
Breakthrough Acute Necrotizing Invasive Fungal Rhinosinusitis by Alternariaalternata in a Patient with Acute Lymphoblastic Leukemia on Anidulafungin Therapy and Case-Based Literature Review

 , ,
, , 
Abstract
:1. Introduction
2. Case Report
3. Mycological Workup
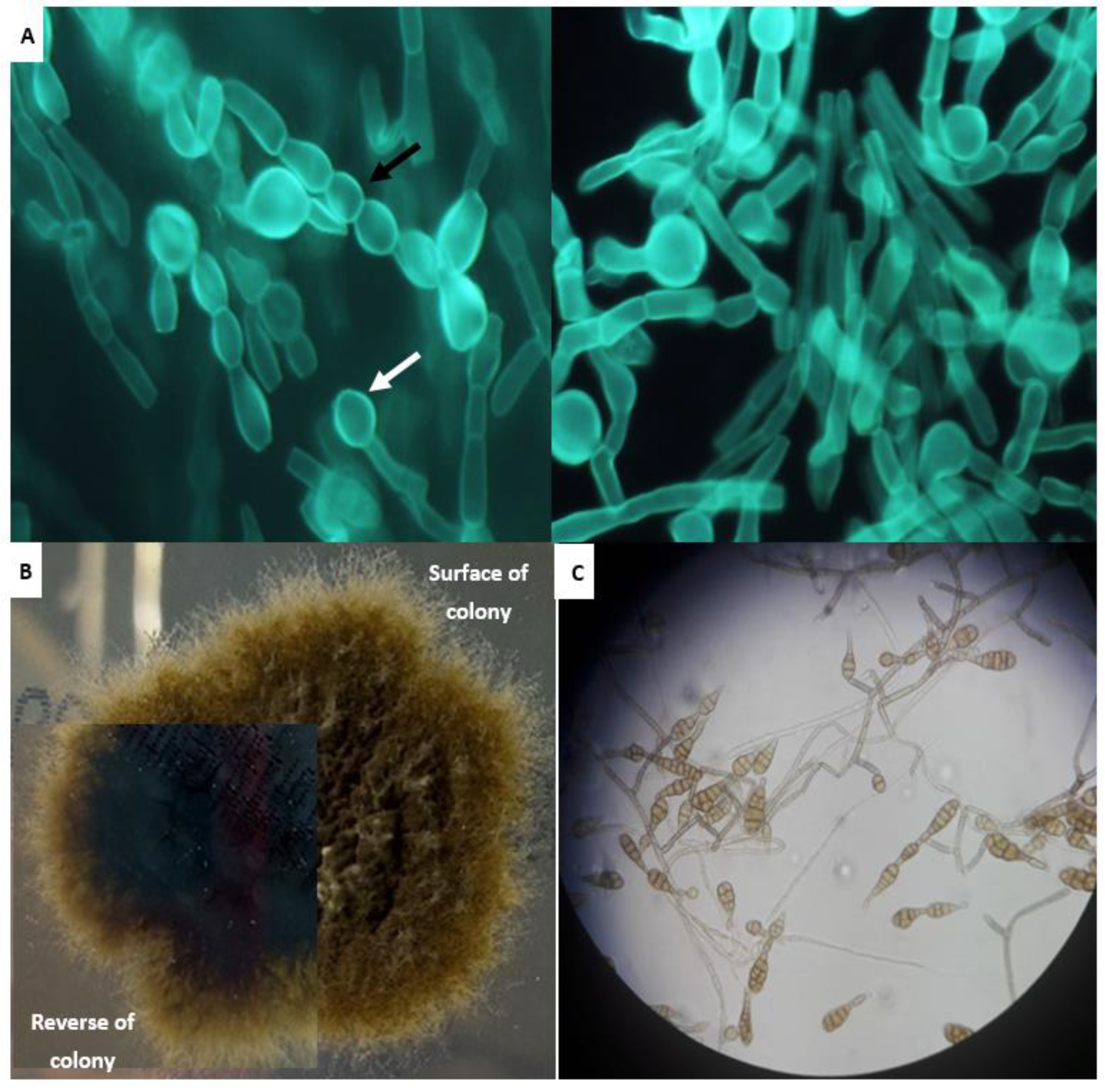
3.1. Culture
3.2. PCR
3.3. Antifungal Susceptibility Testing
4. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year of Publication (Reference) | Country, Study Period | Gender/Age (Years) | Predisposing Factors | Signs | Histopathology | Culture | Treatment | Outcome(Months Post-Surgery) |
|---|---|---|---|---|---|---|---|---|
| Morrison, 1993 [16] | USA, 1984 | M/38 | CML BMT (47 days pre-infection) Neutropenia | Bloody crust on nasal septum, necrotic appearing | Septate branching fungal hyphae invading the involved sinonasal tissue with areas of necrosis and vascular invasion | Alternaria spp. | Surgical debridement AMB therapy WBC transfusions | Died due to respiratory and graft failure; no sign of infection at autopsy (3 weeks) |
| Morrison, 1993 [16] | USA, 1985 | M/25 | ALL BMT (27 days pre-infection) Profound neutropenia | Superficial ulcer on nasal septum | Septate branching fungal hyphae invading the involved sinonasal tissue with areas of necrosis and vascular invasion | Alternaria spp. | Surgical debridement Antifungal therapy (AMB+5-FC) WBC transfusions | Alive (NA) |
| Morrison, 1993 [16] | USA, 1985 | M/13 | ALL BMT (15 days pre-infection) Profound neutropenia | Necrotic black lesion on nasal septum | Septate branching fungal hyphae invading the involved sinonasal tissue with areas of necrosis and vascular invasion | Alternaria spp. | Surgical debridement AMB therapy WBC transfusions | Alive (NA) |
| Morrison, 1993 [16] | USA, 1985 | F/26 | AML BMT (14 days pre-infection) Profound neutropenia | Small dark crust on middle turbinate | Septate branching fungal hyphae invading the involved sinonasal tissue with areas of necrosis and vascular invasion | Alternaria spp. | Surgical debridement AMB therapy | Alive (NA) |
| Morrison, 1993 [16] | USA, 1985 | F/37 | Aplastic anemia BMT (15 days pre-infection) Profound neutropenia | Black plaque on nasal septum | Septate branching fungal hyphae invading the involved sinonasal tissue with areas of necrosis and vascular invasion | Alternaria spp. | Surgical debridement AMB therapy | Died of aspiration pneumonia due to nasal bleeding; no sign of infection at autopsy (5 days post-surgery) |
