
Blastomycosis: A Review of Mycological and Clinical Aspects


Abstract
:1. Introduction
2. Epidemiology and Mycology
3. Clinical Manifestations
3.1. Pulmonary Blastomycosis
3.2. Extrapulmonary Manifestations
3.3. Blastomycosis Due to Less Common Species
4. Diagnosis
4.1. Culture
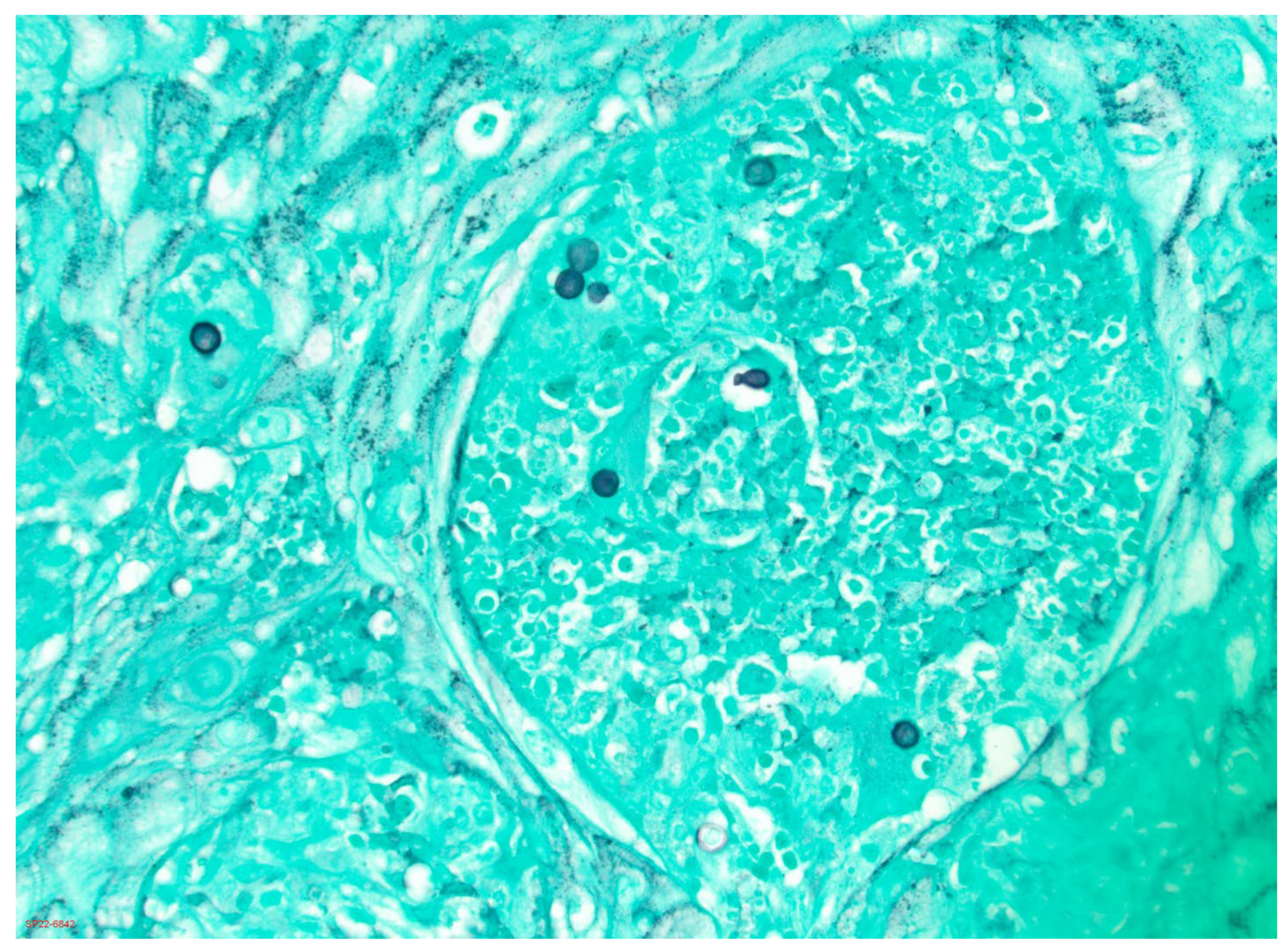
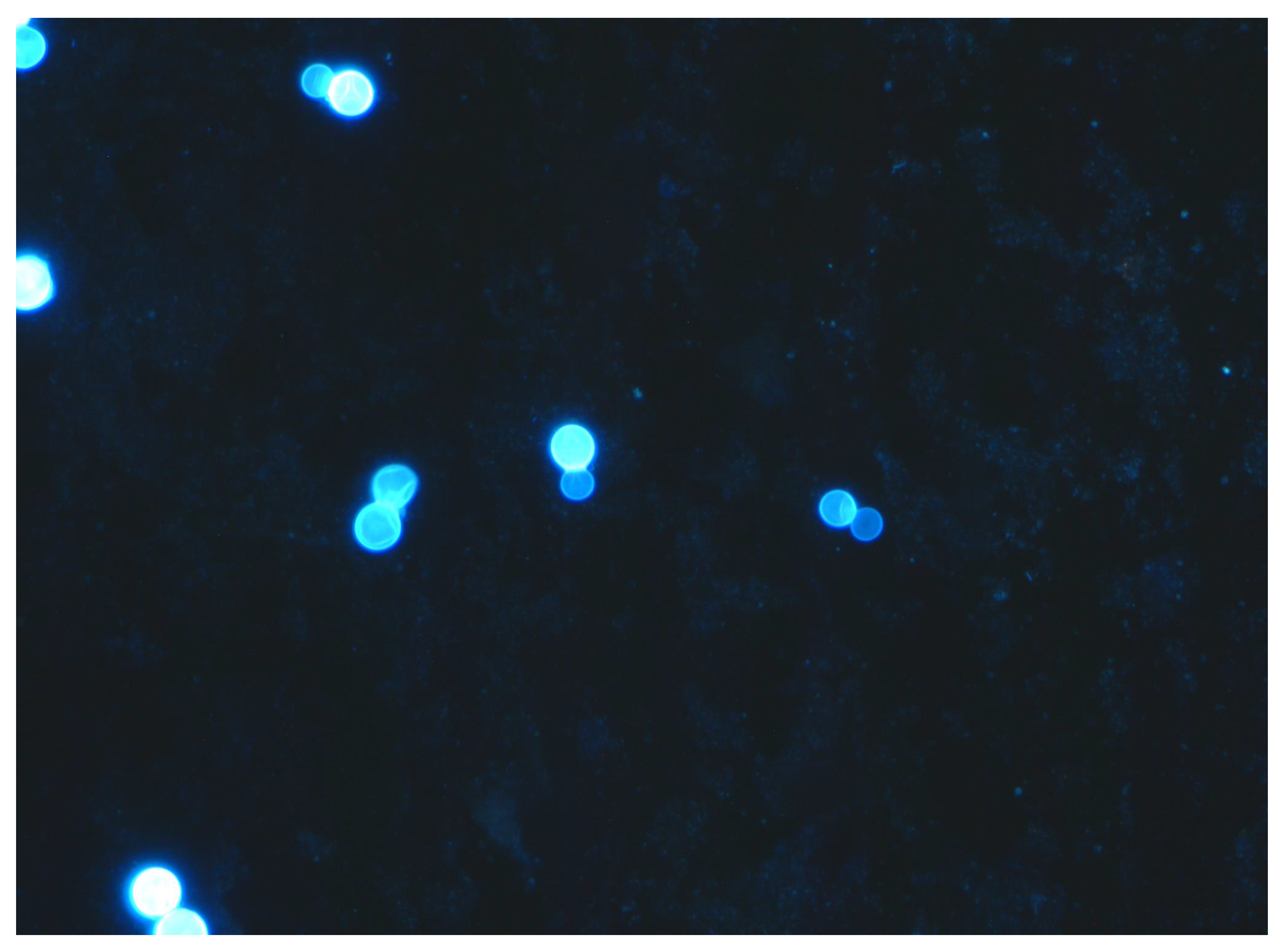
4.2. Histopathology and Cytology
4.3. Antigen Detection
4.4. Antibody Tests
4.5. Nucleic Acid Tests
5. Treatment
5.1. Mild to Moderate Pulmonary or Disseminated Blastomycosis without CNS Involvement
5.2. Moderately Severe to Severe Pulmonary or Disseminated Blastomycosis without CNS Involvement
5.3. Central Nervous System Blastomycosis
5.4. Alternative Antifungal Agents
5.5. Treatment of Blastomycosis in Special Populations
Funding
Conflicts of Interest
References
- Restrepo, A.; Baumgardner, D.J.; Bagagli, E.; Cooper, C.R., Jr.; McGinnis, M.R.; Lazera, M.S.; Barbosa, F.H.; Bosco, S.M.G.; Camargo, Z.P.F.; Coelho, K.I.R.; et al. Clues to the presence of pathogenic fungi in certain environments. Med. Mycol. 2000, 38 (Suppl. 1), 67–77. [Google Scholar] [CrossRef] [Green Version]
- Baumgardner, D.J.; Knavel, E.M.; Steber, D.; Swain, G.R. Geographic distribution of human blastomycosis cases in Milwaukee, Wisconsin, USA: Association with urban watersheds. Mycopathologia 2006, 161, 275–282. [Google Scholar] [CrossRef]
- Klein, B.S.; Vergeront, J.M.; Weeks, R.J.; Kumar, U.; Nanda, U.; Mathai, G.; Varkey, B.; Kaufman, L.; Bradsher, R.; Stoebig, J.F.; et al. Isolation of Blastomyces dermatitidis in soil associated with a large outbreak of blastomycosis in Wisconsin. N. Engl. J. Med. 1986, 314, 529–534. [Google Scholar] [CrossRef]
- Baumgardner, D.J.; Burdick, J.S. An outbreak of human and canine blastomycosis. Rev. Infect. Dis. 1991, 3, 898–905. [Google Scholar] [CrossRef]
- Baumgardner, D.J.; Egan, G.; Giles, S.; Laundre, B. An outbreak of blastomycosis on a United States Indian reservation. Wilderness Environ. Med. 2002, 13, 250–252. [Google Scholar] [CrossRef] [PubMed]
- Pfister, J.R.; Archer, J.R.; Hersil, S.; Boers, T.; Reed, K.D.; Meece, J.K.; Anderson, J.L.; Burgess, J.W.; Sullivan, T.D.; Klein, B.S.; et al. Non-rural point source blastomycosis outbreak near a yard waste collection site. Clin. Med. Res. 2011, 9, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlos, W.G.; Rose, A.S.; Wheat, L.J.; Norris, S.; Sarosi, G.A.; Knox, K.S.; Hage, C.A. Blastomycosis in Indiana: Digging up more cases. Chest 2010, 138, 1377–1382. [Google Scholar] [CrossRef]
- Armstrong, C.W.; Jenkins, S.R.; Kaufman, L.; Kerkering, T.M.; Rouse, B.S.; Miller, G.B., Jr. Common-source outbreak of blastomycosis in hunters and their dogs. J. Infect. Dis. 1987, 155, 568–570. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.; Benedict, K.; Deak, E.; Kirby, M.A.; McNiel, J.T.; Sickler, C.J.; Eckardt, E.; Marx, R.K.; Hefferman, R.T.; Meece, J.K.; et al. A large community outbreak of blastomycosis in Wisconsin with geographic and ethnic clustering. Clin. Infect. Dis. 2013, 57, 655–662. [Google Scholar] [CrossRef]
