352. [Google Scholar] [CrossRef]
- ISO 9920:2007; Ergonomics of the Thermal Environment–Estimation of Thermal Insulation and Water Vapour Resistance of a Clothing Ensemble. International Organization for Standardization: Geneva, Switzerland, 2007.
- Guedes, J.C.; Costa, E.Q.; Baptista, J.S. Using a Climatic Chamber to Measure the Human Psychophysiological Response under Different Combinations of Temperature and Humidity. Thermol. Int. 2012, 22, 49–54. Available online: http://ww.uhlen.at/thermology-international/archive/EAT2012_Book_of_Proceedings.pdf#page=50 (accessed on 13 December 2023).
- ISO 9886:2004; Ergonomics—Evaluation of Thermal Strain by Physiological Measurements. International Organization for Standardization: Geneva, Switzerland, 2004.
- ISO 7730:2005; Ergonomics of the Thermal Environment. Analytical Determination and Interpretation of Thermal Comfort Using Calculation of the PMV and PPD Indices and Local Thermal Comfort Criteria. CEN (European Committee for Standardization): Geneva, Switzerland, 2005.
- ISO 10551:1993; Assessment of the Influence of the Thermal Environment Using Subjective Judgement Scales. International Standards Organization: Geneva, Switzerland, 1993.
- Ozaki, H.; Nagai, Y.; Tochihara, Y. Physiological responses and manual performance in humans following repeated exposure to severe cold at night. Eur. J. Appl. Physiol. 2001, 84, 343–349. [Google Scholar] [CrossRef]
- Zlatar, T.; Barkokébasb, B., Jr.; Bezerra, L.M.; Araujo Brito, M.M.; Costa, J.T.; Vaz, M.; dos Santos Baptista, J. Safety and health risks for workers exposed to cold thermal environments: A frozen food processing industry perspective. Work 2021, 70, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Mäkinen, T.T.; Gavhed, D.; Holmér, I.; Rintamäki, H. Effects of metabolic rate on thermal responses at different air velocities in −10 °C. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2001, 128, 759–768. [Google Scholar] [CrossRef] [PubMed]
- Charkoudian, N. Mechanisms and modifiers of reflex induced cutaneous vasodilation and vasoconstriction in humans. J. Appl. Physiol. 2010, 109, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Mancia, G.; Kreutz, R.; Bundy, J.D.; Williams, B. Harmonization of the American College of Cardiology/American Heart Association and European Society of Cardiology/European Society of Hypertension blood pressure/hypertension guidelines: Comparisons, reflections, and recommendations. Eur. Heart J. 2022, 43, 3302–3311. [Google Scholar] [CrossRef] [PubMed]
- Brajkovic, D.; Ducharme, M.B. Facial cold-induced vasodilation and skin temperature during exposure to cold wind. Eur. J. Appl. Physiol. 2006, 96, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Gavhed, D.C.E.; Holmér, I. Thermal responses at three low ambient temperatures: Validation of the duration limited exposure index. Int. J. Ind. Ergon. 1998, 21, 465–474. [Google Scholar] [CrossRef]
- Baldus, S.; Kluth, K.; Strasser, H. Order-picking in deep cold—Physiological responses of younger and older females. Part 2: Body core temperature and skin surface temperature. Work 2012, 41, 3010–3017. [Google Scholar] [CrossRef]
- Daanen, H.A.M. Manual Performance Deterioration in the Cold Estimated Using the Wind Chill Equivalent Temperature. Ind. Health 2009, 47, 262–270. [Google Scholar] [CrossRef]
- Kim, T.G.; Tochihara, Y.; Fujita, M.; Hashiguchi, N. Physiological responses and performance of loading work in a severely cold environment. Int. J. Ind. Ergon. 2007, 37, 725–732. [Google Scholar] [CrossRef]
- Kluth, K.; Baldus, S.; Strasser, H. Order-picking in deep cold—Physiological responses of younger and older females. Part 1: Heart rate. Work 2012, 41, 3002–3009. [Google Scholar] [CrossRef] [PubMed]
- Kluth, K.; Penzkofer, M.; Strasser, H. Age-Related Physiological Responses to Working in Deep Cold. Hum. Factors Ergon. Manuf. Serv. Ind. 2013, 23, 163–172. [Google Scholar] [CrossRef]
- Wiggen, Ø.N.; Heen, S.; Revik, H.; Reinertsen, R.E. Effect of Cold Conditions on Manual Performance while Wearing Petroleum Industry Protective Clothing. Ind. Health 2011, 49, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Oksa, J.; Kaikkonen, H.; Sorvisto, P.; Vaappo, M.; Martikkala, V.; Rintamäki, H. Changes in maximal cardiorespiratory capacity and submaximal strain while exercising in cold. J. Therm. Biol. 2004, 29, 815–818. [Google Scholar] [CrossRef]