| Wiest, 1993 [18] | USA, 1985 | M/31 | Acquired immunodeficiency syndrome | Black, necrotic-appearing lesion on the mucosa of the right nasal septum | Necrotic tissue with acute inflammation. Numerous, large, irregular septate hyphae | A. alternata | Surgical debridement AMB therapy | Died; no sign of infection at autopsy (8) |
| Morrison, 1993 [16] | USA, 1989 | F/39 | CLL BMT (27 days pre-infection) | Septal pallor, blood crusts in nose | Septate branching fungal hyphae invading the involved sinonasal tissue with areas of necrosis and vascular invasion | Alternaria spp. | Surgical debridement AMB therapy | Alive (NA) |
| Iwen, 1997 [19] | USA, 1985–1994 | F/35 | AML Profound neutropenia (30 days pre-infection) | Nasal necrosis | Pigmented, branching and septated moniliform hyphae | Alternaria spp. | Surgical debridement AMB therapy (25 days) | Alive (NA) |
| Chen, 2004 [17] | USA, 2003 | F/56 | AML Chemotherapy-induced neutropenia | Anterior nasal septal necrotic lesion with the overlying mucosa being slightly edematous and having a dusky appearance. | Multiple small fragments of squamous mucosa with ulceration and necrosis mixed with blood clot. Numerous hyphae elements with microconidia. | A. alternata | Surgical debridement AMB therapy | Died due to bacterial sepsis, but multiple cultures of nasal sinus content were negative (3) |
| Park, 2005 [15] | USA, 2000–2004 | Pediatric patient | Hematologic malignancy Profound neutropenia | Necrosis | NA | A. alternata | Surgical debridement Antifungal therapy | NA |
| Park, 2005 [15] | USA, 2000–2004 | Pediatric patient | Hematologic malignancy Profound neutropenia | Necrosis | NA | A. alternata | Surgical debridement Antifungal therapy | NA |
| Rabagliati, 2009 [20] | Chile, 2004–2008 | Adult patient | Hematologic malignancy Chemotherapy-induced neutropenia | NA | NA | Alternaria spp. | Surgical debridement VRC therapy | NA |
| Montone, 2011 [32] | USA, NA | F/51 | AML | NA | Invasion of fungal forms into submucosal tissue with frequent areas of tissue necrosis and angioinvasion | Alternaria spp. | NA | NA |
| Ardeshirpour, 2014 [14] | USA, 1994–2007 | F/6 | ALL Profound neutropenia (41 days pre-infection) | NA | NA | Alternaria spp. | Surgical debridement Antifungal therapy (AMB+CAS+VRC) G-CSF | Died from recurrent ALL, but without infection (2) |