- Merkhofer, R.M., Jr.; O’Neill, M.B.; Xiong, D.; Hernandez-Santos, N.; Dobson, H.; Fites, J.S.; Shockey, A.C.; Wuethrich, M.; Pepperell, C.S.; Klein, B.S. Investigation of genetic susceptibility to blastomycosis reveals interleukin-6 as a potential susceptibility locus. mBio 2019, 10, e01224-19. [Google Scholar] [CrossRef]
- Anderson, J.L.; Dieckman, J.L.; Reed, D.; Meece, J.K. Canine blastomycosis in Wisconsin: A survey of small animal veterinary practices. Med. Mycol. 2014, 52, 774–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelnutt, L.M.; Kaneene, J.B.; Carneito, P.A.M.; Langlois, D.K. Prevalence, distribution, and risk factors for canine blastomycosis in Michigan, USA. Med. Mycol. 2020, 58, 609–616. [Google Scholar] [CrossRef]
- Jiang, Y.P.; Dukik, K.; Munoz, J.F.; Sigler, L.; Schwartz, I.S.; Govender, N.P.; Kenyon, C.; Feng, P.; van den Ende, B.G.; Stielow, J.B.; et al. Phylogeny, ecology and taxonomy of systemic pathogens and their relatives in Ajellomycetaceae (Onygenales): Blastomyces, Emergomyces, Emmonsia, Emmonsiellopsis. Fungal Divers. 2018, 90, 245–291. [Google Scholar] [CrossRef] [Green Version]
- Brown, E.M.; McTaggart, L.R.; Zhang, S.X.; Low, D.E.; Stevens, D.A.; Richardson, S.E. Phylogenetic analysis reveals a cryptic species Blastomyces gilchristii sp. nov. within the human pathogenic fungus Blastomyces dermatitidis. PLoS ONE 2013, 8, e59237. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, I.S.; Munoz, J.F.; Kenyon, C.R.; Govender, N.P.; McTaggart, L.; Maphanga, T.G.; Richardson, S.; Becker, P.; Cuomo, C.A.; McEwen, J.G.; et al. Blastomycosis in Africa and the Middle East: A comprehensive review of reported cases and reanalysis of historical isolates based on molecular data. Clin. Infect. Dis. 2021, 73, e1560–e1569. [Google Scholar] [CrossRef] [PubMed]
- Maphanga, T.G.; Birkhead, M.; Munoz, J.F.; Allam, M.; Zulu, T.G.; Cuomo, C.A.; Schwartz, I.S.; Ismail, A.; Naicker, S.D.; Mpembe, R.S.; et al. Human blastomycosis in South Africa caused by Blastomyces percursus and Blastomyces emzantsi sp. nov., 1967 to 2014. J. Clin. Microbiol. 2020, 58, e01661-19. [Google Scholar] [CrossRef]
- Sekhon, A.S.; Jackson, F.L.; Jacobs, H.J. Blastomycosis: Report of the first case from Alberta, Canada. Mycopathologia 1982, 79, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.S.; Wiederhold, N.P.; Hanson, K.E.; Patterson, T.F.; Sigler, L. Blastomyces helicus, a new dimorphic fungus causing fatal pulmonary and systemic disease in humans and animals in western Canada and the United States. Clin. Infect. Dis. 2019, 68, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, I.S.; Kenyon, C.; Feng, P.; Govender, N.P.; Gukik, K.; Sigler, L.; Jiang, Y.; Stielow, J.B.; Munoz, J.F.; Cuomo, C.A.; et al. 50 years of Emmonsia disease in humans: The dramatic emergence of a cluster of novel fungal pathogens. PLoS Pathog. 2015, 11, e1005198. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, I.S.; Kauffman, C.A. Blastomycosis. Semin. Respir. Crit. Care Med. 2020, 41, 31–41. [Google Scholar]
- Anderson, J.L.; Meece, J.K.; Hall, M.C.; Frost, H.M. Evidence of delayed dissemination or re-infection with Blastomyces in two immunocompetent hosts. Med. Mycol. Case Rep. 2016, 13, 9–11. [Google Scholar] [CrossRef]