- Hu, S.; Maeda, T. Productivity and physiological responses during exposure to varying air temperatures and clothing conditions. Indoor Air 2020, 30, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Alshaer, H.; Fernie, G. Blood pressure and thermal responses to repeated whole body cold exposure: Effect of winter clothing. Eur. J. Appl. Physiol. 2009, 107, 673. [Google Scholar] [CrossRef]
- Orysiak, J.; Młynarczyk, M.; Irzmańska, E. The Impact of Protective Gloves on Manual Dexterity in Cold Environments—A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 1637. [Google Scholar] [CrossRef]
- Irzmańska, E.; Wójcik, P.; Adamus-Włodarczyk, A. Manual work in cold environments and its impact on selection of materials for protective gloves based on workplace observations. Appl. Ergon. 2018, 68, 186–196. [Google Scholar] [CrossRef]
- Rintamäki, H.; Rissanen, S.; Mänttäri, S.; Oksa, J.; Jussila, K.; Group, M.R. 392 Low hand temperatures can be a risk factor in arctic surface mining. Inj. Prev. 2016, 22, A143. [Google Scholar] [CrossRef]
- Huizenga, C.; Zhang, H.; Arens, E.; Wang, D. Skin and core temperature response to partial- and whole-body heating and cooling. J. Therm. Biol. 2004, 29, 549–558. [Google Scholar] [CrossRef]
- Arens, E.; Zhang, H.; Huizenga, C. Partial- and whole-body thermal sensation and comfort—Part I: Uniform environmental conditions. J. Therm. Biol. 2006, 31, 53–59. [Google Scholar] [CrossRef]
- Ji, W.; De Dear, R.; Kim, J.; Zhu, Y.; Cao, B.; Liu, S. Study on the influence of climatic thermal exposure environment changed from cold to hot on human thermal preference. Build. Environ. 2022, 207, 108430. [Google Scholar] [CrossRef]
- Imamura, R.; Rissanen, S.; Kinnunen, M.; Rintamäki, H. Manual performance in cold conditions while wearing NBC clothing. Ergonomics 1998, 41, 1421–1432. [Google Scholar] [CrossRef]
- ISO 15743:2008; Ergonomics of the Thermal Environment—Cold Workplaces—Risk Assessment and Management. International Standards Organization: Geneva, Switzerland, 2008. Available online: https://www.iso.org/standard/38895.html (accessed on 13 December 2023).
- Yang, L.; Wu, J.; Hu, Z.; Gao, F.; Hu, X. Effects of workload on human cognitive performance of exposure to extremely cold environment. Physiol. Behav. 2021, 230, 113296. [Google Scholar] [CrossRef]
- Ikäheimo, T.M. Cardiovascular diseases, cold exposure and exercise. Temperature 2018, 5, 123–146. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence | Activity | Duration |
|---|---|---|
| 1 | Answer the TSQ | 4 min |
| 2 | Walk and heat the hands (1 min) | |
| 3 | Put four papers in every box (one by one) | |
| 4 | Close the boxes | |
| 5 | Move each box to shelf 1 | |
| 6 | Rest for 1 min (heat the hands) | |
| 7 | Move each box from shelf 1 to 2 (one by one) | 4 min |
| Rest 5 s (heat the hands) | ||
| 8 | Move each box from shelf 2 to 3 (one by one) | |
| Rest 5 s (heat the hands) | ||
| 9 | Move each box from shelf 3 to 4 (one by one) | |
| Rest 5 s (heat the hands) | ||
| 10 | Move each box from shelf 4 to 5 (one by one) | |
| 11 | Rest for 1 min (heat the hands) | 5 min |
| 12 | Do the game with glass balls ten times | |
| 13 | Rest for 1 min (heat the hands) | |
| 14 | Move each box from shelf 5 to 4 (one by one) | 4 min |
| Rest 5 s (heat the hands) | ||
| 15 | Move each box from shelf 4 to 3 (one by one) | |
| Rest 5 s (heat the hands) | ||
| 16 | Move each box from shelf 3 to 2 (one by one) | |
| Rest 5 s (heat the hands) | ||
| 17 | Move each box from shelf 2 to 1 (one by one) | |
| 18 | Rest for 1 min (heat the hands) | 3 min |
| 19 | Put each box on the table (one by one) | |
| 20 | Open the boxes | |
| 21 | Put four papers from each box to the starting point (one by one) | |
| 22 | Walk and heat the hands (1 min) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zlatar, T.; Bustos, D.; Costa, J.T.; Baptista, J.S.; Guedes, J. Physiological and Thermal Sensation Responses to Severe Cold Exposure (−20 °C). Safety 2024, 10, 19. https://doi.org/10.3390/safety10010019
Zlatar T, Bustos D, Costa JT, Baptista JS, Guedes J. Physiological and Thermal Sensation Responses to Severe Cold Exposure (−20 °C). Safety. 2024; 10(1):19. https://doi.org/10.3390/safety10010019
Chicago/Turabian StyleZlatar, Tomi, Denisse Bustos, José Torres Costa, João Santos Baptista, and Joana Guedes. 2024. "Physiological and Thermal Sensation Responses to Severe Cold Exposure (−20 °C)" Safety 10, no. 1: 19. https://doi.org/10.3390/safety10010019