| Ardeshirpour, 2014 [14] | USA, 1994–2007 | F/11 | AML Profound neutropenia (23 days pre-infection) | NA | NA | Alternaria spp. | Surgical debridement Antifungal therapy (AMB,+CAS+VRC) G-CSF | Alive (53) |
| Ardeshirpour, 2014 [14] | USA, 1994–2007 | F/9 | AML Profound neutropenia (13 days pre-infection) | NA | NA | Alternaria spp. | Surgical debridement Antifungal therapy (AMB+CAS+VRC) G-CSF | Alive (48) |
| Ardeshirpour, 2014 [14] | USA, 1994–2007 | M/11 | ALL Profound neutropenia (16 days pre-infection) | NA | NA | Alternaria spp. | Surgical debridement Antifungal therapy (AMB/L-AMB+ITC) G-CSF, WBC transfusions | Died from Scopulariopsis spp. throughout central nervous system (4) |
| Ardeshirpour, 2014 [14] | USA, 1994–2007 | M/2 | ALL Profound neutropenia (22 days pre-infection) | NA | NA | Alternaria spp. | Surgical debridement Antifungal therapy (AMB+ITC) G-CSF, WBC transfusions | Alive (32) |
| Ardeshirpour, 2014 [14] | USA, 1994–2007 | F/4 | AML Profound neutropenia (8 days pre-infection) | NA | NA | Alternaria spp. | Surgical debridement Antifungal therapy (AMB+ITC) WBC transfusions | Alive (37) |
| Ardeshirpour, 2014 [14] | USA, 1994–2007 | F/13 | ALL Profound neutropenia (16 days pre-infection) | NA | NA | Alternaria spp. | Surgical debridement Antifungal therapy (AMB+ITC) G-CSF, WBC transfusions | Alive (24) |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, V. Fungal Rhinosinusitis: Unravelling the Disease Spectrum. J. Maxillofac. Oral Surg. 2019, 18, 164–179. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.; Denning, D.W.; Ferguson, B.J.; Ponikau, J.; Buzina, W.; Kita, H.; Marple, B.; Panda, N.; Vlaminck, S.; Kauffmann-Lacroix, C.; et al. Fungal Rhinosinusitis: A Categorization and Definitional Schema Addressing Current Controversies. Laryngoscope 2009, 119, 1809. [Google Scholar] [CrossRef] [PubMed]
- Montone, K.T. Pathology of Fungal Rhinosinusitis: A Review. Head Neck Pathol. 2016, 10, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, J.R. Updates in management of acute invasive fungal rhinosinusitis. Curr. Opin. Otolaryngol. Head Neck Surg. 2019, 27, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.C.B.; Guimaraes, A.F.; de Oliveira, I.S.; de Sousa, P.H.M.; de Castro Romanelli, R.M.; Kakehasi, F.M.; de Sá Rodrigues, K.E. Acute invasive fungal rhinosinusitis in pediatric patients with oncohematological diseases. Hematol. Transfus. Cell Ther. 2022, 44, 32. [Google Scholar] [CrossRef] [PubMed]