- Bethuel, N.W.; Siddiqui, N.; Edmonds, L. Pulmonary blastomycosis in rural Upstate New York: A case series and review of literature. Ann. Thorac. Med. 2020, 15, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.W.; Lin, A.C.; Hendricks, K.A.; Nolan, R.L.; Currier, M.M.; Morris, K.R.; Turner, H.R. Endemic blastomycosis in Mississippi: Epidemiological and clinical studies. Semin. Respir. Infect. 1997, 12, 219–228. [Google Scholar] [PubMed]
- Baumgardner, D.J.; Halsmer, S.E.; Egan, G. Symptoms of pulmonary blastomycosis: Northern Wisconsin, United States. Wilderness Environ. Med. 2004, 15, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronald, S.; Strzelcyzk, J.; Moore, S.; Trepman, E.; Cheang, M.; Limerick, B.; Wiebe, L.; Sarsfield, P.; Macdonald, K.; Meyers, M.; et al. Computed tomographic scan evaluation of pulmonary blastomycosis. Can. J. Infect. Dis. Med. Microbiol. 2009, 20, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Maini, R.; Ranjha, S.; Tandan, N.; Regmi, M.R.; Ullah, S.; Stone, T.; Nayeemuddin, F.; Pervin, N. Pulmonary blastomycosis: A case series and review of unique radiological findings. Med. Mycol. Case Rep. 2020, 28, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.S.; Embil, J.M.; Sharma, A.; Goulet, S.; Light, R.B. Management and outcomes of acute respiratory distress syndrome caused by blastomycosis. Medicine 2016, 95, e3538. [Google Scholar] [CrossRef]
- Meyer, K.C.; McManus, E.J.; Maki, D.G. Overwhelming pulmonary blastomycosis associated with the adult respiratory distress syndrome. N. Engl. J. Med. 1993, 329, 1231–1236. [Google Scholar] [CrossRef]
- Rush, B.; Lother, S.; Paunovic, B.; Mooney, O.; Kumar, A. Outcomes with severe blastomycosis and respiratory failure in the United States. Clin. Infect. Dis. 2021, 72, 1603–1607. [Google Scholar] [CrossRef]
- Smith, J.A.; Riddell, J., IV; Kauffman, C.A. Cutaneous manifestations of endemic mycoses. Curr. Infect. Dis. Rep. 2013, 15, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Ladizinski, B.; Joy, N.; Reid, D.C. Primary cutaneous blastomycosis after inoculation from a woodworking blade. J. Emerg. Med. 2018, 54, e11–e12. [Google Scholar] [CrossRef] [PubMed]
- Gray, N.A.; Baddour, L.M. Cutaneous inoculation blastomycosis. Clin. Infect. Dis. 2002, 34, 44–49. [Google Scholar] [CrossRef]
- Rammaert, B.; Gamaletsou, M.N.; Zeller, V.; Elie, C.; Prinaopri, R.; Taj-Aldeen, S.J.; Roilides, E.; Kontoyiannis, D.P.; Brause, B.; Sipsas, N.V.; et al. Dimorphic fungal osteoarticular infections. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 2131–2140. [Google Scholar] [CrossRef] [PubMed]
- Kouba, S.; Kobayashi, T.; Meier, J.; Sekar, P. Osseous blastomycosis mimicking malignancy. BMJ Case Rep. 2020, 13, e237688. [Google Scholar] [CrossRef] [PubMed]
- Gamaletsou, M.N.; Rammaert, B.; Brause, B.; Bueno, M.A.; Dadwal, S.S.; Henry, M.W.; Katragkou, A.; Kontoyiannis, D.P.; McCarthy, M.W.; Miller, A.O.; et al. International Consortium for Osteoarticular Mycoses. Osteoarticular mycoses. Clin. Microbiol. Rev. 2022, 35, e0008619. [Google Scholar] [CrossRef]
- Kauffman, C.A. Central nervous system infection with other endemic mycoses: Rare manifestation of blastomycosis, paracoccidioidomycosis, talaromycosis, and sporotrichosis. J. Fungi 2019, 5, 64. [Google Scholar] [CrossRef] [Green Version]