- Wandell, G.M.; Miller, C.; Rathor, A.; Wai, T.H.; Guyer, R.A.; Schmidt, R.A.; Turner, J.H.; Hwang, P.H.; Davis, G.E.; Humphreys, I.M. A multi-institutional review of outcomes in biopsy-proven acute invasive fungal sinusitis. Int. Forum Allergy Rhinol. 2018, 8, 1459–1468. [Google Scholar] [CrossRef] [PubMed]
- Montone, K.T.; Livolsi, V.A.; Feldman, M.D.; Palmer, J.; Chiu, A.G.; Lanza, D.C.; Kennedy, D.W.; Loevner, L.A.; Nachamkin, I. Fungal Rhinosinusitis: A Retrospective Microbiologic and Pathologic Review of 400 Patients at a Single University Medical Center. Int. J. Otolaryngol. 2012, 2012, 684835. [Google Scholar] [CrossRef] [Green Version]
- Derber, C.; Elam, K.; Bearman, G. Invasive sinonasal disease due to dematiaceous fungi in immunocompromised individuals: Case report and review of the literature. Int. J. Infect. Dis. 2010, 14 (Suppl. S3), e329–e332. [Google Scholar] [CrossRef] [Green Version]
- White, T.J.; Bruns, T.; Lee, S.; Taylor, J. Amplification and direct sequencing of fungal ribosomal RNA genes for phylogenetics. In PCR Protocols; Elsevier: Amsterdam, The Netherlands, 1990; pp. 315–322. [Google Scholar]
- De Hoog, G.S.; Horré, R. Molecular taxonomy of the Alternaria and Ulocladium species from humans and their identification in the routine laboratory. Mycoses 2002, 45, 259–276. [Google Scholar] [CrossRef] [Green Version]
- Siopi, M.; Karakatsanis, S.; Roumpakis, C.; Korantanis, K.; Eldeik, E.; Sambatakou, H.; Sipsas, N.V.; Tsirigotis, P.; Pagoni, M.; Meletiadis, J. Performance, Correlation and Kinetic Profile of Circulating Serum Fungal Biomarkers of Invasive Aspergillosis in High- Risk Patients with Hematologic Malignancies. J. Fungi 2021, 7, 211. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi, 3rd ed.; CLSI document M38; Clinical and Laboratory Standards Institute: Malvern, PA, USA, 2017. [Google Scholar]
- Guinea, J.; Meletiadis, J.; Arikan-Akdagli, S.; Muehlethaler, K.; Gunnar, K.; Arendrup, M.; Subcommittee on Antifungal Susceptibility Testing of the ESCMID European Committe for Antimicrobial Susceptibility Testing. Eucast Definitive Document E.Def 9.3.2. Method for the Determination of Broth Dilution Minimum Inhibitory Concentrations of Antifungal Agents for Conidia Forming Moulds. Available online: http://www.eucast.org (accessed on 19 August 2022).