- Bradsher, R.W.; Bariola, J.R. Blastomycosis. In Essentials of Clinical Mycology, 2nd ed.; Kauffman, C.A., Pappas, P.G., Sobel, J.D., Dismukes, W.E., Eds.; Springer: New York, NY, USA, 2011; pp. 337–348. [Google Scholar]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and update of the consensus definitions of invasive fungal disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saccente, M.; Woods, G.L. Clinical and laboratory update on blastomycosis. Clin. Microbiol. Rev. 2010, 23, 367–381. [Google Scholar] [CrossRef] [Green Version]
- Martynowicz, M.A.; Prakash, U.B. Pulmonary blastomycosis: An appraisal of diagnostic techniques. Chest 2002, 121, 768–773. [Google Scholar] [CrossRef] [Green Version]
- Padhye, A.A.; Smith, G.; Standard, P.G.; McLaughlin, D.; Kaufman, L. Comparative evaluation of chemiluminescent DNA probe assays and exoantigen tests for rapid identification of Blastomyces dermatitidis and Coccidioides immitis. J. Clin. Microbiol. 1994, 32, 867–870. [Google Scholar] [CrossRef] [Green Version]
- Durkin, M.; Witt, J.; Lemonte, A.; Wheat, B.; Connolly, P. Antigen assay with the potential to aid in diagnosis of blastomycosis. J. Clin. Microbiol. 2004, 42, 4873–4875. [Google Scholar] [CrossRef]
- Connolly, P.; Hage, C.A.; Bariola, J.R.; Bensadoun, E.; Rodgers, M.; Bradsher, R.W.; Wheat, L.J. Blastomyces dermatitidis antigen detection by quantitative enzyme immunoassay. Clin. Vacc. Immunol. 2012, 19, 53–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hage, C.A.; Knox, K.S.; Davis, T.E.; Wheat, L.J. Antigen detection in bronchoalveolar lavage fluid for diagnosis of fungal pneumonia. Curr. Opin. Pulm. Med. 2011, 17, 167–171. [Google Scholar] [CrossRef]
- Hage, C.A.; Davis, T.E.; Egan, L.; Parker, M.; Fuller, D.; LeMonte, A.M.; Durkin, M.; Connelly, P.; Wheat, L.J.; Blue-Hnidy, D.; et al. Diagnosis of pulmonary histoplasmosis and blastomycosis by detection of antigen in bronchoalveolar lavage fluid using an improved second-generation enzyme-linked immunoassay. Respir. Med. 2007, 101, 43–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bariola, J.R.; Perry, P.; Pappas, P.G.; Proia, L.; Shealey, W.; Wright, P.W.; Sizemore, J.M.; Robinson, M.; Bradsher, R.W., Jr. Blastomycosis of the central nervous system: A multicenter review of diagnosis and treatment in the modern era. Clin. Infect. Dis. 2010, 50, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bariola, J.R.; Hage, C.A.; Durkin, M.; Bensadoun, E.; Gubbins, P.O.; Wheat, L.J.; Bradsher, R.W., Jr. Detection of Blastomyces dermatitidis antigen in patients with newly diagnosed blastomycosis. Diagn. Microbiol. Infect. Dis. 2011, 69, 187–191. [Google Scholar] [CrossRef]
- Frost, H.M.; Novicki, T.J. Blastomyces antigen detection for diagnosis and management of blastomycosis. J. Clin. Microbiol. 2015, 53, 3660–3662. [Google Scholar] [CrossRef] [Green Version]
- Van Der Veer, J.; Lewis, R.J.; Emtiazjoo, A.M.; Allen, S.D.; Wheat, L.J.; Hage, C.A. Cross-reactivity in the Platelia Aspergillus enzyme immunoassay caused by blastomycosis. Med. Mycol. 2012, 50, 396–398. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.R.; Jamison, G.R.; Boudreaux, J.W.; Howles, M.J.; Walsh, T.J.; Hayden, R.T. Cross-reactivity of non-Aspergillus fungal species in the Aspergillus galactomannan enzyme immunoassay. Diagn. Microbiol. Infect. Dis. 2007, 59, 113–115. [Google Scholar] [CrossRef]
- Tarr, M.; Marcinek, J.; Mongkolrattanothai, K.; Burns, J.L.; Wheat, L.J.; Durkin, M.; Ismail, M. Blastomyces antigen detection for monitoring progression of blastomycosis in a pregnant adolescent. Infect. Dis. Obstet. Gynecol. 2007, 2007, 89059. [Google Scholar] [CrossRef]
- Mongkolrattanothai, K.; Peev, M.; Wheat, L.J.; Marcinak, J. Urine antigen detection of blastomycosis in pediatric patients. Ped. Infect. Dis. J. 2006, 25, 1076–1078. [Google Scholar] [CrossRef]
- Foy, D.S.; Trepanier, L.A.; Kirsch, E.J.; Wheat, L.J. Serum and urine Blastomyces antigen concentrations as markers of clinical remission in dogs treated for systemic blastomycosis. J. Vet. Intern. Med. 2014, 28, 305–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, B.S.; Vergeront, J.M.; Kaufman, L.; Bradsher, R.W.; Kumar, U.N.; Mathai, G.; Varkey, B.; Davis, J.P. Serological tests for blastomycosis: Assessments during a large point-source outbreak in Wisconsin. J. Infect. Dis. 1987, 155, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Soufleris, A.J.; Klein, B.S.; Courtney, B.T.; Proctor, M.E.; Jones, J.M. Utility of anti-WI-1 serological testing in the diagnosis of blastomycosis in Wisconsin residents. Clin. Infect. Dis. 1994, 19, 87–92. [Google Scholar] [CrossRef]
- Klein, B.S.; Jones, J.M. Isolation, purification, and radiolabeling of a novel 120-kD surface protein on Blastomyces dermatitidis yeasts to detect antibody in infected patients. J. Clin. Investig. 1990, 85, 152–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richer, S.M.; Smedema, M.L.; Durkin, M.M.; Brandhorst, T.T.; Hage, C.A.; Connolly, P.A.; Leland, D.S.; Davis, T.E.; Klein, B.S.; Wheat, L.J. Development of a highly sensitive and specific blastomycosis antibody enzyme immunoassay using Blastomyces dermatitidis surface protein BAD-1. Clin. Vacc. Immunol. 2014, 21, 143–146. [Google Scholar] [CrossRef] [Green Version]
- Mourning, A.C.; Patterson, E.E.; Kirsch, E.J.; Renschler, J.S.; Wolf, L.A.; Paris, J.K.; Durkin, M.M.; Wheat, L.J. Evaluation of an enzyme immunoassay for antibodies to a recombinant Blastomyces adhesin-1 repeat antigen as an aid in the diagnosis of blastomycosis in dogs. JAVMA 2015, 247, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, M.; Zhu, Y.; Kus, J.V.; McTaggart, L.; Chaturvedi, V.; Chaturvedi, S. Development of a duplex real-time PCR assay for the differentiation of Blastomyces dermatitidis and Blastomyces gilchristii and a retrospective analysis of culture and primary specimens from blastomycosis cases from New York (2005–2019). J. Clin. Microbiol. 2021, 59, 02078-20. [Google Scholar] [CrossRef]
- Sidamonidze, K.; Peck, M.K.; Perez, M.; Baumgardner, D.; Smith, G.; Chaturvedi, V.; Chaturvedi, S. Real-time PCR assay for identification of Blastomyces dermatitidis in culture and in tissue. J. Clin. Microbiol. 2012, 50, 1783–1786. [Google Scholar] [CrossRef] [Green Version]