- Ardeshirpour, F.; Bohm, L.A.; Belani, K.K.; Sencer, S.F.; Lander, T.A.; Sidman, J.D. Surgery for pediatric invasive fungal sinonasal disease. Laryngoscope 2014, 124, 1008–1012. [Google Scholar] [CrossRef] [PubMed]
- Park, A.H.; Muntz, H.R.; Smith, M.E.; Afify, Z.; Pysher, T.; Pavia, A. Pediatric invasive fungal rhinosinusitis in immunocompromised children with cancer. Otolaryngol. Head Neck Surg. 2005, 133, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Morrison, V.A.; Weisdorf, D.J. Alternaria: A Sinonasal Pathogen of Immunocompromised Hosts. Clin. Infect. Dis. 1993, 16, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Thompson, K.; Taxy, J.B. Pathologic Quiz Case: A 56-Year-Old Woman With Anterior Nasal Pain and Intermittent Epistaxis. Arch. Pathol. Lab. Med. 2004, 128, 1451–1452. [Google Scholar] [CrossRef]
- Wiest, P.M.; Wiese, K.; Jacobs, M.R.; Morrissey, A.B.; Abelson, T.I.; Witt, W.; Lederman, M.M. Alternaria Infection in a Patient with Acquired Immunodeficiency Syndrome: Case Report and Review of Invasive Alternaria Infections. Rev. Infect. Dis. 1987, 9, 799–803. [Google Scholar] [CrossRef] [PubMed]
- Iwen, P.C.; Rupp, M.E.; Hinrichs, S.H. Invasive Mold Sinusitis: 17 Cases in Immunocompromised Patients and Review of the Literature. Clin. Infect. Dis. 1997, 24, 1178–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabagliati, B.R.; Fuentes, L.G.; Guzmán, D.A.M.; Orellana, U.E.; Oporto, C.J.; Aedo, C.I.; Garrido, S.M.; Nervi, N.B. Invasive fungal disease in hemato-oncological and hematopoietic stem cell transplantation patients from Hospital Clinico Universidad Católica, Santiago-Chile using revised EORTC/MSG diagnostic criteria. Rev. Chil. Infectol. 2009, 26, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Alastruey-izquierdo, A.; Cuesta, I.; Ros, L.; Mellado, E.; Rodriguez-tudela, J.L. Antifungal susceptibility profile of clinical Alternaria spp. identified by molecular methods. J. Antimicrob. Chemother. 2011, 66, 2585–2587. [Google Scholar] [CrossRef] [Green Version]
- Badali, H.; De Hoog, G.S.; Curfs-Breuker, I.; Andersen, B.; Meis, J.F. In vitro activities of eight antifungal drugs against 70 clinical and environmental isolates of Alternaria species. J. Antimicrob. Chemother. 2009, 63, 1295–1297. [Google Scholar] [CrossRef] [Green Version]
- Lafaurie, M.; Lapalu, J.; Raffoux, E.; Breton, B.; Lacroix, C.; Socié, G.; Porcher, R.; Ribaud, P.; Touratier, S.; Molina, J.M. High rate of breakthrough invasive aspergillosis among patients receiving caspofungin for persistent fever and neutropenia. Clin. Microbiol. Infect. 2010, 16, 1191–1196. [Google Scholar] [CrossRef] [Green Version]
- Lionakis, M.S.; Lewis, R.E.; Kontoyiannis, D.P. Breakthrough Invasive Mold Infections in the Hematology Patient: Current Concepts and Future Directions. Clin Infect Dis. 2018, 67, 1621–1630. [Google Scholar] [CrossRef] [PubMed]
- Siopi, M.; Perlin, D.S.; Arendrup, M.C.; Pournaras, S.; Meletiadis, J. Comparative Pharmacodynamics of Echinocandins against Aspergillus fumigatus Using an In Vitro Pharmacokinetic/Pharmacodynamic Model That Correlates with Clinical Response to Caspofungin Therapy: Is There a Place for Dose Optimization? Antimicrob. Agents Chemother. 2021, 65, e01618-20. [Google Scholar] [CrossRef] [PubMed]
- Chamilos, G.; Lewis, R.E.; Kontoyiannis, D.P. Delaying Amphotericin B–Based Frontline Therapy Significantly Increases Mortality among Patients with Hematologic Malignancy Who Have Zygomycosis. Clin. Infect. Dis. 2008, 47, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.; Babik, J.; Humphreys, I.M.; Davis, G.E. Diagnosis and Treatment of Acute Invasive Fungal Sinusitis in Cancer and Transplant Patients. Curr. Infect. Dis. Reports 2019, 21, 53. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Overview of antifungal ECOFFs and clinical breakpoints for yeasts, moulds and dermatophytes using the EUCAST E.Def 7.3, E.Def 9.4 and E.Def 11.0 procedures. 2022. Available online: https://www.eucast.org (accessed on 19 August 2022).