- Bialek, R.; Cicera, A.C.; Herrmann, T.; Apenus, C.; Shearn-Bochsler, V.A.; Legendre, A.M. Nested PCR assays for detection of Blastomyces dermatitidis DNA in paraffin-embedded canine tissue. J. Clin. Microbiol. 2003, 41, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Burgess, J.W.; Schwan, W.R.; Volk, T.J. PCR-based detection of DNA from the human pathogen Blastomyces dermatitidis from natural soil samples. Med. Mycol. 2006, 44, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Babady, N.E.; Buckwalter, S.P.; Hall, L.; Le Febre, K.M.; Binnicker, M.J.; Wengenack, N.L. Detection of Blastomyces dermatitidis and Histoplasma capsulatum from culture isolates and clinical specimens by use of real-time PCR. J. Clin. Microbiol. 2011, 49, 3204–3208. [Google Scholar] [CrossRef] [Green Version]
- Chapman, S.W.; Dismukes, W.E.; Proia, L.A.; Bradsher, R.W.; Pappas, P.G.; Threlkeld, M.G.; Kauffman, C.A. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 1801–1812. [Google Scholar] [CrossRef] [PubMed]
- Dismukes, W.E.; Bradsher, R.W.; Cloud, G.C.; Kauffman, C.A.; Chapman, S.W.; George, R.B.; Stevens, D.A.; Girard, W.M.; Saag, M.S.; Bowles-Patton, C.; et al. Itraconazole therapy for blastomycosis and histoplasmosis. Am. J. Med. 1992, 9, 489–497. [Google Scholar] [CrossRef]
- Lestner, J.M.; Roberts, S.A.; Moore, C.B.; Howard, S.J.; Denning, D.W.; Hope, W.W. Toxicodynamics of itraconazole: Implications for therapeutic drug monitoring. Clin. Infect. Dis. 2009, 49, 928–930. [Google Scholar] [CrossRef]
- Lahm, T.; Neese, S.; Thornburg, A.T.; Ober, M.D.; Sarosi, G.A.; Hage, C.A. Corticosteroids for blastomycosis-induced ARDS: A report of two patients and review of the literature. Chest 2008, 133, 1478–1480. [Google Scholar] [CrossRef] [PubMed]
- Plamondon, M.; Lamontagne, F.; Allard, C.; Pepin, J. Corticosteroids as adjunctive therapy in severe blastomycosis-induced acute respiratory distress syndrome in an immunosuppressed patient. Clin. Infect. Dis. 2010, 51, e1–e3. [Google Scholar] [CrossRef] [Green Version]
- Dalton, H.J.; Hertzog, J.H.; Hannan, R.L.; Vezza, P.; Hauser, G.J. Extracorporeal membrane oxygenation for overwhelming Blastomyces dermatitidis pneumonia. Crit. Care 1999, 3, 91–94. [Google Scholar] [CrossRef] [Green Version]
- Bednarczyk, J.M.; Kethireddy, S.; White, C.W.; Freed, D.H.; Singal, R.K.; Bell, D.; Ahmed, S.Z.; Kumar, A.; Light, B. Extracorporeal membrane oxygenation for blastomycosis-related acute respiratory distress syndrome: A case series. Can. J. Anaesth. 2015, 62, 807–815. [Google Scholar] [CrossRef] [Green Version]
- Al-Fares, A.; Fan, E.; Husain, S.; Di Nardo, M.; Cypel, M.; Keshavjee, S.; Herridge, M.S.; Del Sorbo, L. Veno-venous extracorporeal life support for blastomycosis-associated acute respiratory distress syndrome. Perfusion 2019, 34, 660–670. [Google Scholar] [CrossRef]
- Agarwal, A.; Losie, J.A.; Kain, D.; Kaul, R. Blastomycosis with rapid-onset acute respiratory distress syndrome in an urban setting. BMJ Case Rep. 2021, 14, e239498. [Google Scholar] [CrossRef] [PubMed]
- Branick, K.; Taylor, M.J.; Trump, M.W.; Wall, G.C. Apparent interference with extracorporeal membrane oxygenation by liposomal amphotericin B in a patient with disseminated blastomycosis receiving continuous renal replacement therapy. Am. J. Health Syst. Pharm. 2019, 76, 810–813. [Google Scholar] [CrossRef]
- Henry, M.E.; Bolo, N.R.; Zuo, C.S.; Villafuerte, R.A.; Cayetano, K.; Glue, P.; Damle, B.D.; Andrews, E.; Lauriat, T.L.; Rana, N.S.; et al. Quantification of brain voriconazole levels in healthy adults using fluorine magnetic resonance spectroscopy. Antimicrob. Agents Chemother. 2013, 57, 5271–5276. [Google Scholar] [CrossRef] [Green Version]
- Ta, M.; Flowers, S.A.; Rogers, P.D. The role of voriconazole in the treatment of central nervous system blastomycosis. Ann. Pharmacother. 2009, 43, 1696–1700. [Google Scholar] [CrossRef]
- Borgia, S.M.; Fuller, J.D.; Sarabia, A.; El-Helou, P. Cerebral blastomycosis: A case series incorporating voriconazole in the treatment regimen. Med. Mycol. 2006, 44, 659–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pappas, P.G.; Spec, A.; Miceli, M.H.; Proia, L.; Arauz, A.B.; Hayes, J.; Peinhardt, A.; McMullen, R.; Moore, M.K.; McGwin, G.; et al. MSG-15: Pharmacokinetic, adverse events, and tolerability data from an open label randomized clinical trial comparing oral suba-itraconazole to conventional itraconazole for treatment of endemic mycosis. Open Forum Infect. Dis. 2020, 7 (Suppl. 1), S202–S203. [Google Scholar] [CrossRef]
- Pappas, P.G.; Bradsher, R.W.; Chapman, S.W.; Kauffman, C.A.; Dine, A.; Cloud, G.A.; Dismukes, W.E. Treatment of blastomycosis with fluconazole: A pilot study. Clin. Infect. Dis. 1995, 20, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Bradsher, R.W.; Kauffman, C.A.; Cloud, G.A.; Thomas, C.J.; Campbell, G.D., Jr.; Chapman, S.W.; Newman, C.; Dismukes, W.E. Treatment of blastomycosis with higher doses of fluconazole. Clin. Infect. Dis. 1997, 25, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Stott, K.E.; Beardsley, J.; Kolamunnage-Dona, R.; Castelazo, A.S.; Kibengo, F.M.; Mai, N.T.H.; Tùng, N.L.N.; Cuc, N.T.K.; Day, J.; Hope, W. Population pharmacokinetics and cerebrospinal fluid penetration of fluconazole in adults with cryptococcal meningitis. Antimicrob. Agents Chemother. 2018, 62, e00885-18. [Google Scholar] [CrossRef] [Green Version]
- Freifeld, A.; Proia, L.; Andes, D.; Baddour, L.M.; Blair, J.; Spellberg, B.; Arnold, S.; Lentnek, A.; Wheat, L.J. Voriconazole use for endemic fungal infections. Antimicrob. Agents Chemother. 2009, 53, 1648–1651. [Google Scholar] [CrossRef] [Green Version]
- Pascual, A.; Calandra, T.; Bolay, S.; Buclin, T.; Bille, J.; Marchetti, O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin. Infect. Dis. 2008, 46, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Proia, L.A.; Harnisch, D.O. Successful use of posaconazole for treatment of blastomycosis. Antimicrob. Agents Chemother. 2012, 56, 4029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauffman, C.A. Treatment of the midwestern endemic mycoses, blastomycosis and histoplasmosis. Curr. Fungal Infect. Rep. 2017, 11, 67–74. [Google Scholar] [CrossRef]