- Clinical and Laboratory Standards Institute (CLSI). Epidemiological Cutoff Values for Antifungal Susceptibility Testing, 3rd ed.; Supplement M59; Clinical and Laboratory Standards Institute (CLSI): Malvern, PA, USA, 2020. [Google Scholar]
- Pastor, F.J.; Guarro, J. Alternaria infections: Laboratory diagnosis and relevant clinical features. Clin. Microbiol. Infect. 2008, 14, 734–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhary, A.; Meis, J.F.F.; Guarro, J.; de Hoog, G.S.S.; Kathuria, S.; Arendrup, M.C.C.; Arikan-Akdagli, S.; Akova, M.; Boekhout, T.; Caira, M.; et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of systemic phaeohyphomycosis: Diseases caused by black fungi. Clin Microbiol. Infect 2014, 20 (Suppl. S3), 47–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montone, K.T.; LiVolsi, V.A.; Lanza, D.C.; Kennedy, D.W.; Palmer, J.; Chiu, A.G.; Feldman, M.D.; Loevner, L.A.; Nachamkin, I. In situ hybridization for specific fungal organisms in acute invasive fungal rhinosinusitis. Am. J. Clin. Pathol. 2011, 135, 190–199. [Google Scholar] [CrossRef] [Green Version]




| Laboratory Parameters | On the Day of ALL Diagnosis (22/6) | On the Day of FRS Diagnosis (14/7) |
|---|---|---|
| CRP (mg/L) | 332 | 88.8 |
| Glucose (mg/dL) | 105 | 119 |
| Urea (mg/dL) | 35.3 | 22.6 |
| White Blood Cells (109/L) | 24.8 | 0.33 |
| Neutrophils (109/L) | 0.23 | 0.16 |
| Lymphocytes (109/L) | 18.30 | 0.16 |
| Monocytes (109/L) | 6.07 | 0.01 |
| Basophils (109/L) | 0.15 | 0 |
| Red Blood Cells (1012/L) | 3.5 | 2.67 |
| Hemoglobin (g/L) | 10.3 | 7.9 |
| Hematocrit (%) | 29.8 | 22.4 |
| Platelet (103/μL) | 70 | 56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyrellis, G.; Siopi, M.; Leventakou, D.; Delides, A.; Maragkoudakis, P.; Korres, G.; Apostolopoulou, C.; Gouloumi, A.-R.; Pappa, V.; Pournaras, S.; et al. Breakthrough Acute Necrotizing Invasive Fungal Rhinosinusitis by Alternariaalternata in a Patient with Acute Lymphoblastic Leukemia on Anidulafungin Therapy and Case-Based Literature Review. J. Fungi 2022, 8, 879. https://doi.org/10.3390/jof8080879
Tyrellis G, Siopi M, Leventakou D, Delides A, Maragkoudakis P, Korres G, Apostolopoulou C, Gouloumi A-R, Pappa V, Pournaras S, et al. Breakthrough Acute Necrotizing Invasive Fungal Rhinosinusitis by Alternariaalternata in a Patient with Acute Lymphoblastic Leukemia on Anidulafungin Therapy and Case-Based Literature Review. Journal of Fungi. 2022; 8(8):879. https://doi.org/10.3390/jof8080879
Chicago/Turabian StyleTyrellis, Giorgos, Maria Siopi, Danai Leventakou, Alexander Delides, Pavlos Maragkoudakis, George Korres, Christina Apostolopoulou, Alina-Roxani Gouloumi, Vasiliki Pappa, Spyros Pournaras, and et al. 2022. "Breakthrough Acute Necrotizing Invasive Fungal Rhinosinusitis by Alternariaalternata in a Patient with Acute Lymphoblastic Leukemia on Anidulafungin Therapy and Case-Based Literature Review" Journal of Fungi 8, no. 8: 879. https://doi.org/10.3390/jof8080879