- Chen, L.; Krekels, E.H.J.; Verweij, P.E.; Buil, J.B.; Knibbe, C.A.J.; Brüggemann, R.J.M. Pharmacokinetics and pharmacodynamics of posaconazole. Drugs 2020, 80, 671–695. [Google Scholar] [CrossRef] [Green Version]
- Gross, B.N.; Ihorst, G.; Jung, M.; Wasch, R.; Engelhardt, M. Posaconazole therapeutic drug monitoring in the real-life setting: A single-center experience and review of the literature. Pharmacotherapy 2013, 33, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Rendon, A.; Ribeiro Dos Santos, R.; Queiroz-Telles, F.; Ostrosky-Zeichner, L.; Azie, N.; Maher, R.; Lee, M.; Kovanda, L.; Engelhardt, M.; et al. Isavuconazole treatment of cryptococcosis and dimorphic mycoses. Clin. Infect. Dis. 2016, 63, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Lewis, J.S., II; Wiederhold, N.P.; Hakki, M.; Thompson, G.R., III. New perspectives on antimicrobial agents: Isavuconazole. Antimicrob. Agents Chemother. 2022, 66, e0017722. [Google Scholar] [CrossRef]
- Wiederhold, N.P. Review of the novel investigational antifungal Olorofim. J. Fungi 2020, 6, 122. [Google Scholar] [CrossRef]
- Pappas, P.G.; Threlkeld, M.G.; Bedsole, G.D.; Cleveland, K.O.; Gelfand, M.S.; Dismukes, W.E. Blastomycosis in immunocompromised patients. Medicine 1993, 72, 311–325. [Google Scholar] [CrossRef]
- Gauthier, G.M.; Safdar, N.; Klein, B.S.; Andes, D.R. Blastomycosis in solid organ transplant recipients. Transpl. Infect. Dis. 2007, 9, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Grim, S.A.; Proia, L.; Miller, R.; Alhyraba, A.; Costas-Chavarri, J.; Oberholzer, J.; Clark, N.M. A multicenter study of histoplasmosis and blastomycosis after solid organ transplantation. Transpl. Infect. Dis. 2012, 14, 17–23. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Species | Geographic Range | Notes |
|---|---|---|
| B. dermatitidis | North America, including midwestern, southern, southeastern United States, the St. Lawrence Seaway, and midwestern Canadian provinces | By far the most common etiology of blastomycosis |
| B. gilchristii | Primarily in certain areas of Wisconsin and Ontario | Only distinguishable from B. dermatitidis by phylogenetic analysis |
| B. helicus | Western Canada and western United States | Rarely causes disease, mostly in immunocompromised hosts |
| B. percursus | Middle East, Africa | More bone and cutaneous manifestations than classic blastomycosis |
| B. emzantsi | South Africa | Geographically restricted, but presents similarly to B. percursus |
| B. parvus | North and South America, Eastern Europe, Australia | Causative agent of adiaspiromycosis in rodents; rare infection in humans |
| B. silverae | Western Canada | Not implicated in human disease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linder, K.A.; Kauffman, C.A.; Miceli, M.H. Blastomycosis: A Review of Mycological and Clinical Aspects. J. Fungi 2023, 9, 117. https://doi.org/10.3390/jof9010117
Linder KA, Kauffman CA, Miceli MH. Blastomycosis: A Review of Mycological and Clinical Aspects. Journal of Fungi. 2023; 9(1):117. https://doi.org/10.3390/jof9010117
Chicago/Turabian StyleLinder, Kathleen A., Carol A. Kauffman, and Marisa H. Miceli. 2023. "Blastomycosis: A Review of Mycological and Clinical Aspects" Journal of Fungi 9, no. 1: 117. https://doi.org/10.3390/jof9010117